
Potential to Improve Therapy of Chronic Myeloid Leukemia (CML), Especially for Patients with Older Age: Incidence, Mortality, and Survival Rates of Patients with CML in Switzerland from 1995 to 2017

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Sources and Inclusion Criteria
2.3. Analytic Methods
3. Results
3.1. Study Population
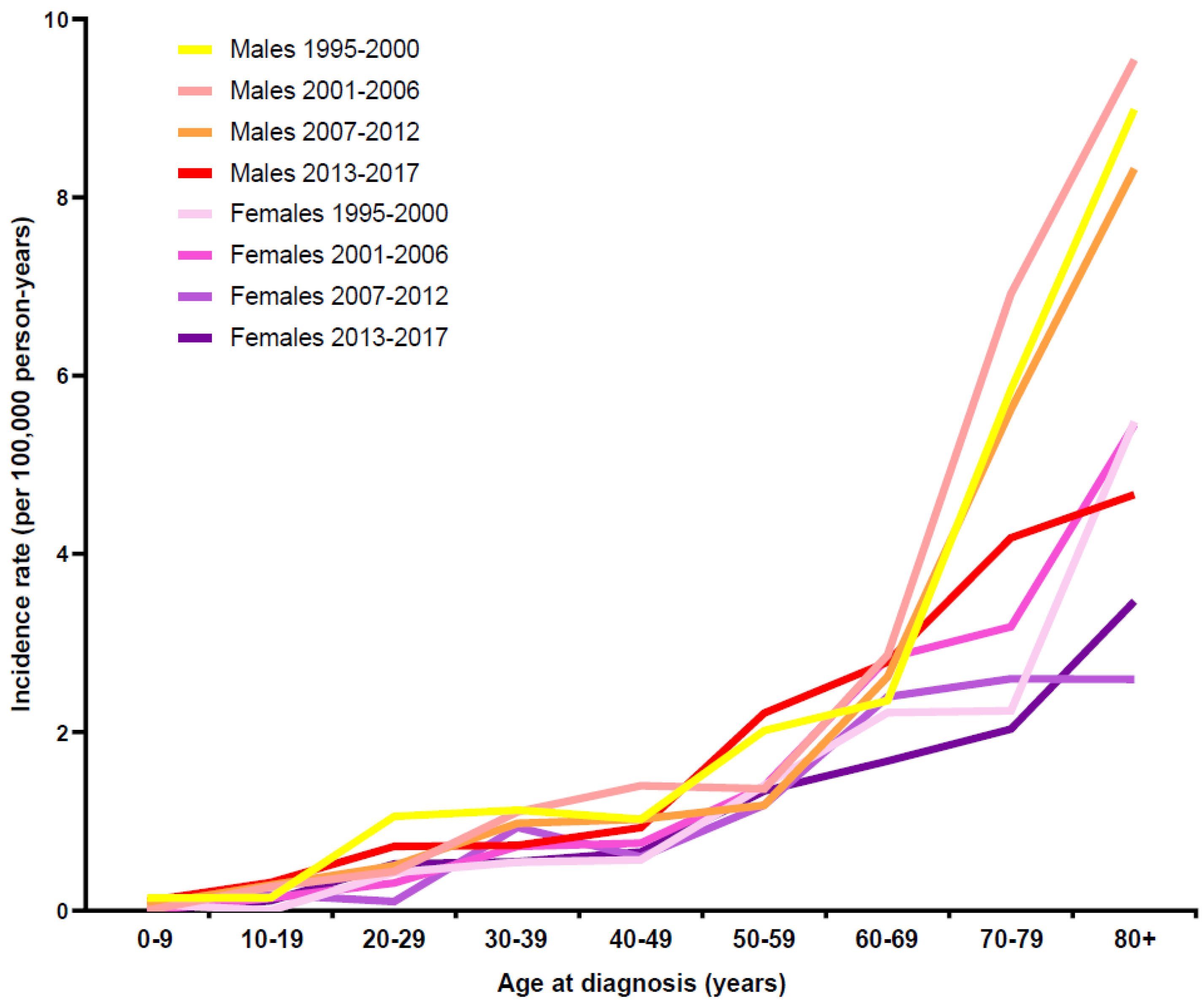
3.2. Incidence
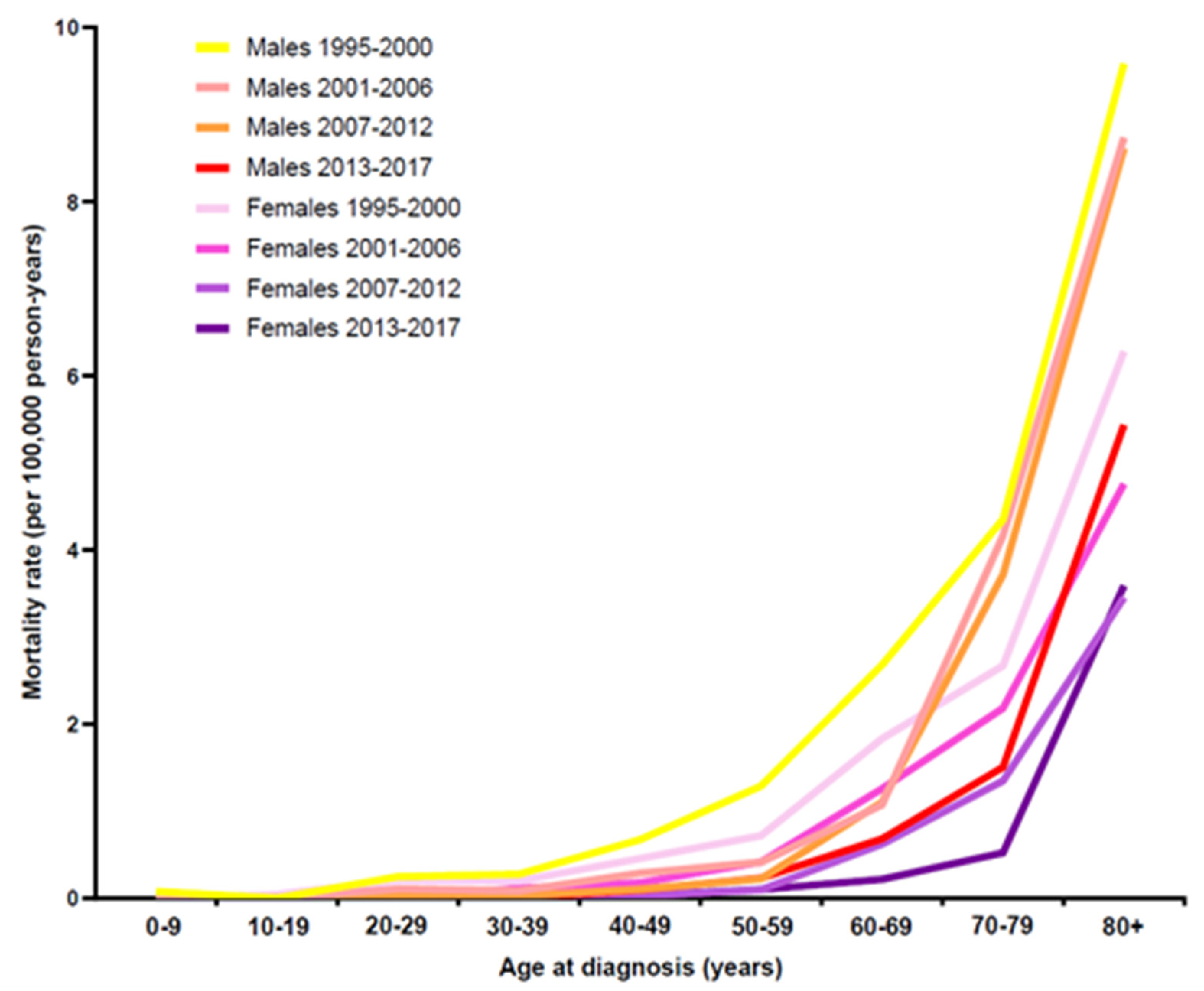
3.3. Mortality
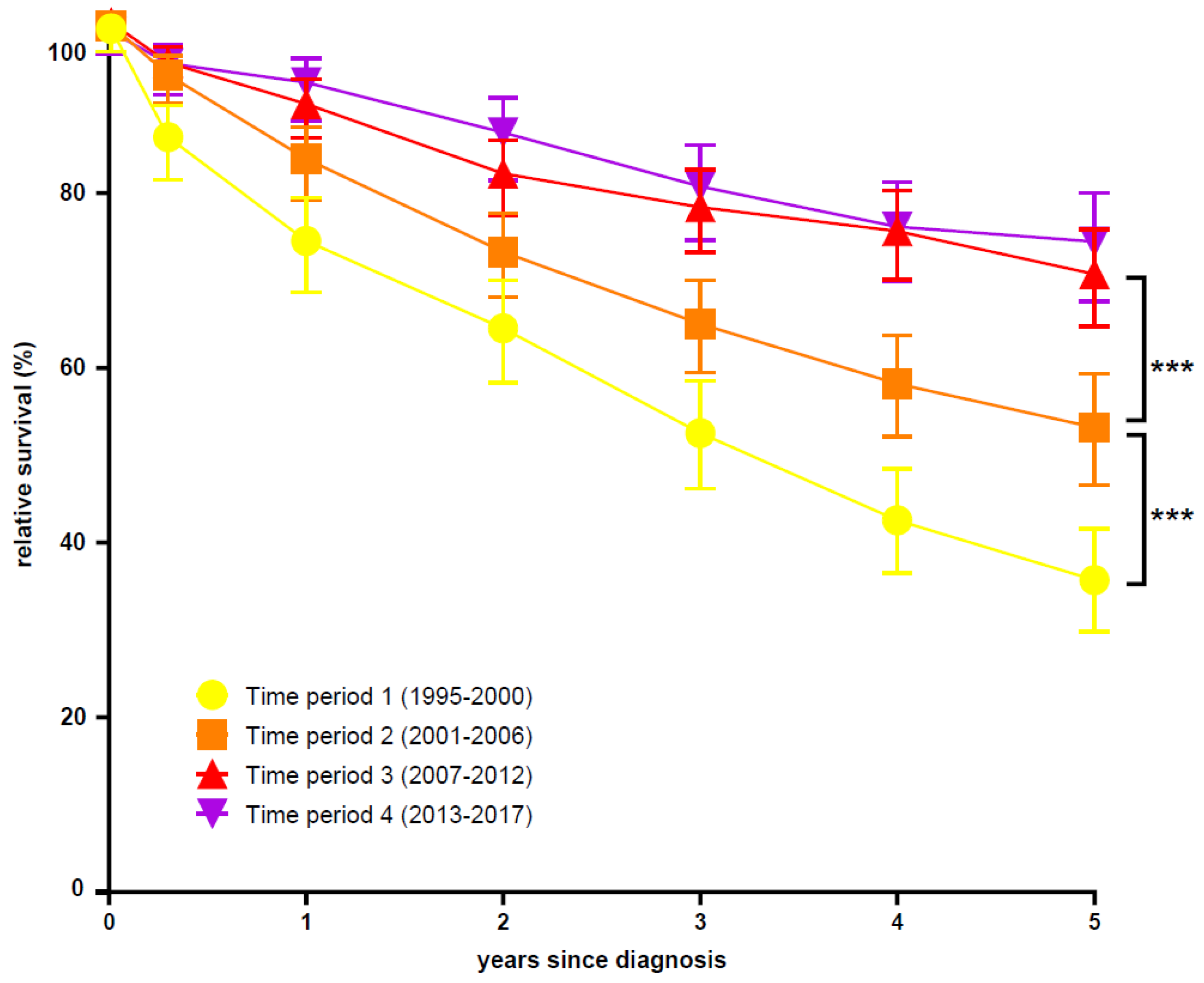
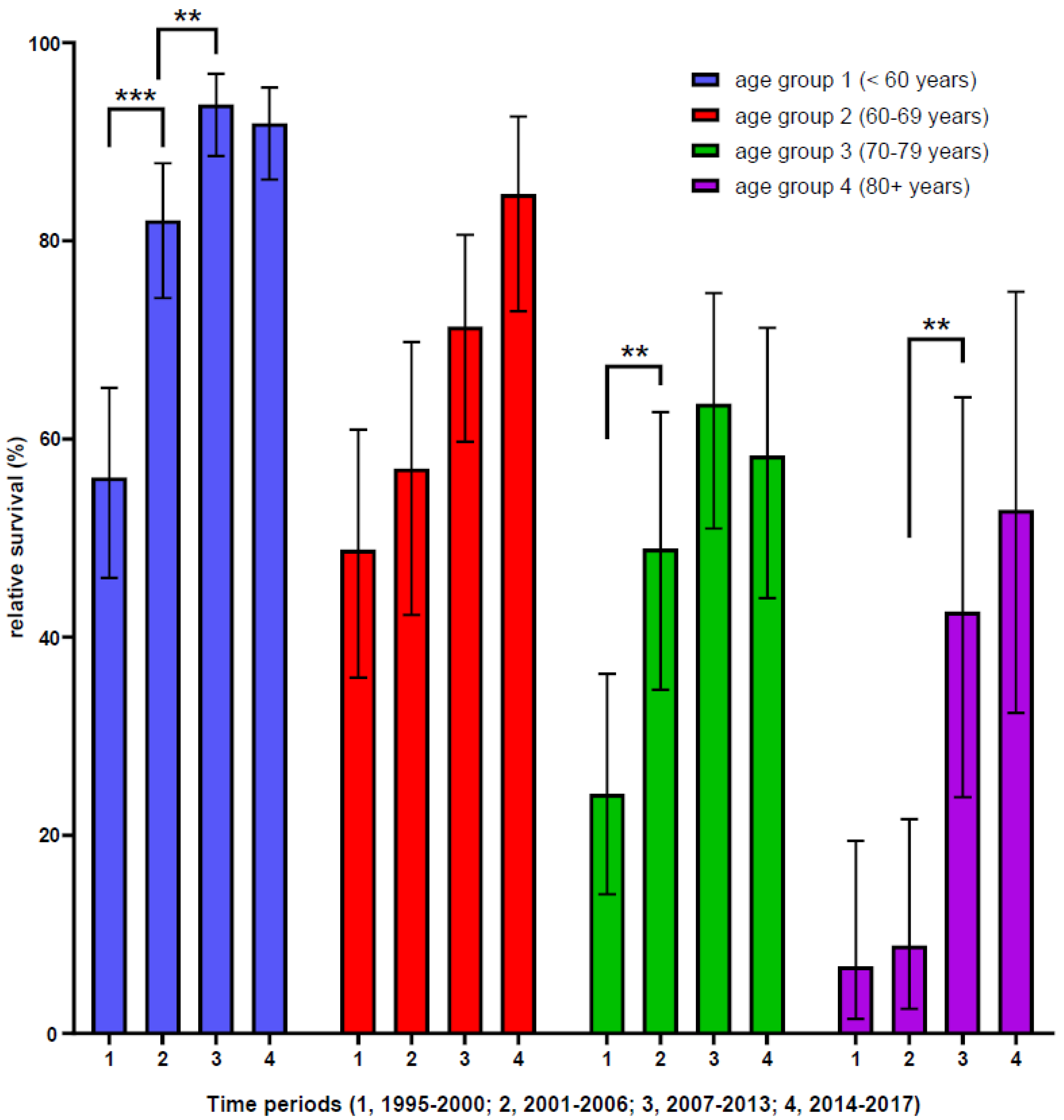
3.4. Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABL1 | Abelson murine leukemia gene 1 |
| ASR | age-standardized rates per 100,000 person years |
| BCR | breakpoint cluster region |
| CCR | cantonal cancer registry |
| CI | confidence interval |
| CML | chronic myeloid leukemia |
| CP-CML | chronic phase of CML |
| CIR | crude incidence rate |
| CR | crude rates per 100,000 person years |
| INF α | interferon alpha |
| IQR | interquartile range |
| NACR | National Agency for Cancer Registration |
| OS | overall survival |
| RS | relative survival |
| SFSO | Swiss Federal Statistical Office |
| Phi | Philadelphia chromosome |
| py | person years |
| t(9;22) | translocation chromosome 9 and 22 |
| TKI | tyrosine kinase inhibitor |
| yrs | years |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2017. CA A Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Wang, H.; Kantarjian, H.; Cortes, J. Trends in chronic myeloid leukemia incidence and survival in the United States from 1975 to 2009. Leuk. Lymphoma 2013, 54, 1411–1417. [Google Scholar] [CrossRef]
- Hoffmann, V.S.; Baccarani, M.; Hasford, J.; Lindoerfer, D.; Burgstaller, S.; Sertic, D.; Costeas, P.; Mayer, J.; Indrak, K.; Everaus, H.; et al. The EUTOS population-based registry: Incidence and clinical characteristics of 2904 CML patients in 20 European Countries. Leukemia 2015, 29, 1336–1343. [Google Scholar] [CrossRef]
