
Impact of Interobserver Variability in Manual Segmentation of Non-Small Cell Lung Cancer (NSCLC) Applying Low-Rank Radiomic Representation on Computed Tomography

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
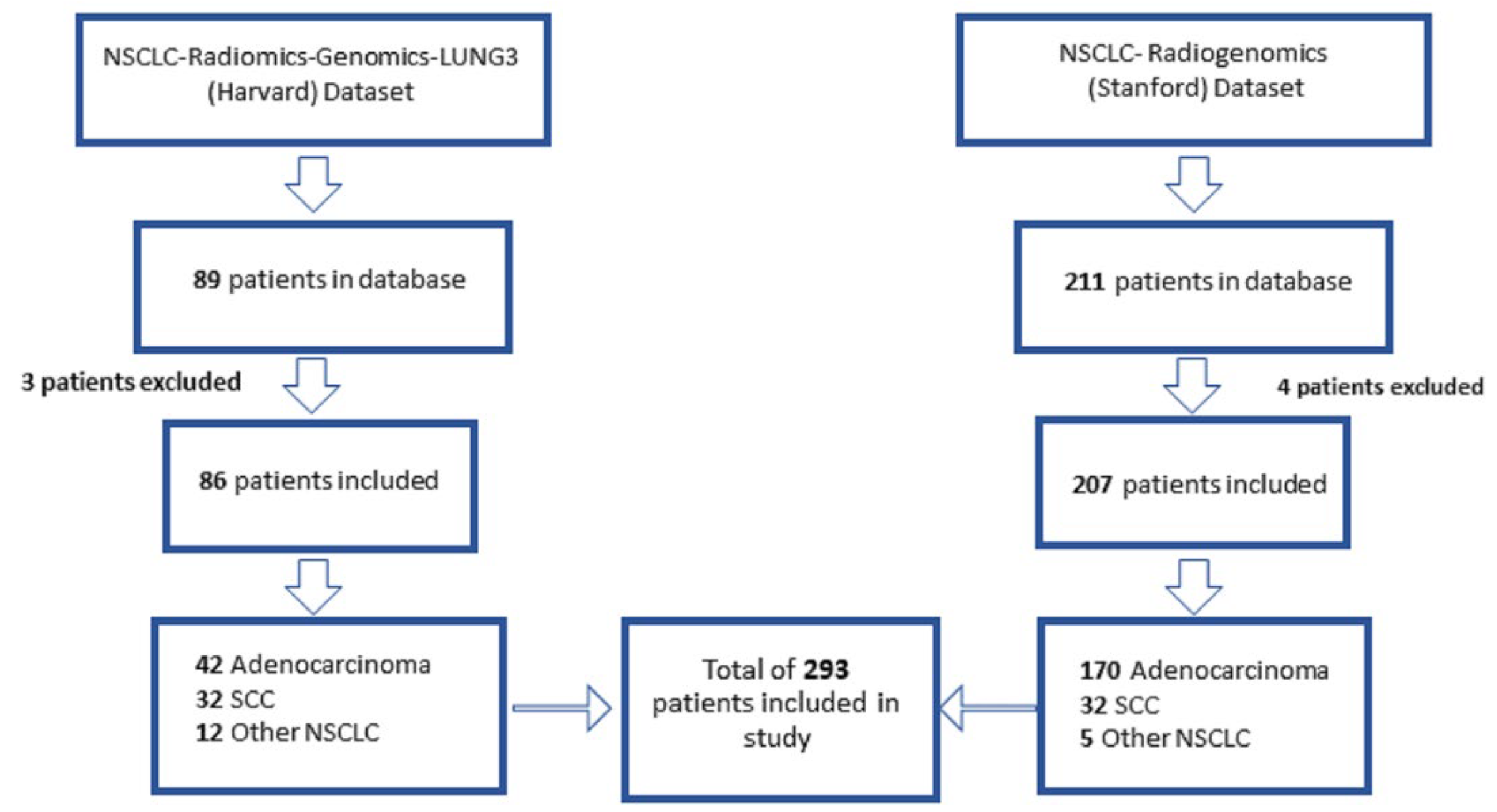
2.1. Patient Population and Study Data
2.2. Radiomic Feature Extraction and Statistical Analysis
3. Results
3.1. Patient Population
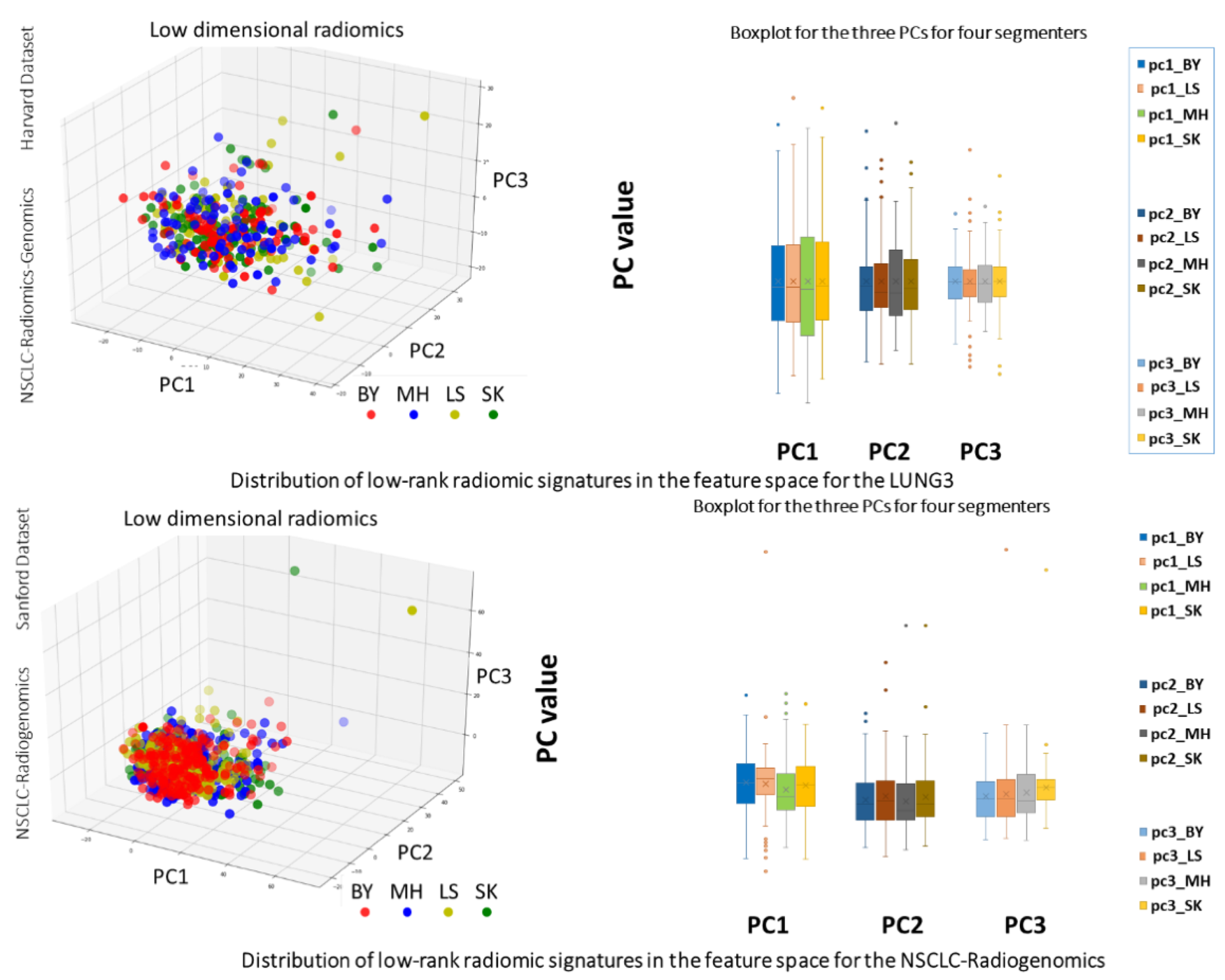
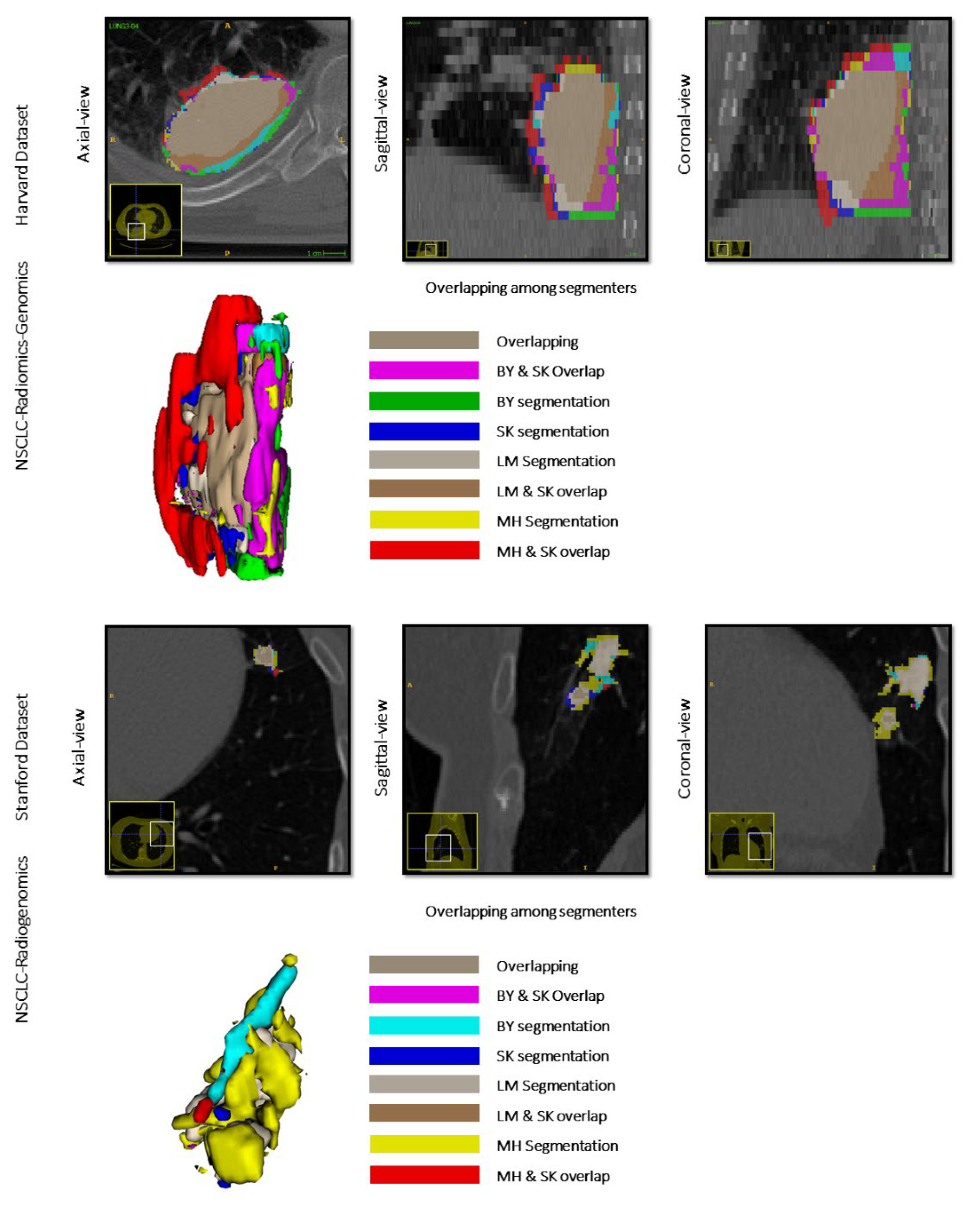
3.2. Analysis of Interobserver Variability on Radiomic Feature Extraction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
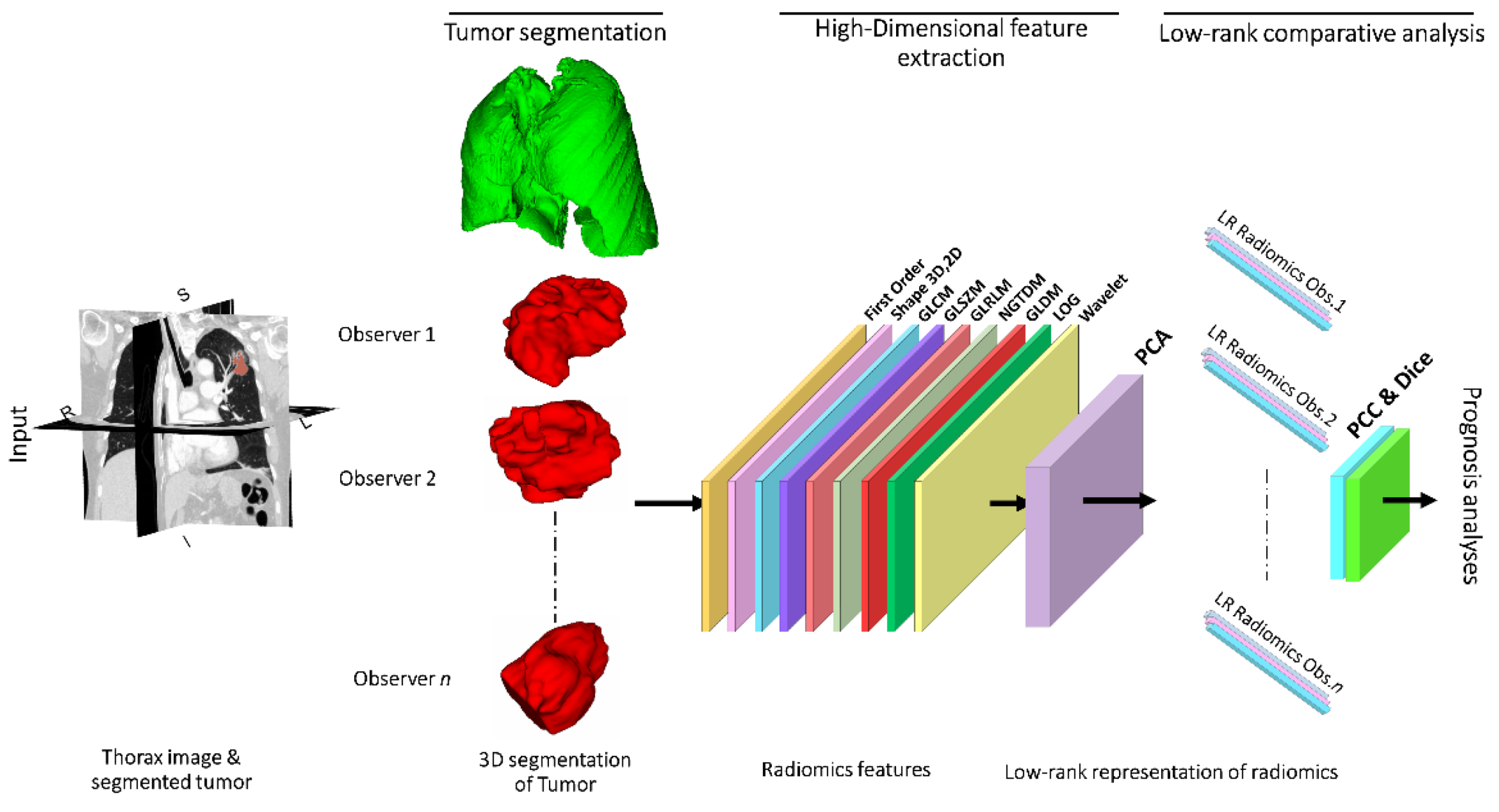
Appendix A.1. Low-Rank Representation of Radiomics
Appendix A.2. Low-Rank Correlation of Interobserver’s Radiomics
References
- Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gastonis, C.; Marcus, P.M.; Sicks, J.D.; et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar]
- van Baardwijk, A.; Wanders, S.; Boersma, L.; Borger, J.; Ollers, M.; Dingemans, A.M.; Bootsma, G.; Geraedts, W.; Pitz, C.; Lunde, R.; et al. Mature results of an individualized radiation dose prescription study based on normal tissue constraints in stages I to III non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 1380–1386. [Google Scholar] [CrossRef]
- Parmar, C.; Rios Velazquez, E.; Leijenaar, R.; Jermoumi, M.; Carvalho, S.; Mak, R.H.; Mitra, S.; Shankar, B.U.; Kikinis, R.; Haibe-Kains, B.; et al. Robust Radiomics feature quantification using semiautomatic volumetric segmentation. PLoS ONE 2014, 9, e102107. [Google Scholar] [CrossRef]
- Huang, Q.; Lu, L.; Dercle, L.; Lichtenstein, P.; Li, Y.; Yin, Q.; Zong, M.; Schwartz, L.; Zhao, B. Interobserver variability in tumor contouring affects the use of radiomics to predict mutational status. J. Med. Imaging 2018, 5, 011005. [Google Scholar] [CrossRef]
- Balagurunathan, Y.; Kumar, V.; Gu, Y.; Kim, J.; Wang, H.; Liu, Y.; Goldgof, D.B.; Hall, L.O.; Korn, R.; Zhao, B.; et al. Test-retest reproducibility analysis of lung CT image features. J. Digit. Imaging 2014, 27, 805–823. [Google Scholar] [CrossRef] [Green Version]
- Wu, W.; Parmar, C.; Grossmann, P.; Quakenbush, J.; Lambin, P.; Bussink, J.; Mak, R.; Aerts, H.J. Exploratory study to identify radiomics classifiers for lung cancer histology. Front. Oncol. 2016, 6, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, D.V.; Tucker, S.L.; Zhou, S.; Liao, Z.; Mawlawi, O.; Ibbott, G.; Court, L.E. Prognostic value and reproducibility of pretreatment CT texture features in stage III non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 834–842. