
Daratumumab May Attenuate Cardiac Dysfunction Related to Carfilzomib in Patients with Relapsed/Refractory Multiple Myeloma: A Prospective Study

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Group Differences in Echocardiographic Changes after Treatment
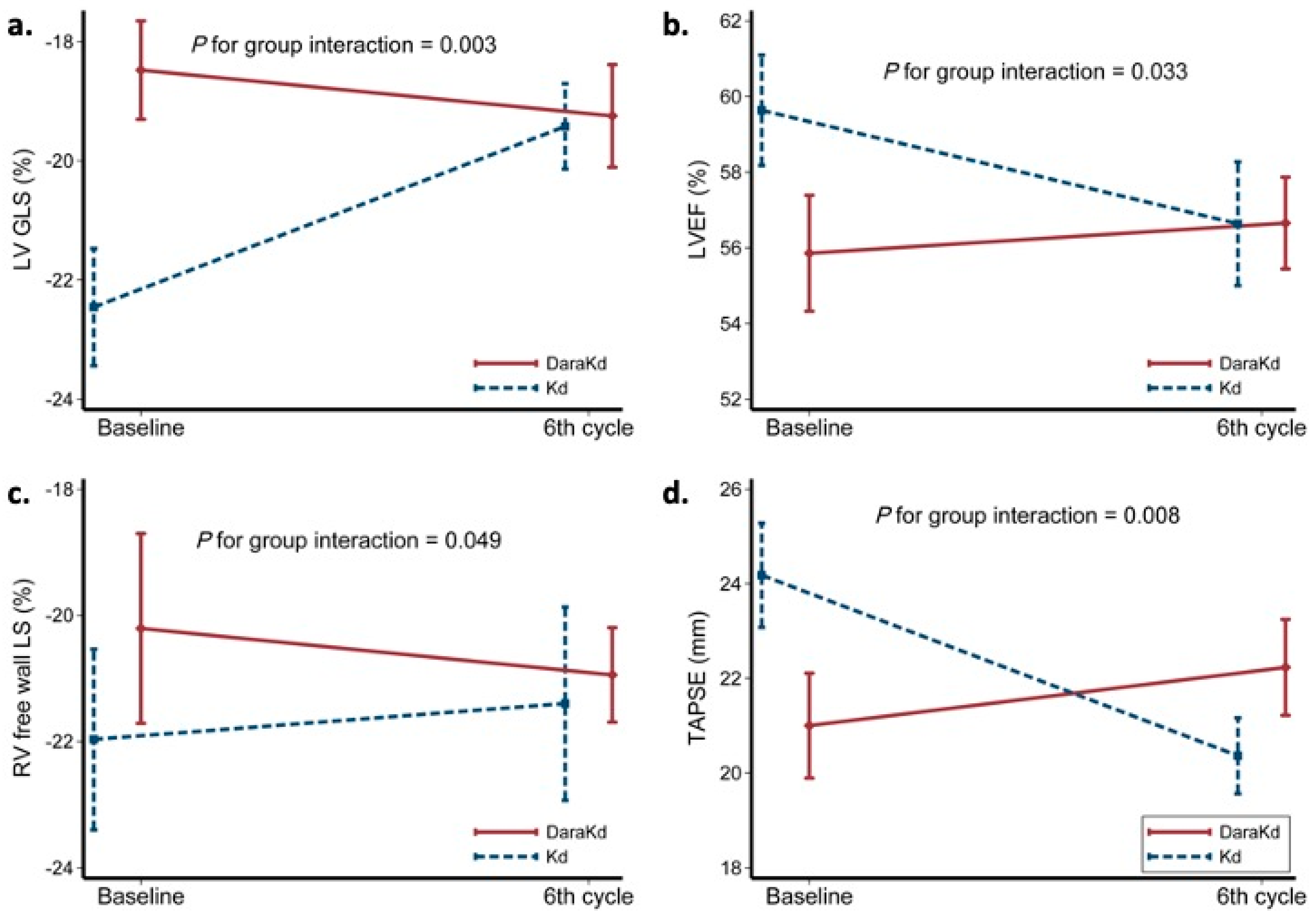
2.2.1. Markers of LV Systolic Function
2.2.2. Markers of LV Diastolic Function
2.2.3. Markers of RV Systolic Function
2.3. Group Differences in CVAEs
3. Discussion
4. Materials and Methods
4.1. Study Design and Population
4.2. Standard Echocardiography
4.3. Speckle Tracking Parameters
4.4. Follow-Up and Adjudication of Cardiovascular Adverse Events (CVAEs)
4.5. Statistical Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramasamy, K.; Gay, F.; Weisel, K.; Zweegman, S.; Mateos, M.V.; Richardson, P. Improving outcomes for patients with relapsed multiple myeloma: Challenges and considerations of current and emerging treatment options. Blood Rev. 2021, 49, 100808. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Moreau, P.; Terpos, E.; Mateos, M.V.; Zweegman, S.; Cook, G.; Delforge, M.; Hajek, R.; Schjesvold, F.; Cavo, M.; et al. Multiple Myeloma: EHA-ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-up. Hemasphere 2021, 5, e528. [Google Scholar] [CrossRef]
- Yee, A.J. The role of carfilzomib in relapsed/refractory multiple myeloma. Ther. Adv. Hematol. 2021, 12, 20406207211019612. [Google Scholar] [CrossRef]
- Bringhen, S.; Milan, A.; D’Agostino, M.; Ferri, C.; Wasch, R.; Gay, F.; Larocca, A.; Offidani, M.; Zweegman, S.; Terpos, E.; et al. Prevention, monitoring and treatment of cardiovascular adverse events in myeloma patients receiving carfilzomib A consensus paper by the European Myeloma Network and the Italian Society of Arterial Hypertension. J. Intern. Med. 2019, 286, 63–74. [Google Scholar] [CrossRef]
- Cornell, R.F.; Ky, B.; Weiss, B.M.; Dahm, C.N.; Gupta, D.K.; Du, L.; Carver, J.R.; Cohen, A.D.; Engelhardt, B.G.; Garfall, A.L.; et al. Prospective Study of Cardiac Events During Proteasome Inhibitor Therapy for Relapsed Multiple Myeloma. J. Clin. Oncol. 2019, 37, 1946–1955. [Google Scholar] [CrossRef]
- Rahman, M.R.; Ball, S.; Paz, P.; Elmassry, M.; Vutthikraivit, W.; Bandyopadhyay, D.; Lavie, C.J.; Fonarow, G.C. Heart Failure with Carfilzomib in Patients with Multiple Myeloma: A Meta-analysis of Randomized Controlled Trials. J. Card. Fail. 2021, 27, 610–612. [Google Scholar] [CrossRef]
- Dimopoulos, M.; Quach, H.; Mateos, M.V.; Landgren, O.; Leleu, X.; Siegel, D.; Weisel, K.; Yang, H.; Klippel, Z.; Zahlten-Kumeli, A.; et al. Carfilzomib, dexamethasone, and daratumumab versus carfilzomib and dexamethasone for patients with relapsed or refractory multiple myeloma (CANDOR): Results from a randomised, multicentre, open-label, phase 3 study. Lancet 2020, 396, 186–197. [Google Scholar] [CrossRef]
- Fernandez, J.E.; Deaglio, S.; Donati, D.; Beusan, I.S.; Corno, F.; Aranega, A.; Forni, M.; Falini, B.; Malavasi, F. Analysis of the distribution of human CD38 and of its ligand CD31 in normal tissues. J. Biol. Regul. Homeost. Agents 1998, 12, 81–91. [Google Scholar]
- Yarbro, J.R.; Emmons, R.S.; Pence, B.D. Macrophage Immunometabolism and Inflammaging: Roles of Mitochondrial Dysfunction, Cellular Senescence, CD38, and NAD. Immunometabolism 2020, 2, e200026. [Google Scholar] [CrossRef]
