
Cirrhosis, Age, and Liver Stiffness-Based Models Predict Hepatocellular Carcinoma in Asian Patients with Chronic Hepatitis B

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Statistics
3. Results
3.1. Study Cohort and Patient Characteristics
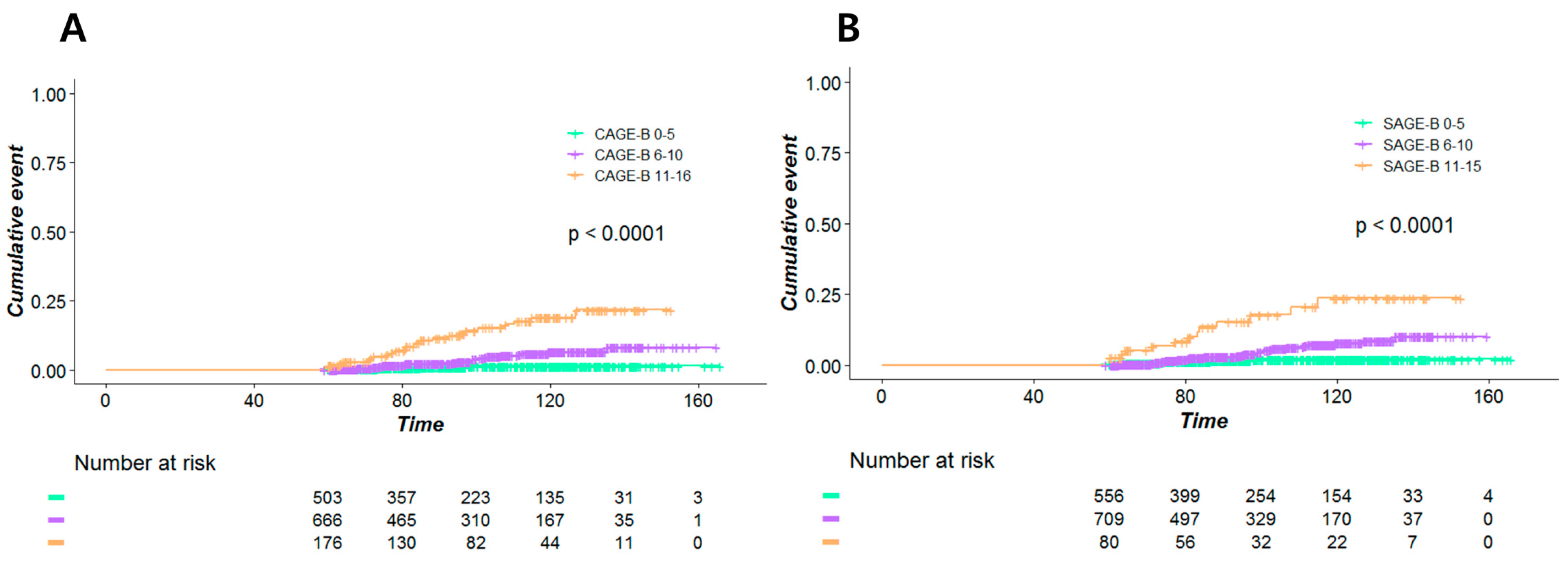
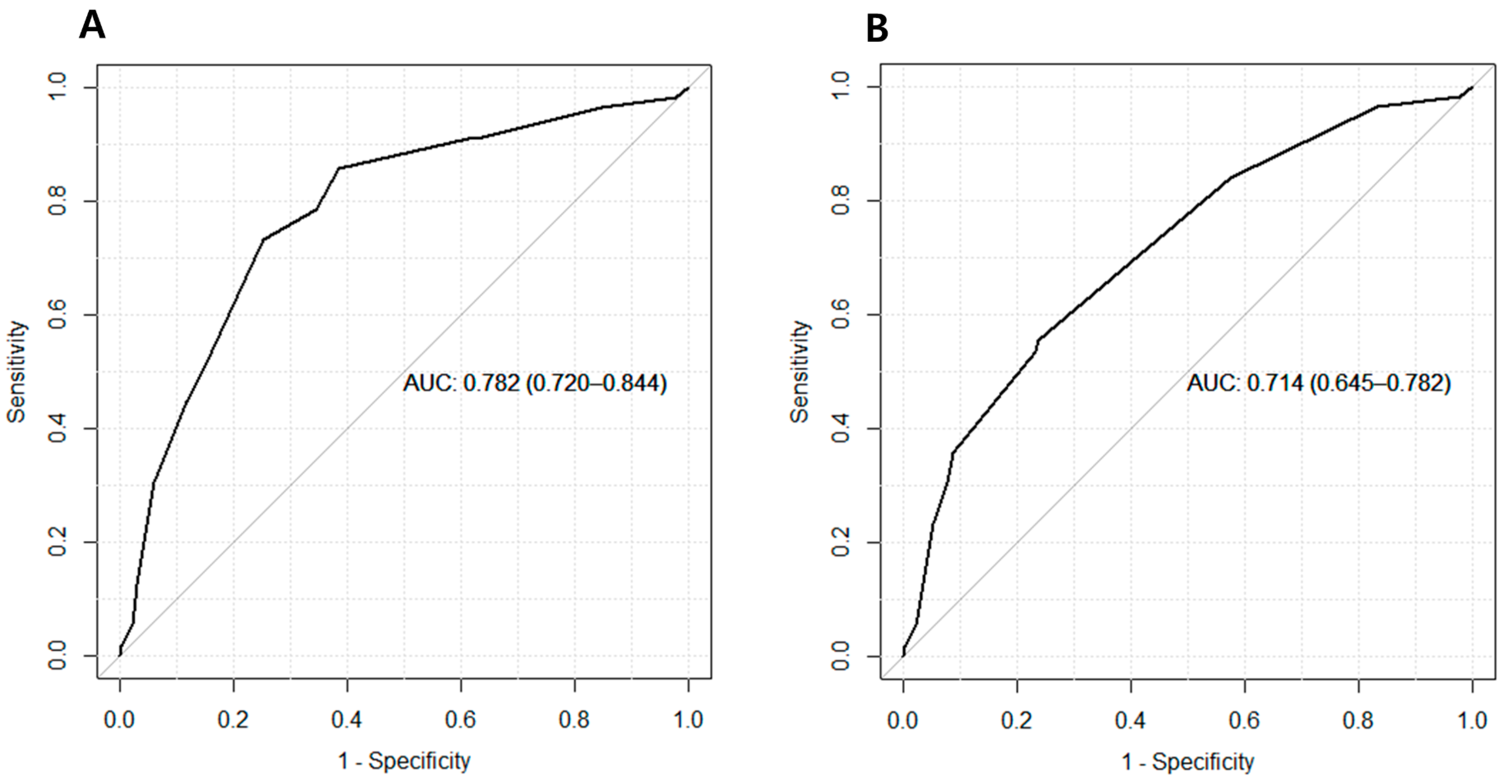
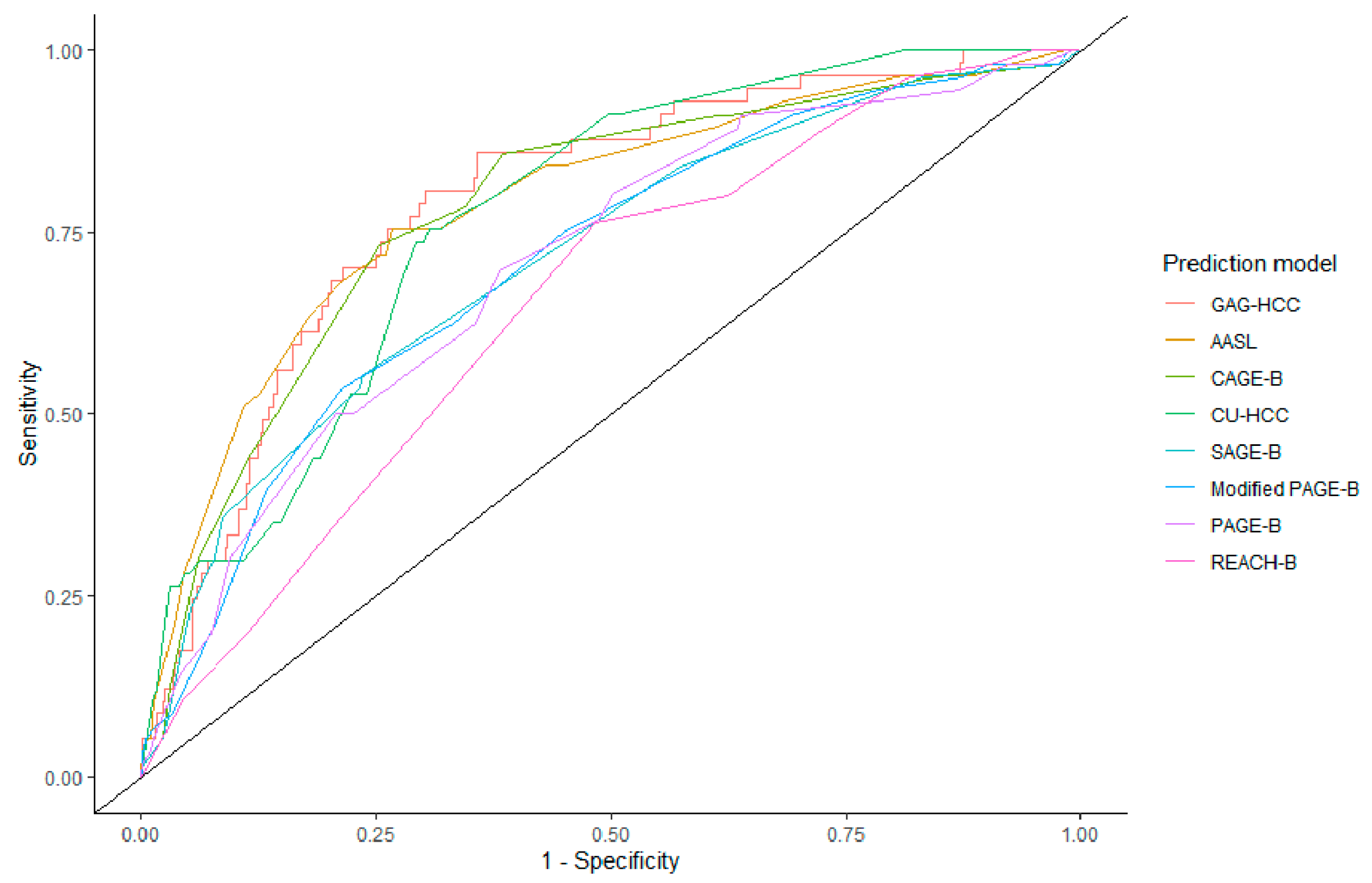
3.2. Performance of CAGE-B, SAGE-B, and Other Prediction Models
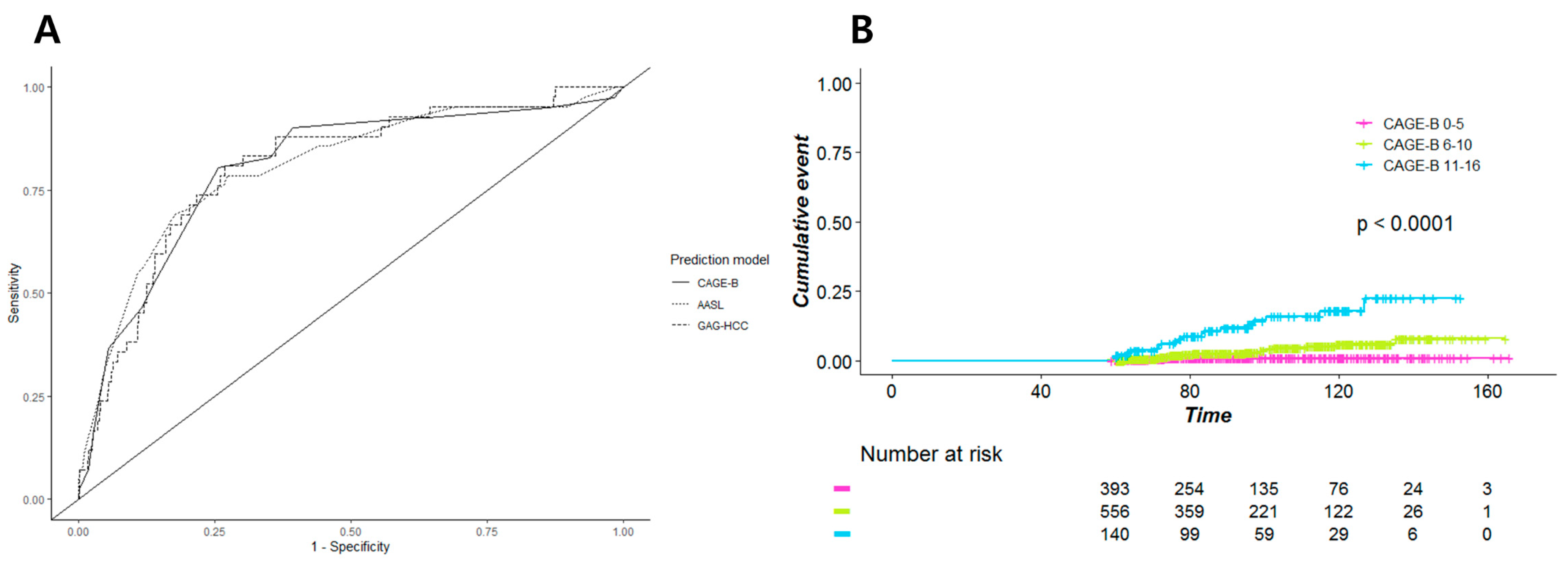
3.3. Subgroup Analysis
3.3.1. Patients without Treatment Modification
3.3.2. Male Patients
3.3.3. Patients with Hepatic Steatosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Korean Association for the Study of the Liver (KASL). Kasl clinical practice guidelines for management of chronic hepatitis b. Clin. Mol. Hepatol. 2019, 25, 93–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis b: Aasld 2018 hepatitis b guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridis, G.V.; Lampertico, P.; Manolakopoulos, S.; Lok, A. Incidence of hepatocellular carcinoma in chronic hepatitis b patients receiving nucleos(t)ide therapy: A systematic review. J. Hepatol. 2010, 53, 348–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papatheodoridis, G.V.; Chan, H.L.; Hansen, B.E.; Janssen, H.L.; Lampertico, P. Risk of hepatocellular carcinoma in chronic hepatitis b: Assessment and modification with current antiviral therapy. J. Hepatol. 2015, 62, 956–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. Easl 2017 clinical practice guidelines on the management of hepatitis b virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.L.; Kao, J.H. Review article: The prevention of hepatitis b-related hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2018, 48, 5–14. [Google Scholar] [CrossRef] [Green Version]