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J.; Grossmann, P.; Tan, Y.; Oxnard, G.R.; Rizvi, N.; Schwartz, L.H.; Zhao, B. Defining a radiomic response phenotype: A pilot study using targeted therapy in NSCLC. Sci. Rep. 2016, 6, 33860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coroller, T.P.; Grossmann, P.; Hou, Y.; Rios Velasquez, E.; Liejenaar, R.T.; Hermann, G.; Lambin, P.; Haibe-Kains, B.; Mak, R.H.; Aerts, H.J. CT-based radiomic signature predicts distant metastasis in lung adenocarcinoma. Radiother. Oncol. 2015, 114, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Yip, S.S.; Aerts, H.J. Applications and limitations of radiomics. Phys. Med. Biol. 2016, 61, R150–R166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Cavalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef] [PubMed]
- Desseroit, M.C.; Visvikis, D.; Tixier, F.; Majdoub, M.; Perdrisot, R.; Guillevin, R.; Cheze le Rest, C.; Hatt, M. Development of a nomogram combining clinical staging with (18)F-FDG PET/CT image features in non-small-cell lung cancer stage I–III. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1477–1485. [Google Scholar] [CrossRef] [Green Version]
- Fave, X.; Cook, M.; Frederick, A.; Zhang, L.; Yang, J.; Fried, D.; Stingo, F.; Court, L. Preliminary investigation into sources of uncertainty in quantitative imaging features. Comput. Med. Imaging Graph. 2015, 44, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Huynh, E.; Coroller, T.P.; Narayan, V.; Agrawal, V.; Romano, J.; Franco, I.; Parmar, C.; Hou, Y.; Mak, R.H.; Aerts, H.J. Associations of radiomic data extracted from static and respiratory-gated CT scans with disease recurrence in lung cancer patients treated with SBRT. PLoS ONE 2017, 12, e0169172. [Google Scholar] [CrossRef] [Green Version]
- Kalpathy-Cramer, J.; Mamomov, A.; Zhao, B.; Lu, L.; Cherezov, D.; Napel, S.; Echegaray, S.; Rubin, D.; McNitt-Gray, M.; Lo, P.; et al. Radiomics of lung nodules: A multi-institutional study of robustness and agreement of quantitative imaging features. Tomography 2016, 2, 430–437. [Google Scholar] [CrossRef] [PubMed]
- Mackin, D.; Fave, X.; Zhang, L.; Fried, D.; Yang, J.; Taylor, B.; Rodriguez-Rivera, E.; Dodge, C.; Jones, A.K.; Court, L. Measuring computed tomography scanner variability of radiomics features. Invest. Radiol. 2015, 50, 757–765. [Google Scholar] [CrossRef]
- Zhao, B.; Tan, Y.; Tsai, W.Y.; Qi, J.; Xie, C.; Lu, L.; Schwartz, L.H. Reproducibility of radiomics for deciphering tumor phenotype with imaging. Sci. Rep. 2016, 6, 23428. [Google Scholar] [CrossRef] [Green Version]
- Traverso, A.; Wee, L.; Dekker, A.; Gillies, R. Repeatability and reproducibility of radiomic features: A systematic review. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1143–1158. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J.; Wee, L.; Rios Velasquez, E.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Lambin, P. Data from NSCLC-radiomics. Cancer Imaging Arch. 2019. [Google Scholar] [CrossRef]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [Green Version]