- Boslett, J.; Hemann, C.; Christofi, F.L.; Zweier, J.L. Characterization of CD38 in the major cell types of the heart: Endothelial cells highly express CD38 with activation by hypoxia-reoxygenation triggering NAD(P)H depletion. Am. J. Physiol. Cell Physiol. 2018, 314, C297–C309. [Google Scholar] [CrossRef]
- Zhao, L.; Wang, B.; Zhang, W.; Sun, L. Effect of miR-499a-5p on damage of cardiomyocyte induced by hypoxia-reoxygenation via downregulating CD38 protein. J. Cell. Biochem. 2020, 121, 996–1004. [Google Scholar] [CrossRef]
- Boslett, J.; Reddy, N.; Alzarie, Y.A.; Zweier, J.L. Inhibition of CD38 with the Thiazoloquin(az)olin(on)e 78c Protects the Heart against Postischemic Injury. J. Pharmacol. Exp. Ther. 2019, 369, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Avet-Loiseau, H.; Fonseca, R.; Siegel, D.; Dimopoulos, M.A.; Spicka, I.; Masszi, T.; Hajek, R.; Rosinol, L.; Goranova-Marinova, V.; Mihaylov, G.; et al. Carfilzomib significantly improves the progression-free survival of high-risk patients in multiple myeloma. Blood 2016, 128, 1174–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavriatopoulou, M.; Terpos, E.; Ntanasis-Stathopoulos, I.; Malandrakis, P.; Eleutherakis-Papaiakovou, E.; Papatheodorou, A.; Kanellias, N.; Migkou, M.; Fotiou, D.; Dialoupi, I.; et al. Consolidation with carfilzomib, lenalidomide, and dexamethasone (KRd) following ASCT results in high rates of minimal residual disease negativity and improves bone metabolism, in the absence of bisphosphonates, among newly diagnosed patients with multiple myeloma. Blood Cancer J. 2020, 10, 25. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Katodritou, E.; Kyrtsonis, M.C.; Douka, V.; Spanoudakis, E.; Papatheodorou, A.; Eleutherakis-Papaiakovou, E.; Kanellias, N.; Gavriatopoulou, M.; et al. Carfilzomib Improves Bone Metabolism in Patients with Advanced Relapsed/Refractory Multiple Myeloma: Results of the CarMMa Study. Cancers 2021, 13, 1257. [Google Scholar] [CrossRef] [PubMed]
- Bringhen, S.; Milan, A.; Ferri, C.; Wasch, R.; Gay, F.; Larocca, A.; Salvini, M.; Terpos, E.; Goldschmidt, H.; Cavo, M.; et al. Cardiovascular adverse events in modern myeloma therapy—Incidence and risks. A review from the European Myeloma Network (EMN) and Italian Society of Arterial Hypertension (SIIA). Haematologica 2018, 103, 1422–1432. [Google Scholar] [CrossRef]
- Astarita, A.; Mingrone, G.; Airale, L.; Vallelonga, F.; Covella, M.; Catarinella, C.; Cesareo, M.; Bruno, G.; Leone, D.; Giordana, C.; et al. Multiple Myeloma Patients Undergoing Carfilzomib: Development and Validation of a Risk Score for Cardiovascular Adverse Events Prediction. Cancers 2021, 13, 1631. [Google Scholar] [CrossRef]
- Bruno, G.; Bringhen, S.; Maffei, I.; Iannaccone, A.; Crea, T.; Ravera, A.; Astarita, A.; Vallelonga, F.; Salvini, M.; Gay, F.; et al. Cardiovascular Organ Damage and Blood Pressure Levels Predict Adverse Events in Multiple Myeloma Patients Undergoing Carfilzomib Therapy. Cancers 2019, 11, 622. [Google Scholar] [CrossRef] [Green Version]
- Bishnoi, R.; Xie, Z.; Shah, C.; Bian, J.; Murthy, H.S.; Wingard, J.R.; Farhadfar, N. Real-world experience of carfilzomib-associated cardiovascular adverse events: SEER-Medicare data set analysis. Cancer Med. 2021, 10, 70–78. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Moreau, P.; Palumbo, A.; Joshua, D.; Pour, L.; Hajek, R.; Facon, T.; Ludwig, H.; Oriol, A.; Goldschmidt, H.; et al. Carfilzomib and dexamethasone versus bortezomib and dexamethasone for patients with relapsed or refractory multiple myeloma (ENDEAVOR): A randomised, phase 3, open-label, multicentre study. Lancet Oncol. 2016, 17, 27–38. [Google Scholar] [CrossRef]