- Roman, E.; Smith, A.; Appleton, S.; Crouch, S.; Kelly, R.; Kinsey, S.; Cargo, C.; Patmore, R. Myeloid malignancies in the real-world: Occurrence, progression and survival in the UK’s population-based Haematological Malignancy Research Network 2004-15. Cancer Epidemiol. 2016, 42, 186–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thielen, N.; Visser, O.; Ossenkoppele, G.; Janssen, J. Chronic myeloid leukemia in the Netherlands: A population-based study on incidence, treatment, and survival in 3585 patients from 1989 to 2012. Eur. J. Haematol. 2016, 97, 145–154. [Google Scholar] [CrossRef]
- Bjorkholm, M.; Ohm, L.; Eloranta, S.; Derolf, A.; Hultcrantz, M.; Sjoberg, J.; Andersson, T.; Hoglund, M.; Richter, J.; Landgren, O.; et al. Success story of targeted therapy in chronic myeloid leukemia: A population-based study of patients diagnosed in Sweden from 1973 to 2008. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 2514–2520. [Google Scholar] [CrossRef] [Green Version]
- Hoglund, M.; Sandin, F.; Simonsson, B. Epidemiology of chronic myeloid leukaemia: An update. Ann. Hematol. 2015, 94 (Suppl. 2), S241–S247. [Google Scholar] [CrossRef]
- Delord, M.; Foulon, S.; Cayuela, J.M.; Rousselot, P.; Bonastre, J. The rising prevalence of chronic myeloid leukemia in France. Leuk. Res. 2018, 69, 94–99. [Google Scholar] [CrossRef]
- Au, W.Y.; Caguioa, P.B.; Chuah, C.; Hsu, S.C.; Jootar, S.; Kim, D.W.; Kweon, I.Y.; O’Neil, W.M.; Saikia, T.K.; Wang, J. Chronic myeloid leukemia in Asia. Int. J. Hematol. 2009, 89, 14–23. [Google Scholar] [CrossRef]
- Jootar, S. CML treatment in Asia-Pacific region. Hematology 2012, 17 (Suppl. 1), S72–S74. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.L.; Preston, D.L.; Soda, M.; Sugiyama, H.; Funamoto, S.; Kodama, K.; Kimura, A.; Kamada, N.; Dohy, H.; Tomonaga, M.; et al. The incidence of leukemia, lymphoma and multiple myeloma among atomic bomb survivors: 1950–2001. Radiat. Res. 2013, 179, 361–382. [Google Scholar] [CrossRef] [Green Version]
- Kabat, G.C.; Wu, J.W.; Moore, S.C.; Morton, L.M.; Park, Y.; Hollenbeck, A.R.; Rohan, T.E. Lifestyle and dietary factors in relation to risk of chronic myeloid leukemia in the NIH-AARP Diet and Health Study. Cancer Epidemiol. Biomark. Prev. 2013, 22, 848–854. [Google Scholar] [CrossRef] [Green Version]
