
Risk of Thrombo-Embolic Events in Ovarian Cancer: Does Bevacizumab Tilt the Scale? A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Selection
2.2. Data Extraction
2.3. Study Objectives and Statistical Analysis
2.4. Protocol Registration
3. Results
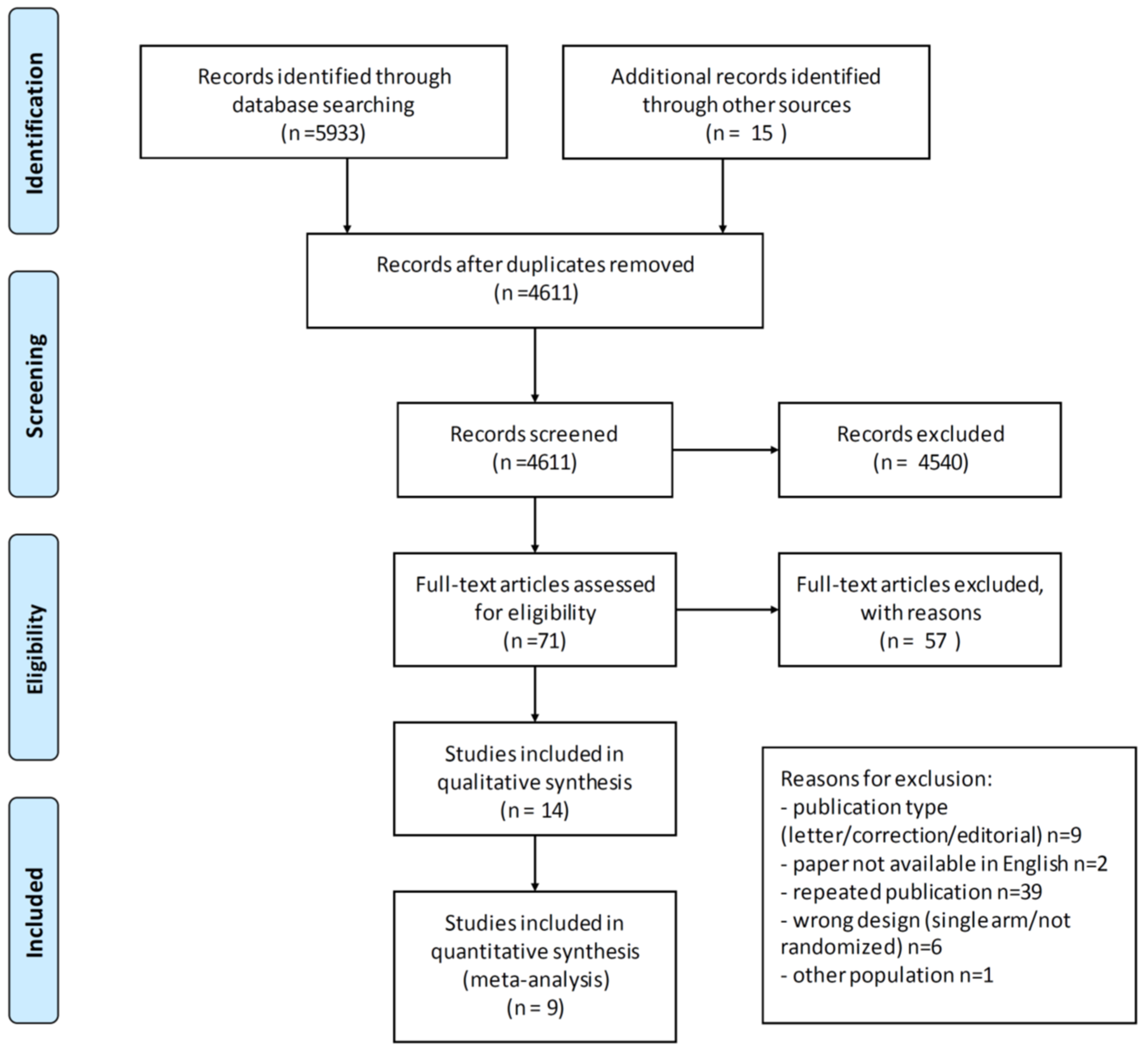
3.1. Study Selection and Characteristics
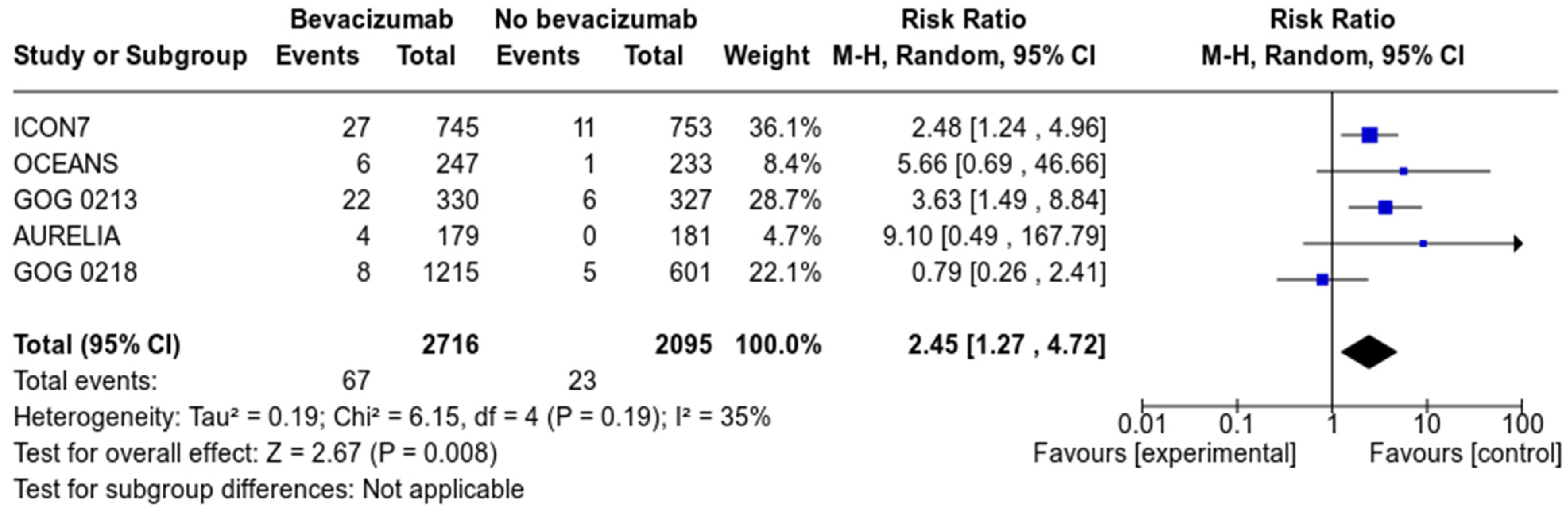
3.2. Arterial Thromboembolic Events
3.3. Venous Thromboembolic Events
3.4. Risk of Bias
4. Discussion
Implications for Clinical Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sorensen, H.T.; Mellemkjaer, L.; Steffensen, F.H.; Olsen, J.H.; Nielsen, G.L. Incidence of cancer after primary deep venous thrombosis or pulmonary embolism. Lakartidningen 2000, 97, 1961–1964. [Google Scholar]
- Chew, H.K.; Wun, T.; Harvey, D.; Zhou, H.; White, R.H. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch. Intern. Med. 2006, 166, 458–464. [Google Scholar] [CrossRef]
- Noble, S.; Pasi, J. Epidemiology and pathophysiology of cancer-associated thrombosis. Br. J. Cancer 2010, 102 (Suppl. 1), S2–S9. [Google Scholar] [CrossRef]
- Prandoni, P.; Falanga, A.; Piccioli, A. Cancer and venous thromboembolism. Lancet. Oncol. 2005, 6, 401–410. [Google Scholar] [CrossRef]
- Elting, L.S.; Escalante, C.P.; Cooksley, C.; Avritscher, E.B.; Kurtin, D.; Hamblin, L.; Khosla, S.G.; Rivera, E. Outcomes and cost of deep venous thrombosis among patients with cancer. Arch. Intern. Med. 2004, 164, 1653–1661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahr, H.S.; Christiansen, O.B.; Grove, A.; Iyer, V.; Torp-Pedersen, C.; Knudsen, A.; Thorlacius-Ussing, O. Venous thromboembolism in epithelial ovarian cancer. A prospective cohort study. Thromb. Res. 2019, 181, 112–119. [Google Scholar] [CrossRef]
- Greco, P.S.; Bazzi, A.A.; McLean, K.; Reynolds, R.K.; Spencer, R.J.; Johnston, C.M.; Liu, J.R.; Uppal, S. Incidence and Timing of Thromboembolic Events in Patients With Ovarian Cancer Undergoing Neoadjuvant Chemotherapy. Obstet. Gynecol. 2017, 129, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Donnellan, E.; Khorana, A.A. Cancer and Venous Thromboembolic Disease: A Review. Oncology 2017, 22, 199–207. [Google Scholar] [CrossRef] [Green Version]
- Abdol Razak, N.B.; Jones, G.; Bhandari, M.; Berndt, M.C.; Metharom, P. Cancer-Associated Thrombosis: An Overview of Mechanisms, Risk Factors, and Treatment. Cancers 2018, 10, 380. [Google Scholar] [CrossRef] [Green Version]
- Leighl, N.B.; Zatloukal, P.; Mezger, J.; Ramlau, R.; Moore, N.; Reck, M.; Manegold, C. Efficacy and safety of bevacizumab-based therapy in elderly patients with advanced or recurrent nonsquamous non-small cell lung cancer in the phase III BO17704 study (AVAiL). J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2010, 5, 1970–1976. [Google Scholar] [CrossRef]
