
Circulating Tumor Cells Enumeration from the Portal Vein for Risk Stratification in Early Pancreatic Cancer Patients

 , , , , , , , , , , , and
, , , , , , , , , , , and
Abstract
:Simple Summary
Abstract
- CTCs can be detected in the early stages of pancreatic cancer.
- CTC inside a cluster is much higher in G3 than in G1–2 in both samples.
- The larger the size of the tumor, the greater the number of total CTC for PV and CVC samples.
- The number of CTC < 185 in PV (HR = 4.464; p = 0.016) and no vascular invasion (HR: 3.663; p = 0.013) were independent predictors of better long-term survival.
1. Introduction
2. Material and Methods
2.1. Study Design and Sample Collection
2.2. Validation of CTC Detection
2.3. CTC Isolation, Detection, and Enumeration
2.4. Statistical Analysis
3. Results
3.1. Validation of CTC Detection
3.2. Longitudinal Enumeration and Cluster Evaluation
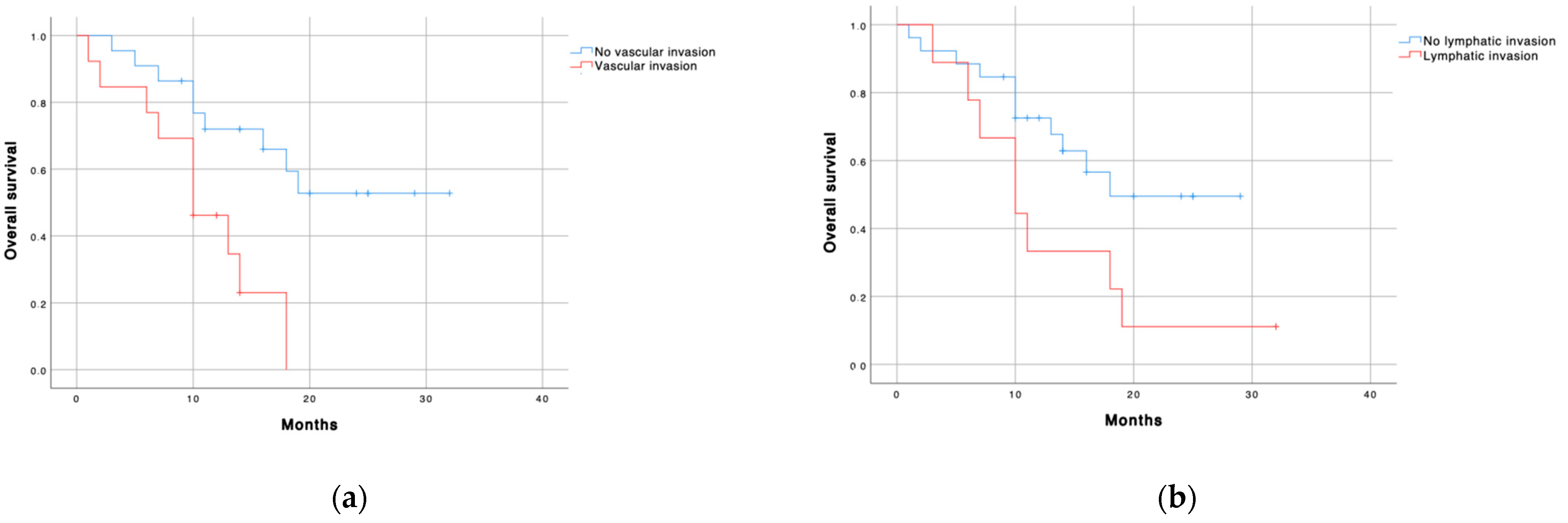
3.3. Prognostic Factors for Long-Term Survival
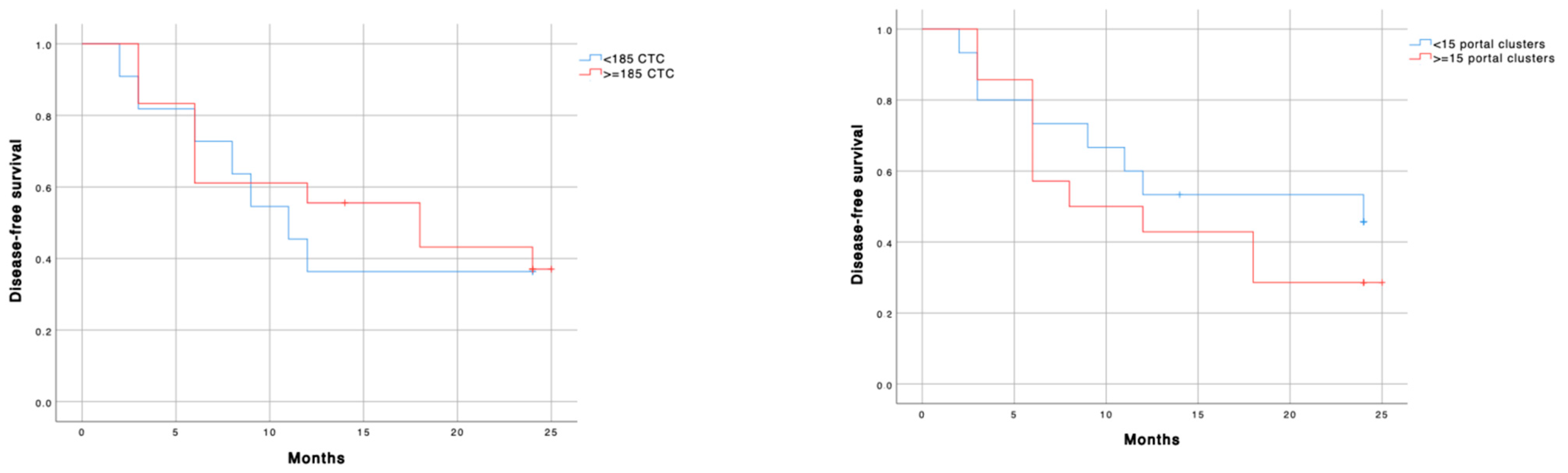
3.4. Prognostic Factors for Long Term Local and Systemic Progression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garrido-Laguna, I.; Hidalgo, M. Pancreatic cancer: From state-of-the-art treatments to promising novel therapies. Nat. Rev. Clin. Oncol. 2015, 12, 319–334. [Google Scholar] [CrossRef] [PubMed]
- Álamo, J.M.; Marín, L.M.; Suárez, G.; Bernal, C.; Serrano, J.; Barrera, L.; Gómez, M.A.; Muntané, J.; Padillo-Ruiz, J. Improving outcomes in pancreatic cancer: Key points in perioperative management. World J. Gastroenterol. 2014, 20, 14237–14245. [Google Scholar] [CrossRef] [PubMed]
- Sabater, L.; Cugat, E.; Serrablo, A.; Suarez, G.; Padillo, J. Does the artery-first approach improve the rate of r0 resection in pancreatoduodenectomy? A multicenter, randomized, controlled trial. Ann. Surg. 2019, 270, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Groot-Koerkamp, B.; Rahbari, N.N.; Buchler, M.W.; Koch, M.; Weitz, J. Circulating tumor cells and prognosis of patients with resectable colorectal liver metastases or widespread metastatic colorectal cancer: A meta-analysis. Ann. Surg. Oncol. 2013, 20, 2156–2165. [Google Scholar] [CrossRef]
- Micalizzi, D.S.; Maheswaran, S.; Haber, D.A. A conduit to metastasis: Circulating tumor cell biology. Genes Dev. 2017, 31, 1827–1840. [Google Scholar] [CrossRef]
