
Prostate-Specific Membrane Antigen in Anaplastic and Poorly Differentiated Thyroid Cancer—A New Diagnostic and Therapeutic Target?

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Imaging Protocol and Analyses of 18F-FDG- and 68Ga-PSMA-PET/CT
2.3. Immunohistochemical Analysis
2.3.1. Tissue Selection
2.3.2. Immunohistochemical Staining for PSMA Antigens
2.3.3. Assessment of PSMA Expression
3. Results
3.1. Patient Characteristics
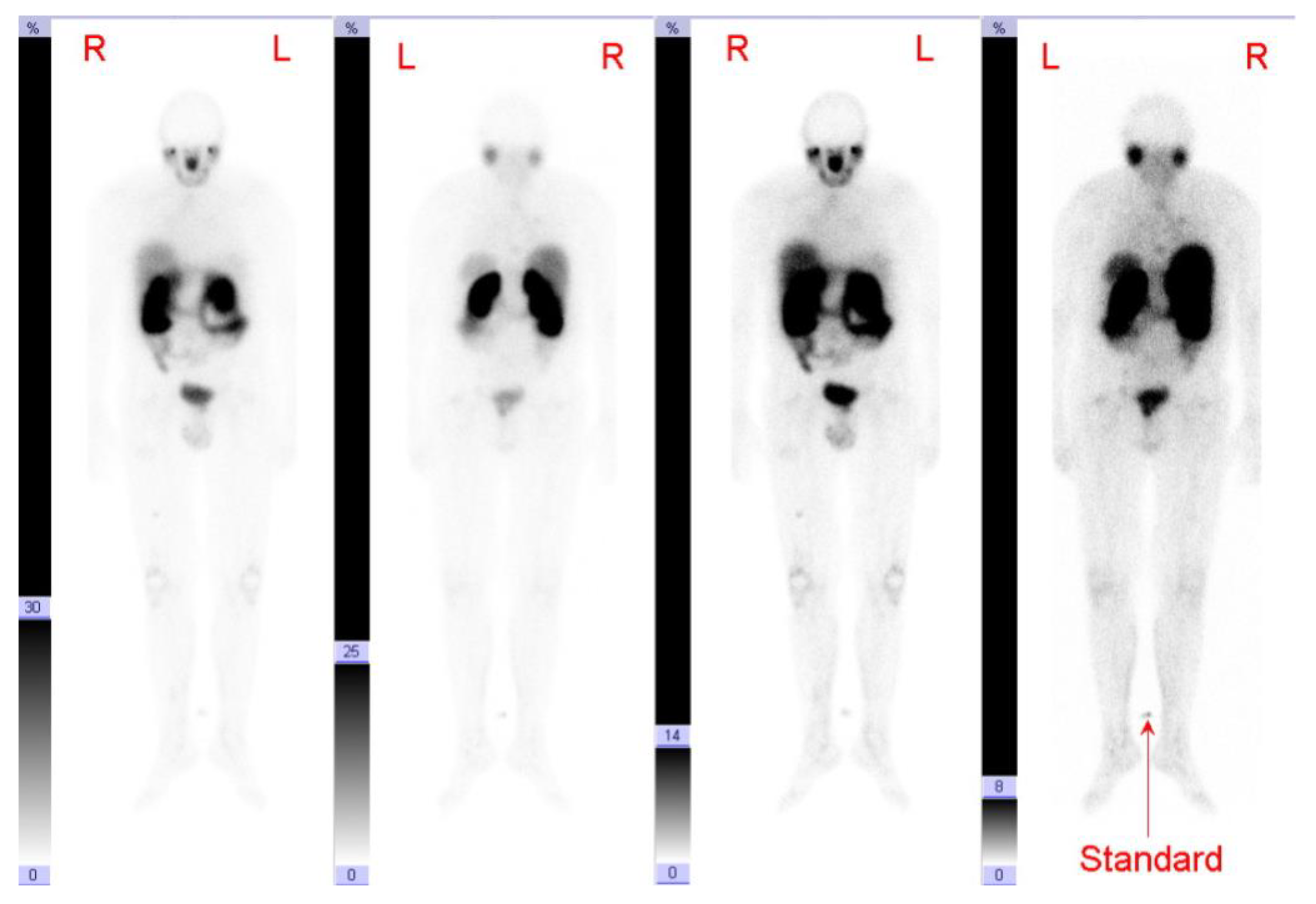
3.2. 68Ga-PSMA-PET/CT
3.3. Case Series
- Patients, in whom 18F-FDG-PET/CT uptake was positive and 68Ga-PSMA-PET/CT negative. This was the case in six of the eight patients evaluated (patient 1–6).
- Patients, in whom 18F-FDG-PET/CT uptake was positive and 68Ga-PSMA-PET/CT showed heterogeneous results. This was the case in one of the eight patients evaluated (patient 7).
- Patients, in whom 68Ga-PSMA-PET/CT uptake was clearly positive and thus a therapeutic option in terms of theranostics—for example, with a 177Lu-PSMA therapy—exists. This was the case in one of the eight patients evaluated (patient 8).
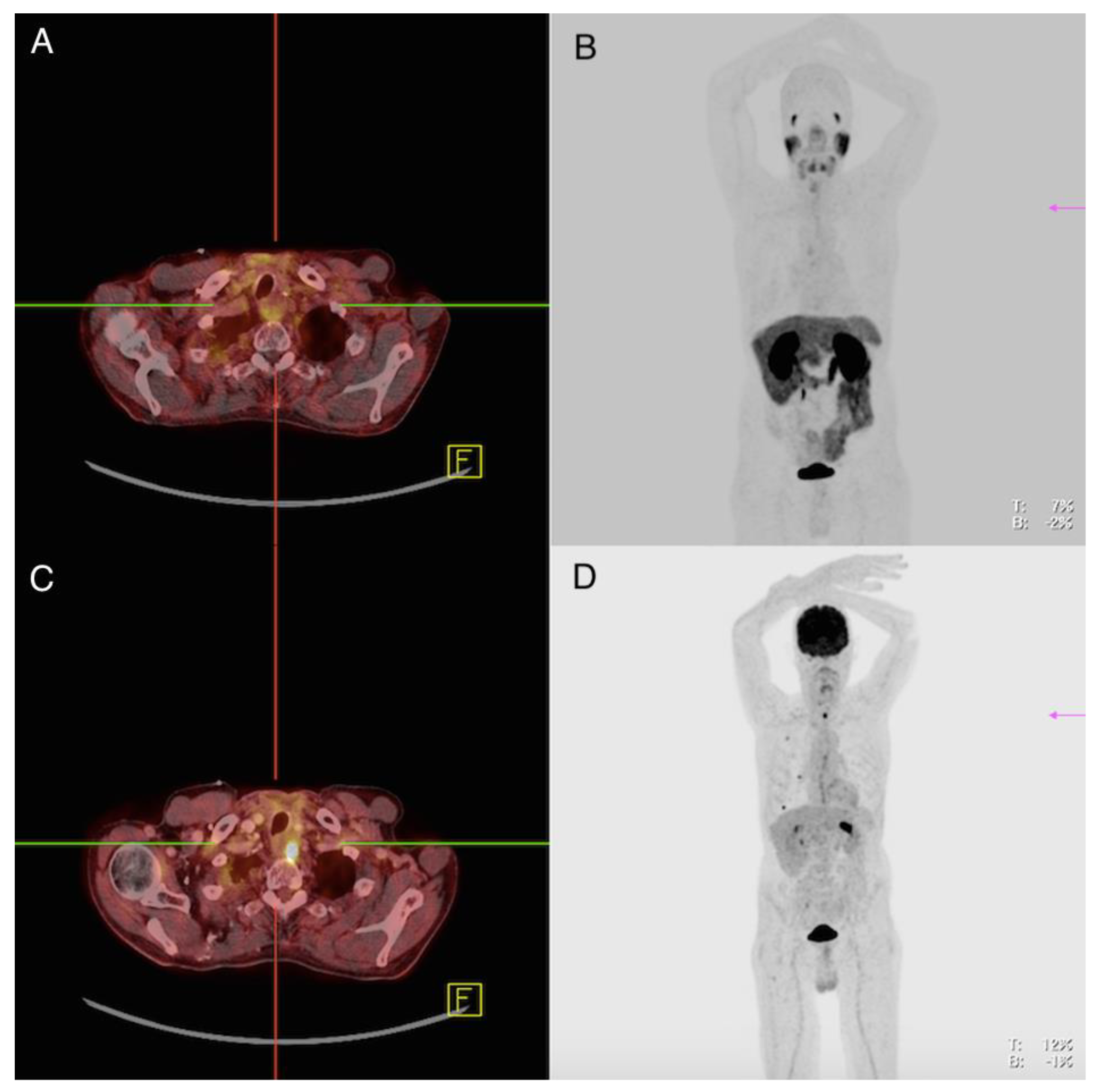
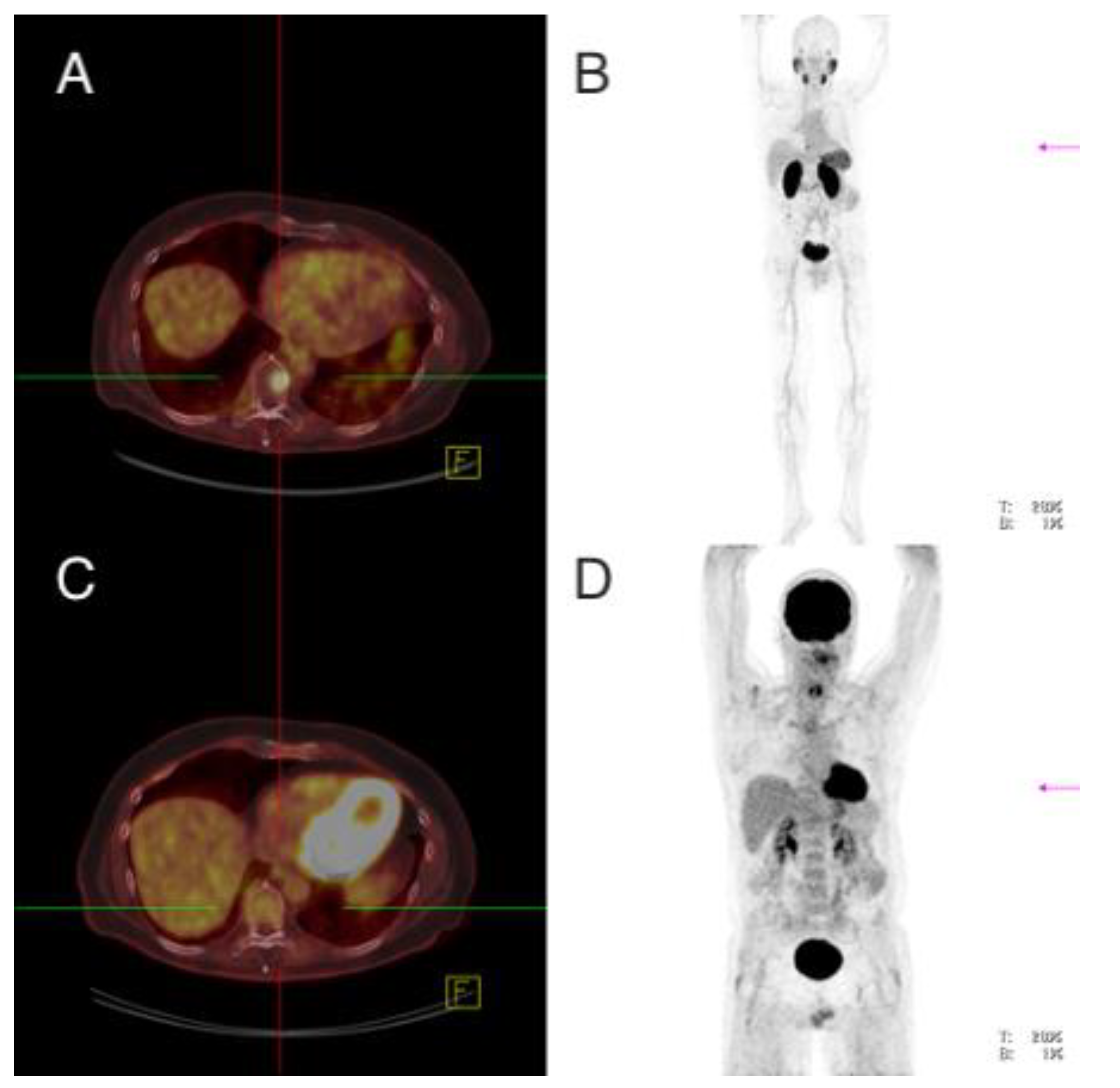
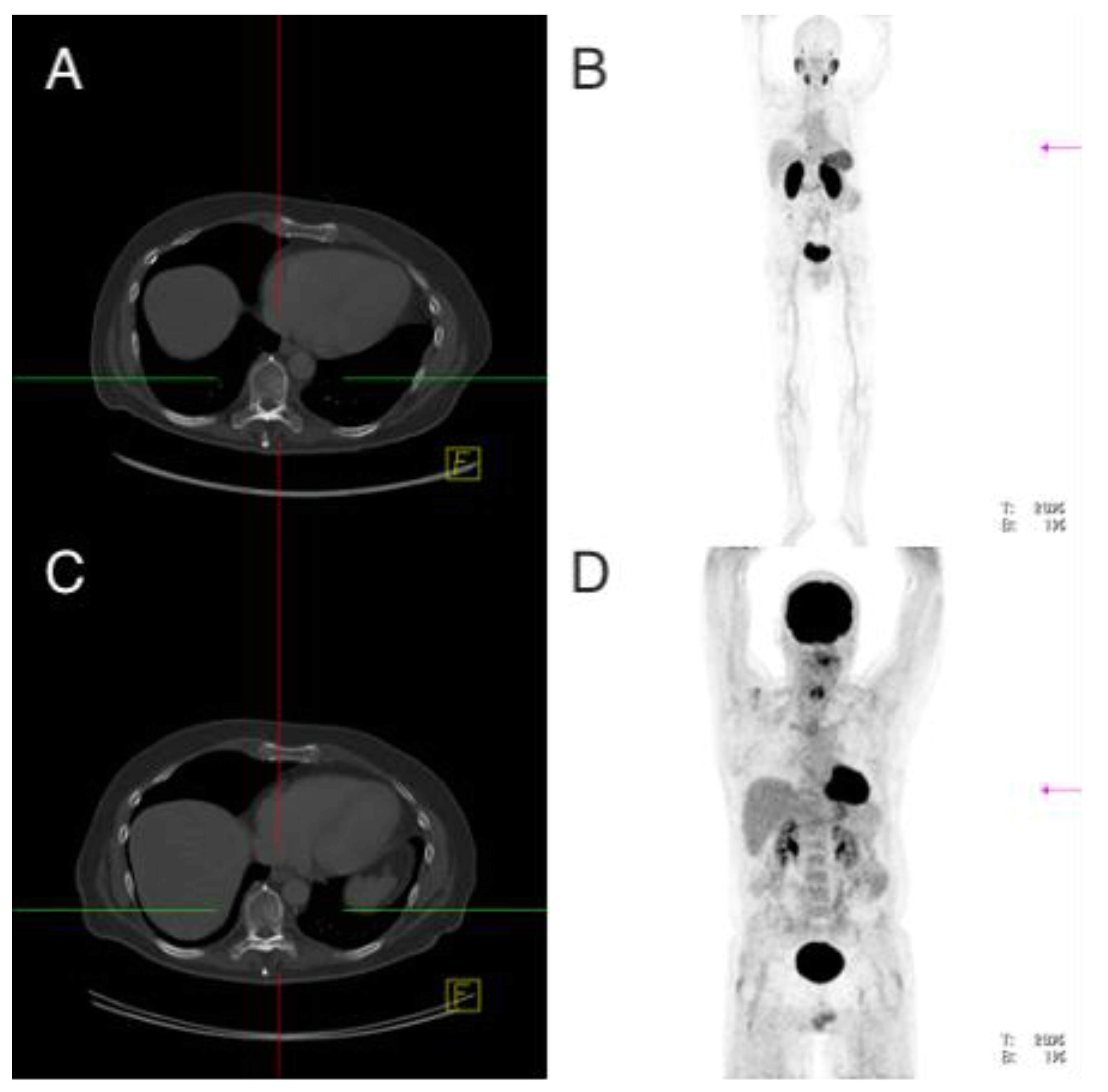
3.3.1. Setting No. 1—18F-FDG-PET/CT Positive, 68Ga-PSMA-PET/CT Negative
Patient 1: Male, ATC, 59 Years Old at the Time of Diagnosis
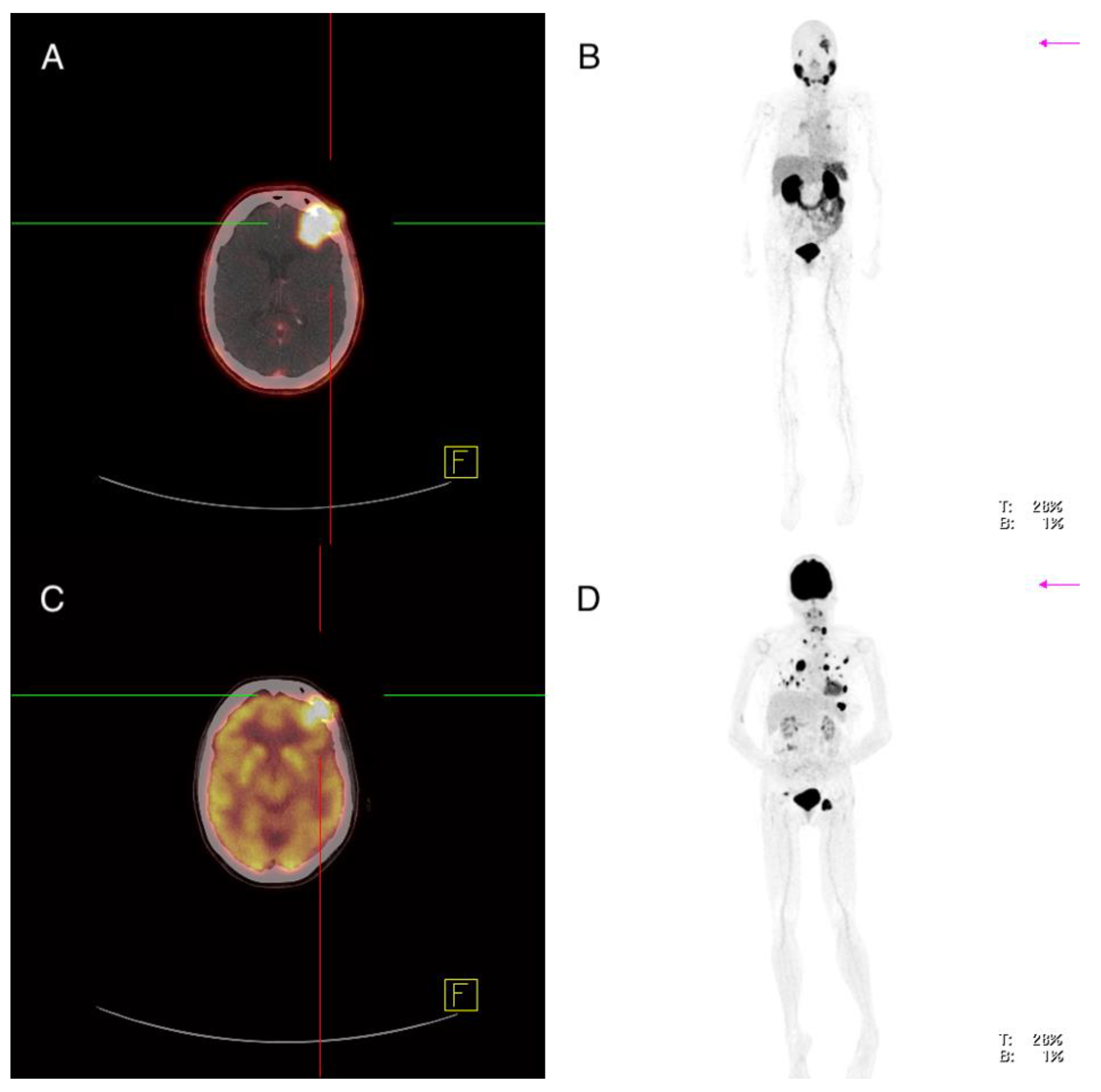
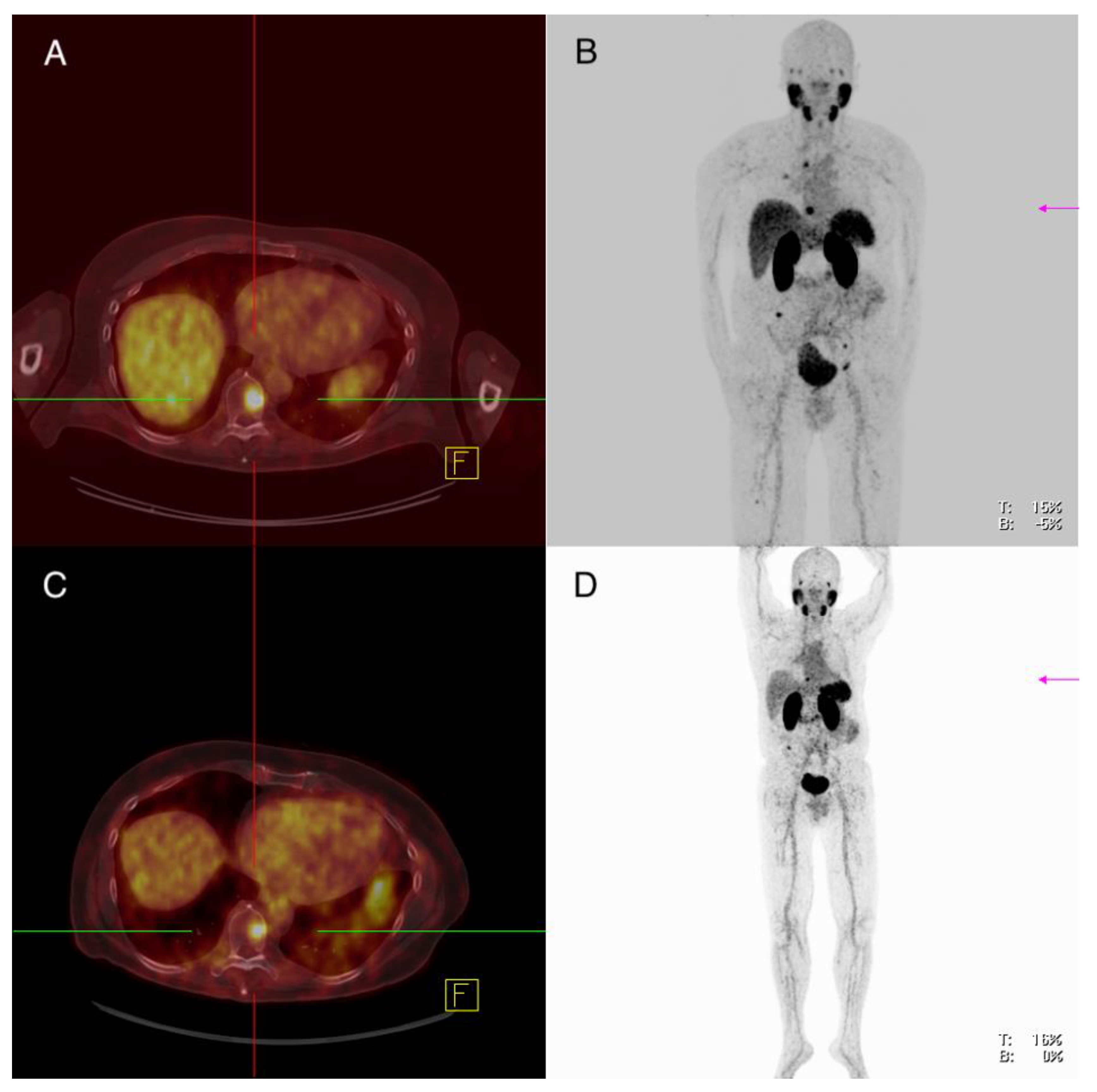
3.3.2. Setting No. 2—18F-FDG-PET/CT Positive, 68Ga-PSMA-PET/CT Heterogenous
Patient 7: Female, PDTC, 61 Years Old at the Time of Diagnosis
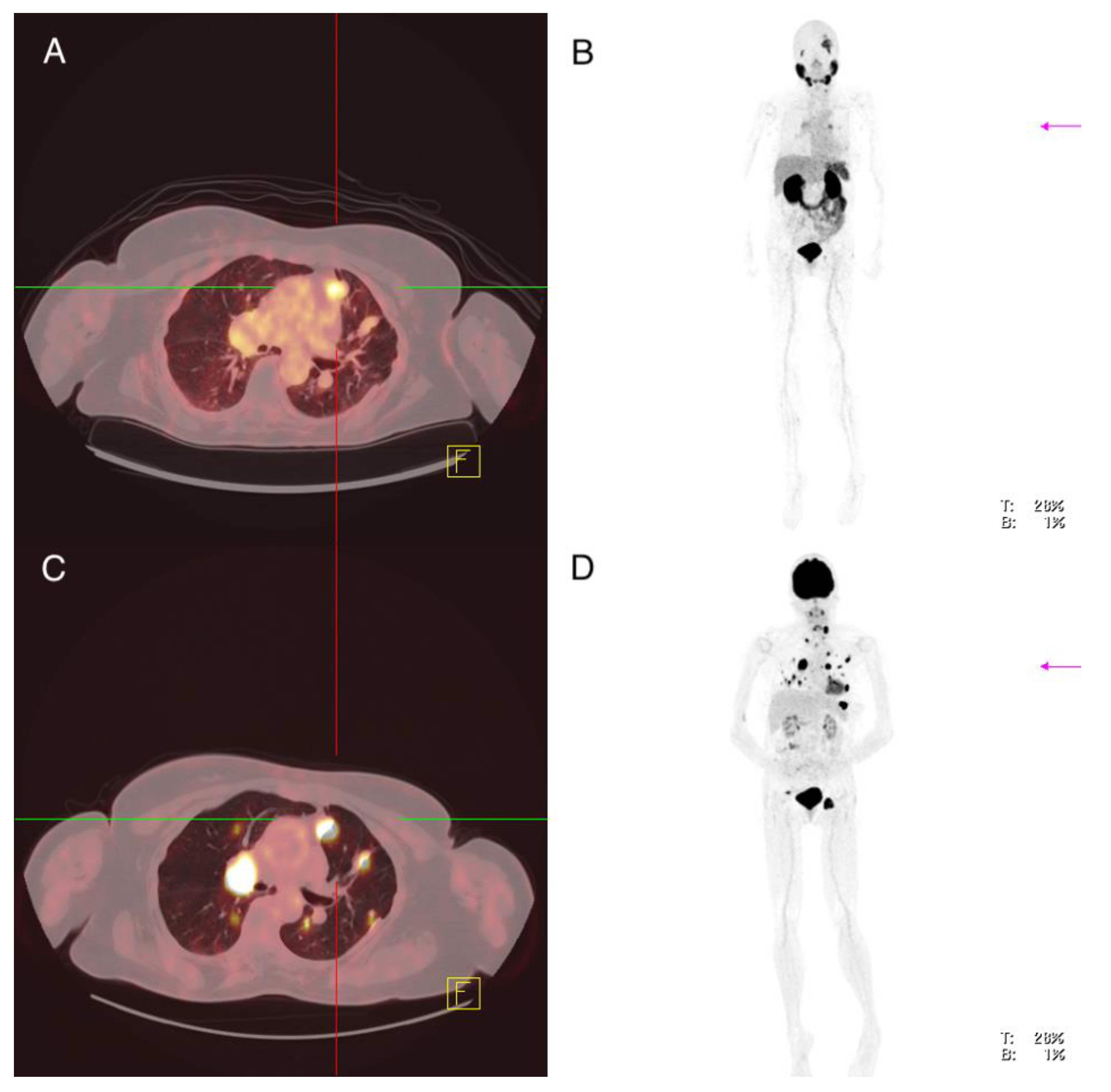
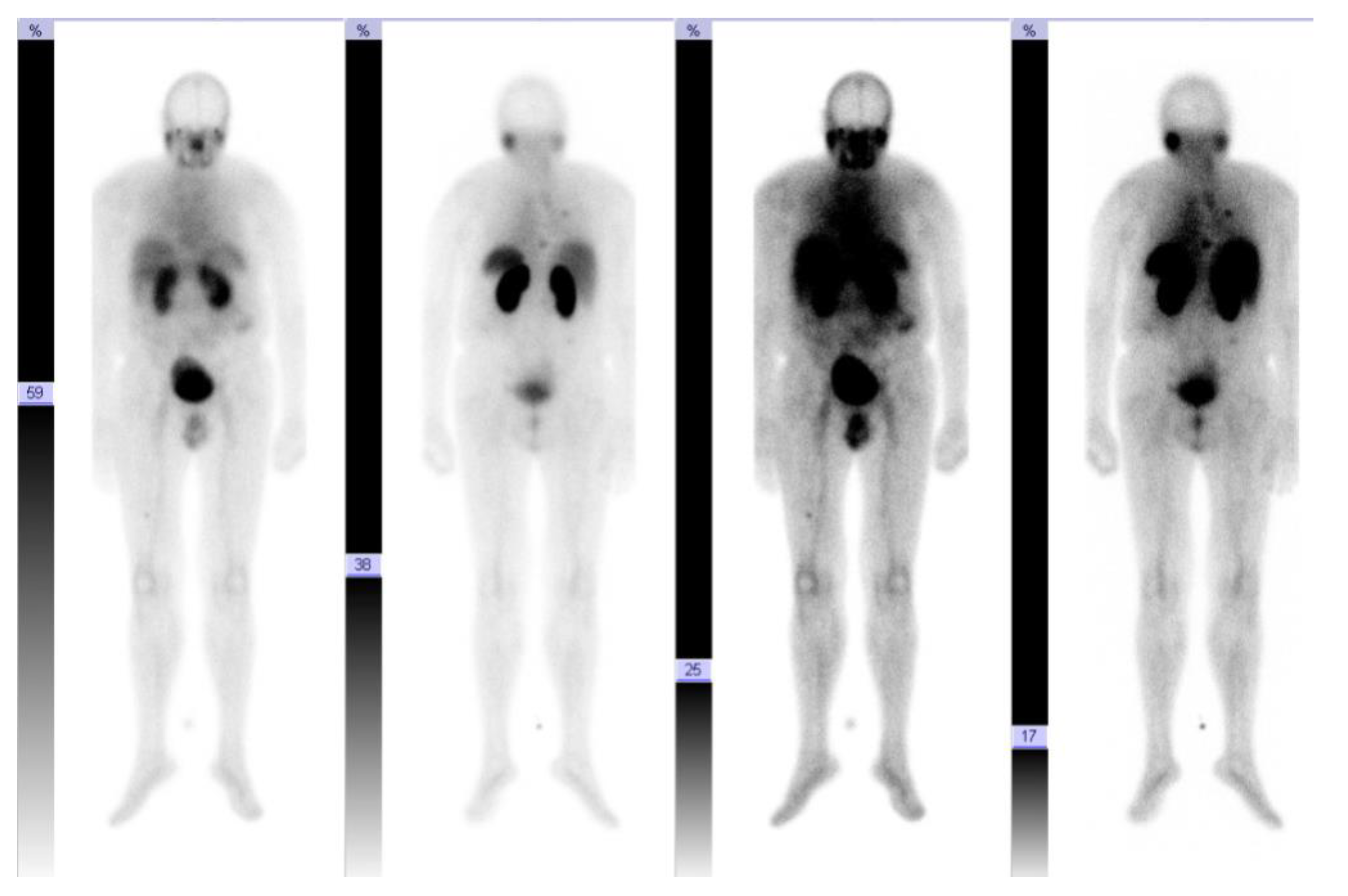
3.3.3. Setting No. 3—68Ga-PSMA-PET/CT Clearly Positive, Theranostic Approach
Patient 8: Male, PDTC, 59 Years Old at Time of Diagnosis
3.4. Imaging Findings
3.5. Correlation between the Extent of Immunohistochemical PSMA Expression in Tissue Samples and Imaging in 68GA-PSMA-PET/CT with Regard to Different Metastatic Sides of ATC and PDTC Patients
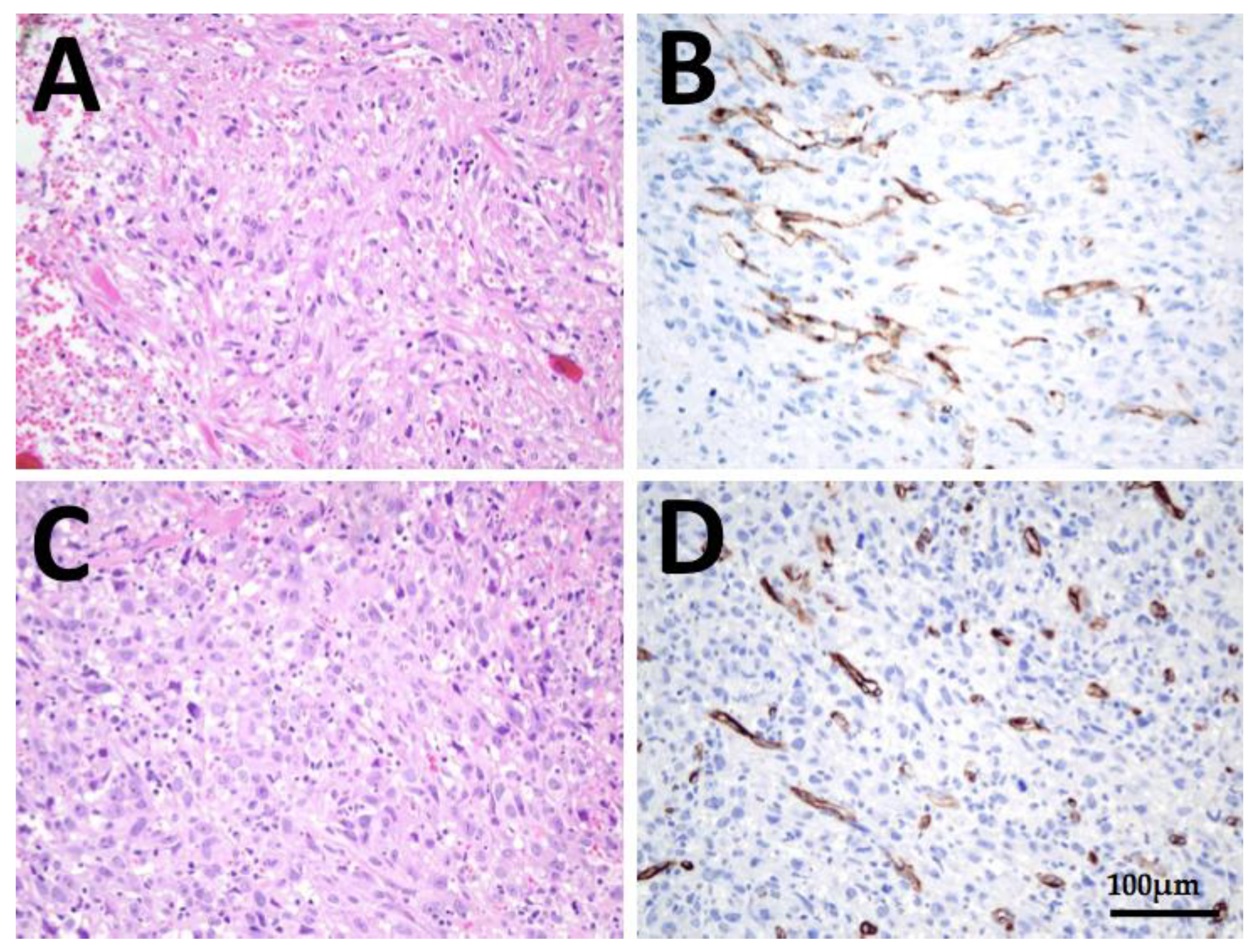
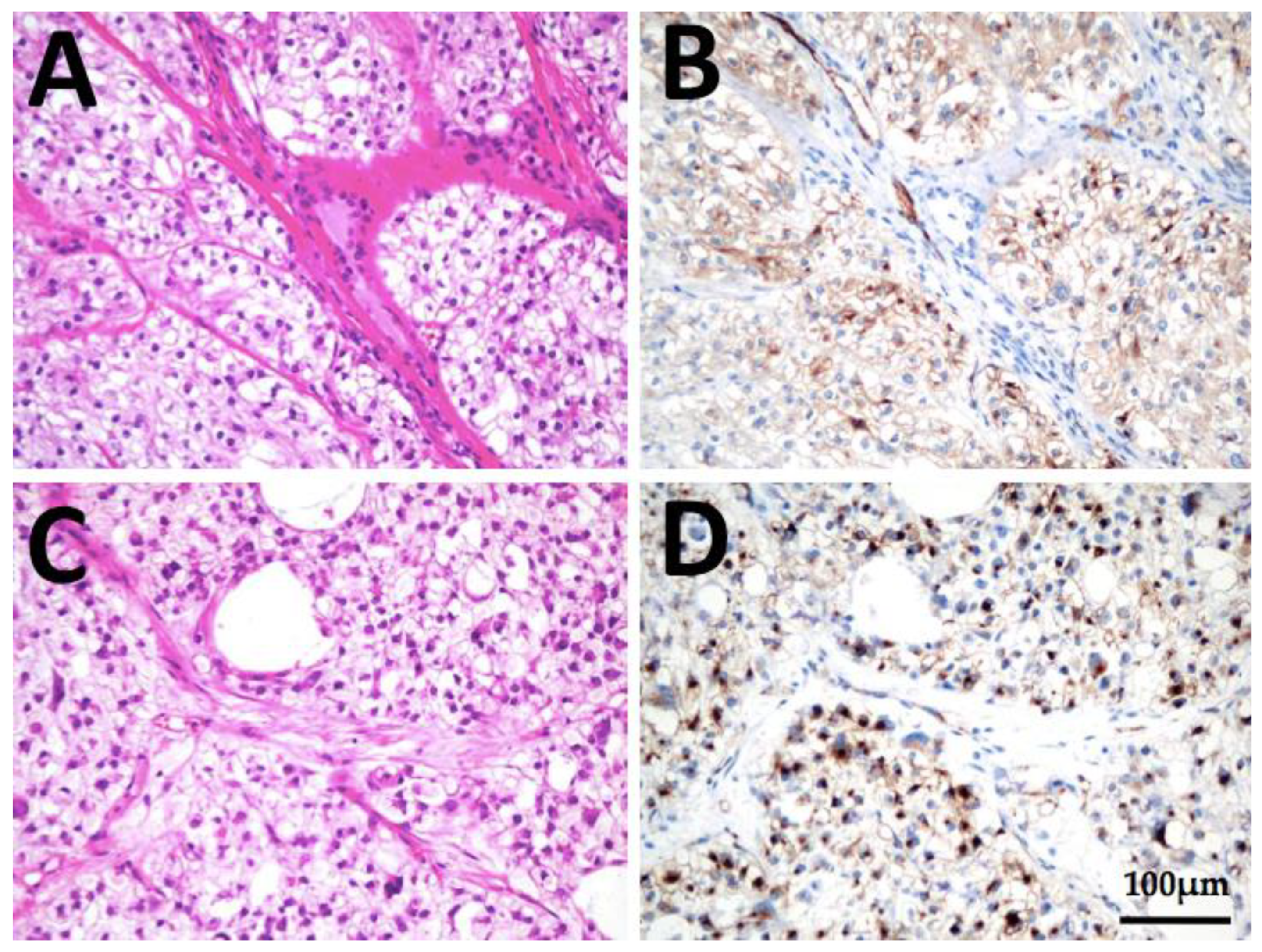
3.6. Immunohistochemical Analysis
PSMA Expression in Anaplastic and Poorly Differentiated Thyroid Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bible, K.C.; Kebebew, E.; Brierley, J.; Brito, J.P.; Cabanillas, M.E.; Clark, T.J.; Di Cristofano, A.; Foote, R.; Giordano, T.; Kasperbauer, J.; et al. 2021 American Thyroid Association Guidelines for Management of Patients with Anaplastic Thyroid Cancer. Thyroid 2021, 31, 337–386. [Google Scholar] [CrossRef]
- Catalano, M.G.; Pugliese, M.; Gargantini, E.; Grange, C.; Bussolati, B.; Asioli, S.; Bosco, O.; Poli, R.; Compagnone, A.; Bandino, A.; et al. Cytotoxic activity of the histone deacetylase inhibitor panobinostat (LBH589) in anaplastic thyroid cancer in vitro and in vivo. Int. J. Cancer 2012, 130, 694–704. [Google Scholar] [CrossRef] [PubMed]
- Are, C.; Shaha, A.R. Anaplastic Thyroid Carcinoma: Biology, Pathogenesis, Prognostic Factors, and Treatment Approaches. Ann. Surg. Oncol. 2006, 13, 453–464. [Google Scholar] [CrossRef]