- Orlowski, R.Z.; Moreau, P.; Niesvizky, R.; Ludwig, H.; Oriol, A.; Chng, W.J.; Goldschmidt, H.; Yang, Z.; Kimball, A.S.; Dimopoulos, M. Carfilzomib-Dexamethasone Versus Bortezomib-Dexamethasone in Relapsed or Refractory Multiple Myeloma: Updated Overall Survival, Safety, and Subgroups. Clin. Lymphoma Myeloma Leuk. 2019, 19, 522–530.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, A.K.; Rajkumar, S.V.; Dimopoulos, M.A.; Masszi, T.; Spicka, I.; Oriol, A.; Hajek, R.; Rosinol, L.; Siegel, D.S.; Mihaylov, G.G.; et al. Carfilzomib, lenalidomide, and dexamethasone for relapsed multiple myeloma. N. Engl. J. Med. 2015, 372, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Waxman, A.J.; Clasen, S.; Hwang, W.T.; Garfall, A.; Vogl, D.T.; Carver, J.; O’Quinn, R.; Cohen, A.D.; Stadtmauer, E.A.; Ky, B.; et al. Carfilzomib-Associated Cardiovascular Adverse Events: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, e174519. [Google Scholar] [CrossRef]
- Zhao, F.; Yang, B.; Wang, J.; Zhang, R.; Liu, J.; Yin, F.; Xu, W.; He, C. Incidence and risk of cardiac toxicities in patients with relapsed and refractory multiple myeloma treated with carfilzomib. Drug Des. Dev. Ther. 2018, 12, 1525–1531. [Google Scholar] [CrossRef] [Green Version]
- Leleu, X.; Beksac, M.; Chou, T.; Dimopoulos, M.; Yoon, S.S.; Prince, H.M.; Pour, L.; Shelekhova, T.; Chari, A.; Khurana, M.; et al. Efficacy and safety of weekly carfilzomib (70 mg/m2), dexamethasone, and daratumumab (KdD70) is comparable to twice-weekly KdD56 while being a more convenient dosing option: A cross-study comparison of the CANDOR and EQUULEUS studies. Leuk. Lymphoma 2021, 62, 358–367. [Google Scholar] [CrossRef]
- Latif, A.; Kapoor, V.; Lateef, N.; Ahsan, M.J.; Usman, R.M.; Malik, S.U.; Ahmad, N.; Rosko, N.; Rudoni, J.; William, P.; et al. Incidence and Management of Carfilzomib-induced Cardiovascular Toxicity; A Systematic Review and Meta-analysis. Cardiovasc. Hematol. Disord. Drug Targets 2021, 21, 30–45. [Google Scholar] [CrossRef]
- Dimopoulos, M.A.; Roussou, M.; Gavriatopoulou, M.; Psimenou, E.; Ziogas, D.; Eleutherakis-Papaiakovou, E.; Fotiou, D.; Migkou, M.; Kanellias, N.; Panagiotidis, I.; et al. Cardiac and renal complications of carfilzomib in patients with multiple myeloma. Blood Adv. 2017, 1, 449–454. [Google Scholar] [CrossRef] [Green Version]
- Grandin, E.W.; Ky, B.; Cornell, R.F.; Carver, J.; Lenihan, D.J. Patterns of cardiac toxicity associated with irreversible proteasome inhibition in the treatment of multiple myeloma. J. Card. Fail. 2015, 21, 138–144. [Google Scholar] [CrossRef]
- Iannaccone, A.; Bruno, G.; Ravera, A.; Gay, F.; Salvini, M.; Bringhen, S.; Sabia, L.; Avenatti, E.; Veglio, F.; Milan, A. Evaluation of Cardiovascular Toxicity Associated with Treatments Containing Proteasome Inhibitors in Multiple Myeloma Therapy. High Blood Press. Cardiovasc. Prev. 2018, 25, 209–218. [Google Scholar] [CrossRef]
- Rosenthal, A.; Luthi, J.; Belohlavek, M.; Kortum, K.M.; Mookadam, F.; Mayo, A.; Fonseca, R.; Bergsagel, P.L.; Reeder, C.B.; Mikhael, J.R.; et al. Carfilzomib and the cardiorenal system in myeloma: An endothelial effect? Blood Cancer J. 2016, 6, e384. [Google Scholar] [CrossRef]