- Papatheodoridis, G.V.; Sypsa, V.; Dalekos, G.; Yurdaydin, C.; van Boemmel, F.; Buti, M.; Goulis, J.; Calleja, J.L.; Chi, H.; Manolakopoulos, S.; et al. Eight-year survival in chronic hepatitis b patients under long-term entecavir or tenofovir therapy is similar to the general population. J. Hepatol. 2018, 68, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Ha, Y.; Chon, Y.E.; Kim, M.N.; Lee, J.H.; Hwang, S.G. Hepatocellular carcinoma and death and transplantation in chronic hepatitis b treated with entecavir or tenofovir disoproxil fumarate. Sci. Rep. 2020, 10, 13537. [Google Scholar] [CrossRef]
- Wiersma, S.T.; McMahon, B.; Pawlotsky, J.M.; Thio, C.L.; Thursz, M.; Lim, S.G.; Ocama, P.; Esmat, G.; Maimuna, M.; Bell, D. Treatment of chronic hepatitis b virus infection in resource-constrained settings: Expert panel consensus. Liver Int. 2011, 31, 755–761. [Google Scholar] [CrossRef]
- Udompap, P.; Tanwandee, T.; Gani, R. Affordability of antiviral therapy in asia-pacific countries and its impact on public health outcomes. Clin. Liver Dis. 2020, 16, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Papatheodoridis, G.V.; Sypsa, V.; Dalekos, G.N.; Yurdaydin, C.; Van Boemmel, F.; Buti, M.; Calleja, J.L.; Chi, H.; Goulis, J.; Manolakopoulos, S.; et al. Hepatocellular carcinoma prediction beyond year 5 of oral therapy in a large cohort of caucasian patients with chronic hepatitis b. J. Hepatol. 