- Smallridge, R.C.; Copland, J.A. Anaplastic Thyroid Carcinoma: Pathogenesis and Emerging Therapies Statement of Search Strategies Used and Sources of Information. Clin. Oncol. 2010, 22, 486–497. [Google Scholar] [CrossRef] [Green Version]
- Smallridge, R.C.; Ain, K.B.; Asa, S.L.; Bible, K.C.; Brierley, J.D.; Burman, K.D.; Kebebew, E.; Lee, N.Y.; Nikiforov, Y.E.; Rosenthal, M.S.; et al. American Thyroid Association Guidelines for Management of Patients with Anaplastic Thyroid Cancer. Thyroid 2012, 22, 1104–1139. [Google Scholar] [CrossRef] [PubMed]
- Kebebew, E.; Greenspan, F.S.; Clark, O.H.; Woeber, K.A.; McMillan, A. Anaplastic thyroid carcinoma. Cancer 2005, 103, 1330–1335. [Google Scholar] [CrossRef]
- Wächter, S.; Vorländer, C.; Schabram, J.; Mintziras, I.; Fülber, I.; Manoharan, J.; Holzer, K.; Bartsch, D.K.; Maurer, E. Anaplastic thyroid carcinoma: Changing trends of treatment strategies and associated overall survival. Eur. Arch. Otorhinolaryngol. 2020, 277, 1507–1514. [Google Scholar] [CrossRef] [PubMed]
- Sanders, E.M.; LiVolsi, V.A.; Brierley, J.; Shin, J.; Randolph, G.W. An evidence-based review of poorly differentiated thyroid cancer. World J. Surg. 2007, 31, 934–945. [Google Scholar] [CrossRef]
- Asioli, S.; Erickson, L.A.; Righi, A.; Jin, L.; Volante, M.; Jenkins, S.; Papotti, M.; Bussolati, G.; Lloyd, R.V. Poorly differentiated carcinoma of the thyroid: Validation of the Turin proposal and analysis of IMP3 expression. Mod. Pathol. 2010, 23, 1269–1278. [Google Scholar] [CrossRef] [Green Version]
- Xu, B.; Ibrahimpasic, T.; Wang, L.; Sabra, M.M.; Migliacci, J.C.; Tuttle, R.M.; Ganly, I.; Ghossein, R. Clinicopathologic Features of Fatal Non-Anaplastic Follicular Cell-Derived Thyroid Carcinomas. Thyroid 2016, 26, 1588–1597. [Google Scholar] [CrossRef] [Green Version]
- Ibrahimpasic, T.; Ghossein, R.; Shah, J.P.; Ganly, I. Poorly Differentiated Carcinoma of the Thyroid Gland: Current Status and Future Prospects. Thyroid 2019, 29, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Lin, B.; Ma, H.; Ma, M.; Zhang, Z.; Sun, Z.; Hsieh, I.-Y.; Okenwa, O.; Guan, H.; Li, J.; Lv, W. The incidence and survival analysis for anaplastic thyroid cancer: A SEER database analysis. Am. J. Transl. Res. 2019, 11, 5888–5896. [Google Scholar] [PubMed]
- Poisson, T.; Deandreis, D.; Leboulleux, S.; Bidault, F.; Bonniaud, G.; Baillot, S.; Aupérin, A.; Al Ghuzlan, A.; Travagli, J.-P.; Lumbroso, J.; et al. 18F-fluorodeoxyglucose positron emission tomography and computed tomography in anaplastic thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 2277–2285. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.D.; Ram, P.C. PET/CT staging and posttherapeutic monitoring of anaplastic thyroid carcinoma. Clin. Nucl. Med. 2007, 32, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Oriuchi, N.; Higuchi, T.; Endo, K. Review of fluorine-18-2-fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) in the follow-up of medullary and anaplastic thyroid carcinomas. Cancer Control 2005, 12, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Bogsrud, T.V.; Karantanis, D.; Nathan, M.A.; Mullan, B.P.; Wiseman, G.A.; Kasperbauer, J.L.; Reading, C.C.; Hay, I.D.; Lowe, V.J. 18F-FDG PET in the management of patients with anaplastic thyroid carcinoma. Thyroid 2008, 18, 713–719. [Google Scholar] [CrossRef]