- Curigliano, G.; Lenihan, D.; Fradley, M.; Ganatra, S.; Barac, A.; Blaes, A.; Herrmann, J.; Porter, C.; Lyon, A.R.; Lancellotti, P.; et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations. Ann. Oncol. 2020, 31, 171–190. [Google Scholar] [CrossRef] [Green Version]
- Narayan, H.K.; Finkelman, B.; French, B.; Plappert, T.; Hyman, D.; Smith, A.M.; Margulies, K.B.; Ky, B. Detailed Echocardiographic Phenotyping in Breast Cancer Patients: Associations with Ejection Fraction Decline, Recovery, and Heart Failure Symptoms Over 3 Years of Follow-Up. Circulation 2017, 135, 1397–1412. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Negishi, T.; Somerset, E.; Negishi, K.; Penicka, M.; Lemieux, J.; Aakhus, S.; Miyazaki, S.; Shirazi, M.; Galderisi, M.; et al. Strain-Guided Management of Potentially Cardiotoxic Cancer Therapy. J. Am. Coll. Cardiol. 2021, 77, 392–401. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Munoz, D.R.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Mingrone, G.; Astarita, A.; Airale, L.; Maffei, I.; Cesareo, M.; Crea, T.; Bruno, G.; Leone, D.; Avenatti, E.; Catarinella, C.; et al. Effects of Carfilzomib Therapy on Left Ventricular Function in Multiple Myeloma Patients. Front. Cardiovasc. Med. 2021, 8, 645678. [Google Scholar] [CrossRef] [PubMed]
- Gavazzoni, M.; Lombardi, C.M.; Vizzardi, E.; Gorga, E.; Sciatti, E.; Rossi, L.; Belotti, A.; Rossi, G.; Metra, M.; Raddino, R. Irreversible proteasome inhibition with carfilzomib as first line therapy in patients with newly diagnosed multiple myeloma: Early in vivo cardiovascular effects. Eur. J. Pharmacol. 2018, 838, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Abe, Y.; Kobayashi, T.; Narita, K.; Kobayashi, H.; Kitadate, A.; Miura, D.; Takeuchi, M.; Matsue, K. Left ventricular diastolic function as a possible predictor of severe carfilzomib-induced cardiovascular events. Blood Adv. 2019, 3, 1725–1728. [Google Scholar] [CrossRef]
- Mathur, P.; Thanendrarajan, S.; Lopez-Candales, A. Severe Right-Sided Heart Failure and Pulmonary Hypertension with Carfilzomib Treatment in Multiple Myeloma. Heart Views 2020, 21, 296–299. [Google Scholar] [CrossRef]
- McGregor, P.C.; Boosalis, V.; Aragam, J. Carfilzomib-induced pulmonary hypertension with associated right ventricular dysfunction: A case report. SAGE Open Med. Case Rep. 2021, 9, 2050313X21994031. [Google Scholar] [CrossRef]
- Boczar, K.E.; Aseyev, O.; Sulpher, J.; Johnson, C.; Burwash, I.G.; Turek, M.; Dent, S.; Dwivedi, G. Right heart function deteriorates in breast cancer patients undergoing anthracycline-based chemotherapy. Echo Res. Pract. 2016, 3, 79–84. [Google Scholar] [CrossRef] [Green Version]
- Chhikara, S.; Hooks, M.; Athwal, P.S.S.; Hughes, A.; Ismail, M.F.; Joppa, S.; Velangi, P.S.; Nijjar, P.S.; Blaes, A.H.; Shenoy, C. Long-term prognostic value of right ventricular dysfunction on cardiovascular magnetic resonance imaging in anthracycline-treated cancer survivors. Eur. Heart J. Cardiovasc. Imaging 2021. [Google Scholar] [CrossRef]