- Jiao, L.R.; Apostolopoulos, C.; Jacob, J.; Szydlo, R.; Johnson, N.; Tsim, N.; Habib, N.A.; Coombes, R.C.; Stebbing, J. Unique Localization of Circulating Tumor Cells in Patients with Hepatic Metastases. J. Clin. Oncol. 2009, 27, 6160–6165. [Google Scholar] [CrossRef]
- Tien, Y.W.; Kuo, H.C.; Ho, B.I.; Chang, M.C.; Chang, Y.T.; Cheng, M.; Chen, H.L.; Liang, T.Y.; Wang, C.F.; Huang, C.Y.; et al. High Circulating Tumor Cell count in portal vein predicts liver metastasis from periampullary or pancreatic cancer. Medicine 2016, 95, e3407. [Google Scholar] [CrossRef]
- Liu, X.; Li, C.; Li, J.; Yu, T.; Zhou, G.; Cheng, J.; Li, G.; Zhou, Y.; Lou, W.; Wang, X.; et al. Detection of CTC in portal vein was associated with intrahepatic metastases and prognosis in patients with advanced pancreatic cancer. J. Cancer 2018, 9, 2038–2045. [Google Scholar] [CrossRef]
- Seufferlein, T.; Mayerle, J. Pancreatic cancer in 2015: Precision medicine in pancreatic cancer-fact or fiction? Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 74–75. [Google Scholar] [CrossRef]
- Song, B.G.; Kwon, W.; Kim, H.; Lee, E.M.; Han, Y.M.; Kim, H.; Byun, Y.; Lee, K.B.; Lee, K.H.; Lee, K.T.; et al. Detection of Circulating Tumor Cells in Resectable Pancreatic Ductal Adenocarcinoma: A Prospective Evaluation as a Prognostic Marker. Front. Oncol. 2021, 10, 616440. [Google Scholar] [CrossRef]
- Adsay, N.V.; Basturk, O.; Saka, B.; Bagci, P.; Ozdemir, D.; Balci, S.; Sarmiento, J.M.; Kooby, D.A.; Staley, C.; Maithel, S.K.; et al. Whipple made simple for surgical pathologists: Orientation, dissection, and sampling of pancreaticoduodenectomy specimens for a more practical and accurate evaluation of pancreatic, distal common bile duct, and ampullary tumors. Am. J. Surg. Pathol. 2014, 38, 480–493. [Google Scholar] [CrossRef] [Green Version]
- Verbeke, C.S.; Gladhaug, I.P. Resection margin involvement and tumor origin in pancreatic head cancer. Br. J. Surg. 2012, 99, 1036–1049. [Google Scholar] [CrossRef]
- Agerbæk, M.Ø.; Bang-Christensen, S.R.; Yang, M.H.; Clausen, T.M.; Pereira, M.A.; Sharma, S.; Ditlev, S.B.; Nielsen, M.A.; Choudhary, S.; Gustavsson, T.; et al. The VAR2CSA malaria protein efficiently retrieves circulating tumor cells in an EpCAM-independent manner. Nat. Commun. 2018, 9, 3279. [Google Scholar] [CrossRef] [Green Version]