- Ilhan, H.; la Fougère, C.; Krause, B.J. PSMA-basierte Theranostik beim Prostatakarzinom. Urologe 2020, 59, 617–625. [Google Scholar] [CrossRef]
- Emmett, L.; Willowson, K.; Violet, J.; Shin, J.; Blanksby, A.; Lee, J. Lutetium 177 PSMA radionuclide therapy for men with prostate cancer: A review of the current literature and discussion of practical aspects of therapy. J. Med. Radiat. Sci. 2017, 64, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, H.; Hänze, J.; Nimphius, W.; Verburg, F.A.; Luster, M.; Hofmann, R.; Hegele, A. Prostate specific membrane antigen (PSMA) in urothelial cell carcinoma (UCC) is associated with tumor grading and staging. J. Cancer Res. Clin. Oncol. 2020, 146, 305–313. [Google Scholar] [CrossRef]
- Verburg, F.A.; Luster, M. A new perspective for nuclear medicine: Expanding the indications for PSMA targeted imaging and therapy. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1611–1613. [Google Scholar] [CrossRef] [Green Version]
- Damle, N.A.; Bal, C.; Singh, T.P.; Gupta, R.; Reddy, S.; Kumar, R.; Tripathi, M. Anaplastic thyroid carcinoma on 68 Ga-PSMA PET/CT: Opening new frontiers. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 667–668. [Google Scholar] [CrossRef]
- Krause, B.J.; Beyer, T.; Bockisch, A.; Delbeke, D.; Kotzerke, J.; Minkov, V.; Reiser, M.; Willich, N. FDG-PET/CT in oncology. German Guideline. Nuklearmedizin 2007, 46, 291–301. [Google Scholar] [CrossRef]
- Heitkötter, B.; Steinestel, K.; Trautmann, M.; Grünewald, I.; Barth, P.; Gevensleben, H.; Bögemann, M.; Wardelmann, E.; Hartmann, W.; Rahbar, K.; et al. Neovascular PSMA expression is a common feature in malignant neoplasms of the thyroid. Oncotarget 2018, 9, 9867–9874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heitkötter, B.; Trautmann, M.; Grünewald, I.; Bögemann, M.; Rahbar, K.; Gevensleben, H.; Wardelmann, E.; Hartmann, W.; Steinestel, K.; Huss, S. Expression of PSMA in tumor neovasculature of high grade sarcomas including synovial sarcoma, rhabdomyosarcoma, undifferentiated sarcoma and MPNST. Oncotarget 2017, 8, 4268. Available online: www.impactjournals.com/oncotarget (accessed on 16 December 2016). [CrossRef] [PubMed] [Green Version]
- Backhaus, P.; Noto, B.; Avramovic, N.; Grubert, L.S.; Huss, S.; Bögemann, M.; Stegger, L.; Weckesser, M.; Schäfers, M.; Rahbar, K. Targeting PSMA by radioligands in non-prostate disease—current status and future perspectives. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 860–877. [Google Scholar] [CrossRef]
- Pfestroff, A.; Luster, M.; Jilg, C.A.; Olbert, P.J.; Ohlmann, C.H.; Lassmann, M.; Maecke, H.R.; Ezziddin, S.; Bodei, L. Radionuclide Therapy Committee of the European Association of Nuclear Medicine Current status and future perspectives of PSMA-targeted therapy in Europe: Opportunity knocks. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1971–1975. [Google Scholar] [CrossRef] [Green Version]