- Keramida, K.; Farmakis, D. Right ventricular involvement in cancer therapy-related cardiotoxicity: The emerging role of strain echocardiography. Heart Fail. Rev. 2021, 26, 1189–1193. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Huang, J.; Wu, W.; Ta, S.; Xie, X. The impact of right ventricular function on prognosis in patients with stage III non-small cell lung cancer after concurrent chemoradiotherapy. Int. J. Cardiovasc. Imaging 2019, 35, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Tannous, P.; Zhu, H.; Nemchenko, A.; Berry, J.M.; Johnstone, J.L.; Shelton, J.M.; Miller, F.J., Jr.; Rothermel, B.A.; Hill, J.A. Intracellular protein aggregation is a proximal trigger of cardiomyocyte autophagy. Circulation 2008, 117, 3070–3078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasinoff, B.B.; Patel, D.; Wu, X. Molecular Mechanisms of the Cardiotoxicity of the Proteasomal-Targeted Drugs Bortezomib and Carfilzomib. Cardiovasc. Toxicol. 2017, 17, 237–250. [Google Scholar] [CrossRef]
- Kastritis, E.; Laina, A.; Georgiopoulos, G.; Gavriatopoulou, M.; Papanagnou, E.D.; Eleutherakis-Papaiakovou, E.; Fotiou, D.; Kanellias, N.; Dialoupi, I.; Makris, N.; et al. Carfilzomib-induced endothelial dysfunction, recovery of proteasome activity, and prediction of cardiovascular complications: A prospective study. Leukemia 2021, 35, 1418–1427. [Google Scholar] [CrossRef]
- Efentakis, P.; Doerschmann, H.; Witzler, C.; Siemer, S.; Nikolaou, P.E.; Kastritis, E.; Stauber, R.; Dimopoulos, M.A.; Wenzel, P.; Andreadou, I.; et al. Investigating the Vascular Toxicity Outcomes of the Irreversible Proteasome Inhibitor Carfilzomib. Int. J. Mol. Sci. 2020, 21, 5185. [Google Scholar] [CrossRef]
- Efentakis, P.; Kremastiotis, G.; Varela, A.; Nikolaou, P.E.; Papanagnou, E.D.; Davos, C.H.; Tsoumani, M.; Agrogiannis, G.; Konstantinidou, A.; Kastritis, E.; et al. Molecular mechanisms of carfilzomib-induced cardiotoxicity in mice and the emerging cardioprotective role of metformin. Blood 2019, 133, 710–723. [Google Scholar] [CrossRef] [Green Version]
- Tantawy, M.; Chekka, L.M.; Huang, Y.; Garrett, T.J.; Singh, S.; Shah, C.P.; Cornell, R.F.; Baz, R.C.; Fradley, M.G.; Waheed, N.; et al. Lactate Dehydrogenase B and Pyruvate Oxidation Pathway Associated with Carfilzomib-Related Cardiotoxicity in Multiple Myeloma Patients: Result of a Multi-Omics Integrative Analysis. Front. Cardiovasc. Med. 2021, 8, 645122. [Google Scholar] [CrossRef]
- Imam, F.; Al-Harbi, N.O.; Al-Harbi, M.M.; Ansari, M.A.; Almutairi, M.M.; Alshammari, M.; Almukhlafi, T.S.; Ansari, M.N.; Aljerian, K.; Ahmad, S.F. Apremilast reversed carfilzomib-induced cardiotoxicity through inhibition of oxidative stress, NF-kappaB and MAPK signaling in rats. Toxicol. Mech. Methods 2016, 26, 700–708. [Google Scholar] [CrossRef]
- Imam, F.; Al-Harbi, N.O.; Al-Harbia, M.M.; Korashy, H.M.; Ansari, M.A.; Sayed-Ahmed, M.M.; Nagi, M.N.; Iqbal, M.; Khalid Anwer, M.; Kazmi, I.; et al. Rutin Attenuates Carfilzomib-Induced Cardiotoxicity through Inhibition of NF-kappaB, Hypertrophic Gene Expression and Oxidative Stress. Cardiovasc. Toxicol. 2017, 17, 58–66. [Google Scholar] [CrossRef]
- Wei, W.; Graeff, R.; Yue, J. Roles and mechanisms of the CD38/cyclic adenosine diphosphate ribose/Ca2+ signaling pathway. World J. Biol. Chem. 2014, 5, 58–67. [Google Scholar] [CrossRef] [Green Version]
- Zuo, W.; Liu, N.; Zeng, Y.; Liu, Y.; Li, B.; Wu, K.; Xiao, Y.; Liu, Q. CD38: A Potential Therapeutic Target in Cardiovascular Disease. Cardiovasc. Drugs Ther. 2021, 35, 815–828. [Google Scholar] [CrossRef]