- Hochster, H.S.; Hart, L.L.; Ramanathan, R.K.; Childs, B.H.; Hainsworth, J.D.; Cohn, A.L.; Wong, L.; Fehrenbacher, L.; Abubakr, Y.; Saif, M.W.; et al. Safety and efficacy of oxaliplatin and fluoropyrimidine regimens with or without bevacizumab as first-line treatment of metastatic colorectal cancer: Results of the TREE Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 3523–3529. [Google Scholar] [CrossRef] [PubMed]
- Saltz, L.B.; Clarke, S.; Diaz-Rubio, E.; Scheithauer, W.; Figer, A.; Wong, R.; Koski, S.; Lichinitser, M.; Yang, T.S.; Rivera, F.; et al. Bevacizumab in combination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: A randomized phase III study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 2013–2019. [Google Scholar] [CrossRef] [Green Version]
- Diaz, R.J.; Ali, S.; Qadir, M.G.; De La Fuente, M.I.; Ivan, M.E.; Komotar, R.J. The role of bevacizumab in the treatment of glioblastoma. J. Neuro-Oncol. 2017, 133, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Powles, T.; Atkins, M.B.; Escudier, B.; McDermott, D.F.; Suarez, C.; Bracarda, S.; Stadler, W.M.; Donskov, F.; Lee, J.L.; et al. Atezolizumab plus bevacizumab versus sunitinib in patients with previously untreated metastatic renal cell carcinoma (IMmotion151): A multicentre, open-label, phase 3, randomised controlled trial. Lancet 2019, 393, 2404–2415. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Tewari, K.S.; Burger, R.A.; Enserro, D.; Norquist, B.M.; Swisher, E.M.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Huang, H.; Homesley, H.D.; et al. Final overall survival of a randomized trial of bevacizumab for primary treatment of ovarian cancer. J. Clin. Oncol. 2019, 37, 2317–2328. [Google Scholar] [CrossRef]
- Perren, T.J.; Swart, A.M.; Pfisterer, J.; Ledermann, J.A.; Pujade Lauraine, E.; Kristensen, G. A phase 3 trial of bevacizumab in ovarian cancer. N. Engl. J. Med. 2011, 365, 2484–2496. [Google Scholar] [CrossRef] [Green Version]
- Perren, T.; Swart, A.M.; Pfisterer, J.; Ledermann, J.; Lortholary, A.; Kristensen, G.; Carey, M.; Beale, P.; Cervantes, A.; Oza, A. Icon7: A phase III randomised gynaecologic cancer intergroup trial of concurrent bevacizumab and chemotherapy followed by maintenance bevacizumab, versus chemotherapy alone in women with newly diagnosed epithelial ovarian (EOC), primary peritoneal (PPC) or fallopian tube cancer (FTC). Ann. Oncol. 2010, 21, viii2–viii3. [Google Scholar]
- Oza, A.M.; Cook, A.D.; Pfisterer, J.; Embleton, A.; Ledermann, J.A.; Pujade-Lauraine, E.; Kristensen, G.; Carey, M.S.; Beale, P.; Cervantes, A.; et al. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): Overall survival results of a phase 3 randomised trial. Lancet Oncol. 2015, 16, 928–936. [Google Scholar] [CrossRef]