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schäfers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef] [Green Version]
- Lawhn-Heath, C.; Yom, S.S.; Liu, C.; Villanueva-Meyer, J.E.; Aslam, M.; Smith, R.; Narwal, M.; Juarez, R.; Behr, S.C.; Pampaloni, M.H.; et al. Gallium-68 prostate-specific membrane antigen ([68 Ga]Ga-PSMA-11) PET for imaging of thyroid cancer: A feasibility study. EJNMMI Res. 2020, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- Verma, P.; Malhotra, G.; Agrawal, R.; Sonavane, S.; Meshram, V.; Asopa, R.V. Evidence of Prostate-Specific Membrane Antigen Expression in Metastatic Differentiated Thyroid Cancer Using 68Ga-PSMA-HBED-CC PET/CT. Clin. Nucl. Med. 2018, 43, e265–e268. [Google Scholar] [CrossRef]
- de Vries, L.H.; Lodewijk, L.; Braat, A.J.A.T.; Krijger, G.C.; Valk, G.D.; Lam, M.G.E.H.; Rinkes, I.H.M.B.; Vriens, M.R.; de Keizer, B. 68Ga-PSMA PET/CT in radioactive iodine-refractory differentiated thyroid cancer and first treatment results with 177Lu-PSMA-617. EJNMMI Res. 2020, 10, 18. [Google Scholar] [CrossRef]
- Lütje, S.; Gomez, B.; Cohnen, J.; Umutlu, L.; Gotthardt, M.; Poeppel, T.D.; Bockisch, A.; Rosenbaum-Krumme, S. Imaging of Prostate-Specific Membrane Antigen Expression in Metastatic Differentiated Thyroid Cancer Using 68Ga-HBED-CC-PSMA PET/CT. Clin. Nucl. Med. 2017, 42, 20–25. [Google Scholar] [CrossRef]
- Forster, J.; Harriss-Phillips, W.; Douglass, M.; Bezak, E. A review of the development of tumor vasculature and its effects on the tumor microenvironment. Hypoxia 2017, 5, 21–32. [Google Scholar] [CrossRef] [Green Version]
- Bielenberg, D.R.; Zetter, B.R. The Contribution of Angiogenesis to the Process of Metastasis. Cancer J. 2015, 21, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Schwenck, J.; Tabatabai, G.; Skardelly, M.; Reischl, G.; Beschorner, R.; Pichler, B.; la Fougère, C. In vivo visualization of prostate-specific membrane antigen in glioblastoma. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 170–171. [Google Scholar] [CrossRef]
- Gorin, M.A.; Rowe, S.P.; Hooper, J.E.; Kates, M.; Hammers, H.-J.; Szabo, Z.; Pomper, M.G.; Allaf, M.E. PSMA-Targeted 18F-DCFPyL PET/CT Imaging of Clear Cell Renal Cell Carcinoma: Results from a Rapid Autopsy. Eur. Urol. 2017, 71, 145–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, H.; Ng, K.L.; Tse, B.W.-C.; Yeh, M.-C.; Russell, P.J.; Nelson, C.; Thomas, P.; Samaratunga, H.; Vela, I.; Gobe, G.; et al. Using prostate specific membrane antigen (PSMA) expression in clear cell renal cell carcinoma for imaging advanced disease. Pathology 2016, 48, 613–616. [Google Scholar] [CrossRef]
- Pyka, T.; Weirich, G.; Einspieler, I.; Maurer, T.; Theisen, J.; Hatzichristodoulou, G.; Schwamborn, K.; Schwaiger, M.; Eiber, M. 68Ga-PSMA-HBED-CC PET for Differential Diagnosis of Suggestive Lung Lesions in Patients with Prostate Cancer. J. Nucl. Med. 2016, 57, 367–371. [Google Scholar] [CrossRef] [Green Version]