- Bakr, S.; Gevaert, O.; Echegaray, S.; Ayers, K.; Zhou, M.; Shafiq, M.; Zheng, H.; Zhang, W.; Leung, A.; Kadoch, M.; et al. Data for NSCLC radiogenomics collection. Cancer Imaging Arch. 2017. [Google Scholar] [CrossRef]
- Bakr, S.; Gevaert, O.; Echegaray, S.; Ayers, K.; Zhou, M.; Shafiq, M.; Zheng, H.; Benson, J.A.; Zhang, W.; Leung, A.; et al. A radiogenomic dataset of non-small cell lung cancer. Sci. Data 2018, 5, 180202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gevaert, O.; Xu, J.; Hoang, C.D.; Leung, A.N.; Xu, Y.; Quon, A.; Rubin, D.L.; Napel, S.; Plevritis, S.K. Non-small cell lung cancer: Identifying prognostic imaging biomarkers by leveraging public gene expression microarray data--methods and preliminary results. Radiology 2012, 264, 387–396. [Google Scholar] [CrossRef]
- Yushkevich, P.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef] [Green Version]
- Dice, L.R. Measures of the amount of ecologic association between species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Meng, Y.; Sun, J.; Qu, N.; Zhang, G.; Yu, T.; Piao, H. Application of radiomics for personalized treatment of cancer patients. Cancer Manag. Res. 2019, 11, 10851–10858. [Google Scholar] [CrossRef] [Green Version]
- Dalal, V.; Carmicheal, J.; Dhaliwal, A.; Jain, M.; Kaur, S.; Batra, S.K. Radiomics in stratification of pancreatic cystic lesions: Machine learning in action. Cancer Lett. 2020, 469, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Waninger, J.J.; Green, M.D.; Cheze Le Rest, C.; Rosen, B.; El Naqa, I. Integrating radiomics into clinical trial design. Q. J. Nucl. Med. Mol. Imaging 2019, 63, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Chaddad, A.; Kucharczyk, M.J.; Daniel, P.; Sabri, S.; Jean-Claude, B.J.; Niazi, T.; Abdulkarim, B. Radiomics in glioblastoma: Current status and challenges facing clinical implementation. Front. Oncol. 2019, 9, 374. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Wang, S.; Dong, D.; Wei, J.; Fang, C.; Zhou, X.; Sun, K.; Li, L.; Li, B.; Wang, M. The applications of radiomics in precision diagnosis and treatment of oncology: Opportunities and challenges. Theranostics 2019, 9, 1303–1322. [Google Scholar] [CrossRef]