2020, 72, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.H.; Suh, Y.J.; Jin, Y.J.; Heo, N.Y.; Jang, J.W.; You, C.R.; An, H.Y.; Lee, J.W. Prediction model for hepatocellular carcinoma risk in treatment-naive chronic hepatitis b patients receiving entecavir/tenofovir. Eur. J. Gastroenterol. Hepatol. 2019, 31, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.; Chan, S.L.; Mo, F.; Chan, T.C.; Loong, H.H.; Wong, G.L.; Lui, Y.Y.; Chan, A.T.; Sung, J.J.; Yeo, W.; et al. Clinical scoring system to predict hepatocellular carcinoma in chronic hepatitis b carriers. J. Clin. Oncol. 2010, 28, 1660–1665. [Google Scholar] [CrossRef] [Green Version]
- Yuen, M.F.; Tanaka, Y.; Fong, D.Y.; Fung, J.; Wong, D.K.; Yuen, J.C.; But, D.Y.; Chan, A.O.; Wong, B.C.; Mizokami, M.; et al. Independent risk factors and predictive score for the development of hepatocellular carcinoma in chronic hepatitis b. J. Hepatol. 2009, 50, 80–88. [Google Scholar] [CrossRef]
- Papatheodoridis, G.; Dalekos, G.; Sypsa, V.; Yurdaydin, C.; Buti, M.; Goulis, J.; Calleja, J.L.; Chi, H.; Manolakopoulos, S.; Mangia, G.; et al. Page-b predicts the risk of developing hepatocellular carcinoma in caucasians with chronic hepatitis b on 5-year antiviral therapy. J. Hepatol. 2016, 64, 800–806. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, Y.D.; Lee, M.; Jun, B.G.; Kim, T.S.; Suk, K.T.; Kang, S.H.; Kim, M.Y.; Cheon, G.J.; Kim, D.J.; et al. Modified page-b score predicts the risk of hepatocellular carcinoma in asians with chronic hepatitis b on antiviral therapy. J. Hepatol. 2018, 69, 1066–1073. [Google Scholar] [CrossRef]
