
Emerging Landscape of Immunotherapy for Primary Central Nervous System Lymphoma

1
Center for Cancer Immunotherapy, Institut Curie, PSL Research University, INSERM U932, 75005 Paris, France
2
Clinical Hematology Unit, Institut Curie, 92210 Saint-Cloud, France
*
Author to whom correspondence should be addressed.
†
Contributed equally to the work.
Cancers 2021, 13(20), 5061; https://doi.org/10.3390/cancers13205061
Submission received: 4 August 2021
/
Revised: 29 September 2021
/
Accepted: 5 October 2021
/
Published: 10 October 2021
(This article belongs to the Special Issue Immunotherapy in B-cell Non-Hodgkin Lymphomas)
Abstract
:Simple Summary
Primary central nervous system lymphoma (PCNSL) is characterized by its location in the central nervous system comprising the brain, the eye, the cerebrospinal fluid and the spinal cord and a poor prognosis with the current chemotherapies. Immunotherapies represent a new paradigm in the care of patients with B-cell lymphoma, but, till recently, immunotherapies studies excluded patients with PCNSL because of the lack of knowledge on the immune network in the brain. Recent studies shed a new light on the origin and characteristics of the CNS immune cells. We review the current experimental preclinical and clinical developments of immunotherapies in CNS lymphoma as well as the effects of targeted therapies on the brain microenvironment. We provide perspectives for improving the efficacy of immunotherapies in the specific setting of PCNSL for a better prognosis of this disease.
Abstract
Primary central nervous system lymphoma (PCNSL) is, mainly, a diffuse large B-cell lymphoma (DLBCL) with a non-germinal center B-cell (non-GCB) origin. It is associated with a poor prognosis and an unmet medical need. Immunotherapy has emerged as one of the most promising areas of research and is now part of the standard treatment for many solid and hematologic tumors. This new class of therapy generated great enthusiasm for the treatment of relapsed/refractory PCNSL. Here, we discuss the challenges of immunotherapy for PCNSL represented by the lymphoma cell itself and the specific immune brain microenvironment. We review the current clinical development from the anti-CD20 monoclonal antibody to CAR-T cells, as well as immune checkpoint inhibitors and targeted therapies with off-tumor effects on the brain microenvironment. Perspectives for improving the efficacy of immunotherapies and optimizing their therapeutic role in PCNSL are suggested.
1. Introduction
Primary central nervous system lymphomas (PCNSL) involve the brain, the eye, the cerebrospinal fluid (CSF) and, less frequently, the spinal cord, without any systemic dissemination. In immunocompetent patients, the histology is almost always a diffuse large B-cell lymphoma (DLBCL), preferentially of a non-germinal center (non-GC) phenotype [1,2]. PCNSL is a rare disease, representing 3% of all non-Hodgkin lymphomas (NHL), with no specific sex ratio and affecting 1900 and 300 new cases per year in the USA and France, respectively [1,3]. The prognosis of PCNSL is poorer than that of nodal non-GC DLBCL [4]. Improved outcomes have been observed in recent decades, especially in young patients who respond to high-dose methotrexate-based induction chemotherapies and who receive a consolidation treatment with either intensive chemotherapy and autologous stem cell transplantation (IC-ASCT) or whole brain radiation therapy (WBRT) [5,6]. IC-ASCT acts on minimal residual disease through the dose-intensity effect of the chemotherapy. IC-ASCT showed a good control of the disease in the first-line setting [5,6]. At relapse, consolidation with IC-ASCT is an effective treatment, allowing a survival gain in patients under the age of 65 years who are eligible for such an intensive treatment [7,8]. However, IC-ASCT exposes to the risk of IC-related toxicities and treatment-related deaths in 4 to 10% of the patients [5,6,7].
Despite these therapeutic improvements, 16 to 26% of patients are primary refractory to high-dose methotrexate [1,9] or, subsequently, relapse [10]. These patients represent an unmet medical need [1,8].
The poor prognosis of PCNSL with the current conventional treatments can be, at least in part, explained by the aggressiveness of non-GC malignant B-cells, with frequent mutations of MYD88 and CD79b [4], and by the anatomical and functional characteristics of the blood–brain barrier (BBB) which limits the bioavailability of many drugs in the brain parenchyma. The homing of PCNSL in the CNS at diagnosis is also observed at relapse, with less than 5% of relapses occurring outside the CNS in a series of 1000 patients in the modern era [1]. This points out the role of the tumor microenvironment (TME) as a key component of lymphomagenesis and homing in the CNS [11,12,13] and, therefore, as a therapeutic target to be explored.
Immunotherapies represent a new paradigm in the care of patients with systemic B-cell malignancies. The benefit of immunotherapies, such as allogeneic hematopoietic stem cell transplantation, monoclonal anti-CD20 antibodies, immune checkpoint inhibitors and CAR-T cells, have been less explored in PCNSL, because of the rarity of the disease and the concerns raised by the expected lack of immune effector cells in the brain. Indeed, the brain, while not being an immune-privileged sanctuary, still provides an immunosuppressive and nurturing tumor environment, which could provide resistance to immunotherapies. The clinical activity of ibrutinib, lenalidomide and pomalidomide has been demonstrated in relapsed PCNSL. How these drugs, known to modulate the microenvironment of B-cell malignancies, impact the immune brain microenvironment remains to be deciphered.
This review aims to present an overview of the knowledge regarding the immune brain microenvironment, the most important preclinical and clinical results, along with suspected underlying mechanisms of resistance, and provide perspectives for improving the efficacy of immunotherapies and optimizing their role in the therapeutic armamentarium of PCNSL.
2. Brain Microenvironment
In recent years, immunotherapy has become increasingly common in the management of solid tumors and some B-cell lymphomas due to clear clinical benefits. Immunotherapy efficacy depends on several aspects that are tumor specific. Both autonomous mechanisms (e.g., the low tumor mutational burden, downregulation of MHC genes and expression of PD-L1/PD-L2), as well as extrinsic properties (e.g., immunosuppressive TME), are at the origin of inconsistent clinical outcome. Although the TME of certain brain tumors is starting to be unraveled, little is known about the cellular and molecular immune players implicated in PCNSL progression. PCNSL can develop in the brain parenchyma, but also in CNS interfaces: the perivascular and meningeal spaces. It is expected that the precise location of PCNSL will drive the composition of the TME (Figure 1).
The CNS has been historically considered to be immune-privileged. This concept has been coined following Medawar’s observation that skin allografts have a prolonged survival when placed in the brain and eye of rabbits [14]. The inability to mount an efficient immune response against the grafts was explained by the presence of physical barriers at the borders between the CNS and the periphery: the blood–brain barrier (BBB) and the blood–cerebrospinal fluid barrier (BCSFB), as well as the apparent lack of lymphatic drainage. Nowadays, the concept of immune privilege has been revisited, due to the better understanding of CNS immunity. Recently, the presence of lymphatic vessels was found in the meninges of mammals. The network of lymphatic vessels runs parallel to dural venous sinuses and allows for the drainage of cells and CSF into deep cervical lymph nodes [15,16,17]. Although the brain does not seem to be directly drained, interstitial fluid (ISF) solutes are constantly being cleared and carried into the CSF through the “glymphatic system”. Instead of lymphatic vessels, the glymphatic system uses periarterial spaces to move CSF into the brain parenchyma and perivenous spaces to drive ISF out [18]. In the steady state, the immune system of the CNS is composed mainly of innate immune cells. These cells are mostly macrophages found in the parenchyma, namely, microglia, but also in the borders of the CNS: meningeal, perivascular and choroid plexus macrophages [19]. Fate-mapping experiments combined with transcriptomic studies have shown that CNS macrophages originate from yolk sac erythro-myeloid progenitors and are believed to be sustained by self-renewal during adulthood [19]. Very recently, the existence of direct vascular connections between the meninges and the skull bone marrow was described in mice. It was shown that the skull and the vertebral bone marrow represent a private reservoir of myeloid cells and B-cells that replenishes the meninges, perivascular spaces and the CNS parenchyma during homeostasis and CNS injury [20,21,22], in complement to blood-derived inflammatory cells (Figure 1). If such reservoirs also exist in humans, it will reshape our interpretation of CNS immunity in health and disease. In light of these findings, it is tempting to speculate that a dural bone marrow reservoir of B-cells might be involved in PCNSL pathophysiology and its exclusive homing to the CNS.
Although a more detailed characterization of the TME in large cohorts of patients is missing, several studies have attempted to identify cellular and molecular mechanisms implicated in the progression of PCNSL. The presence of tumor-infiltrating lymphocytes (TILs) has been observed [13,23,24,25,26], and its accumulation within the perivascular space has been associated with better survival [23]. Some TILs express immune checkpoint receptors (i.e., PD-1 and TIM3) [25,26,27] and a high expression of PD-1 has been associated with inferior survival [28]. Besides lymphoma cells, tumor-associated macrophages (TAMs) have been described as alternative sources of PD-L1 [26,29]. TAMs are a mixed population of macrophages with different ontogenies (microglia, perivascular/meningeal macrophages and monocyte-derived macrophages) and a global increased ratio of M1/M2-like TAMs has been associated with a better outcome [27]. Furthermore, the level of infiltration of TAMs has been correlated with IL-10 in the CSF [30]. IL-10 has been mostly reported as an anti-inflammatory cytokine, which plays a central role in lymphoma development as a growth factor for B-lymphocytes and an inducer of the anti-apoptotic Bcl2 pathway [31]. IL-10 is produced by the lymphoma cells and could have both autocrine and paracrine effects. IL-10 was identified as an effective diagnostic biomarker for PCNSL [32,33]. Finally, besides cells derived from direct immune lineages, other cell populations including astrocytes, mural cells and endothelial cells are likely involved in shaping up the immune landscape of PCNSL TME [13,34].
In the era of single-cell omics, we should soon be able to better understand the complexities of the TME of PCNSL; consequently, boosting the development of more effective immune-based therapies.
3. Available Clinical Data
3.1. Allogeneic Hematopoietic Stem Cell Transplantation (alloHSCT)
From a historical perspective, alloHSCT represents the first success of immunotherapy [35]. Assuming that allogeneic T-cells may traffic to the CNS and mediate the graft-versus-lymphoma (GvL) immunoreaction, alloHSCT may be effective against PCNSL [36]. The GvL immunoreaction, specific to alloHSCT, is exclusively sought if a non-myeloablative conditioning regimen is chosen, or will complete the effect of the intensive chemotherapy on the minimal residual disease if a myeloablative regimen is given. The conditioning regimen’s choice is driven by the patients’ characteristics and previous treatments. Nevertheless, allogeneic T-cells can lead to graft-versus-host disease (GvHD), which can be severe and life-threatening. Mika et al. conducted a retrospective study on 6 PCNSL patients who received alloHSCT following a conditioning regimen with fludarabine, busulfan and cyclophosphamide [37]. All patients had previously received rituximab and high-dose methotrexate, in combination with high-dose cytarabine or ifosfamide, as first-line therapy. All patients had also received IC-ASCT, three of whom in first-line consolidation and the others in second-line. All patients presented with an unconfirmed complete response (uCR) before alloHSCT. Two patients died, one from severe GvHD and one from a lymphoma relapse. Four out of six patients were still alive in complete response (CR) almost 4 years after alloHSCT. Although preliminary, these data suggest that immune mechanisms might be active against PCNSL (Table 1). AlloHSCT may be an interesting option after failure of IC-ASCT. Ideally, prospective trials would help to unravel this therapeutic potential, together with safety considerations, and to better define its position regarding other cell therapies, such as chimeric antigen receptor (CAR) T-cells [38].
