
EGFR Exon 20 Insertion in Metastatic Non-Small-Cell Lung Cancer: Survival and Clinical Efficacy of EGFR Tyrosine-Kinase Inhibitor and Chemotherapy

 , ,
, ,  , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Clinical and Molecular Features at Baseline
2.2. Treatment
2.3. Response to EGFR TKIs
2.4. Response to Platinum-Based Chemotherapy
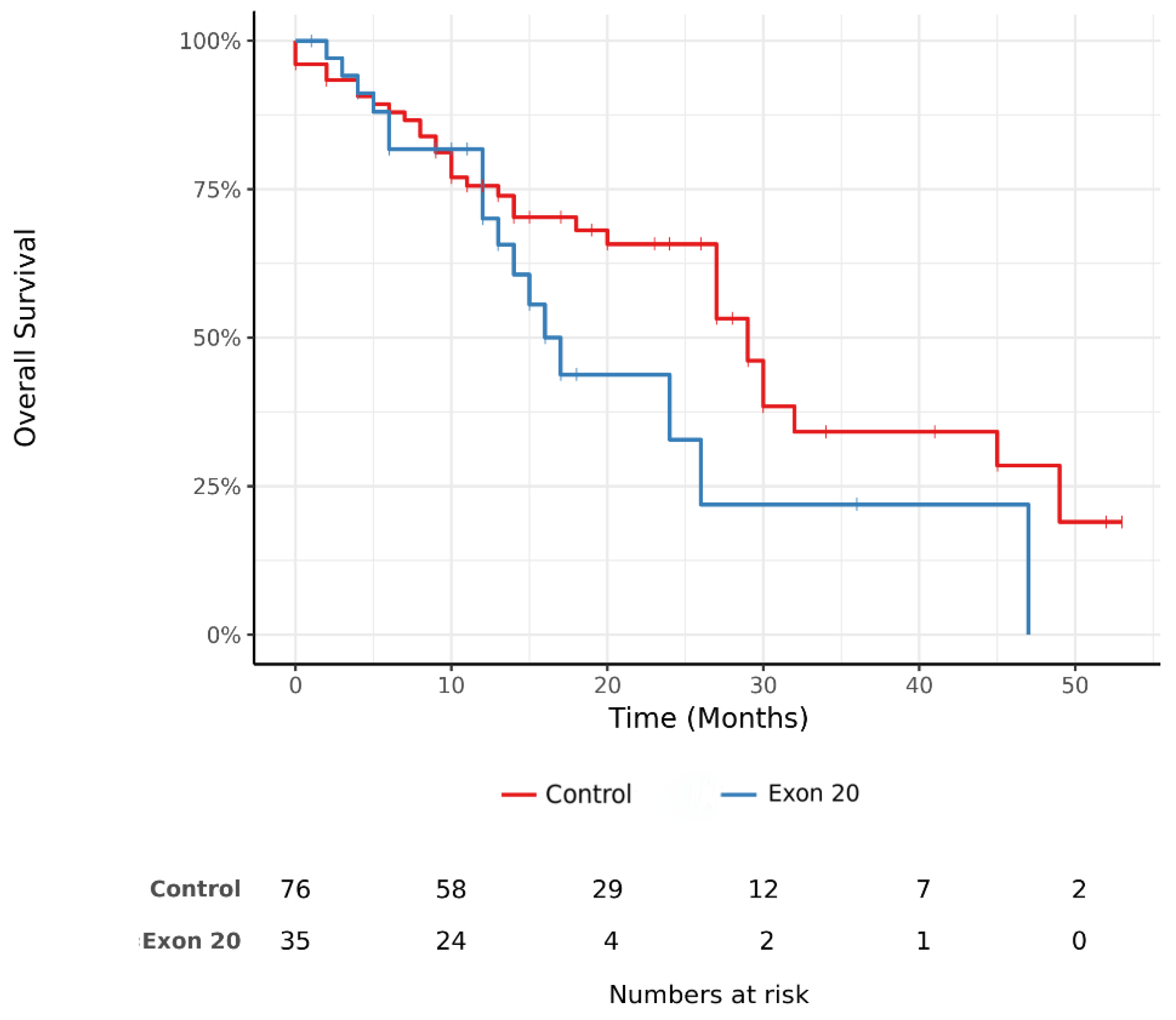
2.5. Overall Survival
2.6. Outlier Long Survivors in Exon 20 Insertion Group
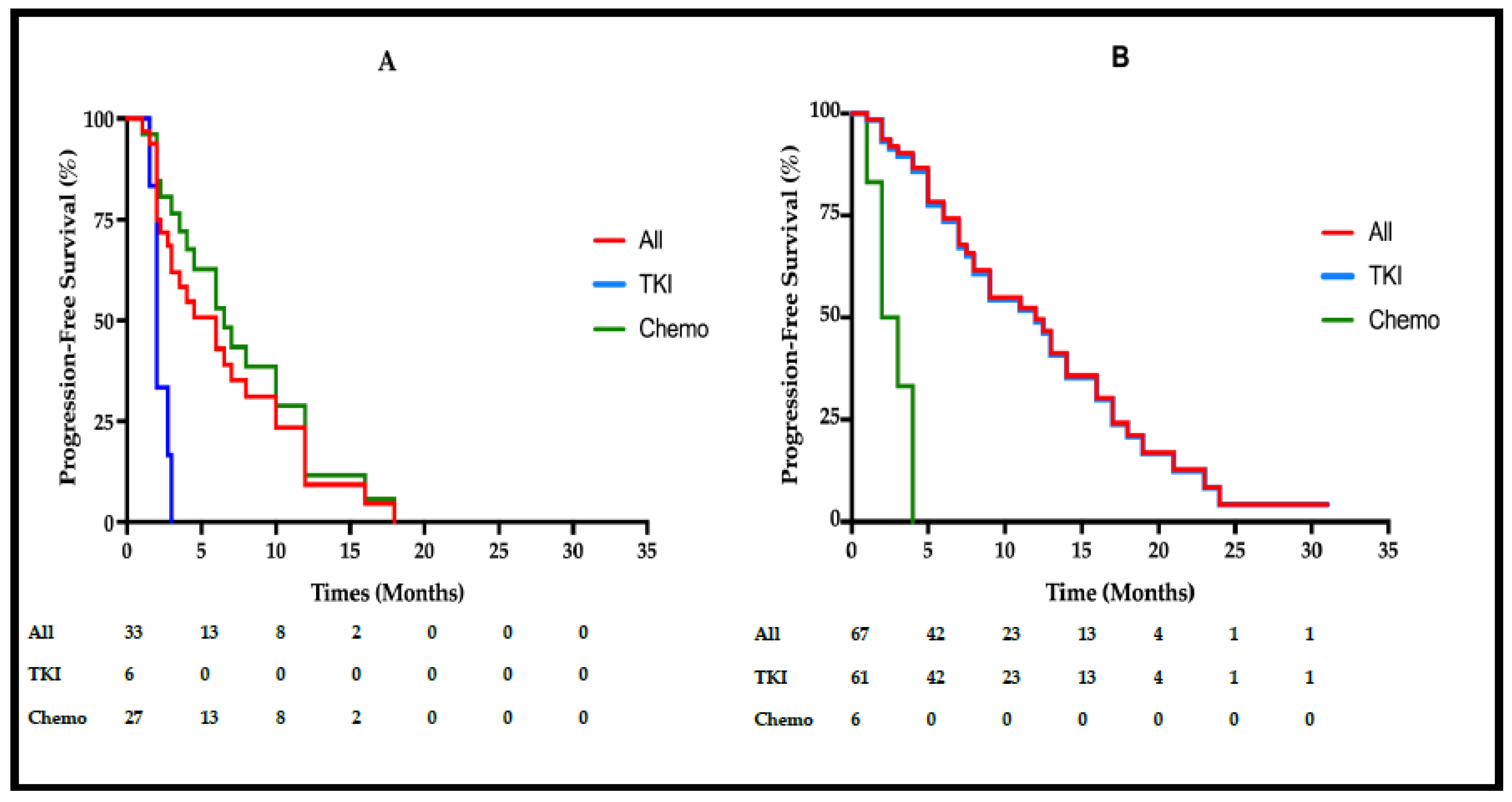
2.7. Progression-Free Survival
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Efficacy Analysis
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barlesi, F.; Mazières, J.; Merlio, J.-P.; Debieuvre, D.; Mosser, J.; Léna, H.; Ouafik, L.; Besse, B.; Rouquette, I.; Westeel, V.; et al. Routine Molecular Profiling of Cancer: Results of a One-Year Nationwide Program of the French Cooperative Thoracic Intergroup (IFCT) for Advanced Non-Small Cell Lung Cancer (NSCLC) Patients. Lancet 2016, 287, 1415–1426. [Google Scholar] [CrossRef]
- Riess, J.; Gandare, D.; Frampton, J.; Madison, R.; Peled, N.; Bufill, J.; Dy, G.; Ou, S.; Stephens, P.; McPherson, J.; et al. Diverse EGFR Exon 20 Insertions and Co-Occurring Molecular Alterations Identified by Comprehensive Genomic Profiling of NSCLC. J. Thorac. Oncol. 2018, 13, 1560–1568. [Google Scholar] [CrossRef] [Green Version]
- Vyse, S.; Huang, P.H. Targeting EGFR Exon 20 Insertion Mutations in Non-Small Cell Lung Cancer. Signal Transduct. Target. Ther. 2019, 4, 51. [Google Scholar] [CrossRef] [Green Version]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The CBio Cancer