- Froehner, M.; Kuithan, F.; Zöphel, K.; Heberling, U.; Laniado, M.; Wirth, M.P. Prostate-specific Membrane Antigen-targeted Ligand Positron Emission Tomography/Computed Tomography and Immunohistochemical Findings in a Patient with Synchronous Metastatic Penile and Prostate Cancer. Urology 2017, 101, e5–e6. [Google Scholar] [CrossRef]
- de Keizer, B.; Krijger, G.C.; Ververs, F.T.; van Es, R.J.J.; de Bree, R.; Willems, S. 68Ga-PSMA PET-CT Imaging of Metastatic Adenoid Cystic Carcinoma. Nucl. Med. Mol. Imaging 2017, 51, 360–361. [Google Scholar] [CrossRef] [Green Version]
- Haberkorn, U.; Eder, M.; Kopka, K.; Babich, J.W.; Eisenhut, M. New Strategies in Prostate Cancer: Prostate-Specific Membrane Antigen (PSMA) Ligands for Diagnosis and Therapy. Clin. Cancer Res. 2016, 22, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Sollini, M.; di Tommaso, L.; Kirienko, M.; Piombo, C.; Erreni, M.; Lania, A.G.; Erba, P.A.; Antunovic, L.; Chiti, A. PSMA expression level predicts differentiated thyroid cancer aggressiveness and patient outcome. EJNMMI Res. 2019, 9, 93. [Google Scholar] [CrossRef] [Green Version]
- Woythal, N.; Arsenic, R.; Kempkensteffen, C.; Miller, K.; Janssen, J.-C.; Huang, K.; Makowski, M.R.; Brenner, W.; Prasad, V. Immunohistochemical Validation of PSMA Expression Measured by 68Ga-PSMA PET/CT in Primary Prostate Cancer. J. Nucl. Med. 2018, 59, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Holzgreve, A.; Biczok, A.; Ruf, V.C.; Liesche-Starnecker, F.; Steiger, K.; Kirchner, M.A.; Unterrainer, M.; Mittlmeier, L.; Herms, J.; Schlegel, J.; et al. PSMA Expression in Glioblastoma as a Basis for Theranostic Approaches: A Retrospective, Correlational Panel Study Including Immunohistochemistry, Clinical Parameters and PET Imaging. Front. Oncol. 2021, 11, 861. [Google Scholar] [CrossRef]
- de Galiza Barbosa, F.; Queiroz, M.A.; Nunes, R.F.; Costa, L.B.; Zaniboni, E.C.; Marin, J.F.G.; Cerri, G.G.; Buchpiguel, C.A. Nonprostatic diseases on PSMA PET imaging: A spectrum of benign and malignant findings. Cancer Imaging 2020, 20, 23. [Google Scholar] [CrossRef]
- Heydarzadeh, S.; Moshtaghie, A.A.; Daneshpoor, M.; Hedayati, M. Regulators of glucose uptake in thyroid cancer cell lines. Cell Commun. Signal. 2020, 18, 83. [Google Scholar] [CrossRef]
- Kim, Y.W.; Do, I.G.; Park, Y.-K. Expression of the GLUT1 glucose transporter, p63 and p53 in thyroid carcinomas. Pathol.-Res. Pract. 2006, 202, 759–765. [Google Scholar] [CrossRef]
- Schönberger, J.; Rüschoff, J.; Grimm, D.; Marienhagen, J.; Rümmele, P.; Meyringer, R.; Kossmehl, P.; Hofstaedter, F.; Eilles, C. Glucose Transporter 1 Gene Expression is Related to Thyroid Neoplasms with an Unfavorable Prognosis: An Immunohistochemical Study. Thyroid 2002, 12, 747–754. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age at Diagnosis (Years) | Year of Diagnosis | Tumor-Type | TNM Stage 1 | UICC Stage 1 | Treatment History |
|---|---|---|---|---|---|---|---|
| 1 | M | 59 | 2020 | ATC | pT4a pN0 M0 | IVB | Surgery of the thyroid gland (2020) Radiochemotherapy (2020) Targeted therapy (Pembrolizumab + Lenvatinib) (2020/2021) |