- Rizzo, S.; Botta, F.; Raimondi, S.; Origgi, D.; Fanciullo, C.; Morganti, A.G.; Bellomi, M. Radiomics: The facts and the challenges of image analysis. Eur. Radiol. Exp. 2018, 2, 36. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Rios-Velazquez, E.; Leijenaar, R.; Carvalho, S.; van Stiphout, R.G.; Granton, P.; Zegers, C.M.; Gillies, R.; Boellard, R.; Dekker, A. Radiomics: Extracting more information from medical images using advanced feature analysis. Eur. J. Cancer 2012, 48, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Lambin, P.; Leijenaar, R.T.; Deist, T.M.; Peerlings, J.; de Jong, E.E.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.; Even, A.J.; Jochems, A. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Chen, B.; Zhang, R.; Gan, Y.; Yang, L.; Li, W. Development and clinical application of radiomics in lung cancer. Radiat. Oncol. 2017, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.; Devaraj, A. Radiomics of pulmonary nodules and lung cancer. Transl. Lung Cancer Res. 2017, 6, 86–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.W.L.; Dekker, A.; Fenstermacher, D.; et al. Radiomics: The process and the challenges. Magn. Reson. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef] [Green Version]
- Henriksson, E.; Kjellen, E.; Wahlberg, P.; Ohlsson, T.; Wennerberg, J.; Brun, E. 2-Deoxy-2-[18F] fluoro-D-glucose uptake and correlation to intratumoral heterogeneity. Anticancer Res. 2007, 27, 2155–2159. [Google Scholar]
- Yang, X.; Knopp, M.V. Quantifying tumor vascular heterogeneity with dynamic contrast-enhanced magnetic resonance imaging: A review. J. Biomed. Biotechnol. 2011, 2011, 732848. [Google Scholar] [CrossRef]
- Basu, S.; Kwee, T.C.; Gatenby, R.; Saboury, B.; Torigian, D.A.; Alavi, A. Evolving role of molecular imaging with PET in detecting and characterizing heterogeneity of cancer tissue at the primary and metastatic sites, a plausible explanation for failed attempts to cure malignant disorders. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 987–991. [Google Scholar] [CrossRef] [Green Version]
- Ganeshan, B.; Abaleke, S.; Young, R.C.; Chatwin, C.R.; Miles, K.A. Texture analysis of non-small cell lung cancer on unenhanced computed tomography: Initial evidence for a relationship with tumour glucose metabolism and stage. Cancer Imaging 2010, 10, 137–143. [Google Scholar] [CrossRef]
- Ganeshan, B.; Panayiotou, E.; Burnand, K.; Dizdarevic, S.; Miles, K. Tumour heterogeneity in non-small cell lung carcinoma assessed by CT texture analysis: A potential marker of survival. Eur. Radiol. 2012, 22, 796–802. [Google Scholar] [CrossRef]
- Ganeshan, B.; Goh, V.; Mandeville, H.C.; Ng, Q.S.; Hoskin, P.J.; Miles, K.A. Non-small cell lung cancer: Histopathologic correlates for texture parameters at CT. Radiology 2013, 266, 326–336. [Google Scholar] [CrossRef]