Genomics Portal: An Open Platform for Exploring Multidimensional Cancer Genomics Data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, J.; Aksoy, B.A.; Dogrusoz, U.; Dresdner, G.; Gross, B.; Sumer, S.O.; Sun, Y.; Jacobsen, A.; Sinha, R.; Larsson, E.; et al. Integrative Analysis of Complex Cancer Genomics and Clinical Profiles Using the CBioPortal. Sci. Signal. 2013, 6, pl1. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.C.-H.; Sequist, L.V.; Geater, S.L.; Tsai, C.-M.; Mok, T.S.K.; Schuler, M.; Yamamoto, N.; Yu, C.-J.; Ou, S.-H.I.; Zhou, C.; et al. Clinical Activity of Afatinib in Patients with Advanced Non-Small-Cell Lung Cancer Harbouring Uncommon EGFR Mutations: A Combined Post-Hoc Analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015, 16, 830–838. [Google Scholar] [CrossRef]
- Oxnard, G.R.; Lo, P.C.; Nishino, M.; Dahlberg, S.E.; Lindeman, N.I.; Butaney, M.; Jackman, D.M.; Johnson, B.E.; Jänne, P.A. Natural History and Molecular Characteristics of Lung Cancers Harboring EGFR Exon 20 Insertions. J. Thorac. Oncol. 2013, 8, 179–184. [Google Scholar] [CrossRef] [Green Version]
- Naidoo, J.; Sima, C.; Rodriguez, K.; Busby, N.; Nafa, K.; Ladanyi, M.; Riely, G.; Kris, M.; Arcila, M.; Yu, H. EGFR Exon 20 Insertions in Advanced Lung Adenocarcinomas: Clinical Outcomes and Response to Erlotinib. Cancer 2015, 121, 3212–3220. [Google Scholar] [CrossRef] [Green Version]
- Beau-Faller, M.; Prim, N.; Ruppert, A.-M.; Nanni-Metéllus, I.; Lacave, R.; Lacroix, L.; Escande, F.; Lizard, S.; Pretet, J.-L.; Rouquette, I.; et al. Rare EGFR Exon 18 and Exon 20 Mutations in Non-Small-Cell Lung Cancer on 10 117 Patients: A Multicentre Observational Study by the French ERMETIC-IFCT Network. Ann. Oncol. 2014, 25, 126–131. [Google Scholar] [CrossRef]