- Lauseker, M.; Hasford, J.; Saussele, S.; Kremers, S.; Kraemer, D.; Lindemann, W.; Hehlmann, R.; Pfirrmann, M. Smokers with chronic myeloid leukemia are at a higher risk of disease progression and premature death. Cancer 2017, 123, 2467–2471. [Google Scholar] [CrossRef]
- Van Maele-Fabry, G.; Duhayon, S.; Lison, D. A systematic review of myeloid leukemias and occupational pesticide exposure. Cancer Causes Control CCC 2007, 18, 457–478. [Google Scholar] [CrossRef]
- Apperley, J.F. Chronic myeloid leukaemia. Lancet 2015, 385, 1447–1459. [Google Scholar] [CrossRef]
- Jabbour, E.; Kantarjian, H. Chronic myeloid leukemia: 2020 update on diagnosis, therapy and monitoring. Am. J. Hematol. 2020, 95, 691–709. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.E.; Talpaz, M.; O’Brien, S.; Faderl, S.; Garcia-Manero, G.; Ferrajoli, A.; Verstovsek, S.; Rios, M.B.; Shan, J.; Kantarjian, H.M. Staging of chronic myeloid leukemia in the imatinib era: An evaluation of the World Health Organization proposal. Cancer 2006, 106, 1306–1315. [Google Scholar] [CrossRef]
- Conan-Doyle, A. Notes on a case of leucocythaemia. Lancet 1882, 119, 490. [Google Scholar] [CrossRef]
- Chronic granulocytic leukaemia: Comparison of radiotherapy and busulphan therapy. Report of the Medical Research Council’s working party for therapeutic trials in leukaemia. Br. Med. J. 1968, 1, 201–208. [CrossRef] [Green Version]
- Talpaz, M.; Kantarjian, H.M.; McCredie, K.; Trujillo, J.M.; Keating, M.J.; Gutterman, J.U. Hematologic remission and cytogenetic improvement induced by recombinant human interferon alpha A in chronic myelogenous leukemia. N. Engl. J. Med. 1986, 314, 1065–1069. [Google Scholar] [CrossRef]
- Hehlmann, R.; Heimpel, H.; Hasford, J.; Kolb, H.J.; Pralle, H.; Hossfeld, D.K.; Queisser, W.; Loffler, H.; Hochhaus, A.; Heinze, B.; et al. Randomized comparison of interferon-alpha with busulfan and hydroxyurea in chronic myelogenous leukemia. The German CML Study Group. Blood 1994, 84, 4064–4077. [Google Scholar] [CrossRef] [Green Version]