3.2. Monoclonal Antibodies
The CD20-directed monoclonal antibody, rituximab, has shown survival improvement in B-cell non-Hodgkin lymphomas (NHL), including systemic DLBCL [39], and is now part of their gold standard therapies [40]. Considering that most of PCNSL are CD20+ subtypes of DLBCL [41], it makes sense hypothesizing that rituximab would improve the outcome of PCNSL patients. However, the addition of rituximab in the treatment of PCNSL is not straightforward. Under physiologic conditions, the BBB prevents the trans-vascular crossing of most molecules larger than 180 Daltons [42]. Nonetheless, the alteration of the BBB observed around large tumor lesions in PCNSL may improve the penetration of monoclonal antibodies.
From a preclinical perspective, rituximab has shown an activity following intravenous injection in a nude rat model of CNS lymphoma [43]. From a clinical perspective, four confirmed radiographic responses (3 CR, 1 partial response (PR)) were reported in a pilot study including twelve patients with recurrent or refractory PCNSL who received rituximab as monotherapy [44]. Promising results have also been reported in retrospective studies, showing that rituximab improves CR rates, progression-free (PFS) and overall survival (OS), in combination with high-dose chemotherapy [45,46]. However, this benefit was challenged by the HOVON/ALLG international, multicentric, randomized phase 3 trial [47] (Table 1). One hundred newly diagnosed PCNSL patients received two cycles of MBVP (methotrexate, carmustine, teniposide and prednisone) and ninety-nine patients received the same induction regimen, in combination with intravenous rituximab on days 0, 7, 14 and 21 in cycle one and days 0 and 14 in cycle two. Patients in response (CR or PR) at the end of induction received a consolidation with high-dose cytarabine and, for patients aged 60 years or younger, low-dose WBRT. The authors found no difference, neither in the terms of event-free survival (EFS, primary endpoint of the study, 49% versus 52% at 1-year) nor PFS, OS or response to induction chemotherapy. An unplanned subgroup analysis showed a trend for enhanced EFS for patients aged 60 years or younger who received rituximab. Another international, multicentric trial aimed at evaluating the effects of rituximab in first line PCNSL [9]. This phase two, IELSG-32 trial, compared three different induction chemotherapy regimens in a randomized manner, i.e., high-dose methotrexate (HD-MTX) plus cytarabine (n = 75 patients), HD-MTX, cytarabine plus rituximab (n = 74 patients), and HD-MTX, cytarabine and rituximab plus thiotepa (n = 78 patients). A second randomization compared consolidation with WBRT or ASCT for patients in response or stable disease. The primary endpoint of the first randomization was the CR rate after four cycles of induction therapy, which was 23%, 30% and 49% in each of the three arms, respectively. A systematic review and meta-analysis including these two randomized trials, for a total of 343 patients, was conducted to provide guidance for clinical practice [48]. Albeit, neither trial demonstrated a benefit for rituximab regarding their primary endpoints, the pooled hazard ratio for PFS suggested a possible benefit of adding rituximab. This meta-analysis also showed that the addition of rituximab was not associated with an increase in clinically significant adverse events. The long-term analysis of the IELSG-32 study was recently presented at the ICML 2021 meeting and showed a better 7-year OS for patients who received HD-MTX, cytarabine plus rituximab (37%) compared to patients who received only HD-MTX plus cytarabine (26%) independently of the consolidation arm [49].
Altogether, the addition of rituximab to HD-MTX-based chemotherapy did not dramatically improve the prognosis of patients with PCNSL as observed in systemic DLBCL. Despite modest evidence, rituximab has been mostly integrated into PCNSL first and subsequent lines of therapy. Of note, to our knowledge, no data regarding the activity of bispecific antibodies in PCNSL are available to date.
3.3. Immune Checkpoint Inhibitors (ICI)
Checkpoint blockade using programmed cell death (ligand) 1 (PD-(L)1) antibodies made a huge breakthrough in the treatment of many tumor types previously limited by the lack of therapeutic options [50,51,52,53]. Particularly, anti-PD-1 antibodies showed dramatic anti-tumor responses in classical Hodgkin lymphoma (HL) [54,55], which is characterized by chromosome 9p24.1 alterations, including polysomy, copy gain and amplification, and resulting in enhanced PD-L1/PD-L2 expression [56]. High-level 9p24.1 copy gain and increased PD-L1 expression are associated with prolonged survival of HL patients upon anti-PD-1 treatment [57]. Interestingly, 9p24.1/PD-L1/PD-L2 copy number alterations and translocations of these loci were reported in more than 50% of EBV-negative PCNSL [4]. These structural bases for PCNSL immune evasion, together with the characterization of the tumor microenvironment [27], support the use of ICI in PCNSL. Preliminary encouraging results have been reported with the anti-PD-1 antibody, nivolumab single agent, in four patients with relapsed/refractory (R/R) PCNSL and one patient with CNS relapse of testicular lymphoma [58]. Overall, nivolumab was well tolerated. All patients had objective responses, including 4 CR and 1 PR, and three patients remained progression-free at 13 to 17 months. Nonetheless, two patients had received radiation therapy immediately prior to the initiation of nivolumab. A high objective response rate was also reported in another monocentric retrospective study, including eight PCNSL patients treated with nivolumab. Three and four patients achieved a CR and a PR, respectively [59]. Unfortunately, these promising results have not been confirmed in a prospective study including 47 PCNSL and 19 patients with CNS relapse of primary testicular lymphoma (NCT02857426), according to the available results posted on clinicaltrials.gov in 2020. These results have not been published yet. Pembrolizumab has also been studied in R/R PCNSL. The first results of the AcSé pembrolizumab multicentric phase II study were presented at the ASH 2020 annual meeting [60] (Table 1). Fifty R/R patients, including 41 PCNSL and 9 primary vitreoretinal lymphomas (PVRL), treated with single agent pembrolizumab were reported. Eight and five patients obtained a CR and a PR, respectively, leading to an overall response rate of 26% and a median PFS of 2.6 months. Responses may be durable as the reported median duration of response (DOR) was 10 months. Considering the good safety profile, further studies evaluating ICI either in combination therapies and/or earlier in the course of the disease are warranted to increase their activity in PCNSL.
3.4. CAR-T Cells
CAR-T are genetically engineered T-cells that express an antibody-like chimeric receptor [61]. Autologous CAR-T targeting CD19 are currently approved and commercialized in third-line systemic DLBCL [62,63,64]. Nevertheless, few data on CAR-T for CNS lymphoma are available to date [38] and most of them concern secondary, but not primary, CNS lymphoma. Patients with CNS infiltration were excluded from most of the pivotal trials because of concerns related to immune effector cell-associated neurotoxicity syndrome (ICANS) after CAR-T therapy [65]. Patients with secondary CNS involvement were eligible for the TRANSCEND prospective study, which aimed to assess the safety and activity of liso-cel in third-line DLBCL [64]. Among 256 evaluable patients, 6 had CNS disease and 3 of them achieved a CR. The largest cohort of secondary CNS lymphoma patients was published by Frigault et al., who reported a retrospective analysis on eight patients who received tisa-cel [66]. The treatment was well tolerated and responses were observed in four patients (2 CR, 2 PR) at day 28 after CAR-T infusion. Li et al. showed results with a longer follow-up for five patients, including one primary and four secondary CNS lymphomas, enrolled in a clinical trial testing CD19 plus CD22 CAR-T cells [67]. All achieved an objective response, but four patients relapsed within 3 to 8 months. The authors suggested that the immunosuppressive brain microenvironment may have contributed to the lymphoma relapse. This interesting hypothesis should be addressed by relevant preclinical and clinical studies. For example, preclinical experiments, including histopathology, flow cytometry and single-cell RNA sequencing, in immunocompetent animals, could assess the role of the brain microenvironment in the relapse following CAR-T therapy. From a clinical perspective, combining CAR-T cells with immunomodulatory agents seems relevant. Recently, the French national network for oculo-cerebral lymphomas (LOC) reported the first and largest cohort of nine immunocompetent patients with relapsed/refractory PCNSL treated with CD19 CAR-T cells (tisa-cel and axi-cel), after at least two previous lines of therapy [68] (Table 1). Despite the recent identification of CD19-expressing mural cells surrounding the brain endothelium as potential off-tumor targets [69], the authors did not observe unexpected neurotoxicity. Responses were centrally reviewed, according to the IPCG criteria [70]. With a median follow-up of 6.5 months, the best response was PR in one patient and CR in five patients, which demonstrated an activity of CAR-T cells in this specific setting. Median PFS was 4 months in the whole group and 7 months in responder patients. Six-month OS was 89%. These encouraging results should be confirmed by prospective clinical trials.
Bridging therapy between leukapheresis and CAR-T infusion may contribute to optimize the results of CAR-T. It is presumable that bridging therapy will be necessary for most of relapsed/refractory PCNSL patients because of the rapid evolution of the disease and the necessary time to manufacture CAR-T. Radiation therapy should be carefully assessed in this setting, as it has been reported feasible [71], and could be associated with a better outcome for relapsed/refractory large B-cell lymphoma treated with axi-cel [72].
3.5. Other Targeted Therapies
Some targeted therapies, such as Bruton’s tyrosine kinase (BTK) inhibitors or immunomodulatory drugs (IMIDs), may have an “on-target, off-tumor” effect on the PCNSL tumor microenvironment (Table 2).
Ibrutinib, the first-in-class BTK inhibitor, showed a favorable brain distribution through the BBB in preclinical mice models [73,74] and substantial activity in PCNSL was reported in retrospective [75] and early phase clinical trials [76,77]. A French group conducted a proof-of-concept phase II study with ibrutinib, a single agent, at 560 mg per day, until progression or unacceptable toxicity, in R/R PCNSL and PVRL [78]. Among 44 evaluable patients, the disease control rate after 2 months of continuous treatment (primary endpoint) was 70%, including 23% CR + uCR, 36% PR and 11% stable disease (SD). Responses were observed in all CNS compartments. The overall safety profile was good, albeit two patients who received concomitant corticosteroids, presented with pulmonary aspergillosis. After a median follow-up of 25.7 months, the median PFS was 4.8 months and the median OS was 19.2 months. Notwithstanding, the duration of response was higher than 12 months in 15 patients. Interestingly, no correlation was found between responses and mutations in the B-cell receptor (BCR) pathway, which were available for 18 patients. This suggests that, beyond BTK inhibition, ibrutinib could modulate the brain microenvironment and enhance local antitumor immune responses. Second generation BTK inhibitors were developed, namely, acalabrutinib, zanubrutinib, orelabrutinib and tirabrutinib and assessed in B-cell malignancies. To date, only tirabrutinib has been prospectively evaluated as a single agent in a phase I/II study, showing a favorable toxicity and efficacy profile in R/R PCNSL [79].