- Calero-Castro, F.J.; Pereira, S.; Villanueva, P.; de la Cruz-Ojeda, P.; Navarro-Villarán, E.; Suarez Artacho, G.; Tinoco-González, J.; Cepeda-Franco, C.; Borrero, J.J.; Dios Barbeito, S.; et al. The use of the Hough´s transform algorithm to count Circulating Tumor Cells from patients with pancreatic cancer. Cancers 2021, in press. [Google Scholar]
- Mukaka, M.M. Statistics Corner: A guide to appropriate use of Correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar]
- Altman, D.G.; Lausen, B.; Sauerbrei, W.; Schumacher, M. Dangers of using "optimal" cutpoints in the evaluation of prognostic factors. J. Natl. Cancer Inst. 1994, 86, 829–835. [Google Scholar] [CrossRef] [Green Version]
- Arnolettia, J.P.; Fanaianb, N.; Rezac, J.; Sausea, N.; Almodovara, A.J.; Srivastavaa, M.; Pateld, S.; Veldhuisd, P.P.; Griffitha, E.; Shaoa, Y.P.; et al. Pancreatic and bile duct cancer circulating tumor cells (CTC) form immune-resistant multi-cell type clusters in the portal venous circulation. Cancer Biol. Ther. 2018, 19, 887–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bausch, D.; Thomas, S.; Mino-Kenudson, M.; Fernandez-del, C.C.; Bauer, T.W.; Williams, M.; Warshaw, A.L.; Thayer, S.P.; Kelly, K.A. Plectin-1 as a novel biomarker for pancreatic cancer. Clin. Cancer Res. 2011, 17, 302–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barriere, G.; Fici, P.; Gallerani, G.; Fabbri, F.; Zoli, W.; Rigaud, M. Circulating tumor cells and epithelial, mesenchymal and stemness markers: Characterization of cell subpopulations. Ann. Transl. Med. 2014, 2, 109. [Google Scholar] [PubMed]
- Malapelle, U.; Pisapia, P.; Addeo, A.; Arrieta, O.; Bellosillo, B.; Cardona, A.F.; Cristofanilli, M.; de Miguel-Perez, D.; Denninghoff, V.; Durán, I.; et al. Liquid Biopsy from research to clinical practice: Focus on Non-Small Cell Lung Cancer. Expert Rev. Mol. Diagn. 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Hugenschmidt, H.; Labori, K., Jr.; Borgen, E.; Brunborg, C.; Schirmer, C.B.; Seeberg, L.T.; Naume, B.R.; Wiedswang, G. Preoperative ctc-detection by cellsearch® is associated with early distant metastasis and impaired survival in resected pancreatic cancer. Cancers 2021, 13, 485. [Google Scholar] [CrossRef]
- White, M.G.; Lee, A.; Vicente, D.; Hall, C.; Kim, M.P.; Katz, M.H.G.; Lee, J.E.; Ikoma, N.; Lucci, A.; Tzeng, C.W. Measurement of portal vein blood circulating tumor cells is safe and may correlate with outcomes in resected pancreatic ductal adenocarcinoma. Ann. Surg. Oncol. 2021, 28, 4615–4622. [Google Scholar] [CrossRef]