- Yang, H.I.; Yuen, M.F.; Chan, H.L.; Han, K.H.; Chen, P.J.; Kim, D.Y.; Ahn, S.H.; Chen, C.J.; Wong, V.W.; Seto, W.K. Risk estimation for hepatocellular carcinoma in chronic hepatitis b (reach-b): Development and validation of a predictive score. Lancet Oncol. 2011, 12, 568–574. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Müller, M. Proc: An open-source package for r and s+ to analyze and compare roc curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Ganne-Carrié, N.; Ziol, M.; de Ledinghen, V.; Douvin, C.; Marcellin, P.; Castera, L.; Dhumeaux, D.; Trinchet, J.C.; Beaugrand, M. Accuracy of liver stiffness measurement for the diagnosis of cirrhosis in patients with chronic liver diseases. Hepatology 2006, 44, 1511–1517. [Google Scholar] [CrossRef]
- Lo, R.C.; Kim, H. Histopathological evaluation of liver fibrosis and cirrhosis regression. Clin. Mol. Hepatol. 2017, 23, 302–307. [Google Scholar] [CrossRef] [Green Version]
- De Ledinghen, V.; Vergniol, J. Transient elastography (fibroscan). Gastroenterol. Clin. Biol. 2008, 32, 58–67. [Google Scholar] [CrossRef]
- Foucher, J.; Chanteloup, E.; Vergniol, J.; Castera, L.; Le Bail, B.; Adhoute, X.; Bertet, J.; Couzigou, P.; de Ledinghen, V. Diagnosis of cirrhosis by transient elastography (fibroscan): A prospective study. Gut 2006, 55, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.L.; Wong, M.L.; Hui, A.Y.; Hung, L.C.; Chan, F.K.; Sung, J.J. Hepatitis b virus genotype c takes a more aggressive disease course than hepatitis b virus genotype b in hepatitis b e antigen-positive patients. J. Clin. Microbiol. 