- Lin, W.K.; Bolton, E.L.; Cortopassi, W.A.; Wang, Y.; O’Brien, F.; Maciejewska, M.; Jacobson, M.P.; Garnham, C.; Ruas, M.; Parrington, J.; et al. Synthesis of the Ca2+-mobilizing messengers NAADP and cADPR by intracellular CD38 enzyme in the mouse heart: Role in beta-adrenoceptor signaling. J. Biol. Chem. 2017, 292, 13243–13257. [Google Scholar] [CrossRef] [Green Version]
- Tannous, C.; Booz, G.W.; Altara, R.; Muhieddine, D.H.; Mericskay, M.; Refaat, M.M.; Zouein, F.A. Nicotinamide adenine dinucleotide: Biosynthesis, consumption and therapeutic role in cardiac diseases. Acta Physiol. 2021, 231, e13551. [Google Scholar] [CrossRef]
- Amici, S.A.; Young, N.A.; Narvaez-Miranda, J.; Jablonski, K.A.; Arcos, J.; Rosas, L.; Papenfuss, T.L.; Torrelles, J.B.; Jarjour, W.N.; Guerau-de-Arellano, M. CD38 Is Robustly Induced in Human Macrophages and Monocytes in Inflammatory Conditions. Front. Immunol. 2018, 9, 1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Li, L.; Zhang, Q.; Wei, Q.; Lin, J.; Jia, J.; Zhang, J.; Yan, T.; Lv, Y.; Jiang, X.; et al. CD38 Causes Autophagic Flux Inhibition and Cardiac Dysfunction Through a Transcriptional Inhibition Pathway Under Hypoxia/Ischemia Conditions. Front. Cell Dev. Biol. 2020, 8, 191. [Google Scholar] [CrossRef]
- Gul, R.; Park, D.R.; Shawl, A.I.; Im, S.Y.; Nam, T.S.; Lee, S.H.; Ko, J.K.; Jang, K.Y.; Kim, D.; Kim, U.H. Nicotinic Acid Adenine Dinucleotide Phosphate (NAADP) and Cyclic ADP-Ribose (cADPR) Mediate Ca2+ Signaling in Cardiac Hypertrophy Induced by beta-Adrenergic Stimulation. PLoS ONE 2016, 11, e0149125. [Google Scholar] [CrossRef]
- Cheng, Y.; Sun, F.; D’Souza, A.; Dhakal, B.; Pisano, M.; Chhabra, S.; Stolley, M.; Hari, P.; Janz, S. Autonomic nervous system control of multiple myeloma. Blood Rev. 2021, 46, 100741. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.H.; Hong, X.; Zhao, N.; Liu, X.H.; Xiao, Y.F.; Chen, T.T.; Deng, L.B.; Wang, X.L.; Wang, J.B.; Ji, G.J.; et al. CD38 promotes angiotensin II-induced cardiac hypertrophy. J. Cell. Mol. Med. 2017, 21, 1492–1502. [Google Scholar] [CrossRef] [PubMed]
- Chen-Scarabelli, C.; Corsetti, G.; Pasini, E.; Dioguardi, F.S.; Sahni, G.; Narula, J.; Gavazzoni, M.; Patel, H.; Saravolatz, L.; Knight, R.; et al. Spasmogenic Effects of the Proteasome Inhibitor Carfilzomib on Coronary Resistance, Vascular Tone and Reactivity. EBioMedicine 2017, 21, 206–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.F.; Huang, C.C.; Xiao, Y.F.; Guan, X.H.; Wang, X.N.; Cao, Q.; Liu, Y.; Huang, X.; Deng, L.B.; Deng, K.Y.; et al. CD38 Deficiency Protects Heart from High Fat Diet-Induced Oxidative Stress via Activating Sirt3/FOXO3 Pathway. Cell. Physiol. Biochem. 2018, 48, 2350–2363. [Google Scholar] [CrossRef] [PubMed]
- van de Donk, N.W.; Janmaat, M.L.; Mutis, T.; Lammerts van Bueren, J.J.; Ahmadi, T.; Sasser, A.K.; Lokhorst, H.M.; Parren, P.W. Monoclonal antibodies targeting CD38 in hematological malignancies and beyond. Immunol. Rev. 2016, 270, 95–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chari, A.; Munder, M.; Weisel, K.; Jenner, M.; Bygrave, C.; Petrucci, M.T.; Boccadoro, M.; Cavo, M.; van de Donk, N.; Turgut, M.; et al. Evaluation of Cardiac Repolarization in the Randomized Phase 2 Study of Intermediate- or High-Risk Smoldering Multiple Myeloma Patients Treated with Daratumumab Monotherapy. Adv. Ther. 2021, 38, 1328–1341. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [Green Version]