- Buscail, E.; Alix-Panabières, C.; Quincy, P.; Cauvin, T.; Chauvet, A.; Degrandi, O.; Caumont, C.; Verdon, S.; Lamrissi, I.; Moranvillier, I.; et al. High clinical value of liquid biopsy to detect circulating tumor cells and tumor exosomes in pancreatic ductal adenocarcinoma patients eligible for up-front surgery. Cancers 2019, 11, 1656. [Google Scholar] [CrossRef] [Green Version]
- Aceto, N.; Bardia, A.; Miyamoto, D.T.; Donaldson, M.C.; Wittner, B.S.; Spencer, J.A.; Yu, M.; Pely, A.; Engstrom, A.; Zhu, H.; et al. Circulating tumor cell clusters are oligoclonal precursors of breast cancer metastasis. Cell 2014, 158, 1110–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fabisiewicz, A.; Grzybowska, E. CTC clusters in cancer progression and metastasis. Med. Oncol. 2017, 34, 1–10. [Google Scholar] [CrossRef]
- Catenacci, D.V.; Chapman, C.G.; Xu, P.; Koons, A.; Konda, V.J.; Siddiqui, U.D.; Waxman, I. Acquisition of portal venous circulating tumor cells from patients with pancreaticobiliary cancers by endoscopic ultrasound. Gastroenterology 2015, 149, 1794–1803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cauley, C.E.; Pitman, M.B.; Zhou, J.; Perkins, J.; Kuleman, B.; Liss, A.S.; Fernandez-Del Castillo, C.; Warshaw, A.L.; Lillemoe, K.D.; Thayer, S.P. circulating epithelial cells in patients with pancreatic lesions: Clinical and pathologic findings. J. Am. Coll. Surg. 2015, 221, 699–707. [Google Scholar] [CrossRef] [Green Version]
- Kulemann, B.; Pitman, M.B.; Liss, A.S.; Valsangkar, N.; Fernandez-Del Castillo, C.; Lillemoe, K.D.; Hoeppner, J.; Kenudson, M.M.; Warshaw, A.L.; Thayer, S.P.; et al. Circulating tumor cells found in patients with localized and advanced pancreatic cancer. Pancreas 2015, 44, 547–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoja, L.; Backen, A.; Sloane, R.; Menasce, L.; Ryder, D.; Krebs, M.; Board, R.; Clack, G.; Hughes, A.; Blackhall, F.; et al. A pilot study to explore circulating tumor cells in pancreatic cancer as a novel biomarker. Br. J. Cancer 2012, 106, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Jakel, C.; Bergmann, F.; Toth, R.; Assenov, Y.; van der Duin, D.; Strobel, O.; Hank, T.; Klöppel, G.; Dorrell, C.; Grompe, M.; et al. Genome-wide genetic and epigenetic analyses of pancreatic acinar cell carcinomas reveal aberrations in genome stability. Nat. Commun. 2017, 8, 1323. [Google Scholar] [CrossRef]