2003, 41, 1277–1279. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.L.; Hui, A.Y.; Wong, M.L.; Tse, A.M.; Hung, L.C.; Wong, V.W.; Sung, J.J. Genotype c hepatitis b virus infection is associated with an increased risk of hepatocellular carcinoma. Gut 2004, 53, 1494–1498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, J.H.; Park, S.Y.; Son, W.J.; Shin, H.J.; Lee, H.; Lee, H.W.; Lee, J.S.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; et al. External validation of cage-b and sage-b scores for asian chronic hepatitis b patients with well-controlled viremia by antivirals. J. Viral Hepat. 2021, 28, 951–958. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 1557) | No HCC (n = 1500) | HCC (n = 57) | p-Value |
|---|---|---|---|---|
| Baseline | ||||
| Age, years | 46.6 ± 10.6 | 46.4 ± 10.6 | 50.9 ± 9.6 | 0.002 |
| Sex | 0.21 | |||
| Male | 993 (63.8) | 952 (63.5) | 41 (71.9) | |
| Female | 564 (36.2) | 548 (36.5) | 16 (28.1) | |
| Cirrhosis | 431 (27.7) | 388 (25.9) | 43 (75.4) | <0.001 |
| LSM, kPa | 7.4 (4.8, 12.3) | 7.3 (4.8, 12.0) | 17.9 (10.9, 26.3) | <0.001 |
| Initial nucleos(t)ide analog | 0.001 | |||
| Entecavir | 868 (55.7) | 824 (54.9) | 44 (77.2) | |
| Tenofovir | 689 (44.3) | 676 (45.1) | 13 (22.8) | |
| Albumin, g/dL | 4.2 (3.8, 4.4) | 4.2 (3.8, 4.4) | 4.0 (3.3, 4.3) | 0.004 |
| Fasting glucose, mg/dL | 98.0 (91.0, 108.0) | 98.0 (91.0, 108.0) | 105.0 (90.8, 120.5) | 0.09 |
| Creatinine, mg/dL | 0.9 (0.7, 1.0) | 0.9 (0.7, 1.0) | 0.9 (0.7, 1.0) | 0.78 |