- Baek, J.H.; Sun, J.-M.; Min, Y.J.; Cho, E.K.; Cho, B.C.; Kim, J.-H.; Ahn, M.-J.; Park, K. Efficacy of EGFR Tyrosine Kinase Inhibitors in Patients with EGFR-Mutated Non-Small Cell Lung Cancer except Both Exon 19 Deletion and Exon 21 L858R: A Retrospective Analysis in Korea. Lung Cancer 2015, 87, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Byeon, S.; Kim, Y.; Lim, S.W.; Cho, J.H.; Park, S.; Lee, J.; Sun, J.M.; Choi, Y.L.; Lee, S.H.; Ahn, J.S.; et al. Clinical Outcomes of EGFR Exon 20 Insertion Mutations in Advanced Non-Small Cell Lung Cancer in Korea. Cancer Res. Treat. 2019, 51, 623–631. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Song, Z.; Cheng, G. Clinical Efficacy of First-Generation EGFR-TKIs in Patients with Advanced Non-Small-Cell Lung Cancer Harboring EGFR Exon 20 Mutations. Onco Targets Ther. 2016, 9, 4181–4186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floc’h, N.; Martin, M.J.; Riess, J.W.; Orme, J.P.; Staniszewska, A.D.; Menard, L.; Cuomo, M.E.; O’Neill, D.J.; Ward, R.A.; Finlay, M.R.V.; et al. Anti-Tumor Activity of Osimertinib, an Irreversible Mutant-Selective EGFR Tyrosine Kinase Inhibitor, in NSCLC Harboring EGFR Exon 20 Insertions. Mol. Cancer Ther. 2018, 17, 885–896. [Google Scholar] [CrossRef] [Green Version]
- Hirano, T.; Yasuda, H.; Tani, T.; Hamamoto, J.; Oashi, A.; Ishioka, K.; Arai, D.; Nukaga, S.; Miyawaki, M.; Kawada, I.; et al. In Vitro Modeling to Determine Mutation Specificity of EGFR Tyrosine Kinase Inhibitors against Clinically Relevant EGFR Mutants in Non-Small-Cell Lung Cancer. Oncotarget 2015, 6, 38789–38803. [Google Scholar] [CrossRef] [Green Version]