- Okubo, K.; Uenosono, Y.; Arigami, T.; Mataki, Y.; Matsushita, D.; Yanagita, S.; Kurahara, H.; Sakoda, M.; Kijima, Y.; Maemura, K.; et al. Clinical impact of circulating tumor cells and therapy response in pancreatic cancer. Eur. J. Surg. Oncol. 2017, 43, 1050–1055. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research Variable | PV (Median, Range) | CVC (Median, Range) | U-Mann Whitney p-Value | Correlation | Correlation p-Value |
|---|---|---|---|---|---|
| Free CTC (cell/mL) | 235.4 (101.3–375.3) | 291.8 (120.0–500.0) | 0.151 | 0.6 | 0.004 |
| Cluster/mL | 12.9 (4.8–33.0) | 14.5 (3.8–35.5) | 0.622 | 0.6 | 0.001 |
| CTC inside a cluster | 30.4 (12.5–89.4) | 37.4 (11.3–89.5) | 0.205 | 0.5 | 0.008 |
| Total CTC (cell/mL) | 310.0 (132.1–446.0) | 405.7 (130.7–553.8) | 0.239 | 0.6 | 0.001 |
| Ratio Free CTC/CTC inside a cluster | 2.6 (2.4–3.0) | 2.5 (2.3–2.9) | 0.051 | 0.2 | 0.306 |
| Free CTC median size | 7.5 (6.8–8.7) | 7.8 (6.7–9.0) | 0.981 | 0.3 | 0.229 |
| CTC inside a cluster median size | 10.2 (8.5–11.6) | 10.3 (8.6–11.7) | 0.990 | 0.3 | 0.074 |
| Research Variable | G1–G2 | G3 | p-Value |
|---|---|---|---|
| Free CTC (cell/mL) | 279.2 (120.3–482.3) | 357.0 (182.5–1020.8) | 0.483 |
| Cluster/mL | 14.0 (3.3–31.7) | 41.0 (17.9–46.8) | 0.107 |
| CTC inside a cluster | 36.7 (8.7–73.7) | 97.3 (54.5–116.3) | 0.071 |
| Total CTC (cell/mL) | 399.0 (129.0–538.5) | 481.0 (243.0–1117.7) | 0.318 |
| Ratio Free CTC/CTC inside a cluster | 2.6 (2.4–2.9) | 2.4 (2.2–3.1) | 0.483 |
| Free CTC median size | 7.8 (6.6–9.1) | 8.6 (6.7–10.2) | 0.521 |
| CTC inside a cluster median size | 10.3 (8.7–11.6) | 10.6 (7.8–13.2) | 0.908 |
| Research Variable | G1–G2 | G3 | p-Value |
|---|---|---|---|
| Free CTC (cell/mL) | 240.3 (102.2–373.3) | 227.0 (140.8–559.0) | 0.841 |
| Cluster/mL | 10.5 (4.3–32.7) | 7.5 (30.0–80.3) | 0.310 |
| CTC inside a cluster | 29.7 (9.2–74.2) | 78.5 (21.3–260.6) | 0.201 |
| Total CTC (cell/mL) | 314.5 (133.0–406.7) | 305.5 (162.1–819.6) | 0.725 |
| Ratio Free CTC/CTC inside a cluster | 2.6 (2.3–2.9) | 2.8 (2.6–3.9) | 0.150 |
| Free CTC median size | 7.3 (6.5–8.5) | 8.5 (7.0–9.6) | 0.310 |
| CTC inside a cluster median size | 9.7 (8.1–11.5) | 10.2 (9.5–12.4) | 0.335 |
| Research Variable | CA 19-9 (Rho) | Tumor Size * (cm) (Rho) |