IMIDs have also been tested in relapsed or refractory PCNSL patients. A phase I study reported that lenalidomide penetrates the ventricular CSF and was associated with an overall response rate (ORR) of 64% as monotherapy in 14 patients with relapsed or refractory CNS lymphoma, including 6 PCNSL [80]. In the phase II REVRI study, R/R PCNSL (n = 34) and PVRL (n = 11) patients received an induction comprising eight cycles of the R2 regimen (rituximab + lenalidomide), followed by a 1-year maintenance of lenalidomide alone in responding patients [81]. At the end-of-induction, the ORR was 36%, including 29% CR/uCR. The R2 combination was active in all CNS compartments. Eighteen and five patients started and completed the maintenance phase, respectively. Four patients remained in CR at the end-of-treatment. The limited benefit observed here differed from a retrospective analysis of lenalidomide maintenance in 10 relapsed PCNSL patients [80]. With a median follow-up of 19.2 months, the median PFS and OS were 7.8 and 17.7 months, respectively. Manageable toxicities were reported, mostly hematological. An interesting analysis of the circulating immune cell populations showed that the blood CD4/CD8 ratio at baseline had a prognostic value in the REVRI study. Indeed, the median PFS was 9.5 months when the CD4/CD8 ratio was ≥ 1.6 versus 2.8 months. This finding highlighted the role played by the microenvironment regarding the response to IMIDs, which needs to be validated in an independent cohort. Another phase I study determined the maximal tolerated dose of pomalidomide as 5 mg in association with dexamethasone within a cohort of 25 R/R PCNSL and PVRL [82]. This combination resulted in an ORR of 48% with 32% CR/uCR and a median PFS of 5.3 months (Table 1).

{kind=link}
{kind=link}
Table 1.
Summary of the main clinical data on PCNSL immunotherapies. ORR, overall response rate; CR, complete response; PFS, progression-free survival; alloHSCT, allogeneic hematopoietic stem cell transplantation; NR, not reached; vs., versus; NA, not available; EFS, event-free survival; HD-MTX, high-dose methotrexate; DoR, duration of response.
Table 1.
Summary of the main clinical data on PCNSL immunotherapies. ORR, overall response rate; CR, complete response; PFS, progression-free survival; alloHSCT, allogeneic hematopoietic stem cell transplantation; NR, not reached; vs., versus; NA, not available; EFS, event-free survival; HD-MTX, high-dose methotrexate; DoR, duration of response.
| Treatment | N Patients | Median Follow-Up | ORR | CR | Median PFS | Comments |
|---|---|---|---|---|---|---|
| AlloHSCT [37] | 6 | 45 months | 4/6 | 4/6 | NR | Retrospective study. Four patients alive in CR at 4 years |
| Rituximab [47] R-MBVP vs. MBVP (1st line) | 199 | 32.9 months | 81% vs. 75% | 68% vs. 66% | NA | 1-year EFS 52% vs. 49% |
| Rituximab [9] HD-MTX plus cytarabine vs. HD-MTX, cytarabine plus rituximab vs. HD-MTX, cytarabine, rituximab plus thiotepa (1st line) | 227 | 30 months | 53% vs. 74% vs. 87% | 23% vs. 30% vs. 49% | NA | Long-term analysis: 7-year OS 37% for HD-MTX plus cytarabine plus rituximab vs. 26% for HD-MTX plus cytarabine independently of the consolidation arm [49] |
| Nivolumab [58] | 5 | 17 months | 5/5 | 4/5 | NA | Results not confirmed in a prospective study (NCT02857426) |
| Nivolumab [59] | 9 | 18 months | 7/9 | 3/9 | 12 months | Results not confirmed in a prospective study (NCT02857426) |
| Pembrolizumab [60] | 50 | 6.7 months | 26% | 16% | 2.6 months | Median DoR 10 months |
| CD19 CAR-T cells [68] | 9 | 6.5 months | 6/9 | 5/9 | 4 months | Median DoR NR |
| Ibrutinib [78] | 44 | 25.7 months | 59% | 23% | 4.8 months | DoR > 12 months in 15 patients |
| Tirabrutinib [79] | 44 | 9.1 months | 64% | 34% | 2.9 months | |
| Lenalidomide [80] | 14 | NA | 9/14 | 3/14 | 6 months | |
| Lenalidomide plus rituximab [81] | 45 | 19.2 months | 36% | 29% | 7.8 months | |
| Pomalidomide plus dexamethasone [82] | 25 | 16.5 months | 48% | 32% | 5.3 months |
Table 2.
Potential “on-target, off-tumor” effects of ibrutinib and lenalidomide/pomalidomide.
| Drug | Cellular Target | Potential Effect | |
|---|---|---|---|
| Ibrutinib | Adaptive immunity | Lymphocytes | ↑ Th1 immunity [83] ↑ Persistence [84] ↓ CD8+ T-cell exhaustion [85] |
| Innate immunity | Myeloid-derived suppressor cells | ↓Migration, depletion [86] | |
| IMIDs (lenalidomide/pomalidomide) | Adaptive immunity | Lymphocytes | ↑ Th1 immunity [87,88] ↑ Effector functions [89] |
| Innate immunity | TAMs NK cells | ↑ M1/M2 phenotype [90] ↑ Effector functions [91] | |
4. Future Perspectives
4.1. Combination Therapies
The significant results reported above sketch an optimistic landscape with new therapeutic combinations to be tested in PCNSL patients. Indeed, despite high antitumor activity in the first months of treatment, the duration of response remains short. This encourages the combination of treatments targeting different immune pathways. Such combinations may involve BTK inhibitors, ICI, IMIDs and/or CAR-T cells, and are described in Figure 2. A synergistic effect on the anti-lymphoma immune response can be expected from these combinations. For example, IMIDs-induced M1 polarization might be associated with an increased production of IFNγ and enhanced PD-L1 expression; thus, impairing T-cell antitumor functions. As such, a combination therapy of lenalidomide with an anti PD-L1 antibody could be beneficial. Ongoing clinical trials of combined therapies targeting immune pathways are reported in Table 3.
Conventional immunochemotherapy might also be optimized by targeting immune pathways. The results presented above call for a further assessment of ibrutinib and lenalidomide or pomalidomide in combination with immunochemotherapy. The ongoing phase II LOC-R01 trial (NCT04446962) randomizes ibrutinib versus lenalidomide, plus rituximab–methotrexate–procarbazine–vincristine (R-MPV) for the induction treatment in first-line PCNSL patients, younger than 60 years-old and eligible for autologous HSCT.
Finally, besides their direct antitumor effect and the immunomodulation of the PCNSL microenvironment, ibrutinib and IMIDs should be tested in combination with CAR-T. Both targeted therapies have been reported to improve the efficacy and safety of CD19 CAR-T in preclinical [92,93,94] and clinical [95] studies. Clinical trials, associated with high-quality biomarker studies, are warranted to evaluate the synergy between CAR-T and such immunomodulatory drugs in order to improve the prognosis of high-risk PCNSL patients.
4.2. Optimizing the Timing of Immunotherapy
To date, the development of most new therapies is focused on chemo-refractory/relapsed PCNSL patients. However, relapses are associated with a poorer prognosis [8] and often worse patients’ fitness. Immunotherapies may be more effective if given earlier in the therapeutic strategy. Das et al. reported an extensive analysis on T-cell phenotypes of cells collected from the peripheral blood of children with solid tumors and lymphomas [96]. Interestingly, the percentage of naïve and central memory T-cells decreased, whereas terminal effectors increased along with cumulative chemotherapy cycles. Moreover, the in vitro expansion capacity of these T-cells significantly declined over time and increased the number of chemotherapy cycles. These data provide a rational basis to introduce immunotherapies as early as possible in the course of the disease. CD19 CAR-T cells are currently being evaluated in high-risk systemic large B-cell lymphoma with suboptimal response to first line therapy (ZUMA-12 study). An intermediate analysis was recently reported and showed a higher median number of naïve T-cells in the final CAR-T product and a higher peak expansion of CAR-T, as compared to patients who received at least two prior lines of immunochemotherapy [97].
ICI were tested in first line treatment for multiple solid tumor indications and showed impressive results [98,99,100]. Overall, immunotherapies which rely on the activation of T-cell antitumor immunity, should be evaluated in the first lines of PCNSL treatment, when endogenous-T cells are prone to better anti-lymphoma effects. Thus, one may expect that the future induction therapy for newly diagnosed PCNSL would include high-dose methotrexate, in combination with ICI and an immunomodulatory drug. CAR-T cells should be evaluated at first relapse and as a consolidation therapy in patients ineligible for ASCT.
4.3. Improving Trafficking
Many hypotheses may explain the modest results observed with rituximab for PCNSL treatment, including the question of poor CNS diffusion and the existence of complement-dependent cytotoxicity, antibody-dependent cellular cytotoxicity and antibody-dependent cellular phagocytosis in the brain. Two phase I trials evaluated the intraventricular injection of rituximab, either as monotherapy [101], or in combination with methotrexate [102]. Intrathecal rituximab was safe at 10 and 25 mg and modest clinical responses were observed in refractory CNS lymphoma. Interestingly, an ancillary study showed the activation of the complement cascade within the brain microenvironment after an intraventricular administration of rituximab [103].
The trafficking of CAR-T to the CNS may also be challenging. Preclinical studies showed enhanced CAR-T activity following local delivery. Mulazzani et al. developed in vivo microscopy in an orthotopic murine model of PCNSL to show that intracerebral, rather than intravenous, injection of CD19 CAR-T resulted in a deeper infiltration and an increased control of the tumor growth [104]. Interestingly, following intracerebral injection, CAR-T persisted in the brain and the blood for up to 159 days, even after a complete regression of the CNS lymphoma. The superiority of intraventricularly injected CD19 CAR-T was recently corroborated in another preclinical study [105]. Importantly, the models developed in both studies were immunodeficient mice, which may hinder the translation to human disease. Notably, due to the lack of circulating human B-cells, CAR-T cells do not rapidly encounter their target once infused intravenously and this may impair their expansion. Ideally, these promising findings should be validated in preclinical studies using immunocompetent models [106]. An intraventricular delivery of CD19 CAR-T via an Ommaya reservoir, following the failure of intravenous infusion, is currently being evaluated in the CAROUSEL trial (NCT04443829). This clinical study also addresses the question of dose reduction when CAR-T are injected directly into the tumor region.
5. Conclusions
A better understanding of the origin and characteristics of the CNS immune cells, along with the growing amount of preclinical and clinical data on immunotherapies in B-cell malignancies, may lead to the development of therapeutic avenues to improve the prognosis of PCNSL.
Author Contributions
M.A., J.F. and C.S. performed the literature review, wrote the manuscript and created the Tables and Figures. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no competing financial interests.