- Aghajanian, C.; Goff, B.; Nycum, L.R.; Wang, Y.V.; Husain, A.; Blank, S.V. Final overall survival and safety analysis of OCEANS, a phase 3 trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent ovarian cancer. Gynecol. Oncol. 2015, 139, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Coleman, R.L.; Brady, M.F.; Herzog, T.J.; Sabbatini, P.; Armstrong, D.K.; Walker, J.L.; Kim, B.G.; Fujiwara, K.; Tewari, K.S.; O’Malley, D.M.; et al. Bevacizumab and paclitaxel-carboplatin chemotherapy and secondary cytoreduction in recurrent, platinum-sensitive ovarian cancer (NRG Oncology/Gynecologic Oncology Group study GOG-0213): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2017, 18, 779–791. [Google Scholar] [CrossRef] [Green Version]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: The AURELIA open-label randomized phase III trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Burger, R.A.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Monk, B.J.; Huang, H. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N. Engl. J. Med. 2011, 365, 2473–2483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, R.L.; Sood, A.K.; Coleman, R.L. Collateral damage: Toxic effects of targeted antiangiogenic therapies in ovarian cancer. Lancet Oncol. 2010, 11, 465–475. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, H.; Yabuno, A.; Fujiwara, K. Critical appraisal of bevacizumab in the treatment of ovarian cancer. Drug Des. Dev. Ther. 2015, 9, 2351–2358. [Google Scholar] [CrossRef] [Green Version]
- Touyz, R.M.; Herrmann, S.M.S.; Herrmann, J. Vascular toxicities with VEGF inhibitor therapies-focus on hypertension and arterial thrombotic events. J. Am. Soc. Hypertens. 2018, 12, 409–425. [Google Scholar] [CrossRef]
- Chen, N.; Ren, M.; Li, R.; Deng, X.; Li, Y.; Yan, K.; Xiao, L.; Yang, Y.; Wang, L.; Luo, M.; et al. Bevacizumab promotes venous thromboembolism through the induction of PAI-1 in a mouse xenograft model of human lung carcinoma. Mol. Cancer 2015, 14, 140. [Google Scholar] [CrossRef] [Green Version]
- Kapelakis, I.; Toutouzas, K.; Drakopoulou, M.; Michelongona, A.; Zagouri, F.; Mpamias, A.; Pliatsika, P.; Dimopoulos, M.A.; Stefanadis, C.; Tousoulis, D. Bevacizumab increases the incidence of cardiovascular events in patients with metastatic breast or colorectal cancer. Hell. J. Cardiol. HJC 2017, 58, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, C.; Chisaki, Y.; Sakimoto, S.; Sakae, H.; Yano, Y. Evaluation of thromboembolic events in cancer patients receiving bevacizumab according to the Japanese Adverse Drug Event Report database. J. Oncol. Pharm. Pract. Off. Publ. Int. Soc. Oncol. Pharm. Pract. 