
A Comparative Study of Serum Angiogenic Biomarkers in Cirrhosis and Hepatocellular Carcinoma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Patients
2.2. Laboratory Procedures
2.3. Ethical Consideration
2.4. Statistical Analysis
3. Results
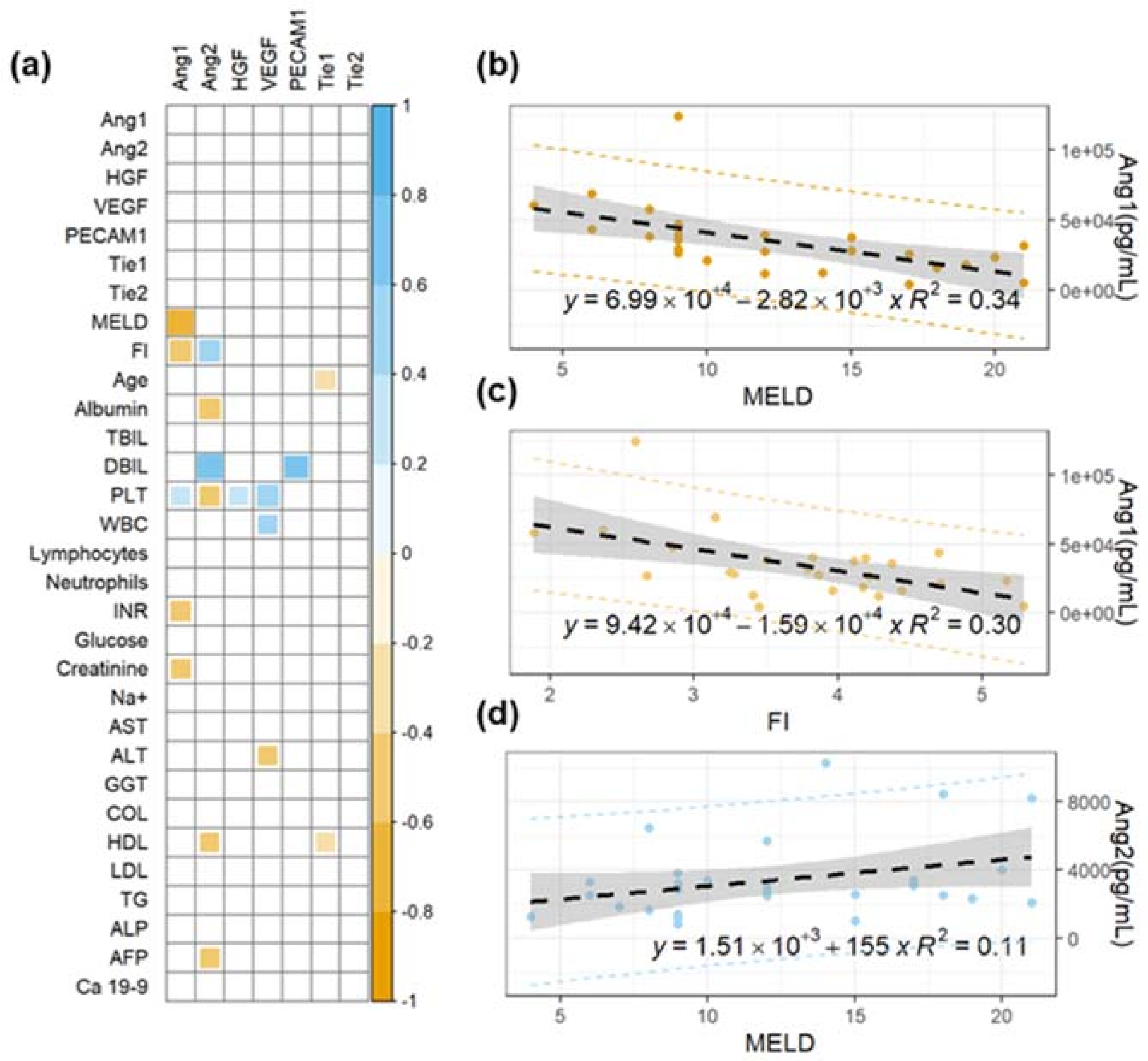
3.1. Analysis of Angiogenic Biomarkers in Cirrhotic Patients and Correlation with Clinical Parameters
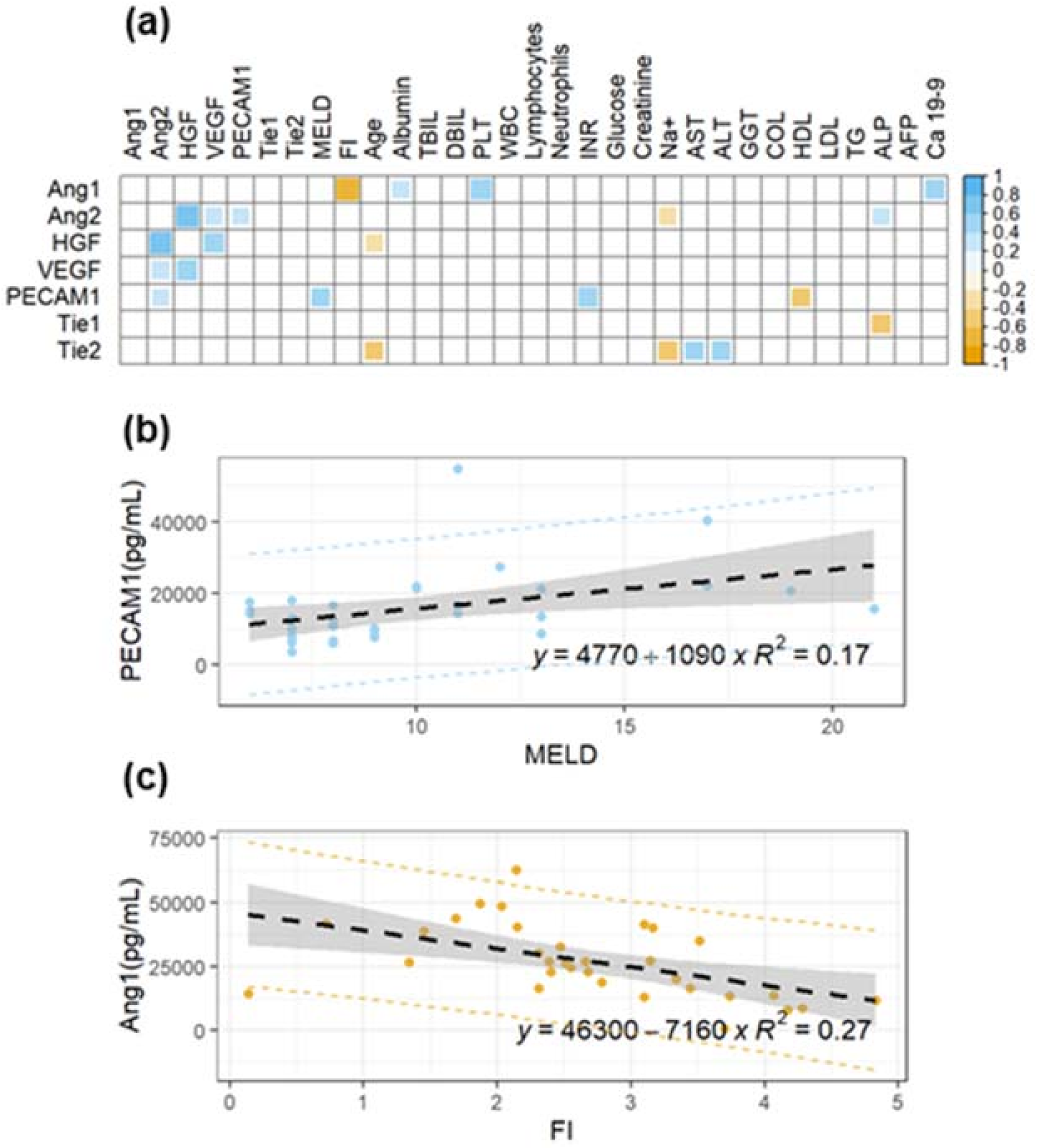
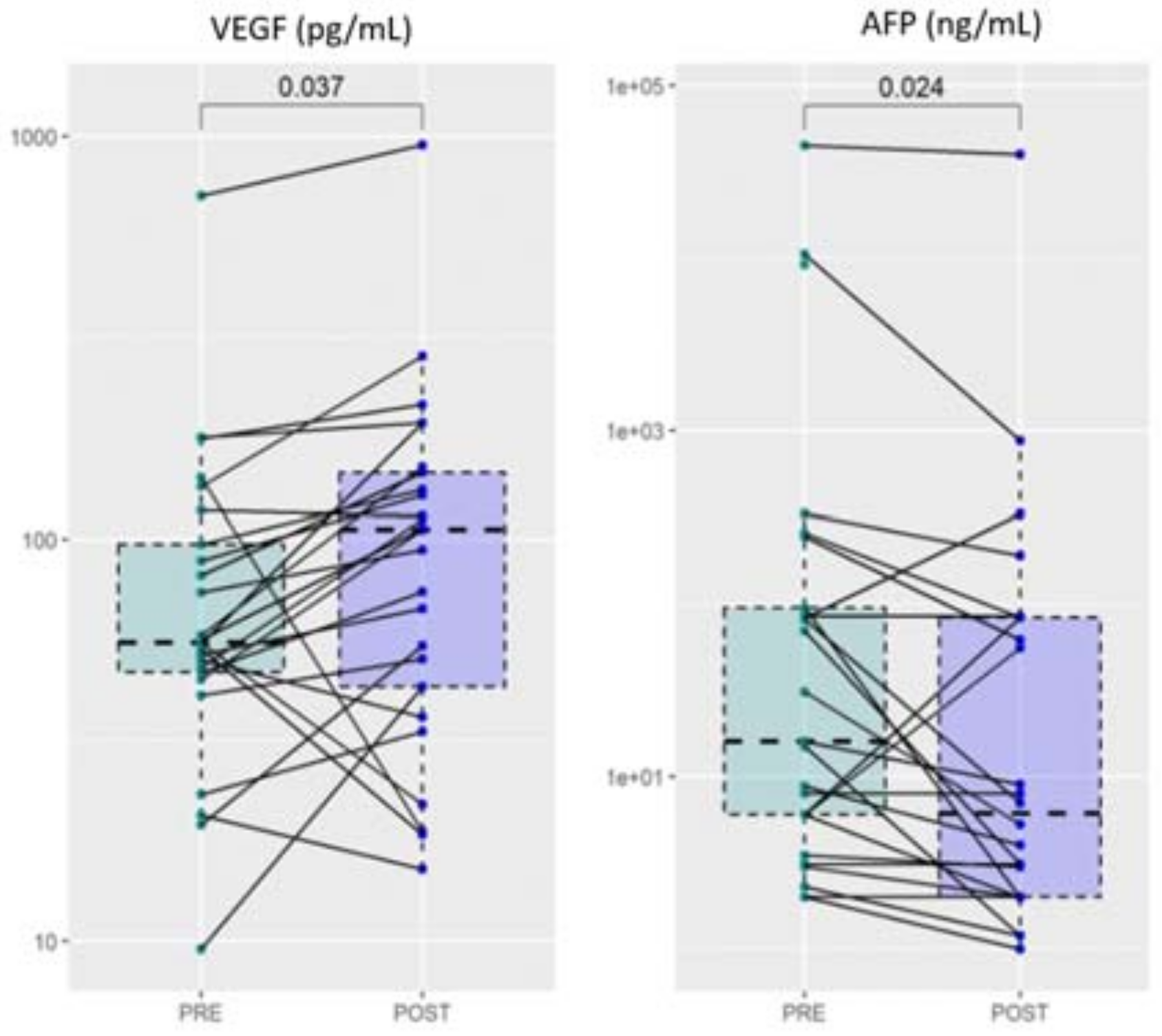
3.2. Analysis of Angiogenic Biomarkers in Patients with Hepatocellular Carcinoma and Correlation with Clinical Parameters
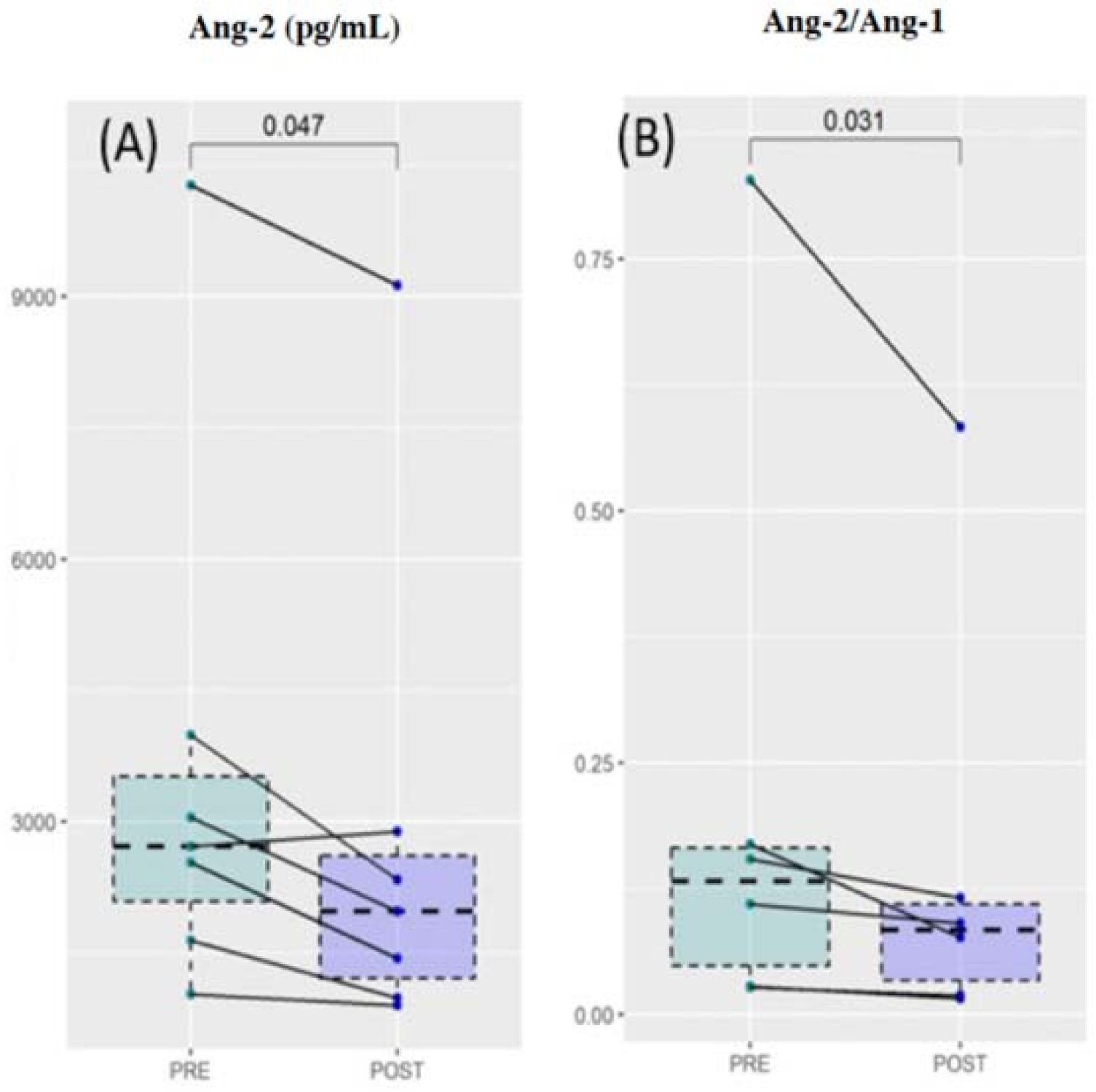
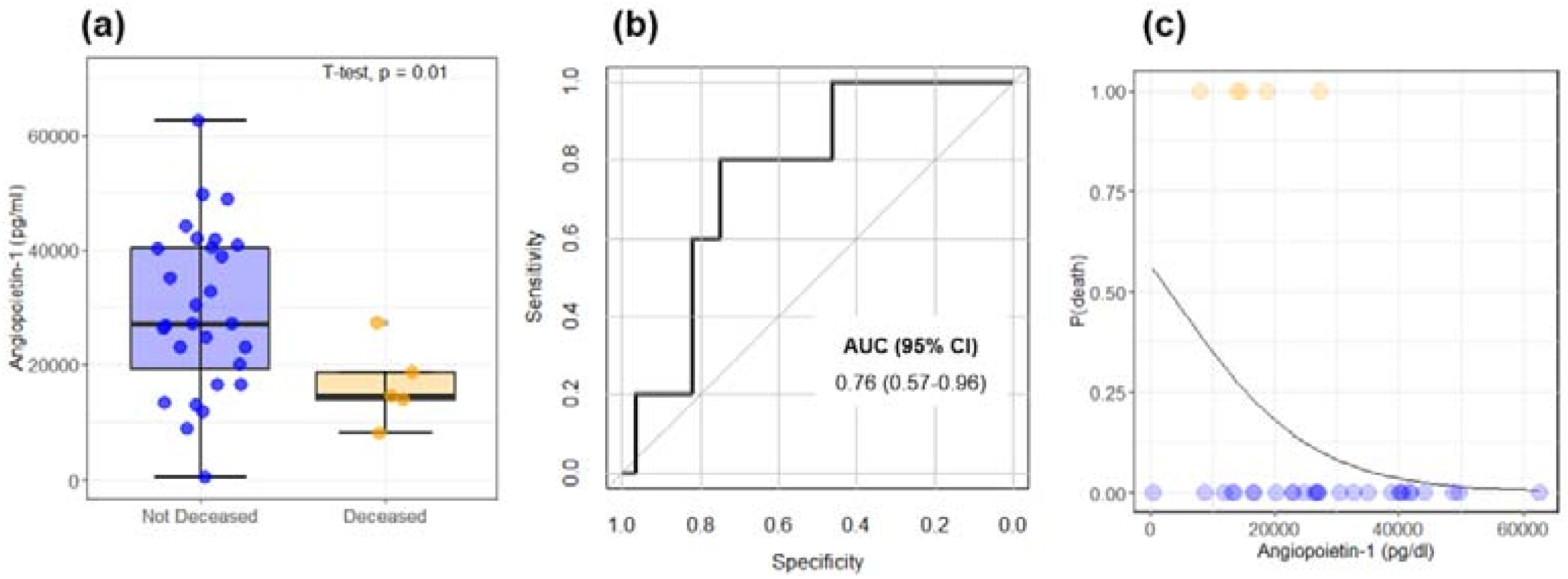
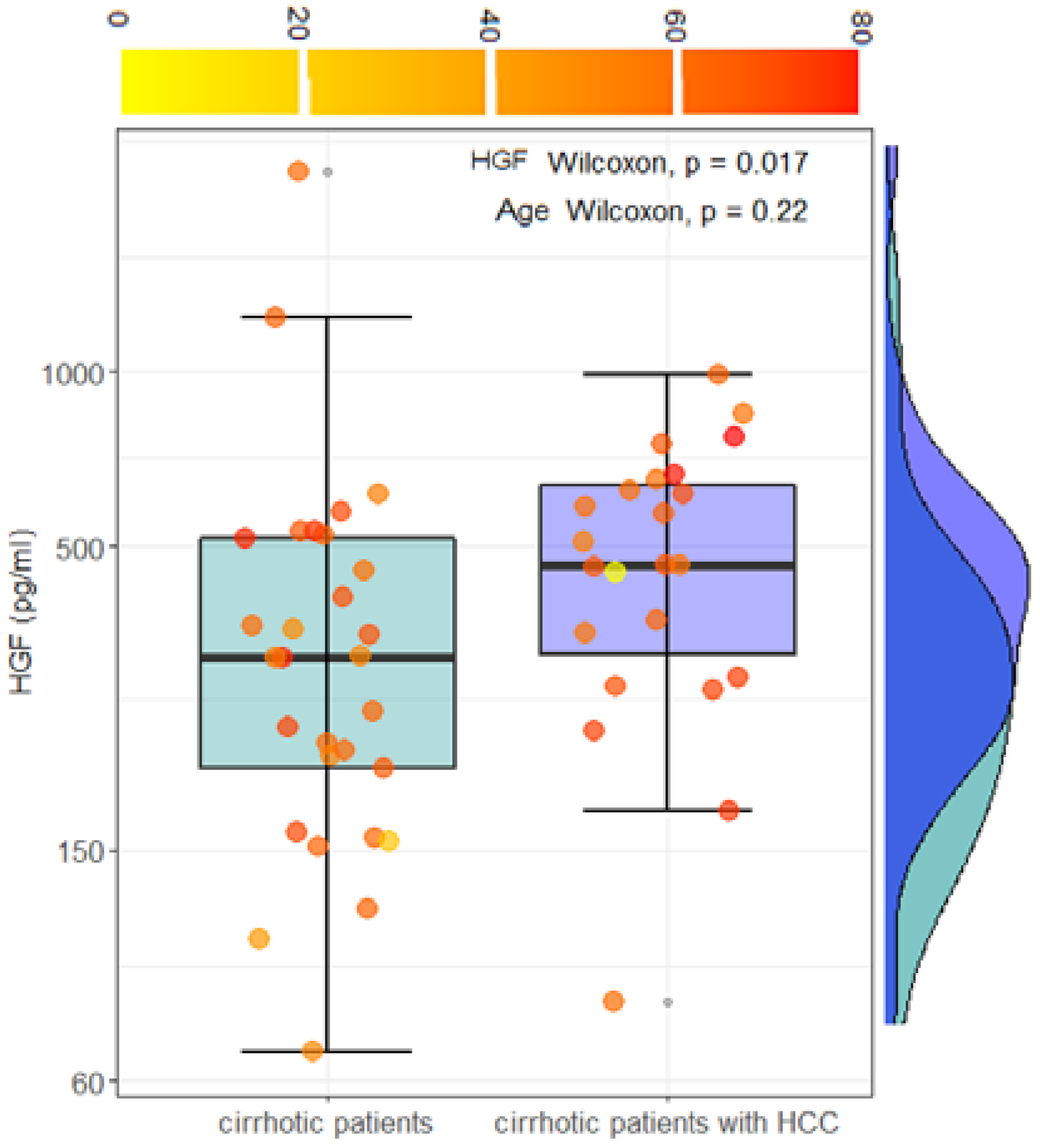
3.3. Clinical Significance of Angiogenic Biomarkers in the Progression of Chronic Liver Disease: A Comparison between Cirrhotic Patients and Cirrhotic Patients with Hepatocellular Carcinoma
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- AIOM, AIRTUM. I Numeri Del Cancro in Italia, X Edizione 2020. Available online: https://www.aiom.it/wp-content/uploads/2020/10/2020_Numeri_Cancro-operatori_web.pdf (accessed on 13 December 2021).
- Chang, M.-H.; You, S.-L.; Chen, C.-J.; Liu, C.-J.; Lee, C.-M.; Lin, S.-M.; Chu, H.-C.; Wu, T.-C.; Yang, S.-S.; Kuo, H.-S.; et al. Decreased Incidence of Hepatocellular Carcinoma in Hepatitis B Vaccinees: A 20-Year Follow-up Study. J. Natl. Cancer Inst. 2009, 101, 1348–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanyal, A.J.; Yoon, S.K.; Lencioni, R. The Etiology of Hepatocellular Carcinoma and Consequences for Treatment. Oncologist 2010, 15 (Suppl. 4), 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchese, S.; Polo, A.; Ariano, A.; Velotto, S.; Costantini, S.; Severino, L. Aflatoxin B1 and M1: Biological Properties and Their Involvement in Cancer Development. Toxins 2018, 10, 214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez-Gea, V.; Toffanin, S.; Friedman, S.L.; Llovet, J.M. Role of the Microenvironment in the Pathogenesis and Treatment of Hepatocellular Carcinoma. Gastroenterology 2013, 144, 512–527. [Google Scholar] [CrossRef] [Green Version]