- Piotrowska, Z.; Wang, Y.; Sequist, L.V.; Ramalingam, S.S. ECOG-ACRIN 5162: A Phase II Study of Osimertinib 160 Mg in NSCLC with EGFR Exon 20 Insertions. J. Clin. Oncol. 2020, 38, 9513. [Google Scholar] [CrossRef]
- Yang, G.; Li, J.; Xu, H.; Yang, Y.; Yang, L.; Xu, F.; Xia, B.; Zhu, V.W.; Nagasaka, M.; Yang, Y.; et al. EGFR Exon 20 Insertion Mutations in Chinese Advanced Non-Small Cell Lung Cancer Patients: Molecular Heterogeneity and Treatment Outcome from Nationwide Real-World Study. Lung Cancer 2020, 145, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus Standard Chemotherapy as First-Line Treatment for European Patients with Advanced EGFR Mutation-Positive Non-Small-Cell Lung Cancer (EURTAC): A Multicentre, Open-Label, Randomised Phase 3 Trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or Chemotherapy for Non–Small-Cell Lung Cancer with Mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Wu, Y.-L.; Chen, G.; Feng, J.; Liu, X.-Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus Chemotherapy as First-Line Treatment for Patients with Advanced EGFR Mutation-Positive Non-Small-Cell Lung Cancer (OPTIMAL, CTONG-0802): A Multicentre, Open-Label, Randomised, Phase 3 Study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.-L.; Thongprasert, S.; Yang, C.-H.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or Carboplatin–Paclitaxel in Pulmonary Adenocarcinoma. Available online: https://www.nejm.org/doi/10.1056/NEJMoa0810699 (accessed on 28 June 2021).