2018, 24, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Kuk, A.; Magnowska, M.; Suchy, W.; Swierczynska, J.; Zaborowski, M.P.; Gaca, M.; Nowak-Markwitz, E. Retrospective Evaluation of Thromboembolism Risk in Ovarian Cancer Patients Treated with Bevacizumab. Target. Oncol. 2017, 12, 495–503. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joly, F.; Cottu, P.H.; Gouy, S.; Lambaudie, E.; Selle, F.; Leblanc, E.; Floquet, A.; Pomel, C.; Chereau, E.; Zohar, S.; et al. Efficacy and long-term safety with bevacizumab included in neoadjuvant and adjuvant therapies in patients with advanced ovarian cancer: Results of the ANTHALYA trial. J. Clin. Oncol. 2017, 35, 5538. [Google Scholar] [CrossRef]
- Garcia Garcia, Y.; de Juan Ferre, A.; Mendiola, C.; Barretina-Ginesta, M.P.; Gaba Garcia, L.; Santaballa Bertran, A.; Bover Barcelo, I.; Gil-Martin, M.; Manzano, A.; Rubio Perez, M.J.; et al. Efficacy and safety results from GEICO 1205, a randomized phase II trial of neoadjuvant chemotherapy with or without bevacizumab for advanced epithelial ovarian cancer. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2019, 29, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Gore, M.; Hackshaw, A.; Brady, W.E.; Penson, R.T.; Zaino, R.; McCluggage, W.G.; Ganesan, R.; Wilkinson, N.; Perren, T.; Montes, A.; et al. An international, phase III randomized trial in patients with mucinous epithelial ovarian cancer (mEOC/GOG 0241) with long-term follow-up: And experience of conducting a clinical trial in a rare gynecological tumor. Gynecol. Oncol. 2019, 153, 541–548. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Chen, C.; Wang, S.; Li, X.; Fan, T. Efficacy of bevacizumab combined with nedaplatin in the treatment of ovarian cancer and its effects on tumor markers and immunity of patients. JBU 2020, 25, 80–86. [Google Scholar]
- Pignata, S.; Lorusso, D.; Joly, F.; Gallo, C.; Colombo, N.; Sessa, C.; Bamias, A.; Salutari, V.; Selle, F.; Frezzini, S.; et al. Carboplatin-based doublet plus bevacizumab beyond progression versus carboplatin-based doublet alone in patients with platinum-sensitive ovarian cancer: A randomised, phase 3 trial. Lancet Oncol. 2021, 22, 267–276. [Google Scholar] [CrossRef]
- Mirza, M.R.; Åvall Lundqvist, E.; Birrer, M.J.; de Pont Christensen, R.; Nyvang, G.B.; Malander, S.; Anttila, M.; Werner, T.L.; Lund, B.; Lindahl, G.; et al. Niraparib plus bevacizumab versus niraparib alone for platinum-sensitive recurrent ovarian cancer (NSGO-AVANOVA2/ENGOT-ov24): A randomised, phase 2, superiority trial. Lancet Oncol. 2019, 20, 1409–1419. [Google Scholar] [CrossRef]