- Kerbel, R.S. Tumor Angiogenesis. N. Engl. J. Med. 2008, 358, 2039–2049. [Google Scholar] [CrossRef] [Green Version]
- Krishna Priya, S.; Nagare, R.P.; Sneha, V.S.; Sidhanth, C.; Bindhya, S.; Manasa, P.; Ganesan, T.S. Tumour Angiogenesis-Origin of Blood Vessels. Int. J. Cancer 2016, 139, 729–735. [Google Scholar] [CrossRef]
- Elpek, G.Ö. Angiogenesis and Liver Fibrosis. World J. Hepatol. 2015, 7, 377–391. [Google Scholar] [CrossRef]
- Tammela, T.; Enholm, B.; Alitalo, K.; Paavonen, K. The Biology of Vascular Endothelial Growth Factors. Cardiovasc. Res. 2005, 65, 550–563. [Google Scholar] [CrossRef]
- Ciasca, G.; Sassun, T.E.; Minelli, E.; Antonelli, M.; Papi, M.; Santoro, A.; Giangaspero, F.; Delfini, R.; Spirito, M.D. Nano-Mechanical Signature of Brain Tumours. Nanoscale 2016, 8, 19629–19643. [Google Scholar] [CrossRef]
- Pezzuto, A.; Carico, E. Role of HIF-1 in Cancer Progression: Novel Insights. A Review. Curr. Mol. Med. 2018, 18, 343–351. [Google Scholar] [CrossRef]
- Tsigkos, S.; Koutsilieris, M.; Papapetropoulos, A. Angiopoietins in Angiogenesis and Beyond. Expert Opin. Investig. Drugs 2003, 12, 933–941. [Google Scholar] [CrossRef]
- Augustin, H.G.; Koh, G.Y.; Thurston, G.; Alitalo, K. Control of Vascular Morphogenesis and Homeostasis through the Angiopoietin-Tie System. Nat. Rev. Mol. Cell Biol. 2009, 10, 165–177. [Google Scholar] [CrossRef]
- Naldini, A.; Carraro, F. Role of Inflammatory Mediators in Angiogenesis. Curr. Drug Targets Inflamm. Allergy 2005, 4, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Jeon, B.H.; Khanday, F.; Deshpande, S.; Haile, A.; Ozaki, M.; Irani, K. Tie-Ing the Antiinflammatory Effect of Angiopoietin-1 to Inhibition of NF-KappaB. Circ. Res. 2003, 92, 586–588. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, C.C.; Du, L.; Chu, D.; Cho, A.J.; Kido, M.; Wolf, P.L.; Jamieson, S.W.; Thistlethwaite, P.A. Induction of Pulmonary Hypertension by an Angiopoietin 1/TIE2/Serotonin Pathway. Proc. Natl. Acad. Sci. USA 2003, 100, 12331–12336. [Google Scholar] [CrossRef] [Green Version]
- Koh, G.Y. Orchestral Actions of Angiopoietin-1 in Vascular Regeneration. Trends Mol. Med. 2013, 19, 31–39. [Google Scholar] [CrossRef]
- Fiedler, U.; Augustin, H.G. Angiopoietins: A Link between Angiogenesis and Inflammation. Trends Immunol. 2006, 27, 552–558. [Google Scholar] [CrossRef]
- Fiedler, U.; Reiss, Y.; Scharpfenecker, M.; Grunow, V.; Koidl, S.; Thurston, G.; Gale, N.W.; Witzenrath, M.; Rosseau, S.; Suttorp, N.; et al. Angiopoietin-2 Sensitizes Endothelial Cells to TNF-Alpha and Has a Crucial Role in the Induction of Inflammation. Nat. Med. 2006, 12, 235–239. [Google Scholar] [CrossRef]
- Scharpfenecker, M.; Fiedler, U.; Reiss, Y.; Augustin, H.G. The Tie-2 Ligand Angiopoietin-2 Destabilizes Quiescent Endothelium through an Internal Autocrine Loop Mechanism. J. Cell Sci. 2005, 118, 771–780. [Google Scholar] [CrossRef] [Green Version]
- Sugimachi, K.; Tanaka, S.; Taguchi, K.; Aishima, S.; Shimada, M.; Tsuneyoshi, M. Angiopoietin Switching Regulates Angiogenesis and Progression of Human Hepatocellular Carcinoma. J. Clin. Pathol. 2003, 56, 854–860. [Google Scholar] [CrossRef] [Green Version]
- Selden, C.; Farnaud, S.; Ding, S.F.; Habib, N.; Foster, C.; Hodgson, H.J. Expression of Hepatocyte Growth Factor MRNA, and c-Met MRNA (Hepatocyte Growth Factor Receptor) in Human Liver Tumours. J. Hepatol. 1994, 21, 227–234. [Google Scholar] [CrossRef]
- Noguchi, O.; Enomoto, N.; Ikeda, T.; Kobayashi, F.; Marumo, F.; Sato, C. Gene Expressions of C-Met and Hepatocyte Growth Factor in Chronic Liver Disease and Hepatocellular Carcinoma. J. Hepatol. 1996, 24, 286–292. [Google Scholar] [CrossRef]