References
- Houillier, C.; Soussain, C.; Ghesquières, H.; Soubeyran, P.; Chinot, O.; Taillandier, L.; Lamy, T.; Choquet, S.; Ahle, G.; Damaj, G.; et al. Management and Outcome of Primary CNS Lymphoma in the Modern Era: An LOC Network Study. Neurology 2020, 94, e1027–e1039. [Google Scholar] [CrossRef]
- Camilleri-Broët, S.; Crinière, E.; Broët, P.; Delwail, V.; Mokhtari, K.; Moreau, A.; Kujas, M.; Raphaël, M.; Iraqi, W.; Sautès-Fridman, C.; et al. A Uniform Activated B-Cell-like Immunophenotype Might Explain the Poor Prognosis of Primary Central Nervous System Lymphomas: Analysis of 83 Cases. Blood 2006, 107, 190–196. [Google Scholar] [CrossRef]
- Villano, J.L.; Koshy, M.; Shaikh, H.; Dolecek, T.A.; McCarthy, B.J. Age, Gender, and Racial Differences in Incidence and Survival in Primary CNS Lymphoma. Br. J. Cancer 2011, 105, 1414–1418. [Google Scholar] [CrossRef]
- Chapuy, B.; Roemer, M.G.M.; Stewart, C.; Tan, Y.; Abo, R.P.; Zhang, L.; Dunford, A.J.; Meredith, D.M.; Thorner, A.R.; Jordanova, E.S.; et al. Targetable Genetic Features of Primary Testicular and Primary Central Nervous System Lymphomas. Blood 2016, 127, 869–881. [Google Scholar] [CrossRef] [Green Version]
- Houillier, C.; Taillandier, L.; Dureau, S.; Lamy, T.; Laadhari, M.; Chinot, O.; Moluçon-Chabrot, C.; Soubeyran, P.; Gressin, R.; Choquet, S.; et al. Radiotherapy or Autologous Stem-Cell Transplantation for Primary CNS Lymphoma in Patients 60 Years of Age and Younger: Results of the Intergroup ANOCEF-GOELAMS Randomized Phase II PRECIS Study. J. Clin. Oncol. 2019, 37, 823–833. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, A.J.M.; Cwynarski, K.; Pulczynski, E.; Fox, C.P.; Schorb, E.; La Rosée, P.; Binder, M.; Fabbri, A.; Torri, V.; Minacapelli, E.; et al. Whole-Brain Radiotherapy or Autologous Stem-Cell Transplantation as Consolidation Strategies after High-Dose Methotrexate-Based Chemoimmunotherapy in Patients with Primary CNS Lymphoma: Results of the Second Randomisation of the International Extranodal Lymphoma Study Group-32 Phase 2 Trial. Lancet Haematol. 2017, 4, e510–e523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soussain, C.; Choquet, S.; Fourme, E.; Delgadillo, D.; Bouabdallah, K.; Ghesquières, H.; Damaj, G.; Dupriez, B.; Vargaftig, J.; Gonzalez, A.; et al. Intensive Chemotherapy with Thiotepa, Busulfan and Cyclophosphamide and Hematopoietic Stem Cell Rescue in Relapsed or Refractory Primary Central Nervous System Lymphoma and Intraocular Lymphoma: A Retrospective Study of 79 Cases. Haematologica 2012, 97, 1751–1756. [Google Scholar] [CrossRef] [PubMed]
- Langner-Lemercier, S.; Houillier, C.; Soussain, C.; Ghesquières, H.; Chinot, O.; Taillandier, L.; Soubeyran, P.; Lamy, T.; Morschhauser, F.; Benouaich-Amiel, A.; et al. Primary CNS Lymphoma at First Relapse/Progression: Characteristics, Management, and Outcome of 256 Patients from the French LOC Network. Neuro Oncol. 2016, 18, 1297–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreri, A.J.M.; Cwynarski, K.; Pulczynski, E.; Ponzoni, M.; Deckert, M.; Politi, L.S.; Torri, V.; Fox, C.P.; Rosée, P.L.; Schorb, E.; et al. Chemoimmunotherapy with Methotrexate, Cytarabine, Thiotepa, and Rituximab (MATRix Regimen) in Patients with Primary CNS Lymphoma: Results of the First Randomisation of the International Extranodal Lymphoma Study Group-32 (IELSG32) Phase 2 Trial. Lancet Haematol. 2016, 3, e217–e227. [Google Scholar] [CrossRef] [Green Version]
- Ambady, P.; Holdhoff, M.; Bonekamp, D.; Wong, F.; Grossman, S.A. Late Relapses in Primary CNS Lymphoma after Complete Remissions with High-Dose Methotrexate Monotherapy. CNS Oncol. 2015, 4, 393–398. [Google Scholar] [CrossRef]
- Rubenstein, J.L.; Fridlyand, J.; Shen, A.; Aldape, K.; Ginzinger, D.; Batchelor, T.; Treseler, P.; Berger, M.; McDermott, M.; Prados, M.; et al. Gene Expression and Angiotropism in Primary CNS Lymphoma. Blood 2006, 107, 3716–3723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tun, H.W.; Personett, D.; Baskerville, K.A.; Menke, D.M.; Jaeckle, K.A.; Kreinest, P.; Edenfield, B.; Zubair, A.C.; O’Neill, B.P.; Lai, W.R.; et al. Pathway Analysis of Primary Central Nervous System Lymphoma. Blood 2008, 111, 3200–3210. [Google Scholar] [CrossRef] [PubMed]
- Brunn, A.; Montesinos-Rongen, M.; Strack, A.; Reifenberger, G.; Mawrin, C.; Schaller, C.; Deckert, M. Expression Pattern and Cellular Sources of Chemokines in Primary Central Nervous System Lymphoma. Acta Neuropathol. 2007, 114, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Medawar, P.B. Immunity to Homologous Grafted Skin. III. The Fate of Skin Homographs Transplanted to the Brain, to Subcutaneous Tissue, and to the Anterior Chamber of the Eye. Br. J. Exp. Pathol. 1948, 29, 58–69. [Google Scholar] [PubMed]
- Aspelund, A.; Antila, S.; Proulx, S.T.; Karlsen, T.V.; Karaman, S.; Detmar, M.; Wiig, H.; Alitalo, K. A Dural Lymphatic Vascular System That Drains Brain Interstitial Fluid and Macromolecules. J. Exp. Med. 2015, 212, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Louveau, A.; Smirnov, I.; Keyes, T.J.; Eccles, J.D.; Rouhani, S.J.; Peske, J.D.; Derecki, N.C.; Castle, D.; Mandell, J.W.; Kevin, S.L.; et al. Structural and Functional Features of Central Nervous System Lymphatics. Nature 2015, 523, 337–341. [Google Scholar] [CrossRef]
- Absinta, M.; Ha, S.-K.; Nair, G.; Sati, P.; Luciano, N.J.; Palisoc, M.; Louveau, A.; Zaghloul, K.A.; Pittaluga, S.; Kipnis, J.; et al. Human and Nonhuman Primate Meninges Harbor Lymphatic Vessels That Can Be Visualized Noninvasively by MRI. eLife 2017, 6, e29738. [Google Scholar] [CrossRef]
- Iliff, J.J.; Wang, M.; Liao, Y.; Plogg, B.A.; Peng, W.; Gundersen, G.A.; Benveniste, H.; Vates, G.E.; Deane, R.; Goldman, S.A.; et al. A Paravascular Pathway Facilitates CSF Flow Through the Brain Parenchyma and the Clearance of Interstitial Solutes, Including Amyloid β. Sci. Transl. Med. 2012, 4, 147ra111. [Google Scholar] [CrossRef] [Green Version]
- Prinz, M.; Masuda, T.; Wheeler, M.A.; Quintana, F.J. Microglia and Central Nervous System–Associated Macrophages—From Origin to Disease Modulation. Annu. Rev. Immunol. 2021, 39, 251–277. [Google Scholar] [CrossRef]
- Cugurra, A.; Mamuladze, T.; Rustenhoven, J.; Dykstra, T.; Beroshvili, G.; Greenberg, Z.J.; Baker, W.; Papadopoulos, Z.; Drieu, A.; Blackburn, S.; et al. Skull and Vertebral Bone Marrow Are Myeloid Cell Reservoirs for the Meninges and CNS Parenchyma. Science 2021. [Google Scholar] [CrossRef]
- Brioschi, S.; Wang, W.-L.; Peng, V.; Wang, M.; Shchukina, I.; Greenberg, Z.J.; Bando, J.K.; Jaeger, N.; Czepielewski, R.S.; Swain, A.; et al. Heterogeneity of Meningeal B Cells Reveals a Lymphopoietic Niche at the CNS Borders. Science 2021, 373. [Google Scholar] [CrossRef]
- Herisson, F.; Frodermann, V.; Courties, G.; Rohde, D.; Sun, Y.; Vandoorne, K.; Wojtkiewicz, G.R.; Masson, G.S.; Vinegoni, C.; Kim, J.; et al. Direct Vascular Channels Connect Skull Bone Marrow and the Brain Surface Enabling Myeloid Cell Migration. Nat. Neurosci. 2018, 21, 1209–1217. [Google Scholar] [CrossRef]
- Ponzoni, M.; Berger, F.; Chassagne-Clement, C.; Tinguely, M.; Jouvet, A.; Ferreri, A.J.M.; Dell’Oro, S.; Terreni, M.R.; Doglioni, C.; Weis, J.; et al. Reactive Perivascular T-Cell Infiltrate Predicts Survival in Primary Central Nervous System B-Cell Lymphomas. Br. J. Haematol. 2007, 138, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Ou, A.; Sumrall, A.; Phuphanich, S.; Spetzler, D.; Gatalica, Z.; Xiu, J.; Michelhaugh, S.; Brenner, A.; Pandey, M.; Kesari, S.; et al. Primary CNS Lymphoma Commonly Expresses Immune Response Biomarkers. Neurooncol. Adv. 2020, 2, vdaa018. [Google Scholar] [CrossRef]
- Alame, M.; Cornillot, E.; Cacheux, V.; Rigau, V.; Costes-Martineau, V.; Lacheretz-Szablewski, V.; Colinge, J. The Immune Contexture of Primary Central Nervous System Diffuse Large B Cell Lymphoma Associates with Patient Survival and Specific Cell Signaling. Theranostics 2021, 11, 3565–3579. [Google Scholar] [CrossRef] [PubMed]
- Alame, M.; Pirel, M.; Costes-Martineau, V.; Bauchet, L.; Fabbro, M.; Tourneret, A.; De Oliveira, L.; Durand, L.; Roger, P.; Gonzalez, S.; et al. Characterisation of Tumour Microenvironment and Immune Checkpoints in Primary Central Nervous System Diffuse Large B Cell Lymphomas. Virchows Arch. 2020, 476, 891–902. [Google Scholar] [CrossRef] [PubMed]
- Marcelis, L.; Antoranz, A.; Delsupehe, A.-M.; Biesemans, P.; Ferreiro, J.F.; Debackere, K.; Vandenberghe, P.; Verhoef, G.; Gheysens, O.; Cattoretti, G.; et al. In-Depth Characterization of the Tumor Microenvironment in Central Nervous System Lymphoma Reveals Implications for Immune-Checkpoint Therapy. Cancer Immunol. Immunother. 2020, 69, 1751–1766. [Google Scholar] [CrossRef]