| 2 | M | 47 | 2020 | ATC | pT4a pN1 M1 | IVC | Surgery of the thyroid gland (2020) Radiochemotherapy (2020) Targeted therapy (Pembrolizumab + Lenvatinib) (2020/2021) |
| 3 | F | 44 | 2007 | PDTC | pT3a pN1 M0 | II | Two-stage surgery of the thyroid gland (2007) Radioiodine therapy (3,7 GBq I-131) (2007) Surgery of mediastinal lymph node metastases (2007) Three further radioiodine therapies (cumulative 16,9 GBq I-131) (last 2009) Twofold resection of lung metastases (2012) Fifth radioiodine therapy (5,5 GBq I-131) (2012) mKI therapy (Lenvatinib) (2019) |
| 4 | M | 51 | 2015 | PDTC | pT4a pN1 M0 | II | Two-stage surgery of the thyroid gland (2015) Radioiodine therapy (3,6 GBq I-131) (2015) Surgery vertebral metastasis (2016) Radioiodine therapy (7,4 GBq I-131) (2017) mKI therapy (Lenvatinib) (2018) |
| 5 | M | 65 | 2014 | PDTC | pT0 cN1 M1 | IVB | Surgery of the thyroid gland (oncocytic adenoma) (2010) Surgery of vertebral metastasis (2014) Residual thyroidectomy without tumor detection (2014) Radioiodine therapy (7,4 GBq I-131) (2015) mKI therapy (Sorafenib) (2015) mKI therapy (Lenvatinib) (2015) External beam radiation of osseous metastases (ribs, os ilium, femur right) (2015) Surgery of vertebral metastasis (2017) mKI therapy (Pazopanib) (2017) mKI therapy (Lenvatinib) (2017) COSMIC study inclusion 2 (2020) |
| 6 | M | 70 | 2010 | PDTC | pT2 pN0 M0 | I | Two-stage surgery of the thyroid gland (2010) Three cycles of radioiodine therapy (cumulative 14,4 GBq I-131) (last 2011) mKI therapy (Sorafenib) (2015) mKI therapy (Lenvatinib) (2016) mKI therapy (Sorafenib) (2017) mKI therapy (Pazopanib) (2017) |
| 7 | F | 61 | 2013 | PDTC | pT3a pN1 M1 | IVB | Surgery of the thyroid gland (2013) Twofold radioiodine therapy (cumulative 9,9 GBq I-131) (2013) Surgery of cervical lymph node metastasis (2014) Lutetium-177-DOTATATE therapy (2014) mKI therapy (Sorafenib) (2014) External beam therapy of vertebral and cervical lymph node metastases (2016) mKI therapy (Lenvatinib) (2016) Surgery of brain metastases (2018) |
| 8 | M | 59 | 2015 | PDTC | pT0 cN0 M1 | IVB | Surgery of the thyroid gland (2011) Surgery of vertebral metastasis (2015) Residual thyroidectomy without tumor detection (2015) Radioiodine therapy (14,9 GBq I-131) (2015) Two cycles of Lutetium-177-PSMA therapy (cumulativ 13,7 GBq) (2017) mKI therapy (Lenvatinib) (2018) COSMIC study 2 inclusion (2020) |
| Patient | 18FDG-PET/CT and 68Ga-PSMA-PET/CT Results | PSMA Expression | ||||||
|---|---|---|---|---|---|---|---|---|
| Diagnosis of Primary Tumor | Year of Scan | Interval between 18FDG-PET/CT and 68Ga-PSMA- PET/CT (Days) | Tumor/Metastases Locations Number of Lesions (N) Median Size, cm (Range) | FDG- PET/CT Median SUVmax (Range) | PSMA- PET/CT Median SUVmax (Range) | Tumor Samples | Extend of PSMA- Expression | |
| 1 | 2020 | PSMA: 2020 FDG: 2020 | 1 | TB 1 (local recurrence) (n = 1) 1.9 | 16.3 | 2.5 | Primary tumor Soft tissue surrounding thyroid gland | Strong expression Strong expression |