| Total bilirubin, mg/dL | 0.9 (0.6, 1.2) | 0.8 (0.6, 1.2) | 1.1 (0.7, 1.7) | 0.001 |
| AST, IU/L | 53.0 (30.0, 106.8) | 53.0 (30.0, 107.0) | 53.0 (43.0, 107.5) | 0.15 |
| AST in patients with AST > 40 IU/L | 86.0 (56.0, 157.5) | 86.5 (57.0, 159.0) | 57.0 (47.0, 133.0) | 0.016 |
| ALT, IU/L | 57.0 (28.0, 130.0) | 58.0 (27.0, 130.0) | 51.0 (37.5, 112.5) | 0.69 |
| ALT in patients with AST > 40 IU/L | 105.0 (62.0, 202.0) | 106.5 (63.0, 202.8) | 76.0 (47.8, 146.0) | 0.017 |
| ALP, IU/L | 93.0 (67.0, 155.8) | 92.5 (67.0, 153.8) | 116.0 (64.0, 184.0) | 0.26 |
| GGT, U/L | 46.0 (23.0, 109.0) | 44.5 (22.0, 108.0) | 67.0 (36.5, 128.0) | 0.011 |
| Platelet, ×1000/mm3 | 166 (126, 204) | 168 (128, 206) | 127 (80, 160) | <0.001 |
| Prothrombin time, INR | 1.1 (1.0, 1.1) | 1.1 (1.0, 1.1) | 1.1 (1.0, 1.4) | 0.001 |
| HBeAg positivity | 830 (60.5) | 802 (60.8) | 28 (50.9) | 0.16 |
| HBV DNA, log IU/mL | 5.8 (3.5, 7.4) | 5.8 (3.4, 7.4) | 6.1 (4.7, 7.2) | 0.23 |
| HBV DNA in patients with detectable HBV DNA, log IU/mL | 6.1 (4.4, 7.6) | 6.2 (4.4, 7.6) | 6.4 (4.8, 7.2) | 0.79 |
| At 5 years of treatment | ||||
| LSM, kPa | 4.9 (4.0, 6.7) | 4.8 (3.9, 6.4) | 8.8 (6.4, 13.0) | <0.001 |
| AST, IU/L | 24.0 (20.0, 29.0) | 24.0 (20.0, 29.0) | 28.0 (22.0, 37.5) | 0.001 |
| ALT, IU/L | 20.0 (14.0, 28.0) | 20.0 (14.0, 28.0) | 22.0 (16.5, 32.5) | 0.12 |
| Platelet, ×1000/mm3 | 189 (151, 228) | 190 (154, 230) | 144 (94, 174) | <0.001 |
| HBeAg seroconversion | 319 (41.3) | 304 (40.8) | 15 (55.6) | 0.16 |
| Undetectable HBV DNA | 1393 (91.0) | 1345 (91.3) | 48 (84.2) | 0.09 |