- Cho, H.; Kim, S.H.; Kim, S.-J.; Chang, J.H.; Yang, W.-I.; Suh, C.-O.; Kim, Y.R.; Jang, J.E.; Cheong, J.-W.; Min, Y.H.; et al. Programmed Cell Death 1 Expression Is Associated with Inferior Survival in Patients with Primary Central Nervous System Lymphoma. Oncotarget 2017, 8, 87317–87328. [Google Scholar] [CrossRef]
- Miyasato, Y.; Takashima, Y.; Takeya, H.; Yano, H.; Hayano, A.; Nakagawa, T.; Makino, K.; Takeya, M.; Yamanaka, R.; Komohara, Y. The Expression of PD-1 Ligands and IDO1 by Macrophage/Microglia in Primary Central Nervous System Lymphoma. J. Clin. Exp. Hematop. 2018, 58, 95–101. [Google Scholar] [CrossRef] [Green Version]
- Sasayama, T.; Tanaka, K.; Mizowaki, T.; Nagashima, H.; Nakamizo, S.; Tanaka, H.; Nishihara, M.; Mizukawa, K.; Hirose, T.; Itoh, T.; et al. Tumor-Associated Macrophages Associate with Cerebrospinal Fluid Interleukin-10 and Survival in Primary Central Nervous System Lymphoma (PCNSL). Brain Pathol. 2016, 26, 479–487. [Google Scholar] [CrossRef]
- Verma, R.; Balakrishnan, L.; Sharma, K.; Khan, A.A.; Advani, J.; Gowda, H.; Tripathy, S.P.; Suar, M.; Pandey, A.; Gandotra, S.; et al. A Network Map of Interleukin-10 Signaling Pathway. J. Cell Commun. Signal. 2016, 10, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Nguyen-Them, L.; Costopoulos, M.; Tanguy, M.-L.; Houillier, C.; Choquet, S.; Benanni, H.; Elias-Shamieh, R.; Armand, M.; Faivre, G.; Glaisner, S.; et al. The CSF IL-10 Concentration Is an Effective Diagnostic Marker in Immunocompetent Primary CNS Lymphoma and a Potential Prognostic Biomarker in Treatment-Responsive Patients. Eur. J. Cancer 2016, 61, 69–76. [Google Scholar] [CrossRef]
- Song, Y.; Zhang, W.; Zhang, L.; Wu, W.; Zhang, Y.; Han, X.; Yang, C.; Zhang, L.; Zhou, D. Cerebrospinal Fluid IL-10 and IL-10/IL-6 as Accurate Diagnostic Biomarkers for Primary Central Nervous System Large B-Cell Lymphoma. Sci. Rep. 2016, 6, 38671. [Google Scholar] [CrossRef]
- Venetz, D.; Ponzoni, M.; Schiraldi, M.; Ferreri, A.J.M.; Bertoni, F.; Doglioni, C.; Uguccioni, M. Perivascular Expression of CXCL9 and CXCL12 in Primary Central Nervous System Lymphoma: T-Cell Infiltration and Positioning of Malignant B Cells. Int. J. Cancer 2010, 127, 2300–2312. [Google Scholar] [CrossRef]
- Mathé, G.; Amiel, J.L.; Schwarzenberg, L.; Cattan, A.; Schneider, M. Haematopoietic Chimera in Man After Allogenic (Homologous) Bone-Marrow Transplantation. Br. Med. J. 1963, 2, 1633–1635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varadi, G.; Or, R.; Kapelushnik, J.; Naparstek, E.; Nagler, A.; Brautbar, C.; Amar, A.; Kirschbaum, M.; Samuel, S.; Slavin, S.; et al. Graft-versus-Lymphoma Effect after Allogeneic Peripheral Blood Stem Cell Transplantation for Primary Central Nervous System Lymphoma. Leuk. Lymphoma 1999, 34, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Mika, T.; Ladigan, S.; Baraniskin, A.; Vangala, D.; Seidel, S.; Hopfer, O.; Kiehl, M.; Schroers, R. Allogeneic Hematopoietic Stem Cell Transplantation for Primary Central Nervous System Lymphoma. Haematologica 2020, 105, e160–e163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karschnia, P.; Blobner, J.; Teske, N.; Schöberl, F.; Fitzinger, E.; Dreyling, M.; Tonn, J.-C.; Thon, N.; Subklewe, M.; von Baumgarten, L. CAR T-Cells for CNS Lymphoma: Driving into New Terrain? Cancers 2021, 13, 2503. [Google Scholar] [CrossRef]
- Coiffier, B.; Lepage, E.; Briere, J.; Herbrecht, R.; Tilly, H.; Bouabdallah, R.; Morel, P.; Van Den Neste, E.; Salles, G.; Gaulard, P.; et al. CHOP Chemotherapy plus Rituximab Compared with CHOP Alone in Elderly Patients with Diffuse Large-B-Cell Lymphoma. N. Engl. J. Med. 2002, 346, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Tilly, H.; Gomes da Silva, M.; Vitolo, U.; Jack, A.; Meignan, M.; Lopez-Guillermo, A.; Walewski, J.; André, M.; Johnson, P.W.; Pfreundschuh, M.; et al. Diffuse Large B-Cell Lymphoma (DLBCL): ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2015, 26 (Suppl. 5), v116–v125. [Google Scholar] [CrossRef]
- Rubenstein, J.; Ferreri, A.J.M.; Pittaluga, S. Primary Lymphoma of the Central Nervous System: Epidemiology, Pathology and Current Approaches to Diagnosis, Prognosis and Treatment. Leuk. Lymphoma 2008, 49, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Muldoon, L.L.; Soussain, C.; Jahnke, K.; Johanson, C.; Siegal, T.; Smith, Q.R.; Hall, W.A.; Hynynen, K.; Senter, P.D.; Peereboom, D.M.; et al. Chemotherapy Delivery Issues in Central Nervous System Malignancy: A Reality Check. J. Clin. Oncol. 2007, 25, 2295–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahnke, K.; Muldoon, L.L.; Varallyay, C.G.; Lewin, S.J.; Brown, R.D.; Kraemer, D.F.; Soussain, C.; Neuwelt, E.A. Efficacy and MRI of Rituximab and Methotrexate Treatment in a Nude Rat Model of CNS Lymphoma. Neuro Oncol. 2009, 11, 503–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batchelor, T.T.; Grossman, S.A.; Mikkelsen, T.; Ye, X.; Desideri, S.; Lesser, G.J. Rituximab Monotherapy for Patients with Recurrent Primary CNS Lymphoma. Neurology 2011, 76, 929–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birnbaum, T.; Stadler, E.A.; von Baumgarten, L.; Straube, A. Rituximab Significantly Improves Complete Response Rate in Patients with Primary CNS Lymphoma. J. Neurooncol. 2012, 109, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Holdhoff, M.; Ambady, P.; Abdelaziz, A.; Sarai, G.; Bonekamp, D.; Blakeley, J.; Grossman, S.A.; Ye, X. High-Dose Methotrexate with or without Rituximab in Newly Diagnosed Primary CNS Lymphoma. Neurology 2014, 83, 235–239. [Google Scholar] [CrossRef] [Green Version]
- Bromberg, J.E.C.; Issa, S.; Bakunina, K.; Minnema, M.C.; Seute, T.; Durian, M.; Cull, G.; Schouten, H.C.; Stevens, W.B.C.; Zijlstra, J.M.; et al. Rituximab in Patients with Primary CNS Lymphoma (HOVON 105/ALLG NHL 24): A Randomised, Open-Label, Phase 3 Intergroup Study. Lancet Oncol. 2019, 20, 216–228. [Google Scholar] [CrossRef]
- Schmitt, A.M.; Herbrand, A.K.; Fox, C.P.; Bakunina, K.; Bromberg, J.E.C.; Cwynarski, K.; Doorduijn, J.K.; Ferreri, A.J.M.; Illerhaus, G.; Issa, S.; et al. Rituximab in Primary Central Nervous System Lymphoma-A Systematic Review and Meta-Analysis. Hematol. Oncol. 2019, 37, 548–557. [Google Scholar] [CrossRef] [PubMed]
- Mutter, J.A.; Alig, S.; Lauer, E.M.; Esfahani, M.S.; Mitschke, J.; Kurtz, D.M.; Olsen, M.; Liu, C.L.; Jin, M.C.; Bleul, S.; et al. Matrix induction followed by autologous stem cell transplant or whole-brain irradiation in primary cns lymphoma. 7-year results of the ielsg32 randomized trial. Hematol. Oncol. 2021, 39. [Google Scholar] [CrossRef]
- Wei, S.C.; Duffy, C.R.; Allison, J.P. Fundamental Mechanisms of Immune Checkpoint Blockade Therapy. Cancer Discov. 2018, 8, 1069–1086. [Google Scholar] [CrossRef] [Green Version]
- Postow, M.A.; Chesney, J.; Pavlick, A.C.; Robert, C.; Grossmann, K.; McDermott, D.; Linette, G.P.; Meyer, N.; Giguere, J.K.; Agarwala, S.S.; et al. Nivolumab and Ipilimumab versus Ipilimumab in Untreated Melanoma. N. Engl. J. Med. 2015, 372, 2006–2017. [Google Scholar] [CrossRef] [Green Version]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.-P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients With Noncolorectal High Microsatellite Instability/Mismatch Repair-Deficient Cancer: Results From the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for First-Line Treatment of PD-L1-Selected Patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef] [PubMed]
- Armand, P.; Engert, A.; Younes, A.; Fanale, M.; Santoro, A.; Zinzani, P.L.; Timmerman, J.M.; Collins, G.P.; Ramchandren, R.; Cohen, J.B.; et al. Nivolumab for Relapsed/Refractory Classic Hodgkin Lymphoma After Failure of Autologous Hematopoietic Cell Transplantation: Extended Follow-Up of the Multicohort Single-Arm Phase II CheckMate 205 Trial. J. Clin. Oncol. 2018, 36, 1428–1439. [Google Scholar] [CrossRef]
- Chen, R.; Zinzani, P.L.; Lee, H.J.; Armand, P.; Johnson, N.A.; Brice, P.; Radford, J.; Ribrag, V.; Molin, D.; Vassilakopoulos, T.P.; et al. Pembrolizumab in Relapsed or Refractory Hodgkin Lymphoma: 2-Year Follow-up of KEYNOTE-087. Blood 2019, 134, 1144–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roemer, M.G.M.; Advani, R.H.; Ligon, A.H.; Natkunam, Y.; Redd, R.A.; Homer, H.; Connelly, C.F.; Sun, H.H.; Daadi, S.E.; Freeman, G.J.; et al. PD-L1 and PD-L2 Genetic Alterations Define Classical Hodgkin Lymphoma and Predict Outcome. J. Clin. Oncol. 2016, 34, 2690–2697. [Google Scholar] [CrossRef] [Green Version]