- Cong, J.; Liu, R.; Hou, J.; Wang, X.; Jiang, H.; Wang, J. Therapeutic effect of bevacizumab combined with paclitaxel and carboplatin on recurrent ovarian cancer. JBU 2019, 24, 1003–1008. [Google Scholar]
- Zhang, Y.M.; Xu, S.J.; Huo, D.M. Clinical efficacy and mechanism of bevacizumab combined with conventional chemotherapy in the treatment of recurrent ovarian cancer. Acta Med. Mediterr. 2019, 35, 2635–2640. [Google Scholar]
- Liu, B.; An, R.; Yu, J. Efficacy of bevacizumab combined with albumin-bound paclitaxel in the treatment of platinum-resistant recurrent ovarian cancer. JBU 2019, 24, 2303–2309. [Google Scholar]
- Pant, A.; Liu, D.; Schink, J.; Lurain, J. Venous thromboembolism in advanced ovarian cancer patients undergoing frontline adjuvant chemotherapy. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2014, 24, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Bertelli, G.; Li, L.; Green, C.; Chan, S.; Yeoh, C.C.; Hasan, J.; Jones, R.; Ograbek, A.; Perren, T.J. Role of front-line bevacizumab in advanced ovarian cancer: The OSCAR study. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2020, 30, 213–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scappaticci, F.A.; Skillings, J.R.; Holden, S.N.; Gerber, H.P.; Miller, K.; Kabbinavar, F.; Bergsland, E.; Ngai, J.; Holmgren, E.; Wang, J.; et al. Arterial thromboembolic events in patients with metastatic carcinoma treated with chemotherapy and bevacizumab. J. Natl. Cancer Inst. 2007, 99, 1232–1239. [Google Scholar] [CrossRef] [Green Version]
- Nalluri, S.R.; Chu, D.; Keresztes, R.; Zhu, X.; Wu, S. Risk of venous thromboembolism with the angiogenesis inhibitor bevacizumab in cancer patients: A meta-analysis. JAMA 2008, 300, 2277–2285. [Google Scholar] [CrossRef] [PubMed]
- Minor, D.R. Risk of venous thromboembolism with bevacizumab in cancer patients. JAMA 2009, 301, 1434, discussion 1435–1436. [Google Scholar] [CrossRef] [PubMed]
- Kilickap, S.; Arslan, C. Risk of venous thromboembolism with bevacizumab in cancer patients. JAMA 2009, 301, 1435, discussion 1435–1436. [Google Scholar] [CrossRef]
- Cortes, J.; Saura, C.; Atzori, F. Risk of venous thromboembolism with bevacizumab in cancer patients. JAMA 2009, 301, 1434–1435, discussion 1435–1436. [Google Scholar] [CrossRef]
- Ranpura, V.; Hapani, S.; Chuang, J.; Wu, S. Risk of cardiac ischemia and arterial thromboembolic events with the angiogenesis inhibitor bevacizumab in cancer patients: A meta-analysis of randomized controlled trials. Acta Oncol. 2010, 49, 287–297. [Google Scholar] [CrossRef]
- Azzi, G.R.; Schutz, F.A.; Je, Y.; Choueiri, T.K. Bevacizumab (BEV) and the risk of arterial thromboembolic evets (ATE) in patients with renal cell carcinoma and other cancers: A large comprehensive meta-analysis of more than 13,000 patients. J. Clin. Oncol. 2010, 28. [Google Scholar] [CrossRef]