|---|---|---|
| Free CTC (cell/mL) | 0.5 | 0.1 |
| Cluster/mL | 0.2 | −0.1 |
| CTC inside a cluster | 0.2 | −0.1 |
| Total CTC (cell/mL) | 0.4 | 0.4 |
| Ratio Free CTC/CTC inside a cluster | −0.3 | −0.3 |
| Free CTC median size | −0.5 | −0.1 |
| CTC inside a cluster median size | −0.6 | −0.6 |
| Research Variable | CA 19-9 (Rho) | Tumor Size * (cm) (Rho) |
|---|---|---|
| Free CTC (cell/mL) | 0.4 | 0.3 |
| Cluster/mL | 0.3 | 0.3 |
| CTC inside a cluster | 0.3 | −0.1 |
| Total CTC (cell/mL) | 0.4 | 0.4 |
| Ratio Free CTC/CTC inside a cluster | 0 | 0 |
| Free CTC median size | −0.1 | −0.1 |
| CTC inside a cluster median size | −0.2 | 0 |
| Research Variable | Free CTC (Cell/mL) | p-Value | Cluster/mL | p-Value | Total CTC (Cell/mL) | p-Value |
|---|---|---|---|---|---|---|
| Vascular invasion | 304.9 (151.6–656.4) | 0.662 | 12.1 (3.1–29.5) | 0.368 | 421.8 (162.7–697.9) | 0.692 |
| No vascular invasion | 291.8 (116.1–480.9) | 26.6 (4.3–41.0) | 384.4 (123.3–522.5) | |||
| Lymphatic invasion | 304.9 (79.1–455.7) | 0.504 | 31.1 (2.7–42.6) | 0.565 | 421.8 (87.8–501.6) | 0.629 |
| No lymphatic invasion | 291.8 (133.1–582.6) | 13.3 (3.8–31.0) | 384.4 (161.0–627.4) | |||
| Neural invasion | 350.5 (84.9–498.5) | 0.728 | 13.4 (2.7–42.1) | 0.667 | 443.1 (86.8–537.7) | 0.728 |
| No neural invasion | 275.8 (164.5–625.3) | 14.5 (10.5–32.8) | 384.4 (198.2–668.0) |
| Research Variable | Free CTC (Cell/mL) | p-Value | Cluster/mL | p-Value | Total CTC (Cell/mL) | p-Value |
|---|---|---|---|---|---|---|
| Vascular invasion | 321.7 (217.4–451.3) | 0.104 | 16.3 (5.5–41.5) | 0.362 | 374.2 (271.0–508.7) | 0.089 |
| No vascular invasion | 184.5 (97.2–322.3) | 12.3 (3.2–29.9) | 247.2 (125.4–401.0) | |||
| Lymphatic invasion | 204.7 (74.0–514.3) | 0.489 | 23.8 (5.8–52-5) | 0.397 | 350.5 (88.9–635.6) | 0.939 |
| No lymphatic invasion | 248.2 (118.2–377.3) | 12.3 (4.3–31.3) | 305.5 (138.2–419.2) | |||
| Neural invasion | 247.3 (94.3–375.3) | 0.905 | 13.8 (5.5–34.5) | 0.528 | 327.3 (120.6–492.4) | 0.798 |
| No neural invasion | 222.5 (113.0–370.8) | 10.3 (3.1–32.2) | 285.2 (141.1–404.7) |
| Research Variable | Deaths N (%) | Median Survival | 95% CI | Log-Rank-Value |
|---|---|---|---|---|
| <185 portal CTC | 5 (38.5) | 24.5 | 19.6–29.4 | 0.018 |
| ≥185 portal CTC | 14 (63.6) | 10.0 | 7.4–12.5 | |
| <15 portal clusters | 8 (42.1) | 19.0 | 15.8–22.2 | 0.040 |