- El Naqa, I.; Grigsby, P.; Apte, A.; Kidd, E.; Donnelly, E.; Khullar, D.; Chaudhari, S.; Yang, D.; Schmitt, M.; Laforest, R. Exploring feature-based approaches in PET images for predicting cancer treatment outcomes. Pattern Recognit. 2009, 42, 1162–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vaidya, M.; Creach, K.M.; Frye, J.; Dehdashti, F.; Bradley, J.D.; El Naqa, I. Combined PET/CT image characteristics for radiotherapy tumor response in lung cancer. Radiother. Oncol. 2012, 102, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, B.; LaRiviere, M.J.; Cohen, E.A.; Buckingham, T.H.; Yee, S.S.; Black, T.A.; Chien, A.L.; Noel, P.; Hwang, W.; Katz, S.I.; et al. Combining radiomic phenotypes of non-small cell lung cancer with liquid biopsy data may improve prediction of response to EGFR inhibitors. Sci. Rep. 2021, 11, 9984. [Google Scholar] [CrossRef] [PubMed]
- Emaminejad, N.; Qian, W.; Guan, Y.; Tan, M.; Qiu, Y.; Liu, H.; Zheng, B. Fusion of quantitative image and genomic biomarkers to improve prognosis assessment of early stage lung cancer patients. IEEE Trans. Biomed. Eng. 2016, 63, 1034–1043. [Google Scholar] [CrossRef]
- Weltens, C.; Menten, J.; Feron, M.; Bellon, E.; Demaerel, P.; Maes, F.; Van de Bogaert, W.; van der Schueren, E. Interobserver variations in gross tumor volume delineation of brain tumors on computed tomography and impact of magnetic resonance imaging. Radiother. Oncol. 2001, 60, 49–59. [Google Scholar] [CrossRef]
- Leunens, G.; Menten, J.; Weltens, C.; Verstraete, J.; van der Schueren, E. Quality assessment of medical decision making in radiation oncology: Variability in target volume delineation for brain tumours. Radiother. Oncol. 1993, 29, 169–175. [Google Scholar] [CrossRef]
- Cazzaniga, L.F.; Marinoni, M.A.; Bossi, A.; Bianchi, E.; Cagna, E.; Cosentino, D.; Scandolaro, L.; Valli, M.; Frigero, M. Interphysician variability in defining the planning target volume in the irradiation of prostate and seminal vesicles. Radiother. Oncol. 1998, 47, 293–296. [Google Scholar] [CrossRef]
- Hamilton, C.S.; Denham, J.W.; Joseph, D.J.; Lamb, D.S.; Spry, N.A.; Gray, A.J.; Atkinson, C.H.; Wynne, C.J.; Abdelaal, A.; Bydder, P.V. Treatment and planning decisions in non-small cell carcinoma of the lung: An Australasian patterns of practice study. Clin. Oncol. (R. Coll. Radiol.) 1992, 4, 141–147. [Google Scholar] [CrossRef]
- Tai, P.; Van Dyk, J.; Yu, E.; Battista, J.; Stitt, L.; Coad, T. Variability of target volume delineation in cervical esophageal cancer. Int. J. Radiat. Oncol. Biol. Phys. 1998, 42, 277–288. [Google Scholar] [CrossRef]
- Valley, J.F.; Mirimanoff, R.O. Comparison of treatment techniques for lung cancer. Radiother. Oncol. 1993, 28, 168–173. [Google Scholar] [CrossRef]
- Graham, M.V.; Purdy, J.A.; Emami, B.; Matthews, J.W.; Harms, W.B. Preliminary results of a prospective trial using three dimensional radiotherapy for lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 1995, 33, 993–1000. [Google Scholar] [CrossRef]