- Cortes, J.; Calvo, V.; Ramirez-Merino, N.; O’Shaughnessy, J.; Brufsky, A.; Robert, N.; Vidal, M.; Munoz, E.; Perez, J.; Dawood, S.; et al. Adverse events risk associated with bevacizumab addition to breast cancer chemotherapy: A meta-analysis. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2012, 23, 1130–1137. [Google Scholar] [CrossRef]
- Totzeck, M.; Mincu, R.I.; Rassaf, T. Cardiovascular Adverse Events in Patients With Cancer Treated With Bevacizumab: A Meta-Analysis of More Than 20,000 Patients. J. Am. Heart Assoc. 2017, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.J.; Chen, D.F.; Wu, G.F.; Guan, W.J.; Zhu, Z.; Liu, Y.Q.; Gao, G.Y.; Qin, Y.Y.; Zhong, N.S. Incidence and risk of thromboembolism associated with bevacizumab in patients with non-small cell lung carcinoma. J. Thorac. Dis. 2018, 10, 5010–5022. [Google Scholar] [CrossRef] [PubMed]
- Hurwitz, H.I.; Saltz, L.B.; Van Cutsem, E.; Cassidy, J.; Wiedemann, J.; Sirzen, F.; Lyman, G.H.; Rohr, U.P. Venous thromboembolic events with chemotherapy plus bevacizumab: A pooled analysis of patients in randomized phase II and III studies. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 1757–1764. [Google Scholar] [CrossRef]
- Zhou, M.; Yu, P.; Qu, X.; Liu, Y.; Zhang, J. Phase III trials of standard chemotherapy with or without bevacizumab for ovarian cancer: A meta-analysis. PLoS ONE 2013, 8, e81858. [Google Scholar] [CrossRef]
- Li, J.; Zhou, L.; Chen, X.; Ba, Y. Addition of bevacizumab to chemotherapy in patients with ovarian cancer: A systematic review and meta-analysis of randomized trials. Clin. Transl. Oncol. Off. Publ. Fed. Span. Oncol. Soc. Natl. Cancer Inst. Mex. 2015, 17, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.; Zeng, L.; Kuang, Y.; Cao, Z.; Zheng, C.; Zhang, Y.; Liao, M.; Yang, L. Antiangiogenic drugs used with chemotherapy for patients with recurrent ovarian cancer: A meta-analysis. OncoTargets Ther. 2017, 10, 973–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Xu, T.; Zheng, L.; Li, G. Angiogenesis Inhibitors for the Treatment of Ovarian Cancer: An Updated Systematic Review and Meta-analysis of Randomized Controlled Trials. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2018, 28, 903–914. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.S.; Shui, L.; Shen, D.; Chen, X. Bevacizumab combined with chemotherapy for ovarian cancer: An updated systematic review and meta-analysis of randomized controlled trials. Oncotarget 2017, 8, 10703–10713. [Google Scholar] [CrossRef]