| Follow-up duration, months | 92.8 (72.7, 119.3) | 92.0 (72.7, 118.7) | 113.6 (85.7, 129.6) | <0.001 |
| CAGE-B | SAGE-B | AASL | CU-HCC | GAG-HCC | PAGE-B | Modified PAGE-B | REACH-B | |
|---|---|---|---|---|---|---|---|---|
| AUC (95% CI) | 0.78 (0.72–0.84) | 0.71 (0.65–0.78) | 0.79 (0.72–0.85) | 0.77 (0.72–0.82) | 0.79 (0.74–0.85) | 0.71 (0.64–0.77) | 0.71 (0.64–0.78) | 0.65 (0.59–0.72) |
| Sensitivity (LL–UL) | 0.73 (0.60–0.83) | 0.55 (0.42–0.68) | 0.75 (0.63–0.86) | 0.75 (0.63–0.86) | 0.81 (0.67–0.89) | 0.70 (0.55–0.81) | 0.54 (0.39–0.52) | 0.76 (0.64–0.86) |
| Specificity (LL–UL) | 0.75 (0.63–0.80) | 0.76 (0.64–0.85) | 0.73 (0.54–0.82) | 0.69 (0.57–0.74) | 0.70 (0.46–0.79) | 0.62 (0.48–0.70) | 0.79 (0.63–0.85) | 0.52 (0.32–0.60) |
| PPV | 0.11 | 0.09 | 0.10 | 0.09 | 0.09 | 0.07 | 0.09 | 0.06 |
| NPV | 0.98 | 0.98 | 0.99 | 0.99 | 0.99 | 0.98 | 0.98 | 0.98 |
| Cutoff | 5, 10 | 5, 10 | 5, 19 | 5, 20 | 100 | 9, 17 | 8, 12 | 7 |
| AUC (95% CI) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Prediction Model | CAGE-B | SAGE-B | AASL | CU-HCC | GAG-HCC | PAGE-B | Modified PAGE-B | REACH-B | |
| Subgroup | |||||||||
| No change in treatment regimen (n = 1295) | 0.81 (0.73–0.88) | 0.73 (0.64–0.81) | 0.81 (0.73–0.88) | 0.78 (0.72–0.84) | 0.81 (0.74–0.87) | 0.72 (0.64–0.80) | 0.71 (0.64–0.78) | 0.66 (0.58–0.74) | |
| TFV (n = 680) | 0.72 (0.52–0.93) | 0.65 (0.44–0.85) | 0.67 (0.48–0.86) | 0.71 (0.59–0.82) | 0.70 (0.52–0.88) | 0.71 (0.55–0.87) | 0.66 (0.47–0.84) | 0.73 (0.60–0.87) | |