- Le, X.; Goldman, J.W.; Clarke, J.M.; Tchekmedyian, N.; Piotrowska, Z.; Chu, D.; Bhat, G.; Lebel, F.M.; Socinski, M.A. Poziotinib Shows Activity and Durability of Responses in Subgroups of Previously Treated EGFR Exon 20 NSCLC Patients. J. Clin. Oncol. 2020, 38, 9514. [Google Scholar] [CrossRef]
- Le, X.; Shum, E.; Suga, J. Twice- versus Once-Daily Dosing of Investigational Poziotinib for HER2 and EGFR Mutations in Exon 20 Was More Efficacious and Better Tolerated, According to Results of the Phase 2 ZENITH20 Trial. Cancer Res. 2021, 81 (Suppl. S13), CT169. [Google Scholar] [CrossRef]
- Riely, G.J.; Neal, J.W.; Camidge, D.R.; Spira, A.I.; Piotrowska, Z.; Costa, D.B.; Tsao, A.S.; Patel, J.D.; Gadgeel, S.M.; Bazhenova, L.; et al. Activity and Safety of Mobocertinib (TAK-788) in Previously Treated Non–Small Cell Lung Cancer with EGFR Exon 20 Insertion Mutations from a Phase I/II Trial. Cancer Discov. 2021, 11, 1688–1699. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Ramalingam, S.; Li, B.; Fang, J.; Kim, T.M.; Kim, S.; Yang, J.C.; Riely, G.; Mekhail, T.; Nguyen, D.; et al. OA04.03 Mobocertinib in NSCLC With EGFR Exon 20 Insertions: Results From EXCLAIM and Pooled Platinum-Pretreated Patient Populations. J. Thorac. Oncol. 2021, 16, S108. [Google Scholar] [CrossRef]
- Piotrowska, Z.; Yu, H.A.; Yang, J.C.-H.; Koczywas, M.; Smit, E.F.; Tan, D.S.-W.; Lee, V.H.-F.; Soo, R.A.; Wrangle, J.M.; Spira, A.I.; et al. Safety and Activity of CLN-081 (TAS6417) in NSCLC with EGFR Exon 20 Insertion Mutations (Ins20). J. Clin. Oncol. 2021, 39, 9077. [Google Scholar] [CrossRef]
- Yang, J.C.-H.; Wang, M.; Mitchell, P.; Fang, J.; Nian, W.; Chiu, C.-H.; Zhou, J.; Zhao, Y.; Su, W.-C.; Camidge, D.R.; et al. Preliminary Safety and Efficacy Results from Phase 1 Studies of DZD9008 in NSCLC Patients with EGFR Exon20 Insertion Mutations. J. Clin. Oncol. 2021, 39, 9008. [Google Scholar] [CrossRef]
- Sabari, J.K.; Shu, C.A.; Park, K.; Leighl, N.; Mitchell, P.; Kim, S.; Lee, J.; Kim, D.; Viteri, S.; Spira, A.; et al. OA04.04 Amivantamab in Post-Platinum EGFR Exon 20 Insertion Mutant Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2021, 16, S108–S109. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Exon20ins 1 Group n = 35 | Control Group n = 76 | p-Value | |
|---|---|---|---|---|
| n (%) | ||||
| Age (y) | 63.8 | 69.9 | 0.02 * | |
| Gender | F/M | 19/16 (54/46) | 54/22 (71/29) | 0.08 # |
| ECOG 2 | 0.6 # | |||
| 0–1 | 29 (83) | 56 (74) | ||
| ≥2 | 5 (14) | 13 (17) | ||
| Unknown | 1 (3) | 7 (9) | ||
| Smoking status | 0.6 # | |||
| Active or former | 14 (40) | 27 (36) | ||