- Wang, T.S.; Lei, W.; Cui, W.; Wen, P.; Guo, H.F.; Ding, S.G.; Yang, Y.P.; Xu, Y.Q.; Lv, S.W.; Zhu, Y.L. A meta-analysis of bevacizumab combined with chemotherapy in the treatment of ovarian cancer. Indian J. Cancer 2014, 51 (Suppl. 3), e95–e98. [Google Scholar] [CrossRef]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood 2008, 111, 4902–4907. [Google Scholar] [CrossRef] [Green Version]
- Ay, C.; Dunkler, D.; Marosi, C.; Chiriac, A.L.; Vormittag, R.; Simanek, R.; Quehenberger, P.; Zielinski, C.; Pabinger, I. Prediction of venous thromboembolism in cancer patients. Blood 2010, 116, 5377–5382. [Google Scholar] [CrossRef]
- Verso, M.; Agnelli, G.; Barni, S.; Gasparini, G.; LaBianca, R. A modified Khorana risk assessment score for venous thromboembolism in cancer patients receiving chemotherapy: The Protecht score. Intern. Emerg. Med. 2012, 7, 291–292. [Google Scholar] [CrossRef] [PubMed]
- Pelzer, U.; Sinn, M.; Stieler, J.; Riess, H. Primary pharmacological prevention of thromboembolic events in ambulatory patients with advanced pancreatic cancer treated with chemotherapy? Dtsch. Med. Wochenschr. 2013, 138, 2084–2088. [Google Scholar] [CrossRef]
- Gerotziafas, G.T.; Taher, A.; Abdel-Razeq, H.; AboElnazar, E.; Spyropoulos, A.C.; El Shemmari, S.; Larsen, A.K.; Elalamy, I.; Group, C.-C.W. A Predictive Score for Thrombosis Associated with Breast, Colorectal, Lung, or Ovarian Cancer: The Prospective COMPASS-Cancer-Associated Thrombosis Study. Oncology 2017, 22, 1222–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khorana, A.A.; Cohen, A.T.; Carrier, M.; Meyer, G.; Pabinger, I.; Kavan, P.; Wells, P. Prevention of venous thromboembolism in ambulatory patients with cancer. ESMO Open 2020, 5, e000948. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; George, D.J.; Kakkar, A.K.; Fisher, W.; Lassen, M.R.; Mismetti, P.; Mouret, P.; Chaudhari, U.; Lawson, F.; Turpie, A.G.; et al. Semuloparin for thromboprophylaxis in patients receiving chemotherapy for cancer. N. Engl. J. Med. 2012, 366, 601–609. [Google Scholar] [CrossRef] [Green Version]
- Agnelli, G.; Gussoni, G.; Bianchini, C.; Verso, M.; Mandala, M.; Cavanna, L.; Barni, S.; Labianca, R.; Buzzi, F.; Scambia, G.; et al. Nadroparin for the prevention of thromboembolic events in ambulatory patients with metastatic or locally advanced solid cancer receiving chemotherapy: A randomised, placebo-controlled, double-blind study. Lancet. Oncol. 2009, 10, 943–949. [Google Scholar] [CrossRef]
- Khorana, A.A.; Francis, C.W.; Kuderer, N.M.; Carrier, M.; Ortel, T.L.; Wun, T.; Rubens, D.; Hobbs, S.; Iyer, R.; Peterson, D.; et al. Dalteparin thromboprophylaxis in cancer patients at high risk for venous thromboembolism: A randomized trial. Thromb. Res. 2017, 151, 89–95. [Google Scholar] [CrossRef]