- Roemer, M.G.M.; Redd, R.A.; Cader, F.Z.; Pak, C.J.; Abdelrahman, S.; Ouyang, J.; Sasse, S.; Younes, A.; Fanale, M.; Santoro, A.; et al. Major Histocompatibility Complex Class II and Programmed Death Ligand 1 Expression Predict Outcome After Programmed Death 1 Blockade in Classic Hodgkin Lymphoma. J. Clin. Oncol. 2018, 36, 942–950. [Google Scholar] [CrossRef]
- Nayak, L.; Iwamoto, F.M.; LaCasce, A.; Mukundan, S.; Roemer, M.G.M.; Chapuy, B.; Armand, P.; Rodig, S.J.; Shipp, M.A. PD-1 Blockade with Nivolumab in Relapsed/Refractory Primary Central Nervous System and Testicular Lymphoma. Blood 2017, 129, 3071–3073. [Google Scholar] [CrossRef] [Green Version]
- Gavrilenko, A.N.; Volkov, N.P.; Shmidt, D.I.; Polushin, A.Y.; Kondakova, E.; Lepik, K.V.; Zalaylov, Y.R.; Popova, M.O.; Kulagin, A.D.; Afanasyev, B.V.; et al. Nivolumab in Primary CNS Lymphoma and Primary Testicular Lymphoma with CNS Involvement: Single Center Experience. Blood 2020, 136, 4. [Google Scholar] [CrossRef]
- Hoang-Xuan, K.; Houot, R.; Soussain, C.; Blonski, M.; Schmitt, A.; Delwail, V.; Damaj, G.L.; Ghesquieres, H.; Peyrade, F.; Tempescul, A.; et al. First Results of the Acsé Pembrolizumab Phase II in the Primary CNS Lymphoma (PCNSL) Cohort. Blood 2020, 136, 15–16. [Google Scholar] [CrossRef]
- Sadelain, M.; Rivière, I.; Brentjens, R. Targeting Tumours with Genetically Enhanced T Lymphocytes. Nat. Rev. Cancer 2003, 3, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jäger, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Locke, F.L.; Ghobadi, A.; Jacobson, C.A.; Miklos, D.B.; Lekakis, L.J.; Oluwole, O.O.; Lin, Y.; Braunschweig, I.; Hill, B.T.; Timmerman, J.M.; et al. Long-Term Safety and Activity of Axicabtagene Ciloleucel in Refractory Large B-Cell Lymphoma (ZUMA-1): A Single-Arm, Multicentre, Phase 1-2 Trial. Lancet Oncol. 2019, 20, 31–42. [Google Scholar] [CrossRef]
- Abramson, J.S.; Palomba, M.L.; Gordon, L.I.; Lunning, M.A.; Wang, M.; Arnason, J.; Mehta, A.; Purev, E.; Maloney, D.G.; Andreadis, C.; et al. Lisocabtagene Maraleucel for Patients with Relapsed or Refractory Large B-Cell Lymphomas (TRANSCEND NHL 001): A Multicentre Seamless Design Study. Lancet 2020, 396, 839–852. [Google Scholar] [CrossRef]
- Morris, E.C.; Neelapu, S.S.; Giavridis, T.; Sadelain, M. Cytokine release syndrome and associated neurotoxicity in cancer immunotherapy. Nat Rev Immunol. 2021, 17, 1–12. [Google Scholar] [CrossRef]
- Frigault, M.J.; Dietrich, J.; Martinez-Lage, M.; Leick, M.; Choi, B.D.; DeFilipp, Z.; Chen, Y.-B.; Abramson, J.; Crombie, J.; Armand, P.; et al. Tisagenlecleucel CAR T-Cell Therapy in Secondary CNS Lymphoma. Blood 2019, 134, 860–866. [Google Scholar] [CrossRef]
- Li, T.; Zhao, L.; Zhang, Y.; Xiao, Y.; Wang, D.; Huang, L.; Ma, L.; Chen, L.; Liu, S.; Long, X.; et al. CAR T-Cell Therapy Is Effective but Not Long-Lasting in B-Cell Lymphoma of the Brain. Front. Oncol. 2020, 10, 1306. [Google Scholar] [CrossRef]
- Alcantara, M.; Houillier, C.; Le Garff-Tavernier, M.; Souchet, L.; Roos-Weil, D.; Morel, V.; Uzunov, M.; Metz, C.; Nguyen-Quoc, S.; Jacque, N.; et al. CAR-T Cell Therapy in Primary Central Nervous System Lymphoma (PCNSL): The Experience of the French Network for Oculo-Cerebral Lymphomas (LOC). In Proceedings of the 16th International Conference on Malignant Lymphoma, Online, 18–22 June 2021. [Google Scholar]
- Parker, K.R.; Migliorini, D.; Perkey, E.; Yost, K.E.; Bhaduri, A.; Bagga, P.; Haris, M.; Wilson, N.E.; Liu, F.; Gabunia, K.; et al. Single-Cell Analyses Identify Brain Mural Cells Expressing CD19 as Potential Off-Tumor Targets for CAR-T Immunotherapies. Cell 2020, 183, 126–142.e17. [Google Scholar] [CrossRef]
- Abrey, L.E.; Batchelor, T.T.; Ferreri, A.J.M.; Gospodarowicz, M.; Pulczynski, E.J.; Zucca, E.; Smith, J.R.; Korfel, A.; Soussain, C.; DeAngelis, L.M.; et al. Report of an International Workshop to Standardize Baseline Evaluation and Response Criteria for Primary CNS Lymphoma. J. Clin. Oncol. 2005, 23, 5034–5043. [Google Scholar] [CrossRef]
- Sim, A.J.; Jain, M.D.; Figura, N.B.; Chavez, J.C.; Shah, B.D.; Khimani, F.; Lazaryan, A.; Krivenko, G.; Davila, M.L.; Liu, H.D.; et al. Radiation Therapy as a Bridging Strategy for CAR T Cell Therapy With Axicabtagene Ciloleucel in Diffuse Large B-Cell Lymphoma. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, 1012–1021. [Google Scholar] [CrossRef]
- Pinnix, C.C.; Gunther, J.R.; Dabaja, B.S.; Strati, P.; Fang, P.; Hawkins, M.C.; Adkins, S.; Westin, J.; Ahmed, S.; Fayad, L.; et al. Bridging Therapy Prior to Axicabtagene Ciloleucel for Relapsed/Refractory Large B-Cell Lymphoma. Blood Adv. 2020, 4, 2871–2883. [Google Scholar] [CrossRef] [PubMed]
- Pouzoulet, F.; Rezai, K.; Li, Z.; Yushi, Q.; Tun, H.W.; Labiod, D.; Bonnet-Boissinot, S.; Soussain, C. Preclinical Evaluation of Ibrutinib for Central Nervous System Lymphoma. Blood 2016, 128, 4170. [Google Scholar] [CrossRef]
- Goldwirt, L.; Beccaria, K.; Ple, A.; Sauvageon, H.; Mourah, S. Ibrutinib Brain Distribution: A Preclinical Study. Cancer Chemother Pharmacol. 2018, 81, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Chamoun, K.; Choquet, S.; Boyle, E.; Houillier, C.; Larrieu-Ciron, D.; Al Jijakli, A.; Delrieu, V.; Delwail, V.; Morschhauser, F.; Hoang-Xuan, K.; et al. Ibrutinib Monotherapy in Relapsed/Refractory CNS Lymphoma: A Retrospective Case Series. Neurology 2017, 88, 101–102. [Google Scholar] [CrossRef]
- Grommes, C.; Pastore, A.; Palaskas, N.; Tang, S.S.; Campos, C.; Schartz, D.; Codega, P.; Nichol, D.; Clark, O.; Hsieh, W.-Y.; et al. Ibrutinib Unmasks Critical Role of Bruton Tyrosine Kinase in Primary CNS Lymphoma. Cancer Discov. 2017, 7, 1018–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lionakis, M.S.; Dunleavy, K.; Roschewski, M.; Widemann, B.C.; Butman, J.A.; Schmitz, R.; Yang, Y.; Cole, D.E.; Melani, C.; Higham, C.S.; et al. Inhibition of B Cell Receptor Signaling by Ibrutinib in Primary CNS Lymphoma. Cancer Cell 2017, 31, 833–843.e5. [Google Scholar] [CrossRef] [Green Version]
- Soussain, C.; Choquet, S.; Blonski, M.; Leclercq, D.; Houillier, C.; Rezai, K.; Bijou, F.; Houot, R.; Boyle, E.; Gressin, R.; et al. Ibrutinib Monotherapy for Relapse or Refractory Primary CNS Lymphoma and Primary Vitreoretinal Lymphoma: Final Analysis of the Phase II “proof-of-Concept” ILOC Study by the Lymphoma Study Association (LYSA) and the French Oculo-Cerebral Lymphoma (LOC) Network. Eur. J. Cancer 2019, 117, 121–130. [Google Scholar] [CrossRef]
- Narita, Y.; Nagane, M.; Mishima, K.; Terui, Y.; Arakawa, Y.; Yonezawa, H.; Asai, K.; Fukuhara, N.; Sugiyama, K.; Shinojima, N.; et al. Phase I/II Study of Tirabrutinib, a Second-Generation Bruton’s Tyrosine Kinase Inhibitor, in Relapsed/Refractory Primary Central Nervous System Lymphoma. Neuro Oncol. 2021, 23, 122–133. [Google Scholar] [CrossRef]
- Rubenstein, J.L.; Geng, H.; Fraser, E.J.; Formaker, P.; Chen, L.; Sharma, J.; Killea, P.; Choi, K.; Ventura, J.; Kurhanewicz, J.; et al. Phase 1 Investigation of Lenalidomide/Rituximab plus Outcomes of Lenalidomide Maintenance in Relapsed CNS Lymphoma. Blood Adv. 2018, 2, 1595–1607. [Google Scholar] [CrossRef] [Green Version]
- Ghesquieres, H.; Chevrier, M.; Laadhari, M.; Chinot, O.; Choquet, S.; Moluçon-Chabrot, C.; Beauchesne, P.; Gressin, R.; Morschhauser, F.; Schmitt, A.; et al. Lenalidomide in Combination with Intravenous Rituximab (REVRI) in Relapsed/Refractory Primary CNS Lymphoma or Primary Intraocular Lymphoma: A Multicenter Prospective “proof of Concept” Phase II Study of the French Oculo-Cerebral Lymphoma (LOC) Network and the Lymphoma Study Association (LYSA). Ann. Oncol. 2019, 30, 621–628. [Google Scholar] [CrossRef]
- Tun, H.W.; Johnston, P.B.; DeAngelis, L.M.; Atherton, P.J.; Pederson, L.D.; Koenig, P.A.; Reeder, C.B.; Omuro, A.M.P.; Schiff, D.; O’Neill, B.; et al. Phase 1 Study of Pomalidomide and Dexamethasone for Relapsed/Refractory Primary CNS or Vitreoretinal Lymphoma. Blood 2018, 132, 2240–2248. [Google Scholar] [CrossRef] [Green Version]
- Dubovsky, J.A.; Beckwith, K.A.; Natarajan, G.; Woyach, J.A.; Jaglowski, S.; Zhong, Y.; Hessler, J.D.; Liu, T.-M.; Chang, B.Y.; Larkin, K.M.; et al. Ibrutinib Is an Irreversible Molecular Inhibitor of ITK Driving a Th1-Selective Pressure in T Lymphocytes. Blood 2013, 122, 2539–2549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, M.; Beckwith, K.; Do, P.; Mundy, B.L.; Gordon, A.; Lehman, A.M.; Maddocks, K.J.; Cheney, C.; Jones, J.A.; Flynn, J.M.; et al. Ibrutinib Treatment Improves T Cell Number and Function in CLL Patients. J. Clin. Investig. 2017, 127, 3052–3064. [Google Scholar] [CrossRef] [PubMed]