- Senan, S.; van Sörnsen de Koste, J.; Samson, M.; Tankink, H.; Jansen, P.; Nowak, P.J.; Krol, A.D.; Schmitz, P.; Lagerwaard, F.J. Evaluation of a target contouring protocol for 3D conformal radiotherapy in non-small cell lung cancer. Radiother. Oncol. 1999, 53, 247–255. [Google Scholar] [CrossRef]
- Harris, K.M.; Adams, H.; Lloyd, D.C.; Harvey, D.J. The effect on apparent size of simulated pulmonary nodules of using three standard CT window settings. Clin. Radiol. 1993, 47, 241–244. [Google Scholar] [CrossRef]
- Graham, M.V.; Matthews, J.W.; Harms, W.B.; Emami, B.; Glazer, H.S.; Purdy, J.A. Three-dimensional radiation treatment planning study for patients with carcinoma of the lung. Int. J. Radiat. Oncol. Biol. Phys. 1994, 29, 1105–1117. [Google Scholar] [CrossRef]
- Leijenaar, R.T.; Carvalho, S.; Velazquez, E.R.; van Elmpt, W.J.; Parmar, C.; Hoekstra, O.S.; Hoekstra, C.J.; Boellaard, R.; Dekker, A.L.; Gillies, R.J.; et al. Stability of FDG-PET Radiomics features: An integrated analysis of test-retest and inter-observer variability. Acta Oncol. 2013, 52, 1391–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forgacs, A.; Pall Jonsson, H.; Dahlbom, M.; Daver, F.; Difranco, M.; Opposits, G.; Krizsan, A.; Garai, I.; Czernin, J.; Varga, J.; et al. A study on the basic criteria for selecting heterogeneity parameters of F18-FDG PET images. PLoS ONE 2016, 11, e0164113. [Google Scholar] [CrossRef]
- Buch, K.; Li, B.; Qureshi, M.M.; Kuno, H.; Anderson, S.W.; Sakai, O. Quantitative assessment of variation in CT parameters on texture features: Pilot study using a nonanatomic phantom. Am. J. Neuroradiol. 2017, 38, 981–985. [Google Scholar] [CrossRef] [Green Version]
- Zhao, B.; Tan, Y.; Tsai, W.Y.; Schwartz, L.H.; Lu, L. Exploring variability in CT characterization of tumors: A preliminary phantom study. Transl. Oncol. 2014, 7, 88–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logue, J.P.; Sharrock, C.L.; Cowan, R.A.; Read, G.; Marrs, J.; Mott, D. Clinical variability of target volume description in conformal radiotherapy planning. Int. J. Radiat. Oncol. Biol. Phys. 1998, 41, 929–931. [Google Scholar] [CrossRef]
- Van de Steene, J.; Linthout, N.; de Mey, J.; Vinh-Hung, V.; Claassens, C.; Noppen, M.; Bel, A.; Storme, G. Definition of gross tumor volume in lung cancer: Inter-observer variability. Radiother. Oncol. 2002, 62, 37–49. [Google Scholar] [CrossRef]
- Giraud, P.; Elles, S.; Helfre, S.; De Rycke, Y.; Servois, V.; Carette, M.F.; Alzieu, C.; Bondiau, P.Y.; Dubray, B.; Touboul, E.; et al. Conformal radiotherapy for lung cancer: Different delineation of the gross tumor volume (GTV) by radiologists and radiation oncologists. Radiother. Oncol. 2002, 62, 27–36. [Google Scholar] [CrossRef]