| ETV (n = 615) | 0.82 (0.76–0.89) | 0.75 (0.66–0.84) | 0.85 (0.79–0.91) | 0.79 (0.72–0.87) | 0.83 (0.78–0.89) | 0.74 (0.65–0.82) | 0.74 (0.66–0.83) | 0.63 (0.52–0.73) | |
| Male (n = 993) | 0.79 (0.71–0.86) | 0.72 (0.64–0.80) | 0.77 (0.69–0.85) | 0.78 (0.72–0.84) | 0.79 (0.73–0.85) | 0.73 (0.66–0.80) | 0.71 (0.63–0.78) | 0.64 (0.55–0.72) | |
| CAP at baseline ≥ 238 dB/m (n = 155) | 0.71 (0.47–0.95) | 0.62 (0.37–0.87) | 0.74 (0.47–1.00) | 0.77 (0.63–0.91) | 0.74 (0.48–0.99) | 0.71 (0.49–0.93) | 0.63 (0.38–0.88) | 0.66 (0.49–0.84) | |
| CAP at 5-year ≥ 238 dB/m (n = 567) | 0.78 (0.67–0.90) | 0.68 (0.55–0.80) | 0.83 (0.72–0.94) | 0.83 (0.77–0.89) | 0.85 (0.75–0.94) | 0.74 (0.63–0.84) | 0.71 (0.59–0.83) | 0.65 (0.54–0.75) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, J.; Chon, Y.E.; Kim, M.N.; Lee, J.H.; Hwang, S.G.; Lee, H.C.; Ha, Y. Cirrhosis, Age, and Liver Stiffness-Based Models Predict Hepatocellular Carcinoma in Asian Patients with Chronic Hepatitis B. Cancers 2021, 13, 5609. https://doi.org/10.3390/cancers13225609
Lim J, Chon YE, Kim MN, Lee JH, Hwang SG, Lee HC, Ha Y. Cirrhosis, Age, and Liver Stiffness-Based Models Predict Hepatocellular Carcinoma in Asian Patients with Chronic Hepatitis B. Cancers. 2021; 13(22):5609. https://doi.org/10.3390/cancers13225609
Chicago/Turabian StyleLim, Jihye, Young Eun Chon, Mi Na Kim, Joo Ho Lee, Seong Gyu Hwang, Han Chu Lee, and Yeonjung Ha. 2021. "Cirrhosis, Age, and Liver Stiffness-Based Models Predict Hepatocellular Carcinoma in Asian Patients with Chronic Hepatitis B" Cancers 13, no. 22: 5609. https://doi.org/10.3390/cancers13225609