| ≥15 portal clusters | 11 (68.8) | 10.0 | 7.2–12.8 | |
| No vascular invasion | 9 (40.1) | 22.5 | 17.7–27.2 | 0.005 |
| Vascular invasion | 10 (76.9) | 10.0 | 5.3–14.7 | |
| No lymphatic invasion | 11 (42.3) | 18.0 | 15.6–23.8 | 0.044 |
| Lymphatic invasion | 8 (88.8) | 10.0 | 5.6–14.4 | |
| No neural invasion | 7 (41.2) | 21.5 | 15.5–27.4 | 0.249 |
| Neural invasion | 12 (66.7) | 13.0 | 4.9–21.0 | |
| Degree of differentiation | 0.003 | |||
| G1–G2 | 15 (53.5) | 19.0 | 4.6–23.1 | |
| G3 | 2 (40.0) | 16.0 | 7.7–24.7 | |
| Global survival | 18.0 | 12.5–23.5 |
| Research Variable | Univariate | Multiple | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Sex (male) | 2.050 | 0.789–5.325 | 0.140 | |||
| Age | 1.000 | 0.949–1.054 | 0.988 | - | ||
| Stage I vs. II | 1.566 | 0.555–4.415 | 0.396 | - | ||
| ≥185 portal CTC | 3.236 | 1.135–5.221 | 0.028 | 4.464 | 1.316–15.152 | 0.016 |
| ≥15 portal clusters | 2.486 | 0.989–6.247 | 0.053 | 1.330 | 0.443–4.528 | 0.624 |
| Vascular invasion | 3.568 | 1.346–9.457 | 0.011 | 3.663 | 1.321–10.204 | 0.013 |
| Lymphatic invasion | 2.418 | 0.969–6.031 | 0.058 | 2.512 | 0.940–6.711 | 0.066 |
| Neural invasion | 1.698 | 0.666–4.328 | 0.268 | - | ||
| G1–2 vs. G3 | 0.841 | 0.196–3.771 | 0.841 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padillo-Ruiz, J.; Suarez, G.; Pereira, S.; Calero-Castro, F.J.; Tinoco, J.; Marin, L.; Bernal, C.; Cepeda-Franco, C.; Alamo, J.M.; Almoguera, F.; et al. Circulating Tumor Cells Enumeration from the Portal Vein for Risk Stratification in Early Pancreatic Cancer Patients. Cancers 2021, 13, 6153. https://doi.org/10.3390/cancers13246153
Padillo-Ruiz J, Suarez G, Pereira S, Calero-Castro FJ, Tinoco J, Marin L, Bernal C, Cepeda-Franco C, Alamo JM, Almoguera F, et al. Circulating Tumor Cells Enumeration from the Portal Vein for Risk Stratification in Early Pancreatic Cancer Patients. Cancers. 2021; 13(24):6153. https://doi.org/10.3390/cancers13246153
Chicago/Turabian StylePadillo-Ruiz, Javier, Gonzalo Suarez, Sheila Pereira, Francisco José Calero-Castro, Jose Tinoco, Luis Marin, Carmen Bernal, Carmen Cepeda-Franco, Jose Maria Alamo, Francisco Almoguera, and et al. 2021. "Circulating Tumor Cells Enumeration from the Portal Vein for Risk Stratification in Early Pancreatic Cancer Patients" Cancers 13, no. 24: 6153. https://doi.org/10.3390/cancers13246153