- Bonifazi, F.; de Vivo, A.; Rosti, G.; Guilhot, F.; Guilhot, J.; Trabacchi, E.; Hehlmann, R.; Hochhaus, A.; Shepherd, P.C.; Steegmann, J.L.; et al. Chronic myeloid leukemia and interferon-alpha: A study of complete cytogenetic responders. Blood 2001, 98, 3074–3081. [Google Scholar] [CrossRef]
- Goldman, J.M.; Baughan, A.S.; McCarthy, D.M.; Worsley, A.M.; Hows, J.M.; Gordon-Smith, E.C.; Catovsky, D.; Batchelor, J.R.; Goolden, A.W.; Galton, D.A. Marrow transplantation for patients in the chronic phase of chronic granulocytic leukaemia. Lancet 1982, 2, 623–625. [Google Scholar] [CrossRef]
- Pavlu, J.; Szydlo, R.M.; Goldman, J.M.; Apperley, J.F. Three decades of transplantation for chronic myeloid leukemia: What have we learned? Blood 2011, 117, 755–763. [Google Scholar] [CrossRef] [Green Version]
- Silver, R.T.; Woolf, S.H.; Hehlmann, R.; Appelbaum, F.R.; Anderson, J.; Bennett, C.; Goldman, J.M.; Guilhot, F.; Kantarjian, H.M.; Lichtin, A.E.; et al. An evidence-based analysis of the effect of busulfan, hydroxyurea, interferon, and allogeneic bone marrow transplantation in treating the chronic phase of chronic myeloid leukemia: Developed for the American Society of Hematology. Blood 1999, 94, 1517–1536. [Google Scholar] [PubMed]
- Hansen, J.A.; Gooley, T.A.; Martin, P.J.; Appelbaum, F.; Chauncey, T.R.; Clift, R.A.; Petersdorf, E.W.; Radich, J.; Sanders, J.E.; Storb, R.F.; et al. Bone marrow transplants from unrelated donors for patients with chronic myeloid leukemia. N. Engl. J. Med. 1998, 338, 962–968. [Google Scholar] [CrossRef] [PubMed]
- Dazzi, F.; Szydlo, R.M.; Cross, N.C.; Craddock, C.; Kaeda, J.; Kanfer, E.; Cwynarski, K.; Olavarria, E.; Yong, A.; Apperley, J.F.; et al. Durability of responses following donor lymphocyte infusions for patients who relapse after allogeneic stem cell transplantation for chronic myeloid leukemia. Blood 2000, 96, 2712–2716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raiola, A.M.; Van Lint, M.T.; Valbonesi, M.; Lamparelli, T.; Gualandi, F.; Occhini, D.; Bregante, S.; di Grazia, C.; Dominietto, A.; Soracco, M.; et al. Factors predicting response and graft-versus-host disease after donor lymphocyte infusions: A study on 593 infusions. Bone Marrow Transplant. 