- Parry, H.M.; Mirajkar, N.; Cutmore, N.; Zuo, J.; Long, H.; Kwok, M.; Oldrieve, C.; Hudson, C.; Stankovic, T.; Paneesha, S.; et al. Long-Term Ibrutinib Therapy Reverses CD8+ T Cell Exhaustion in B Cell Chronic Lymphocytic Leukaemia. Front. Immunol. 2019, 10, 2832. [Google Scholar] [CrossRef] [Green Version]
- Stiff, A.; Trikha, P.; Wesolowski, R.; Kendra, K.; Hsu, V.; Uppati, S.; McMichael, E.; Duggan, M.; Campbell, A.; Keller, K.; et al. Myeloid-Derived Suppressor Cells Express Bruton’s Tyrosine Kinase and Can Be Depleted in Tumor Bearing Hosts by Ibrutinib Treatment. Cancer Res. 2016, 76, 2125–2136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aue, G.; Sun, C.; Liu, D.; Park, J.-H.; Pittaluga, S.; Tian, X.; Lee, E.; Soto, S.; Valdez, J.; Maric, I.; et al. Activation of Th1 Immunity within the Tumor Microenvironment Is Associated with Clinical Response to Lenalidomide in Chronic Lymphocytic Leukemia. J. Immunol. 2018, 201, 1967–1974. [Google Scholar] [CrossRef]
- Luptakova, K.; Rosenblatt, J.; Glotzbecker, B.; Mills, H.; Stroopinsky, D.; Kufe, T.; Vasir, B.; Arnason, J.; Tzachanis, D.; Zwicker, J.I.; et al. Lenalidomide Enhances Anti-Myeloma Cellular Immunity. Cancer Immunol. Immunother. 2013, 62, 39–49. [Google Scholar] [CrossRef]
- Ménard, C.; Rossille, D.; Dulong, J.; Nguyen, T.-T.; Papa, I.; Latour, M.; Bescher, N.; Bezier, I.; Chouteau, M.; Fest, T.; et al. Lenalidomide Triggers T-Cell Effector Functions in Vivo in Patients with Follicular Lymphoma. Blood Adv. 2021, 5, 2063–2074. [Google Scholar] [CrossRef]
- Li, Z.; Qiu, Y.; Personett, D.; Huang, P.; Edenfield, B.; Katz, J.; Babusis, D.; Tang, Y.; Shirely, M.A.; Moghaddam, M.F.; et al. Pomalidomide Shows Significant Therapeutic Activity against CNS Lymphoma with a Major Impact on the Tumor Microenvironment in Murine Models. PLoS ONE 2013, 8, e71754. [Google Scholar] [CrossRef]
- Lagrue, K.; Carisey, A.; Morgan, D.J.; Chopra, R.; Davis, D.M. Lenalidomide Augments Actin Remodeling and Lowers NK-Cell Activation Thresholds. Blood 2015, 126, 50–60. [Google Scholar] [CrossRef] [Green Version]
- Ruella, M.; Kenderian, S.S.; Shestova, O.; Fraietta, J.A.; Qayyum, S.; Zhang, Q.; Maus, M.V.; Liu, X.; Nunez-Cruz, S.; Klichinsky, M.; et al. The Addition of the BTK Inhibitor Ibrutinib to Anti-CD19 Chimeric Antigen Receptor T Cells (CART19) Improves Responses against Mantle Cell Lymphoma. Clin. Cancer Res. 2016, 22, 2684–2696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuramitsu, S.; Ohno, M.; Ohka, F.; Shiina, S.; Yamamichi, A.; Kato, A.; Tanahashi, K.; Motomura, K.; Kondo, G.; Kurimoto, M.; et al. Lenalidomide Enhances the Function of Chimeric Antigen Receptor T Cells against the Epidermal Growth Factor Receptor Variant III by Enhancing Immune Synapses. Cancer Gene Ther. 2015, 22, 487–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Walter, M.; Urak, R.; Weng, L.; Huynh, C.; Lim, L.; Wong, C.W.; Chang, W.-C.; Thomas, S.H.; Sanchez, J.F.; et al. Lenalidomide Enhances the Function of CS1 Chimeric Antigen Receptor-Redirected T Cells Against Multiple Myeloma. Clin. Cancer Res. 2018, 24, 106–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gauthier, J.; Hirayama, A.V.; Purushe, J.; Hay, K.A.; Lymp, J.; Li, D.; Yeung, C.; Sheih, A.; Pender, B.S.; Hawkins, R.M.; et al. Feasibility and Efficacy of CD19-Targeted CAR-T Cells with Concurrent Ibrutinib for CLL after Ibrutinib Failure. Blood 2020, 135, 1650–1660. [Google Scholar] [CrossRef]
- Das, R.K.; Vernau, L.; Grupp, S.A.; Barrett, D.M. Naïve T-Cell Deficits at Diagnosis and after Chemotherapy Impair Cell Therapy Potential in Pediatric Cancers. Cancer Discov. 2019, 9, 492–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neelapu, S.S.; Dickinson, M.; Ulrickson, M.L.; Oluwole, O.O.; Herrera, A.F.; Thieblemont, C.; Ujjani, C.S.; Lin, Y.; Riedell, P.A.; Kekre, N.; et al. Interim Analysis of ZUMA-12: A Phase 2 Study of Axicabtagene Ciloleucel (Axi-Cel) as First-Line Therapy in Patients (Pts) With High-Risk Large B Cell Lymphoma (LBCL). Blood 2020, 136, 49. [Google Scholar] [CrossRef]
- Mittendorf, E.A.; Zhang, H.; Barrios, C.H.; Saji, S.; Jung, K.H.; Hegg, R.; Koehler, A.; Sohn, J.; Iwata, H.; Telli, M.L.; et al. Neoadjuvant Atezolizumab in Combination with Sequential Nab-Paclitaxel and Anthracycline-Based Chemotherapy versus Placebo and Chemotherapy in Patients with Early-Stage Triple-Negative Breast Cancer (IMpassion031): A Randomised, Double-Blind, Phase 3 Trial. Lancet 2020, 396, 1090–1100. [Google Scholar] [CrossRef]
- Baas, P.; Scherpereel, A.; Nowak, A.K.; Fujimoto, N.; Peters, S.; Tsao, A.S.; Mansfield, A.S.; Popat, S.; Jahan, T.; Antonia, S.; et al. First-Line Nivolumab plus Ipilimumab in Unresectable Malignant Pleural Mesothelioma (CheckMate 743): A Multicentre, Randomised, Open-Label, Phase 3 Trial. Lancet 2021, 397, 375–386. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.-E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-Line Nivolumab plus Ipilimumab Combined with Two Cycles of Chemotherapy in Patients with Non-Small-Cell Lung Cancer (CheckMate 9LA): An International, Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2021, 22, 198–211. [Google Scholar] [CrossRef]
- Rubenstein, J.L.; Fridlyand, J.; Abrey, L.; Shen, A.; Karch, J.; Wang, E.; Issa, S.; Damon, L.; Prados, M.; McDermott, M.; et al. Phase I Study of Intraventricular Administration of Rituximab in Patients with Recurrent CNS and Intraocular Lymphoma. J. Clin. Oncol. 2007, 25, 1350–1356. [Google Scholar] [CrossRef]
- Rubenstein, J.L.; Li, J.; Chen, L.; Advani, R.; Drappatz, J.; Gerstner, E.; Batchelor, T.; Krouwer, H.; Hwang, J.; Auerback, G.; et al. Multicenter Phase 1 Trial of Intraventricular Immunochemotherapy in Recurrent CNS Lymphoma. Blood 2013, 121, 745–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadoch, C.; Li, J.; Wong, V.S.; Chen, L.; Cha, S.; Munster, P.; Lowell, C.A.; Shuman, M.A.; Rubenstein, J.L. Complement Activation and Intraventricular Rituximab Distribution in Recurrent Central Nervous System Lymphoma. Clin. Cancer Res. 2014, 20, 1029–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulazzani, M.; Fräßle, S.P.; von Mücke-Heim, I.; Langer, S.; Zhou, X.; Ishikawa-Ankerhold, H.; Leube, J.; Zhang, W.; Dötsch, S.; Svec, M.; et al. Long-Term in Vivo Microscopy of CAR T Cell Dynamics during Eradication of CNS Lymphoma in Mice. Proc. Natl. Acad. Sci. USA 2019, 116, 24275–24284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Huynh, C.; Urak, R.; Weng, L.; Walter, M.; Lim, L.; Vyas, V.; Chang, W.-C.; Aguilar, B.; Brito, A.; et al. The Cerebroventricular Environment Modifies CAR T Cells for Potent Activity against Both Central Nervous System and Systemic Lymphoma. Cancer Immunol. Res. 2021, 9, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Boulch, M.; Cazaux, M.; Loe-Mie, Y.; Thibaut, R.; Corre, B.; Lemaître, F.; Grandjean, C.L.; Garcia, Z.; Bousso, P. A Cross-Talk between CAR T Cell Subsets and the Tumor Microenvironment Is Essential for Sustained Cytotoxic Activity. Sci. Immunol. 2021, 6, eabd4344. [Google Scholar] [CrossRef]
Figure 1.
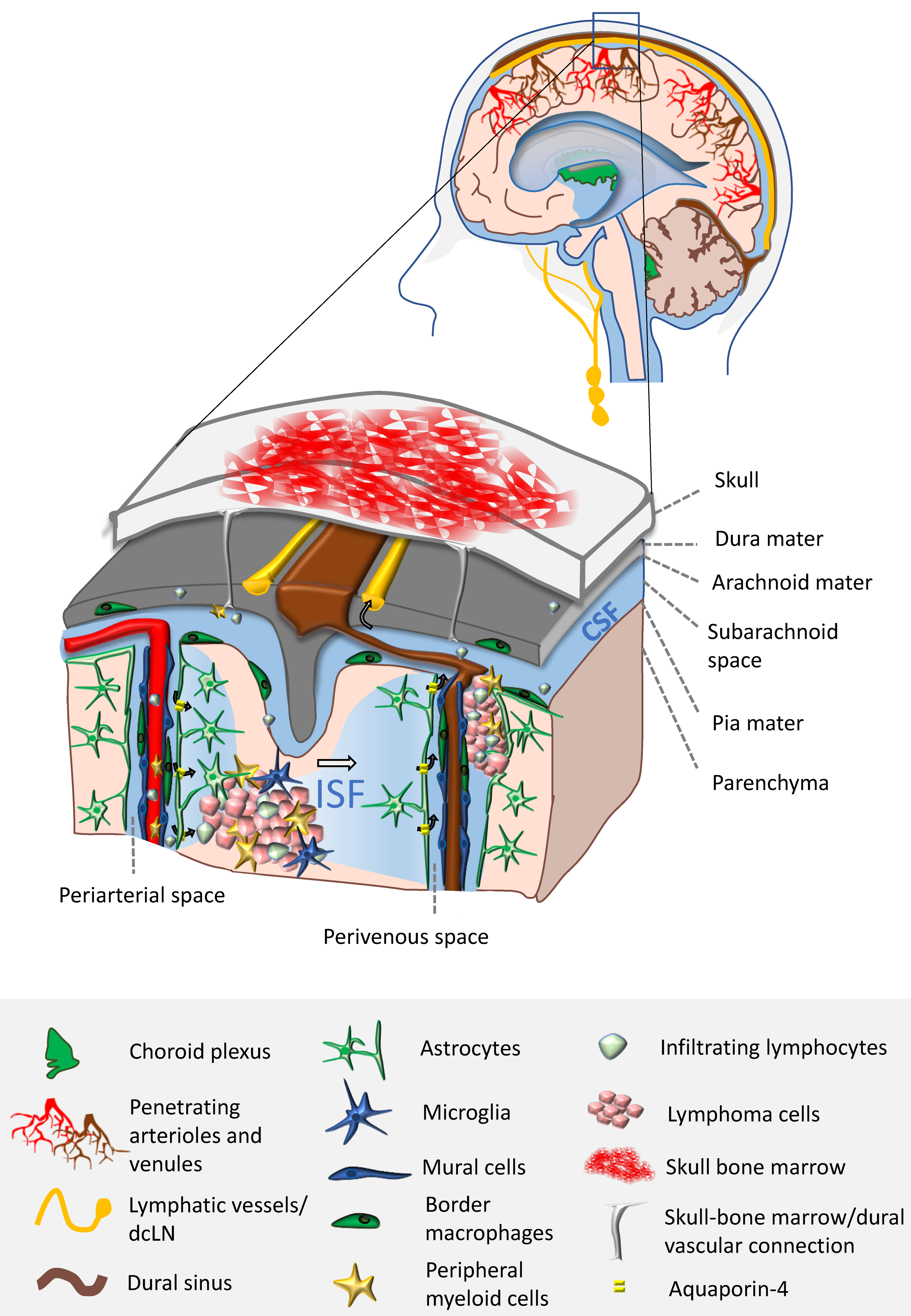
The TME in PCNSL is driven by the unique immune landscape and properties of the CNS. PCNSL are tumors that develop in alternative locations within the CNS. This has an impact on the TME cellular composition. When developing in cerebrospinal fluid (CSF) compartments (perivascular and meningeal spaces), lymphoma cells interact directly with border macrophages, lymphocytes, the glia limitans (formed by astrocytic endfeet), endothelial cells and mural cells (pericytes and smooth muscle cells). Inside the CNS parenchyma, tumor cells are in close contact with microglia, astrocytes and infiltrating immune cells: lymphocytes and peripheral myeloid cells. There are three potential sources of immune cells within PCNSL TME: derived from resident populations, from the blood and also from skull bone marrow reservoirs. Very recently, direct vascular connections between the skull bone marrow and the dura mater were found in mice. Antigens and immune cells from the TME of PCNSL are drained from the CSF compartment into deep cervical lymph nodes (dcLN) through meningeal lymphatic vessels, to potentially elicit anti-tumor responses. It is the role of the glymphatic system to clear CNS solutes, carrying antigens to the CSF compartment. Arrows indicate the directionality of CSF/Interstitial fluid (ISF) bulk flow, which is facilitated by Aquaporin-4 expressed on astrocytes.