- Guirouilh, J.; Castroviejo, M.; Balabaud, C.; Desmouliere, A.; Rosenbaum, J. Hepatocarcinoma Cells Stimulate Hepatocyte Growth Factor Secretion in Human Liver Myofibroblasts. Int. J. Oncol. 2000, 17, 777–781. [Google Scholar] [CrossRef]
- Vejchapipat, P.; Tangkijvanich, P.; Theamboonlers, A.; Chongsrisawat, V.; Chittmittrapap, S.; Poovorawan, Y. Association between Serum Hepatocyte Growth Factor and Survival in Untreated Hepatocellular Carcinoma. J. Gastroenterol. 2004, 39, 1182–1188. [Google Scholar] [CrossRef]
- Breuhahn, K.; Longerich, T.; Schirmacher, P. Dysregulation of Growth Factor Signaling in Human Hepatocellular Carcinoma. Oncogene 2006, 25, 3787–3800. [Google Scholar] [CrossRef] [Green Version]
- Nalesnik, M.A.; Michalopoulos, G.K. Growth Factor Pathways in Development and Progression of Hepatocellular Carcinoma. Front. Biosci. 2012, 4, 1487–1515. [Google Scholar] [CrossRef]
- DeLisser, H.M.; Newman, P.J.; Albelda, S.M. Molecular and Functional Aspects of PECAM-1/CD31. Immunol. Today 1994, 15, 490–495. [Google Scholar] [CrossRef]
- DeLisser, H.M.; Christofidou-Solomidou, M.; Strieter, R.M.; Burdick, M.D.; Robinson, C.S.; Wexler, R.S.; Kerr, J.S.; Garlanda, C.; Merwin, J.R.; Madri, J.A.; et al. Involvement of Endothelial PECAM-1/CD31 in Angiogenesis. Am. J. Pathol. 1997, 151, 671–677. [Google Scholar]
- McCormick, B.A.; Zetter, B.R. Adhesive Interactions in Angiogenesis and Metastasis. Pharmacol. Ther. 1992, 53, 239–260. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver A; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar]
- Ohta, T.; Sakaguchi, K.; Fujiwara, A.; Fujioka, S.; Iwasaki, Y.; Makino, Y.; Araki, Y.; Shiratori, Y. Simple Surrogate Index of the Fibrosis Stage in Chronic Hepatitis C Patients Using Platelet Count and Serum Albumin Level. Acta Med. Okayama 2006, 60, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Jung, G.E.; Encke, J.; Schmidt, J.; Rahmel, A. Model for end-stage liver disease. Chirurg 