2003, 31, 687–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantarjian, H.; O’Brien, S.; Jabbour, E.; Garcia-Manero, G.; Quintas-Cardama, A.; Shan, J.; Rios, M.B.; Ravandi, F.; Faderl, S.; Kadia, T.; et al. Improved survival in chronic myeloid leukemia since the introduction of imatinib therapy: A single-institution historical experience. Blood 2012, 119, 1981–1987. [Google Scholar] [CrossRef]
- Stomper, J.; Rotondo, J.C.; Greve, G.; Lübbert, M. Hypomethylating agents (HMA) for the treatment of acute myeloid leukemia and myelodysplastic syndromes: Mechanisms of resistance and novel HMA-based therapies. Leukemia 2021, 35, 1873–1889. [Google Scholar] [CrossRef] [PubMed]
- Saxena, K.; Jabbour, E.; Issa, G.; Sasaki, K.; Ravandi, F.; Maiti, A.; Daver, N.; Kadia, T.; DiNardo, C.D.; Konopleva, M.; et al. Impact of frontline treatment approach on outcomes of myeloid blast phase CML. J. Hematol. Oncol. 2021, 14, 94. [Google Scholar] [CrossRef]
- Radich, J.P.; Deininger, M.; Abboud, C.N.; Altman, J.K.; Berman, E.; Bhatia, R.; Bhatnagar, B.; Curtin, P.; DeAngelo, D.J.; Gotlib, J.; et al. Chronic Myeloid Leukemia, Version 1.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2018, 16, 1108–1135. [Google Scholar] [CrossRef]
- Hochhaus, A.; Baccarani, M.; Silver, R.T.; Schiffer, C.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Deininger, M.W.; Guilhot, F.; et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia 2020, 34, 966–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baccarani, M.; Deininger, M.W.; Rosti, G.; Hochhaus, A.; Soverini, S.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Guilhot, F.; et al. European LeukemiaNet recommendations for the management of chronic myeloid leukemia: 2013. Blood 2013, 122, 872–884. [Google Scholar] [CrossRef] [PubMed]
- Hochhaus, A.; Saussele, S.; Rosti, G.; Mahon, F.X.; Janssen, J.; Hjorth-Hansen, H.; Richter, J.; Buske, C. Chronic myeloid leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, iv41–iv51. [Google Scholar] [CrossRef]