| LN2 (mediastinal) (n = 1) 2.2 | 2.7 | 3.3 | ||||||
| PM 3 (n = 7) 0.7 (0.3–1.2) | 2.7 (1.5–7.9) | 1.3 (0.6–2.6) | ||||||
| 2 | 2020 | PSMA: 2020 FDG: 2020 | 1 | PM 3 (n = 2) 2.1; 2.2 | 21.2 (14.1; 28.3) | 3.25 (4.0; 2.5) | Primary tumor Pulmonary metastasis | Strong expression Strong expression |
| 3 | 2007 | PSMA: 2017 FDG: 2016 | 83 | PM 3 (n > 10) 1.0 (0.5–1.1) | 12.6 (6.6–25.3) | 3.4 (2.0–4.3) | Primary tumor Lymph node metastasis (cervical) Pulmonary metastasis | Low expression Low expression Low expression |
| 4 | 2015 | PSMA: 2017 FDG: 2016 | 232 | OM 4 (vertebra) (n = 1) 1.1 | 7.4 | Not per-formed before surgery | Osseous metastases of the vertebra | Strong expression |
| LN2 (mediastinal) (n = 1) 0.8 | 5.6 | 2.1 | ||||||
| 5 | 2014 | PSMA: 2017 FDG: 2017 | 40 | OM 4 (vertebra) (n = 1) 4.2 | 17.9 | 3.7 | Osseous metastases of the vertebra | Strong expression |
| OM 4 (n > 10) 4.2 (2.7–6.1) | 17.9 (9.9–31.2) | 3.7 (1.8–4.2) | ||||||
| TB 1 (local recurrence) (n = 1) 10.7 | 19.1 | 2.4 | ||||||
| 6 | 2010 | PSMA: 2017 FDG: 2017 | 171 | TB1 (tumor recurrence) (n = 1) 10.7 | 67.9 | 4.2 | Tumor recurrence Lymph node metastasis (cervical) | Low expression Low expression |
| LN 2 cervical (n = 1) 1.9 mediastinal (n = 1) 6.7 | 48.4 55.9 | 4.1 5.7 | ||||||
| PM 3 (n > 10) 1.9 (1.6–3.6) | 35.4 (29.4–51.5) | 3.8 (2.5–6.3) | ||||||
| 7 | 2013 | PSMA: 2017 FDG: 2016 | 76 | CM 5 (n = 1) 2.9 | 31.4 | 12.3 | Primary tumor Lymph node metastasis (cervical) | Strong expression Strong expression |
| LN 2 cervical (n = 1) 2.0 mediastinal (n = 2) (3.6; 1.4) inguinal (n = 1) 5.4 | 32.1 30.85 (36.4; 25.3) 35.2 | 7.4 8.2 (6.3; 10.1) 6.2 | ||||||
| PM 3 (n > 10) 1.1 (1.0–1.8) | 12.5 (11.7–14.1) | 3.3 (2.1–4.0) | ||||||
| ST 6 (thoracic wall) (n = 1) 2.1 | 31.0 | 4.3 | ||||||
| OM 4 (Os occipital) (n = 1) 2.9 | 16.9 | 7.2 | ||||||
| 8 | 2015 | PSMA: 2016 FDG: 2016 | 81 | OM 4 (n = 4) 1.25 (0 *–1.6) | 2.3 (1.2–2.7) | 5.55 (2.9–9.0) | No tissue sample of this patient was available | |
| Disease Location | 68Ga-PSMA- PET/CT Median SUVmax (Range) * | Clearly (Discreet) PSMA-Positive Lesions/ Total Rated Lesions | 18FDG-PET/CT Median SUVmax (Range) * | Clearly (Discreet) FDG-Positive Lesions/ Total Rated Lesions 1 | Number of Clearly Dis-Cordant Lesions 2/Total Rated Lesions 1 | Description of Clearly Discordant Lesions 1 |
|---|---|---|---|---|---|---|
| ATC | ||||||
| Mediastinal lymph node | 3.3 | 0 (1)/1 | 2.7 | 0 (1)/1 | 0/1 | - |
| Pulmonary metastases | 1.3 (0.6–4) | 0 (0)/9 | 5.0 (1.5–28.3) | 9 (0)/9 | 9/9 | 9 FDG+, PSMA− |
| Local tumor recurrence/ thyroid bed lesions | 2.5 | 0 (0)/1 | 16.3 | 1 (0)/1 | 1/1 | 1 FDG+, PSMA− |
| PDTC | ||||||
| Osseous metastases | 3.85 (1.8–9.0) | 2 (3)/10 | 9.9 (1.2–31.2) | 6 (0)/10 | 7/10 3 | 2 PSMA+, FDG− 5 FDG+, PSMA- |
| Cervical lymph nodes | 5.75 (4.1–7.4) | 0 (1)/2 | 40.25 (32.1–48.4) | 2 (0)/2 | 1/2 4 | 1 FDG+, PSMA− |
| Mediastinal lymph nodes | 6.0 (2.1–10.1) | 1 (1)/4 | 30.85 (5.6–55.9) | 4 (0)/4 | 2/4 5 | 2 FDG+, PSMA− |
| Pulmonary metastases | 3.45 (2.0–6.3) | 0 (0)/15 | 15.5 (6.6–51.5) | 15 (0)/15 | 15/15 | 15 FDG+, PSMA− |