2008, 79, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tsao, G.; Groszmann, R.J.; Fisher, R.L.; Conn, H.O.; Atterbury, C.E.; Glickman, M. Portal Pressure, Presence of Gastroesophageal Varices and Variceal Bleeding. Hepatology 1985, 5, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Paquet, K.J. Prophylactic Endoscopic Sclerosing Treatment of the Esophageal Wall in Varices—A Prospective Controlled Randomized Trial. Endoscopy 1982, 14, 4–5. [Google Scholar] [CrossRef]
- Wei, T.; Simko, V.; Levy, M.; Xie, Y.; Jin, Y.; Zemla, J. Package ‘Corrplot’. Statistician 2017, 56, e24. [Google Scholar]
- Napodano, C.; Callà, C.; Fiorita, A.; Marino, M.; Taddei, E.; Di Cesare, T.; Passali, G.C.; Di Santo, R.; Stefanile, A.; Fantoni, M.; et al. Salivary Biomarkers in COVID-19 Patients: Towards a Wide-Scale Test for Monitoring Disease Activity. J. Pers. Med. 2021, 11, 385. [Google Scholar] [CrossRef]
- Basile, U.; Miele, L.; Napodano, C.; Ciasca, G.; Gulli, F.; Pocino, K.; De Matthaeis, N.; Liguori, A.; De Magistris, A.; Marrone, G.; et al. The Diagnostic Performance of PIVKA-II in Metabolic and Viral Hepatocellular Carcinoma: A Pilot Study. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 12675–12685. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.-C.; Müller, M. PROC: An Open-Source Package for R and S+ to Analyze and Compare ROC Curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Pestana, R.C.; Hassan, M.M.; Abdel-Wahab, R.; Abugabal, Y.I.; Girard, L.M.; Li, D.; Chang, P.; Raghav, K.; Morris, J.; Wolff, R.A. Clinical and Prognostic Significance of Circulating Levels of Angiopoietin-1 and Angiopoietin-2 in Hepatocellular Carcinoma. Oncotarget 2018, 9, 37721. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Bartolomé, Á.; López-Rodríguez, R.; Borque, M.J.; González-Moreno, L.; Real-Martínez, Y.; García-Buey, L.; Moreno-Otero, R.; Sanz-Cameno, P. Angiopoietin-2/Angiopoietin-1 as Non-Invasive Biomarker of Cirrhosis in Chronic Hepatitis C. World J. Gastroenterol. 2016, 22, 9744. [Google Scholar] [CrossRef]