Figure 1.
The TME in PCNSL is driven by the unique immune landscape and properties of the CNS. PCNSL are tumors that develop in alternative locations within the CNS. This has an impact on the TME cellular composition. When developing in cerebrospinal fluid (CSF) compartments (perivascular and meningeal spaces), lymphoma cells interact directly with border macrophages, lymphocytes, the glia limitans (formed by astrocytic endfeet), endothelial cells and mural cells (pericytes and smooth muscle cells). Inside the CNS parenchyma, tumor cells are in close contact with microglia, astrocytes and infiltrating immune cells: lymphocytes and peripheral myeloid cells. There are three potential sources of immune cells within PCNSL TME: derived from resident populations, from the blood and also from skull bone marrow reservoirs. Very recently, direct vascular connections between the skull bone marrow and the dura mater were found in mice. Antigens and immune cells from the TME of PCNSL are drained from the CSF compartment into deep cervical lymph nodes (dcLN) through meningeal lymphatic vessels, to potentially elicit anti-tumor responses. It is the role of the glymphatic system to clear CNS solutes, carrying antigens to the CSF compartment. Arrows indicate the directionality of CSF/Interstitial fluid (ISF) bulk flow, which is facilitated by Aquaporin-4 expressed on astrocytes.

Figure 2.
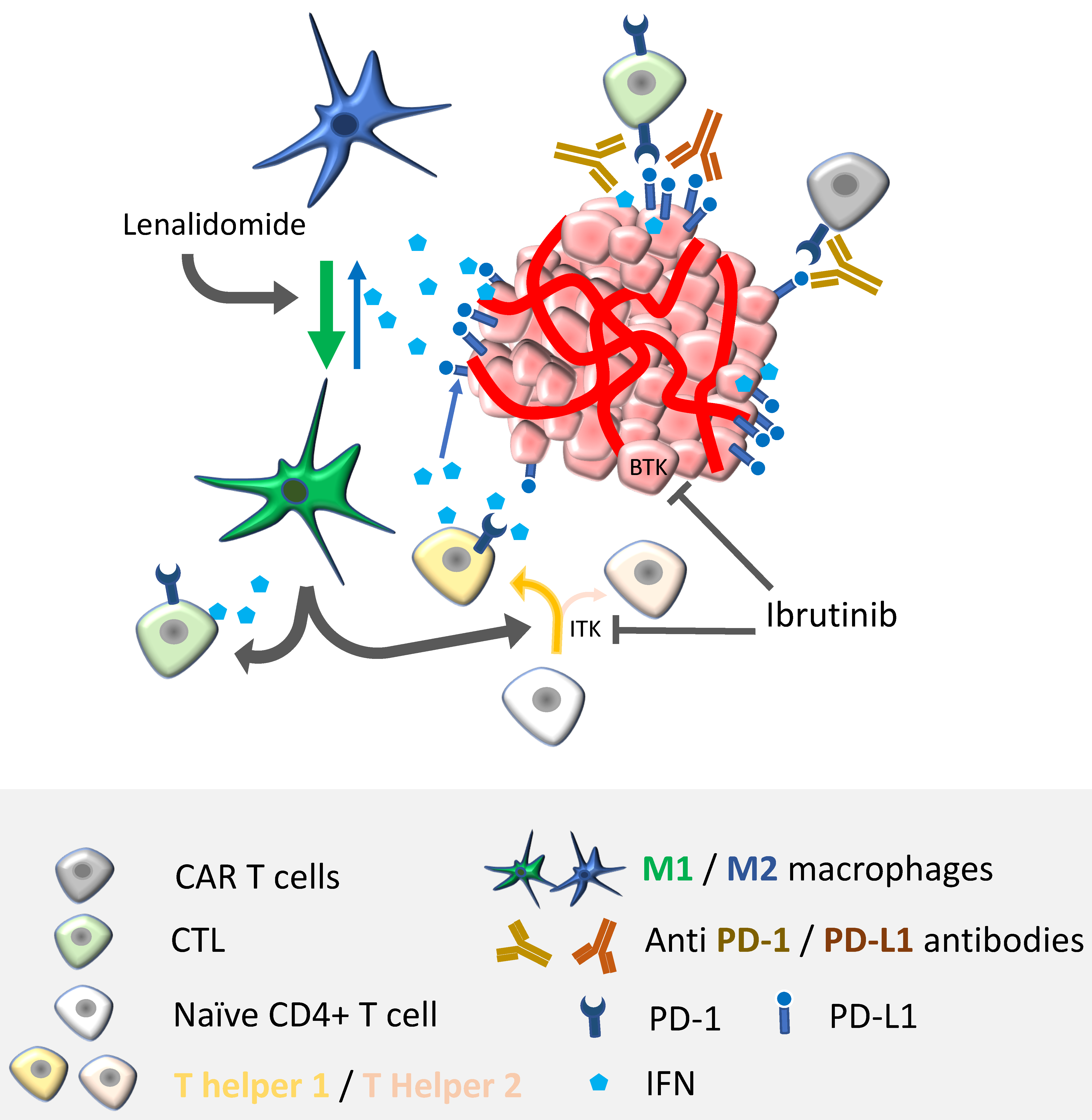
Perspectives for combination therapy in PCNSL. Besides just adding the effects from different treatments, one of the goals of combination immunotherapies is to find synergistic antitumor effects. Most of the direct antitumor activity is driven by antigen-specific or redirected T-cells (i.e., CAR-T cells). Therefore, unleashing antitumor response with immune checkpoint inhibitors should potentiate not only CAR-T cell responses, but also the effects of BTK/ITK inhibitors and immunomodulatory drugs, such as ibrutinib and lenalidomide/pomalidomide, respectively. Ibrutinib targets lymphoma cells by inhibiting BTK. Additionally, it regulates T-helper responses by limiting Th2 activation and inducing a shift in the Th2/Th1 ratio by targeting interleukin-2-inducible T-cell kinase (ITK). Lenalidomide/pomalidomide, by skewing M2-like macrophages towards M1 phenotypes, indirectly boosts cytotoxic T lymphocytes (CTL) activity and Th1 responses; therefore, enhancing IFN production, a cytokine that is well known for upregulating PD-L1 on tumor cells. Enhancing the adaptive antitumor immunity by using ibrutinib or lenalidomide/pomalidomide should, directly or indirectly, potentiate CAR-T cell functions.
Figure 2.
Perspectives for combination therapy in PCNSL. Besides just adding the effects from different treatments, one of the goals of combination immunotherapies is to find synergistic antitumor effects. Most of the direct antitumor activity is driven by antigen-specific or redirected T-cells (i.e., CAR-T cells). Therefore, unleashing antitumor response with immune checkpoint inhibitors should potentiate not only CAR-T cell responses, but also the effects of BTK/ITK inhibitors and immunomodulatory drugs, such as ibrutinib and lenalidomide/pomalidomide, respectively. Ibrutinib targets lymphoma cells by inhibiting BTK. Additionally, it regulates T-helper responses by limiting Th2 activation and inducing a shift in the Th2/Th1 ratio by targeting interleukin-2-inducible T-cell kinase (ITK). Lenalidomide/pomalidomide, by skewing M2-like macrophages towards M1 phenotypes, indirectly boosts cytotoxic T lymphocytes (CTL) activity and Th1 responses; therefore, enhancing IFN production, a cytokine that is well known for upregulating PD-L1 on tumor cells. Enhancing the adaptive antitumor immunity by using ibrutinib or lenalidomide/pomalidomide should, directly or indirectly, potentiate CAR-T cell functions.

Table 3.
Ongoing clinical trials of combined therapies targeting immune pathways. PCNSL: primary central nervous system lymphoma; sCNSL: secondary central nervous system lymphoma; R/R: relapsed or refractory; MTD: maximal tolerated dose; ORR: overall response rate; CR: complete response; PFS: progression-free survival.
Table 3.
Ongoing clinical trials of combined therapies targeting immune pathways. PCNSL: primary central nervous system lymphoma; sCNSL: secondary central nervous system lymphoma; R/R: relapsed or refractory; MTD: maximal tolerated dose; ORR: overall response rate; CR: complete response; PFS: progression-free survival.
| Clinicaltrials.gov Identification | Study Design | Treatment | Objective | Status |
|---|---|---|---|---|
| NCT04609046 | Phase I PCNSL first-line | Induction: methotrexate, rituximab, lenalidomide and nivolumab Maintenance: lenalidomide and nivolumab | Ongoing (estimated enrolment: 27 patients) | |
| NCT03703167 | Phase Ib R/R PCNSL and R/R sCNSL | Combination of ibrutinib with rituximab and lenalidomide with dose expansion of ibrutinib and lenalidomide | MTD of ibrutinib PFS | Ongoing (estimated enrolment: 40 patients) |
| NCT04938297 | Phase II PCNSL and sCNSL | Rituximab, zanubrutinib in combination with lenalidomide, followed by zanubrutinib or lenalidomide maintenance | ORR | Ongoing (estimated enrolment: 100 patients) |
| NCT04899427 | Phase II R/R PCNSL | Orelabrutinib combined with PD-1 inhibitor | ORR | Ongoing (estimated enrolment: 32 patients) |
| NCT04831658 | Phase II PCNSL first-line | BTK inhibitor, PD-1 inhibitor and formustine | CR rate | Ongoing (estimated enrolment: 40 patients) |
| NCT04737889 | Phase II PCNSL | Rituximab, lenalidomide combined with methotrexate and temozolomide | 2-year PFS | Ongoing (estimated enrolment: 30 patients) |
| NCT04688151 | Phase I PCNSL | Rituximab, acalabrutinib and durvalumab (RAD) | MTD Acalabrutinib | Ongoing |
| NCT04462328 | Phase I PCNSL and sCNSL R/R and first-line | Dose expansion of acalabrutinib and durvalumab | MTD Acalabrutinib | Ongoing (estimated enrolment: 21 patients) |
| NCT04421560 | Phase Ib/II R/R PCNSL | Pembrolizumab, ibrutinib and rituximab | 6-month PFS | Ongoing (estimated enrolment: 37 patients) |
| NCT03770416 | Phase I R/R PCNSL and sCNSL | Nivolumab and ibrutinib | ORR | Ongoing (estimated enrolment: 40 patients) |
| NCT04446962 | Phase Ib/II PCNSL first-line | Lenalidomide or ibrutinib in association with rituximab–methotrexate–procarbazine–vincristine (R-MPV) | MTD lenalidomide/ibrutinib CR rate at the end of induction | Ongoing (estimated enrolment: 92 patients in phase II) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Alcantara, M.; Fuentealba, J.; Soussain, C. Emerging Landscape of Immunotherapy for Primary Central Nervous System Lymphoma. Cancers 2021, 13, 5061. https://doi.org/10.3390/cancers13205061
AMA Style
Alcantara M, Fuentealba J, Soussain C. Emerging Landscape of Immunotherapy for Primary Central Nervous System Lymphoma. Cancers. 2021; 13(20):5061. https://doi.org/10.3390/cancers13205061
Chicago/Turabian StyleAlcantara, Marion, Jaime Fuentealba, and Carole Soussain. 2021. "Emerging Landscape of Immunotherapy for Primary Central Nervous System Lymphoma" Cancers 13, no. 20: 5061. https://doi.org/10.3390/cancers13205061
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.