| Local tumor recurrence/thyroid bed lesions | 3.3 (2.4–4.2) | 0 (0)/2 | 43.5 (19.1–67.9) | 2 (0)/2 | 2/2 | 2 FDG+, PSMA− |
| Cerebral metastases | 12.3 | 1 (0)/1 | 31.4 | 1 (0)/1 | 0/1 | - |
| Soft tissue/others (inguinal lymph node metastasis) | 5.25 (4.3–6.2) | 0 (1)/2 | 33.1 (31–35.2) | 2 (0)/2 | 1/2 4 | 1 FDG+, PSMA− |
| Immunohistochemical Analysis of ATC and PDTC Tissue Samples 1 | Imaging Analysis 2 | |||||
|---|---|---|---|---|---|---|
| Metastatic Side | No PSMA Expression | PSMA-Labelling Index 1 “Low Expression” | PSMA-Labelling Index 2 “Strong Expression” | PSMA-Labelling Index 3 “Strong Expresion” | Clearly PSMA-Positive Lesions/Total Rated Lesions | Discreet PSMA-Positive Lesions/Total Rated Lesions |
| ATC | ||||||
| Pulmonary/pleural metastases (n = 1) | 0 | 0 | 1 | 0 | 0/2 | 0/2 |
| PDTC | ||||||
| Cervical lymph node metastases (n = 2) | 0 | 1 | 1 | 0 | 0/2 | 1/2 |
| Pulmonary metastases (n = 1) | 0 | 1 | 0 | 0 | 0/>10 | 0/>10 |
| Local recurrence (n = 1) | 0 | 1 | 0 | 0 | 0/1 | 0/1 |
| Osseous metastases (n = 1) | 0 | 0 | 1 | 0 | 0/>10 | 0/>10 |
| Disease Location | No of Total Tissue Samples | Tissue Samples without Any PSMA Expression | Tissue Samples with “Low Expression“ 1, PSMA-Labelling Index 1 | Tissue Samples with “Strong Expression“ 2, PSMA-Labelling Index 2 | Tissue Samples with “Strong Expression” 2, PSMA-Labelling Index 3 |
|---|---|---|---|---|---|
| ATC | |||||
| Primary tumor | 22 | 1 | 3 | 18 | 0 |
| Lymph node metastases | 5 | 1 | 1 | 3 | 0 |
| Pulmonary/pleural metastases | 4 | 0 | 1 | 3 | 0 |
| Soft tissue—surrounding thyroid gland—presternal metastasis | 7 1 | 1 0 | 3 1 | 3 0 | 0 0 |
| PDTC | |||||
| Primary tumor | 6 | 0 | 1 | 4 | 1 |
| Lymph node metastases | 6 | 0 | 3 | 2 | 1 |
| Pulmonary metastases | 3 | 0 | 1 | 2 | 0 |
| Others—renal metastasis—local recurrence | 1 2 | 0 0 | 0 1 | 1 1 | 0 0 |
| Osseous metastases | 4 | 1 | 0 | 3 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wächter, S.; Di Fazio, P.; Maurer, E.; Manoharan, J.; Keber, C.; Pfestroff, A.; Librizzi, D.; Bartsch, D.K.; Luster, M.; Eilsberger, F. Prostate-Specific Membrane Antigen in Anaplastic and Poorly Differentiated Thyroid Cancer—A New Diagnostic and Therapeutic Target? Cancers 2021, 13, 5688. https://doi.org/10.3390/cancers13225688
Wächter S, Di Fazio P, Maurer E, Manoharan J, Keber C, Pfestroff A, Librizzi D, Bartsch DK, Luster M, Eilsberger F. Prostate-Specific Membrane Antigen in Anaplastic and Poorly Differentiated Thyroid Cancer—A New Diagnostic and Therapeutic Target? Cancers. 2021; 13(22):5688. https://doi.org/10.3390/cancers13225688
Chicago/Turabian StyleWächter, Sabine, Pietro Di Fazio, Elisabeth Maurer, Jerena Manoharan, Corinna Keber, Andreas Pfestroff, Damiano Librizzi, Detlef K. Bartsch, Markus Luster, and Friederike Eilsberger. 2021. "Prostate-Specific Membrane Antigen in Anaplastic and Poorly Differentiated Thyroid Cancer—A New Diagnostic and Therapeutic Target?" Cancers 13, no. 22: 5688. https://doi.org/10.3390/cancers13225688