- Haga, A.; Takahashi, W.; Aoki, S.; Nawa, K.; Yamashita, H.; Abe, O.; Nakagawa, K. Classification of early stage non-small cell lung cancers on computed tomographic images into histological types using radiomic features: Interobserver delineation variability analysis. Radiol. Phys. Technol. 2018, 11, 27–35. [Google Scholar] [CrossRef]
- Pearson, K. LIII. On lines and planes of closest fit to systems of points in space. Lond. Edinb. Dublin Philos. Mag. J. Sci. 1901, 2, 559–572. [Google Scholar] [CrossRef] [Green Version]
- Hotelling, H. Analysis of a complex of statistical variables into principal components. J. Educ. Psychol. 1933, 24, 417–441. [Google Scholar] [CrossRef]
- Jolliffe, I.T. Principle Component Analysis, 2nd ed.; Springer: New York, NY, USA, 2002; 487p. [Google Scholar]
- Pearson, K., VII. Note on regression and inheritance in the case of two parents. Proc. R. Soc. Lond. 1895, 58. [Google Scholar] [CrossRef]
- Sørenson, T. A method of establishing groups of equal amplitude in plant sociology based on similarity of species content and its application to analyses of the vegetation on Danish commons. K. Dan. Vidensk. Selsk. Biol. Skr. 1948, 5, 3–34. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NSCLC-Radiomics-Genomics | ||
|---|---|---|
| Gender | Male Female | 61 (68.5%) 28 (31.5%) |
| Clinical combined stage curated | Stage I Stage II Stage III Unknown | 39 (43.8%) 25 (28.1%) 12 (13.5%) 11 (12.4%) |
| Non-small cell lung cancer (NSCLC) | Adenocarcinoma, Squamous cell carcinoma Other or unknown | 42 (47.2%) 33 (37.1%) 12 (13.5%) |
| Event | Recurrence or death | 46 (51.7%) |
| NSCLC-Radiogenomics | ||
|---|---|---|
| Age | Median (±IQR) | 69 (43,87) |
| Gender | Male Female | 133 (64.2%) 74 (35.8%) |
| Race | Caucasian Asian Hispanic/Latino African-American Native Hawaiian/Pacific Islander Unknown | 120 (57.4%) 24 (11.8%) 5 (2.4%) 6 (2.9%) 3 (1.5%) 48(23.2) |
| Smoking Status | Non-smoking Smoking Former smoking | 47 (22.7%) 34 (16.4%) 126 (60.9%) |
| EGFR-Mutation Status | Wildtype Mutant Unknown | 128 (61.8%) 42 (20.2%) 37 (17.8%) |
| KRAS Mutation Status | Wildtype Mutant Unknown | 130 (62.8%) 38 (18.3%) 39 (18.8%) |
| Histology | Adenocarcinoma Squamous cell carcinoma NSCLC NOS (not otherwise specified) | 170 (82.1%) 32 (15.5%) 5 (2.4%) |
| Solid-Subsolid (Morphology) | Solid Subsolid Unknown | 134 (64.7%) 68 (32.8%) 5 (2.4%) |
| Event | Recurrence or death | 41(21.1%) |
| NSCLC Dataset | Similarity among Segmenters | ||||||
|---|---|---|---|---|---|---|---|
| Segmenters ID | Correlation Score | Dice Score | Precision(%) | Recall (%) | Boundary Distance | Volume Difference | |