- Di Sandro, S.; Benuzzi, L.; Lauterio, A.; Botta, F.; De Carlis, R.; Najjar, M.; Centonze, L.; Danieli, M.; Pezzoli, I.; Rampoldi, A.; et al. Single Hepatocellular Carcinoma Approached by Curative-Intent Treatment: A Propensity Score Analysis Comparing Radiofrequency Ablation and Liver Resection. Eur. J. Surg. Oncol. 2019, 45, 1691–1699. [Google Scholar] [CrossRef]
- Lee, S.C.; Tan, H.T.; Chung, M.C.M. Prognostic Biomarkers for Prediction of Recurrence of Hepatocellular Carcinoma: Current Status and Future Prospects. World J. Gastroenterol. 2014, 20, 3112–3124. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.-R.; Moon, H.-E.; Kim, K.-W. Hypoxia-Induced Angiogenesis in Human Hepatocellular Carcinoma. J. Mol. Med. 2002, 80, 703–714. [Google Scholar] [CrossRef]
- Dong, G.; Lin, X.-H.; Liu, H.-H.; Gao, D.-M.; Cui, J.-F.; Ren, Z.-G.; Chen, R.-X. Intermittent Hypoxia Alleviates Increased VEGF and Pro-Angiogenic Potential in Liver Cancer Cells. Oncol. Lett. 2019, 18, 1831–1839. [Google Scholar] [CrossRef]
- Scholz, A.; Rehm, V.A.; Rieke, S.; Derkow, K.; Schulz, P.; Neumann, K.; Koch, I.; Pascu, M.; Wiedenmann, B.; Berg, T.; et al. Angiopoietin-2 Serum Levels Are Elevated in Patients with Liver Cirrhosis and Hepatocellular Carcinoma. Am. J. Gastroenterol. 2007, 102, 2471–2481. [Google Scholar] [CrossRef]
- Ljubimova, J.Y.; Petrovic, L.M.; Wilson, S.E.; Geller, S.A.; Demetriou, A.A. Expression of HGF, Its Receptor c-Met, c-Myc, and Albumin in Cirrhotic and Neoplastic Human Liver Tissue. J. Histochem. Cytochem. 1997, 45, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.-Y.; Kong, L.-Q.; Zhu, X.-D.; Cai, H.; Wang, C.-H.; Shi, W.-K.; Cao, M.-Q.; Li, X.-L.; Li, K.-S.; Zhang, S.-Z.; et al. CD31 Regulates Metastasis by Inducing Epithelial-Mesenchymal Transition in Hepatocellular Carcinoma via the ITGB1-FAK-Akt Signaling Pathway. Cancer Lett. 2018, 429, 29–40. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Cirrhosis | HCC |