- Bower, H.; Bjorkholm, M.; Dickman, P.W.; Hoglund, M.; Lambert, P.C.; Andersson, T.M. Life Expectancy of Patients With Chronic Myeloid Leukemia Approaches the Life Expectancy of the General Population. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 2851–2857. [Google Scholar] [CrossRef] [Green Version]
- Crugnola, M.; Castagnetti, F.; Breccia, M.; Ferrero, D.; Trawinska, M.M.; Abruzzese, E.; Annunziata, M.; Stagno, F.; Tiribelli, M.; Binotto, G.; et al. Outcome of very elderly chronic myeloid leukaemia patients treated with imatinib frontline. Ann. Hematol. 2019, 98, 2329–2338. [Google Scholar] [CrossRef]
- Lauseker, M.; Gerlach, R.; Worseg, W.; Haferlach, T.; Tauscher, M.; Hasford, J.; Hoffmann, V.S. Differences in treatment and monitoring of chronic myeloid leukemia with regard to age, but not sex: Results from a population-based study. Eur. J. Haematol. 2019, 103, 362–369. [Google Scholar] [CrossRef] [Green Version]
- Seo, H.Y.; Ko, T.H.; Hyun, S.Y.; Song, H.; Lim, S.T.; Shim, K.Y.; Lee, J.I.; Kong, J.H. Tyrosine Kinase Inhibitor Dosing Patterns in Elderly Patients With Chronic Myeloid Leukemia. Clin. Lymphoma Myeloma Leuk. 2019, 19, 735–743.e732. [Google Scholar] [CrossRef] [PubMed]
- Lokesh, K.N.; Pehalajani, J.K.; Loknatha, D.; Jacob, L.A.; Babu, M.C.S.; Rudresha, A.H.; Rajeev, L.K.; Smitha, S.C.; Ashok, K.P.; Madhumathi, D.S. CML in Elderly: Does Age Matter? Indian J. Hematol. Blood Transfus. Off. J. Indian Soc. Hematol. Blood Transfus. 2020, 36, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Arndt, V.; NICER Working Group. Population-based cancer registration and research in Switzerland: Examples, limitations and perspectives. Swiss Cancer Bull. 2016, 2, 163–167. [Google Scholar]
- Noseda, G. The future of cancer registration in Switzerland. Swiss Cancer Bull 2018, 38, 315–316. [Google Scholar]
- Classification of Diseases (ICD-10). Available online: https://www.who.int/classifications/icd/icdonlineversions/en/ (accessed on 12 December 2018).