| LUNG3 NSCLC-Radiomics-Genomics Harvard Dataset | BY | 0.92 | 0.89 (±0.25) | 81.8 (±21.8) | 86.1 (±24.5) | 1.2 (±2.7) | 1.1 (±0.5) |
| LS | 0.94 | 0.82 (±0.14) | 81.2 (±2.7) | 69.6 (±24.5) | 6.5 (±26.4) | 2.3 (±21.1) | |
| MH | 0.95 | 0.84 (±0.20) | 72.3 (±22.4) | 88.7 (±18.9) | 4.2 (±15.1) | 0.6 (±1.9) | |
| NSCLC-Radiogenomics Stanford Dataset | BY | 0.93 | 0.69 (±0.28) | 77.8 (±25.1) | 87.3 (±25.2) | 2.92 (±10.7) | 0.3 (±0.8) |
| LS | 0.72 | 0.80 (±0.27) | 84.2 (±31.5) | 47.8 (±29.9) | 16.6 (±52.6) | 0.3 (±1.2) | |
| MH | 0.87 | 0.83 (±0.23) | 80 (±24.3) | 77.1 (±24.7) | 6.2 (±26.1) | 1.4 (±16.9) | |
| Prediction Survival | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| NSCLC Datasets | Modeling Covariates | BY | LS | MH | SK-RS | ||||
| c-Statistic (95% CI) | p Versus Null 1 | c-Statistic (95% CI) | p Versus Null 1 | c-Statistic (95% CI) | p Versus Null 1 | c-Statistic(95% CI) | p Versus Null 1 | ||
| LUNG3 NSCLC-Radiomics-Genomics Harvard Dataset | clinical and demographic 2 | 0.64 | 0.2 | ||||||
| Three PC radiomic signatures | 0.6 | 0.5 | 0.62 | 0.08 | 0.59 | 0.2 | 0.65 | 0.03 | |
| Radiomic signatures, clinical and demographic | 0.65 | 0.3 | 0.68 | 0.04 | 0.66 | 0.2 | 0.7 | 0.03 | |
| NSCLC-Radiogenomics Stanford Dataset | clinical and demographic 3 | 0.6 | 0.007 | ||||||
| Three PC radiomic signatures | 0.65 | 0.001 | 0.64 | 0.04 | 0.67 | 0.003 | 0.65 | 0.003 | |
| Radiomic signatures, clinical and demographic | 0.71 | <0.005 | 0.68 | 0.003 | 0.71 | <0.005 | 0.69 | <0.005 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hershman, M.; Yousefi, B.; Serletti, L.; Galperin-Aizenberg, M.; Roshkovan, L.; Luna, J.M.; Thompson, J.C.; Aggarwal, C.; Carpenter, E.L.; Kontos, D.; et al. Impact of Interobserver Variability in Manual Segmentation of Non-Small Cell Lung Cancer (NSCLC) Applying Low-Rank Radiomic Representation on Computed Tomography. Cancers 2021, 13, 5985. https://doi.org/10.3390/cancers13235985
Hershman M, Yousefi B, Serletti L, Galperin-Aizenberg M, Roshkovan L, Luna JM, Thompson JC, Aggarwal C, Carpenter EL, Kontos D, et al. Impact of Interobserver Variability in Manual Segmentation of Non-Small Cell Lung Cancer (NSCLC) Applying Low-Rank Radiomic Representation on Computed Tomography. Cancers. 2021; 13(23):5985. https://doi.org/10.3390/cancers13235985
Chicago/Turabian StyleHershman, Michelle, Bardia Yousefi, Lacey Serletti, Maya Galperin-Aizenberg, Leonid Roshkovan, José Marcio Luna, Jeffrey C. Thompson, Charu Aggarwal, Erica L. Carpenter, Despina Kontos, and et al. 2021. "Impact of Interobserver Variability in Manual Segmentation of Non-Small Cell Lung Cancer (NSCLC) Applying Low-Rank Radiomic Representation on Computed Tomography" Cancers 13, no. 23: 5985. https://doi.org/10.3390/cancers13235985