|---|---|---|
| No. of patients | 29 | 33 |
| Age mean/median (IQR) | 62/63(11) | 67/67(15) |
| Gender (M/F) | 11/18 | 24/9 |
| Underlying liver disease | ||
| Cirrhosis | 29 | 24 |
| Steatosis (NASH) | – | 4 |
| Healthy liver | – | 5 |
| Etiology | ||
| HCV | 4 | 11 |
| HBV | 2 | 5 |
| HCV and HBV | 1 | 1 |
| Potus | 2 | 7 |
| Metabolic | 7 | 8 |
| Cryptogenic | 13 | 6 |
| Portal hypertension | 7 | 17 |
| Esophageal varices | 16 | 9 |
| Nodule size (cm) | – | |
| <2 | 8 | |
| 2–5 | 14 | |
| >5 | 11 | |
| Vascular thrombosis | – | 4 |
| Ascites | 6 | 7 |
| Encephalopathy | 6 | 2 |
| Diabetes | 18 | 10 |
| BCLC | – | |
| 0 | 4 | |
| A | 14 | |
| B | 4 | |
| C | 3 | |
| D | 1 | |
| Child–Pugh | ||
| A | 14 | 20 |
| B | 11 | 7 |
| C | 4 | – |
| MELD | ||
| 0–9 | 13 | 20 |
| 10–19 | 13 | 12 |
| 20–29 | 3 | 1 |
| Treatment | ||
| HCV treatment (DAAs) | 5 | 12 |
| HBV treatment | 2 | 5 |
| Hepatic resection | - | 6 |
| Transplant | - | 3 |
| Sorafenib | - | 4 |
| Local–regional | - | 9 |
| Best supportive care | - | 5 |
| Exitus (death) | - | 5 |
| Cirrhotic Patients without HCC | Cirrhotic Patients with HCC | Wilcoxon | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Angiogenic Markers | n | Mean | SD | Median | IQR | n | Mean | SD | Median | IQR | w | p |
| Ang-1 (pg/mL) | 26 | 34,435 | 24,517 | 28,900 | 20,541 | 23 | 23,005 | 10,517 | 22,900 | 12,965 | 391 | 0.066 |
| Ang-2 (pg/mL) | 29 | 3401.4 | 2312.83 | 2869.45 | 1322.51 | 23 | 3377.96 | 2113.74 | 2906.95 | 1680. | 311 | 0.688 |
| Ang2/Ang1 | 22 | 0.25 | 0.36 | 0.13 | 0.09 | 23 | 0.19 | 0.14 | 0.14 | 0.22 | 245 | 0.866 |
| HGF (pg/mL) | 29 | 411.45 | 414.51 | 320.93 | 309.30 | 23 | 500.32 | 224.58 | 464.56 | 310.90 | 203 | 0.017 |
| VEGF (pg/mL) | 29 | 91.91 | 73.99 | 69.75 | 72.22 | 23 | 92.63 | 66.63 | 56.36 | 91.04 | 312 | 0.701 |