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: Consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Sugimoto, T.; Dulgheru, R.; Bernard, A.; Ilardi, F.; Contu, L.; Addetia, K.; Caballero, L.; Akhaladze, N.; Athanassopoulos, G.D.; Barone, D.; et al. Echocardiographic reference ranges for normal left ventricular 2D strain: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 833–840. [Google Scholar] [CrossRef]
- Kuznetsova, T.; Herbots, L.; Richart, T.; D’Hooge, J.; Thijs, L.; Fagard, R.H.; Herregods, M.C.; Staessen, J.A. Left ventricular strain and strain rate in a general population. Eur. Heart J. 2008, 29, 2014–2023. [Google Scholar] [CrossRef] [Green Version]
- Vieira, M.J.; Teixeira, R.; Goncalves, L.; Gersh, B.J. Left atrial mechanics: Echocardiographic assessment and clinical implications. J. Am. Soc. Echocardiogr. 2014, 27, 463–478. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.A.; Krisper, M.; Nakatani, S.; Kohncke, C.; Otsuji, Y.; Belyavskiy, E.; Radha Krishnan, A.K.; Kropf, M.; Osmanoglou, E.; Boldt, L.H.; et al. Normal range and usefulness of right ventricular systolic strain to detect subtle right ventricular systolic abnormalities in patients with heart failure: A multicentre study. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 212–223. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Paiva, B.; Anderson, K.C.; Durie, B.; Landgren, O.; Moreau, P.; Munshi, N.; Lonial, S.; Blade, J.; Mateos, M.V.; et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016, 17, e328–e346. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, G.M.; Laird, N.M.; Ware, J.H. Applied Longitudinal Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2004. [Google Scholar]


{kind=link}
| Baseline Parameters | Kd (n = 11) | DaraKd (n = 14) | p Value |
|---|---|---|---|
| Age (years), mean ± SD | 69.45 ± 9 | 66.43 ± 6.3 | 0.34 |
| Male gender, [n (%)] | 7 (50) | 8 (72.7) | 0.26 |
| Prior lines of therapy (1 vs. 2) | 6 vs. 5 | 11 vs. 3 | 0.20 |
| Prior HDM/ASCT | 1 | 3 | 0.40 |
| Prior PI | 10 | 13 | 0.86 |
| Prior IMiD | 8 | 12 | 0.42 |
| BMI (kg/m2), mean ± SD | 28.91 ± 2.6 | 28.89 ± 3.8 | 0.98 |
| Hyperlipidemia, [n (%)] | 0 (0) | 3 (21.4) | 0.1 |
| Smoking, [n (%)] | 2 (18.2) | 2 (14.3) | 0.79 |
| Cardiovascular disease, [n (%)] | 4 (36.4) | 4 (28.6) | 0.68 |
| Hypertension, [n (%)] | 6 (54.5) | 6 (42.9) | 0.56 |
| Diabetes, [n (%)] | 2 (18.2) | 1 (7.1) | 0.4 |
| Kidney disease, [n (%)] | 1 (9.1) | 0 (0) | 0.25 |
| Systolic BP (mmHg), mean ± SD | 138.09 ± 13.4 | 126.7 ± 21.1 | 0.13 |
| Diastolic BP (mmHg), mean ± SD | 71.64 ± 9.2 | 68.64 ± 7.9 | 0.39 |
| Echocardiographic Parameters | |||
| LV diastolic diameter (mm), mean ± SD | 50.14 ± 5.8 | 46 ± 4.6 | 0.58 |
| LV mass (g), mean ± SD | 178.4 ±49.7 | 125.9 ± 30.3 | 0.003 |
| LVEF (%), mean ± SD | 59.64 ± 4.8 | 55.86 ± 5.7 | 0.094 |
| LV GLS (%), mean ± SD | −22.46 ± 2.9 | −18.48 ± 3 | 0.006 |
| LV strain rate s wave (s−1), mean ± SD | −1.16 ± 0.3 | −1.38 ± 0.2 | 0.071 |
| LV Radial strain (%), mean ± SD | 52.56 ± 22.7 | 46.51 ± 22 | 0.545 |
| Diastolic dysfunction, [n (%)] | 10 (90.9) | 10 (71.4) | 0.23 |
| E/Ea, mean ± SD | 11.18 ± 4.5 | 9.64 ± 3.6 | 0.35 |
| LA diameter (mm), mean ± SD | 43.6 ± 7.6 | 34.7 ± 4.6 | 0.037 |
| LAVi (mL/m2), mean ± SD | 40.95 ± 9.1 | 31.45 ± 9.7 | 0.032 |
| PALS (%), mean ± SD | 28.72 ± 5.1 | 34.34 ± 5.4 | 0.029 |