- Waterhouse, J.; Muir, C.; Correa, P.; Powell, J. Cancer Incidence in Five Continents; International Agency for Research on Cancer: Lyon, France, 1976; Volume 3, p. 456. [Google Scholar]
- Dickman, P.W.; Coviello, E.; Hills, M. Estimating and modeling relative survival. Stata J. 2015, 15, 186–215. [Google Scholar] [CrossRef] [Green Version]
- Corazziari, I.; Quinn, M.; Capocaccia, R. Standard cancer patient population for age standardising survival ratios. Eur. J. Cancer 2004, 40, 2307–2316. [Google Scholar] [CrossRef]
- Parkin, D.; Hakulinen, T. Analysis of Survival. In Cancer Registration: Principles and Methods; International Agency for Research on Cancer (IACR): Lyon, France, 1991; pp. 159–176. [Google Scholar]
- Beinortas, T.; Tavoriene, I.; Zvirblis, T.; Gerbutavicius, R.; Jurgutis, M.; Griskevicius, L. Chronic myeloid leukemia incidence, survival and accessibility of tyrosine kinase inhibitors: A report from population-based Lithuanian haematological disease registry 2000-2013. BMC Cancer 2016, 16, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dikshit, R.P.; Nagrani, R.; Yeole, B.; Koyande, S.; Banawali, S. Changing trends of chronic myeloid leukemia in greater Mumbai, India over a period of 30 years. Indian J. Med. Paediatr. Oncol. 2011, 32, 96–100. [Google Scholar] [CrossRef] [Green Version]
- Kulikov, S.M.; Vinogradova, O.; Chelysheva, E.; Tishchenko, I.A.; Galaiko, M.A.; Lazareva, O.V.; Senderova, O.M.; Pepeliaeva, V.M.; Meresii, S.V.; Luchinin, A.S.; et al. Incidence of chronic myeloid leukemia in 6 regions of Russia according to the data of the 2009-2012 population-based study. Ter. Arkhiv. 2014, 86, 24–30. [Google Scholar]
- Nguyen, L.T.; Guo, M.; Naugler, C.; Rashid-Kolvear, F. Incidence of chronic myeloid leukemia in Calgary, Alberta, Canada. BMC Res. Notes 2018, 11, 780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.W.; Banavali, S.D.; Bunworasate, U.; Goh, Y.T.; Ganly, P.; Huang, H.; Irving, I.; Jootar, S.; Goh, H.G.; Koh, L.P.; et al. Chronic myeloid leukemia in the Asia-Pacific region: Current practice, challenges and opportunities in the targeted therapy era. Leuk. Res. 2010, 34, 1459–1471. [Google Scholar] [CrossRef]
- Chang, C.S.; Lee, K.; Yang, Y.H.; Lin, M.T.; Hsu, C.N. Estimation of CML incidence: Disagreement between national cancer registry and health claims data system in Taiwan. Leuk. Res. 2011, 35, e53–e54. [Google Scholar] [CrossRef]
- Ning, L.; Hu, C.; Lu, P.; Que, Y.; Zhu, X.; Li, D. Trends in disease burden of chronic myeloid leukemia at the global, regional, and national levels: A population-based epidemiologic study. Exp. Hematol. Oncol. 2020, 9, 29. [Google Scholar] [CrossRef]
- Lin, Q.; Mao, L.; Shao, L.; Zhu, L.; Han, Q.; Zhu, H.; Jin, J.; You, L. Global, Regional, and National Burden of Chronic Myeloid Leukemia, 1990-2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Front. Oncol. 2020, 10, 580759. [Google Scholar] [CrossRef]
- Kantarjian, H.M.; O’Brien, S.; Cortes, J.E.; Shan, J.; Giles, F.J.; Rios, M.B.; Faderl, S.H.; Wierda, W.G.; Ferrajoli, A.; Verstovsek, S.; et al. Complete cytogenetic and molecular responses to interferon-alpha-based therapy for chronic myelogenous leukemia are associated with excellent long-term prognosis. Cancer 2003, 97, 1033–1041. [Google Scholar] [CrossRef]
- Hoglund, M.; Sandin, F.; Hellstrom, K.; Bjoreman, M.; Bjorkholm, M.; Brune, M.; Dreimane, A.; Ekblom, M.; Lehmann, S.; Ljungman, P.; et al. Tyrosine kinase inhibitor usage, treatment outcome, and prognostic scores in CML: Report from the population-based Swedish CML registry. Blood 2013, 122, 1284–1292. [Google Scholar] [CrossRef]
- Hoffmann, V.S.; Baccarani, M.; Hasford, J.; Castagnetti, F.; Di Raimondo, F.; Casado, L.F.; Turkina, A.; Zackova, D.; Ossenkoppele, G.; Zaritskey, A.; et al. Treatment and outcome of 2904 CML patients from the EUTOS population-based registry. Leukemia 2017, 31, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Hehlmann, R.; Lauseker, M.; Saussele, S.; Pfirrmann, M.; Krause, S.; Kolb, H.J.; Neubauer, A.; Hossfeld, D.K.; Nerl, C.; Gratwohl, A.; et al. Assessment of imatinib as first-line treatment of chronic myeloid leukemia: 10-year survival results of the randomized CML study IV and impact of non-CML determinants. Leukemia 2017, 31, 2398–2406. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Strom, S.S.; O’Brien, S.; Jabbour, E.; Ravandi, F.; Konopleva, M.; Borthakur, G.; Pemmaraju, N.; Daver, N.; Jain, P.; et al. Relative survival in patients with chronic-phase chronic myeloid leukaemia in the tyrosine-kinase inhibitor era: Analysis of patient data from six prospective clinical trials. Lancet Haematol. 2015, 2, e186–e193. [Google Scholar] [CrossRef] [Green Version]