| Never | 20 (57) | 47 (62) | ||
| Unknown | 1 (3) | 2 (2) | ||
| Mean tobacco consumption | Pack-years | 21 | 27 | 0.49 * |
| Pleural effusion | 16 (46) | 39 (51) | 0.5 # | |
| Pericardial effusion | 0 (0) | 6 (8) | 0.17 § | |
| TNM classification (7th edition) | ||||
| T indicator | 0.6 § | |||
| Tx | 4 (11) | 15 (20) | ||
| T1 | 1 (3) | 7 (9) | ||
| T2 | 12 (34) | 19 (25) | ||
| T3 | 7 (20) | 13 (17) | ||
| T4 | 11 (32) | 22 (29) | ||
| N indicator | 0.2 § | |||
| Nx | 5 (14) | 11 (15) | ||
| N0 | 2 (6) | 17 (22) | ||
| N1 | 3 (9) | 6 (8) | ||
| N2 | 12 (34) | 23 (30) | ||
| N3 | 13 (37) | 19 (25) | ||
| M indicator | 0.74 # | |||
| M1a | 11 (31) | 19 (25) | ||
| M1b | 8 (23) | 17 (22) | ||
| M1c | 16 (46) | 40 (53) | ||
| Numbers of metastatic sites | Mean number | 1.89 | 2.26 | 0.16 * |
| Brain metastasis | Brain | 10 (29) | 25 (33) | 0.5 # |
| Amino Acid in EGFR Exon 20 | EGFR Exon 20 Insertions (n = 35) | Type of Insertion | n |
|---|---|---|---|
| A767 | 17% (n = 6) | p.Ala767_Val769dup | n = 6 |
| S768 | 20% (n = 7) | p.Ser768_Asp770dup p.Ser768_Val769delinsIleLeu | n = 6 n = 1 |
| V769 | 3% (n = 1) | p.Val769_Asp770insGlyCysVal | n = 1 |
| D770 | 17% (n = 6) | p.Asp770_Asn771insArgVal p.Asp770_Asn771insGly p.Asp770delinsGlyTyr | n = 2 n = 2 n = 2 |
| N771 | 17% (n = 6) | p.Asn771_Pro772insGly p.Asn771_Pro772insValArgGln p.Asn771_Pro772insCysAlaTyr p.Asn771_His773dup | n = 1 n = 1 n = 1 n = 3 |
| P772 | 14% (n = 5) | p.Pro772_His773delinsGln p.Pro772delinsAsnAsnAsnAla p.Pro772_His773dup p.Pro772_Cys775dup | n = 1 n = 1 n = 2 n = 1 |
| H773 | 11% (n = 4) | p.His773_Val774insAlaHis p.His773_Val774delinsLeuMet p.His773delinsTyrProAsnProTyr | n = 1 n = 2 n = 1 |
| Treatment Lines n (%) | Exon20ins 1 Group n = 35 (%) | Control Group n = 76 (%) | p-Value |
|---|---|---|---|
| n (%) | |||
| TKIs 2 | |||
| TKIs administration | 21 (60) | 74 (97) | <0.01 # |
| 1 TKI line | 19 (54) | 41 (54) | |
| 2 TKI lines | 1 (3) | 21 (28) | |
| ≥3 TKI lines | 1 (3) | 10 (13) | |
| Chemotherapy | |||
| Chemo administration | 33 (94) | 28 (37) | <0.01 # |
| 1 Chemo line | 13 (37) | 20 (26) | |
| 2 Chemo lines | 7 (20) | 5 (7) | |
| ≥3 Chemo lines | 12 (34) | 1 (2) | |
| Type of First-Line Treatment | Exon20ins 1 Group n = 35 | Control Group n = 76 |
|---|---|---|
| n (%) | ||
| TKIs 2 | ||
| Erlotinib | 3 | 19 |
| Gefitinib | 0 | 35 |
| Afatinib | 3 | 9 |
| Chemotherapy | ||
| Platin–pemetrexed | 16 | 7 |
| Platin–pemetrexed–bevacizumab | 5 | 1 |
| Platin–paclitaxel | 1 | 0 |
| Platin–paclitaxel–bevacizumab | 3 | 0 |