| LA strain rate s wave (s−1), mean ± SD | 1.39 ± 0.18 | 1.92 ± 1.1 | 0.66 |
| RVSTDI (cm/s), mean ± SD | 13.91 ± 2.6 | 13.31 ± 2.4 | 0.56 |
| TAPSE (mm), mean ± SD | 24.18 ± 3.7 | 21 ± 4.2 | 0.1 |
| RV GLS (%), mean ± SD | −21.97 ± 4.3 | −20.21 ± 5.2 | 0.42 |
| RV free wall LS (%), mean ± SD | −31.89 ± 3.4 | −24.39 ± 4.3 | <0.001 |
| Treatment | Echocardiographic Parameter | Baseline Values (Mean ± SD) | Follow-Up Values (Mean ± SD) | p Value | p for GroupInteraction |
|---|---|---|---|---|---|
| LV function | |||||
| Kd | LVEF (%) | 59.64 ± 4.8 | 56.64 ± 5.4 | 0.026 | 0.033 |
| DaraKd | 55.86 ± 5.7 | 56.65 ± 4.4 | 0.539 | ||
| Kd | LV diastolic diameter (mm) | 50.14 ± 5.8 | 50.23 ± 6.3 | 0.898 | 0.179 |
| DaraKd | 46 ± 4.6 | 47.85 ± 3.8 | 0.047 | ||
| Kd | LV GLS (%) | −22.46 ± 2.9 | −19.42 ± 2.1 | 0.007 | 0.003 |
| DaraKd | −18.48 ± 3 | −19.25 ± 3.1 | 0.309 | ||
| Kd | LV strain rate s wave (s−1) | −1.16 ± 0.3 | −1.09 ± 0.2 | 0.383 | 0.111 |
| DaraKd | −1.38 ± 0.2 | −1.13 ± 0.1 | 0.005 | ||
| Kd | LV radial strain (%) | 52.56 ± 22.7 | 49.56 ± 26.2 | 0.589 | 0.818 |
| DaraKd | 46.51 ± 22 | 41.39 ± 12.4 | 0.463 | ||
| Kd | LAVi (mL/m2) | 40.95 ± 9.1 | 45.84 ± 8.8 | 0.002 | 0.182 |
| DaraKd | 31.45 ± 9.7 | 34.47 ± 10.8 | 0.003 | ||
| Kd | E/Ea | 11.18 ± 4.5 | 11.73 ± 6 | 0.512 | 0.919 |
| DaraKd | 9.64 ± 3.6 | 10 ± 3 | 0.547 | ||
| Kd | PALS (%) | 28.72 ± 5.1 | 24.22 ± 5.6 | 0.030 | 0.808 |
| DaraKd | 34.34 ± 5.4 | 29.14 ± 6.7 | 0.022 | ||
| Kd | LA strain rate s wave (s−1) | 1.39 ± 0.18 | 1.14 ± 0.2 | 0.053 | 0.540 |
| DaraKd | 1.92 ± 1.1 | 1.27 ± 0.6 | 0.102 | ||
| RV function | |||||
| Kd | TAPSE (mm) | 24.18 ± 3.7 | 20.36 ± 2.7 | 0.008 | 0.008 |
| DaraKd | 21 ± 4.2 | 22.23 ± 3.7 | 0.438 | ||
| Kd | RVSTDI (cm/s) | 13.91 ± 2.6 | 14 ± 2.3 | 0.911 | 0.347 |
| DaraKd | 13.31 ± 2.4 | 12.54 ± 1.8 | 0.137 | ||
| Kd | RV LS | −21.97 ± 4.3 | −21.4 ± 4.6 | 0.547 | 0.583 |
| DaraKd | −20.21 ± 5.2 | −20.95 ± 2.6 | 0.705 | ||
| Kd | RV free wall LS (%) | −31.89 ± 3.4 | −22.23 ± 4.3 | 0.012 | 0.049 |
| DaraKd | −24.39 ± 4.3 | −25.75 ± 4.5 | 0.485 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terpos, E.; Stamatelopoulos, K.; Makris, N.; Georgiopoulos, G.; Ntanasis-Stathopoulos, I.; Gavriatopoulou, M.; Laina, A.; Eleutherakis-Papaiakovou, E.; Fotiou, D.; Kanellias, N.; et al. Daratumumab May Attenuate Cardiac Dysfunction Related to Carfilzomib in Patients with Relapsed/Refractory Multiple Myeloma: A Prospective Study. Cancers 2021, 13, 5057. https://doi.org/10.3390/cancers13205057
Terpos E, Stamatelopoulos K, Makris N, Georgiopoulos G, Ntanasis-Stathopoulos I, Gavriatopoulou M, Laina A, Eleutherakis-Papaiakovou E, Fotiou D, Kanellias N, et al. Daratumumab May Attenuate Cardiac Dysfunction Related to Carfilzomib in Patients with Relapsed/Refractory Multiple Myeloma: A Prospective Study. Cancers. 2021; 13(20):5057. https://doi.org/10.3390/cancers13205057
Chicago/Turabian StyleTerpos, Evangelos, Kimon Stamatelopoulos, Nikolaos Makris, Georgios Georgiopoulos, Ioannis Ntanasis-Stathopoulos, Maria Gavriatopoulou, Ageliki Laina, Evangelos Eleutherakis-Papaiakovou, Despina Fotiou, Nikolaos Kanellias, and et al. 2021. "Daratumumab May Attenuate Cardiac Dysfunction Related to Carfilzomib in Patients with Relapsed/Refractory Multiple Myeloma: A Prospective Study" Cancers 13, no. 20: 5057. https://doi.org/10.3390/cancers13205057