- Saussele, S.; Krauss, M.P.; Hehlmann, R.; Lauseker, M.; Proetel, U.; Kalmanti, L.; Hanfstein, B.; Fabarius, A.; Kraemer, D.; Berdel, W.E.; et al. Impact of comorbidities on overall survival in patients with chronic myeloid leukemia: Results of the randomized CML study IV. Blood 2015, 126, 42–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penot, A.; Preux, P.M.; Le Guyader, S.; Collignon, A.; Herry, A.; Dufour, V.; Monnereau, A.; Woronoff, A.S.; Troussard, X.; Pons, E.; et al. Incidence of chronic myeloid leukemia and patient survival: Results of five French population-based cancer registries 1980-2009. Leuk. Lymphoma 2015, 56, 1771–1777. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.G.; Painter, D.; Howell, D.A.; Evans, P.; Smith, G.; Patmore, R.; Jack, A.; Roman, E. Determinants of survival in patients with chronic myeloid leukaemia treated in the new era of oral therapy: Findings from a UK population-based patient cohort. BMJ Open 2014, 4, e004266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunnarsson, N.; Sandin, F.; Hoglund, M.; Stenke, L.; Bjorkholm, M.; Lambe, M.; Olsson-Stromberg, U.; Richter, J.; Sjalander, A. Population-based assessment of chronic myeloid leukemia in Sweden: Striking increase in survival and prevalence. Eur. J. Haematol. 2016, 97, 387–392. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variation | 1995–2000 | 2001–2006 | 2007–2012 | 2013–2017 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % * | MedianAge (IQR) | n | % * | Median Age (IQR) | n | % * | Median Age (IQR) | n | % * | Median Age (IQR) | |
| Males | 186 | 57.6 | 59.5 (41–73) | 210 | 54.6 | 64.5 (46–76) | 227 | 58.2 | 66 (47–77) | 268 | 59.0 | 61 (48.5–72) |
| <60 years | 93 | 50.0 | 85 | 40.5 | 88 | 38.8 | 129 | 48.1 | ||||
| 60–69 years | 25 | 13.4 | 35 | 16.7 | 42 | 18.5 | 54 | 20.2 | ||||
| 70–79 years | 40 | 21.5 | 54 | 25.7 | 55 | 24.2 | 54 | 20.2 | ||||
| 80+ years | 28 | 15.1 | 36 | 17.1 | 42 | 18.5 | 31 | 11.6 | ||||
| Females | 137 | 42.4 | 65 (50–80) | 175 | 45.5 | 67 (53–79) | 163 | 41.8 | 64 (47–76) | 186 | 41.0 | 63 (50–78) |
| <60 years | 51 | 37.2 | 61 | 34.9 | 65 | 39.9 | 81 | 43.6 | ||||
| 60–69 years | 27 | 19.7 | 38 | 21.7 | 41 | 25.2 | 34 | 18.3 | ||||
| 70–79 years | 22 | 16.1 | 34 | 19.4 | 32 | 19.6 | 31 | 16.7 | ||||
| 80+ years | 37 | 27.0 | 42 | 24.0 | 25 | 15.3 | 40 | 21.5 | ||||
| Total | 323 | 100.0 | 63 (45–77) | 385 | 100.0 | 66 (49–77) | 390 | 100.0 | 65 (47–77) | 454 | 100.0 | 61.5 (49–74) |
| <60 years | 144 | 44.6 | 146 | 37.9 | 153 | 39.2 | 210 | 46.3 | ||||
| 60–69 years | 52 | 16.1 | 73 | 19.0 | 83 | 21.3 | 88 | 19.4 | ||||
| 70–79 years | 62 | 19.2 | 88 | 22.9 | 87 | 22.3 | 85 | 18.7 | ||||
| 80+ years | 65 | 20.1 | 78 | 20.3 | 67 | 17.2 | 71 | 15.6 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daskalakis, M.; Feller, A.; Noetzli, J.; Bonadies, N.; Arndt, V.; Baerlocher, G.M.; The NICER Working Group. Potential to Improve Therapy of Chronic Myeloid Leukemia (CML), Especially for Patients with Older Age: Incidence, Mortality, and Survival Rates of Patients with CML in Switzerland from 1995 to 2017. Cancers 2021, 13, 6269. https://doi.org/10.3390/cancers13246269
Daskalakis M, Feller A, Noetzli J, Bonadies N, Arndt V, Baerlocher GM, The NICER Working Group. Potential to Improve Therapy of Chronic Myeloid Leukemia (CML), Especially for Patients with Older Age: Incidence, Mortality, and Survival Rates of Patients with CML in Switzerland from 1995 to 2017. Cancers. 2021; 13(24):6269. https://doi.org/10.3390/cancers13246269
Chicago/Turabian StyleDaskalakis, Michael, Anita Feller, Jasmine Noetzli, Nicolas Bonadies, Volker Arndt, Gabriela Maria Baerlocher, and The NICER Working Group. 2021. "Potential to Improve Therapy of Chronic Myeloid Leukemia (CML), Especially for Patients with Older Age: Incidence, Mortality, and Survival Rates of Patients with CML in Switzerland from 1995 to 2017" Cancers 13, no. 24: 6269. https://doi.org/10.3390/cancers13246269