| Platin–vinorelbine | 1 | 0 |
| Platin–pemetrexed–nivolumab | 1 | 0 |
| Other | ||
| No treatment | 2 | 5 |
| Variation | First-Line TKIs 1 | p-Value | First-Line Chemotherapy | p-Value | ||
|---|---|---|---|---|---|---|
| Exon20ins 2 n = 6 (%) | Control n = 63 (%) | Exon20ins 2 n = 27 (%) | Control n = 8 (%) | |||
| Complete Response (CR) | 0 | 2 | 0 | 0 | ||
| Partial Response (PR) | 0 | 41 | 11 | 1 | ||
| Objective response rate (ORR) = CR + PR | 0% | 68% | <0.01 § | 41% | 12% | 0.2 § |
| Stable disease (SD) | 0 | 10 | 11 | 4 | ||
| Disease Control (DC) = CR + PR + SD | 0% | 84% | <0.01 § | 82% | 64% | 0.3 § |
| Progressive Disease | 6 100% | 3 5% | 3 11% | 2 24% | ||
| Non Assessable (NA) | 0 0% | 7 11% | 2 7% | 1 12% | ||
| Patients | Sex/Age/ECOG | Brain Metastasis | TNM (7th ed.) | Type of Exon 20 Insertions | Treatments | OS (Months) |
|---|---|---|---|---|---|---|
| 1 | F/68/0 | Yes | cT2N2M 1c | p.Asn771_Pro772insCysAlaTyr | Cisplatin–pemetrexed–bevacizumab (M) 1 Afatinib | 24 |
| 2 | F/53/0 | Yes | cT3N1M 1b | p.Asn771_His773dup | Cisplatin–navelbin Paclitaxel–bevacizumab Carboplatin–pemetrexed Erlotinib | 26 |
| 3 | F/65/1 | Yes | cT2N2M 1c | p.Ala767_Val769dup | Carboplatin–paclitaxel–bevacizumab (M) 1 Pemetrexed Docetaxel Carboplatin–pemetrexed (M) 1 Nivolumab Erlotinib | 47 |
| 4 | M/72/1 | No | cT3N3M1b | p.Asn771_Pro772insGly | Carboplatin–pemetrexed (M) 1 Nivolumab Afatinib | 36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chelabi, S.; Mignard, X.; Leroy, K.; Monnet, I.; Brosseau, S.; Theou-Anton, N.; Massiani, M.-A.; Friard, S.; Duchemann, B.; Fabre, E.; et al. EGFR Exon 20 Insertion in Metastatic Non-Small-Cell Lung Cancer: Survival and Clinical Efficacy of EGFR Tyrosine-Kinase Inhibitor and Chemotherapy. Cancers 2021, 13, 5132. https://doi.org/10.3390/cancers13205132
Chelabi S, Mignard X, Leroy K, Monnet I, Brosseau S, Theou-Anton N, Massiani M-A, Friard S, Duchemann B, Fabre E, et al. EGFR Exon 20 Insertion in Metastatic Non-Small-Cell Lung Cancer: Survival and Clinical Efficacy of EGFR Tyrosine-Kinase Inhibitor and Chemotherapy. Cancers. 2021; 13(20):5132. https://doi.org/10.3390/cancers13205132
Chicago/Turabian StyleChelabi, Samy, Xavier Mignard, Karen Leroy, Isabelle Monnet, Solenn Brosseau, Nathalie Theou-Anton, Marie-Ange Massiani, Sylvie Friard, Boris Duchemann, Elizabeth Fabre, and et al. 2021. "EGFR Exon 20 Insertion in Metastatic Non-Small-Cell Lung Cancer: Survival and Clinical Efficacy of EGFR Tyrosine-Kinase Inhibitor and Chemotherapy" Cancers 13, no. 20: 5132. https://doi.org/10.3390/cancers13205132