| PECAM1 (pg/mL) | 29 | 15,237 | 5415.34 | 14,483.60 | 9571.68 | 23 | 16,260.82 | 11,400.07 | 13,429.44 | 7652.7 | 369 | 0.522 |
| TIE1 (pg/mL) | 29 | 9.82 | 3.79 | 9.11 | 5.17 | 23 | 9.57 | 7.10 | 7.52 | 7.75 | 412 | 0.152 |
| TIE2 (pg/mL) | 29 | 22.40 | 8.36 | 22.51 | 10.86 | 23 | 20.91 | 7.48 | 21.25 | 10.62 | 357 | 0.674 |
| Cirrhotic Patients without HCC | Cirrhotic Patients with HCC | Wilcoxon | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Plasma Markers | n | Mean | SD | Median | IQR | n | Mean | SD | Median | IQR | w | p-Value |
| Albumin | 29 | 30.3448 | 6.48777 | 29 | 9 | 23 | 37.2174 | 6.68755 | 39 | 11 | 154.5 | 0.001 |
| COL | 29 | 134.241 | 39.5769 | 133 | 30 | 23 | 155.609 | 46.2884 | 144 | 44 | 216 | 0.031 |
| LDL | 29 | 78.9517 | 31.7226 | 76 | 32.4 | 23 | 95.087 | 31.8661 | 92 | 19 | 184.5 | 0.0062 |
| AFP | 29 | 3.76931 | 3.00572 | 3 | 4 | 23 | 667.313 | 2273.62 | 8.8 | 80 | 126 | 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pocino, K.; Napodano, C.; Marino, M.; Di Santo, R.; Miele, L.; De Matthaeis, N.; Gulli, F.; Saporito, R.; Rapaccini, G.L.; Ciasca, G.; et al. A Comparative Study of Serum Angiogenic Biomarkers in Cirrhosis and Hepatocellular Carcinoma. Cancers 2022, 14, 11. https://doi.org/10.3390/cancers14010011
Pocino K, Napodano C, Marino M, Di Santo R, Miele L, De Matthaeis N, Gulli F, Saporito R, Rapaccini GL, Ciasca G, et al. A Comparative Study of Serum Angiogenic Biomarkers in Cirrhosis and Hepatocellular Carcinoma. Cancers. 2022; 14(1):11. https://doi.org/10.3390/cancers14010011
Chicago/Turabian StylePocino, Krizia, Cecilia Napodano, Mariapaola Marino, Riccardo Di Santo, Luca Miele, Nicoletta De Matthaeis, Francesca Gulli, Raffaele Saporito, Gian Ludovico Rapaccini, Gabriele Ciasca, and et al. 2022. "A Comparative Study of Serum Angiogenic Biomarkers in Cirrhosis and Hepatocellular Carcinoma" Cancers 14, no. 1: 11. https://doi.org/10.3390/cancers14010011