- Carrier, M.; Abou-Nassar, K.; Mallick, R.; Tagalakis, V.; Shivakumar, S.; Schattner, A.; Kuruvilla, P.; Hill, D.; Spadafora, S.; Marquis, K.; et al. Apixaban to Prevent Venous Thromboembolism in Patients with Cancer. N. Engl. J. Med. 2019, 380, 711–719. [Google Scholar] [CrossRef]
- Khorana, A.A.; McNamara, M.G.; Kakkar, A.K.; Streiff, M.B.; Riess, H.; Vijapurkar, U.; Kaul, S.; Wildgoose, P.; Soff, G.A.; Investigators, C. Assessing Full Benefit of Rivaroxaban Prophylaxis in High-Risk Ambulatory Patients with Cancer: Thromboembolic Events in the Randomized CASSINI Trial. TH Open Companion J. Thromb. Haemost. 2020, 4, e107–e112. [Google Scholar] [CrossRef]
- Li, A.; Garcia, D.A.; Lyman, G.H.; Carrier, M. Direct oral anticoagulant (DOAC) versus low-molecular-weight heparin (LMWH) for treatment of cancer associated thrombosis (CAT): A systematic review and meta-analysis. Thromb. Res. 2019, 173, 158–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandala, M.; Falanga, A.; Roila, F.; Group, E.G.W. Management of venous thromboembolism (VTE) in cancer patients: ESMO Clinical Practice Guidelines. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2011, 22 (Suppl. 6), vi85–vi92. [Google Scholar] [CrossRef]
- Farge, D.; Frere, C.; Connors, J.M.; Ay, C.; Khorana, A.A.; Munoz, A.; Brenner, B.; Kakkar, A.; Rafii, H.; Solymoss, S.; et al. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet. Oncol. 2019, 20, e566–e581. [Google Scholar] [CrossRef] [Green Version]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.R.; Francis, C.W.; et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 496–520. [Google Scholar] [CrossRef]
- Wang, T.F.; Zwicker, J.I.; Ay, C.; Pabinger, I.; Falanga, A.; Antic, D.; Noble, S.; Khorana, A.A.; Carrier, M.; Meyer, G. The use of direct oral anticoagulants for primary thromboprophylaxis in ambulatory cancer patients: Guidance from the SSC of the ISTH. J. Thromb. Haemost. JTH 2019, 17, 1772–1778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, A.; Kuderer, N.M.; Garcia, D.A.; Khorana, A.A.; Wells, P.S.; Carrier, M.; Lyman, G.H. Direct oral anticoagulant for the prevention of thrombosis in ambulatory patients with cancer: A systematic review and meta-analysis. J. Thromb. Haemost. JTH 2019, 17, 2141–2151. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Carlson, J.J.; Kuderer, N.M.; Schaefer, J.K.; Li, S.; Garcia, D.A.; Khorana, A.A.; Carrier, M.; Lyman, G.H. Cost-effectiveness analysis of low-dose direct oral anticoagulant (DOAC) for the prevention of cancer-associated thrombosis in the United States. Cancer 2020, 126, 1736–1748. [Google Scholar] [CrossRef]
- Weeks, K.S.; Herbach, E.; McDonald, M.; Charlton, M.; Schweizer, M.L. Meta-Analysis of VTE Risk: Ovarian Cancer Patients by Stage, Histology, Cytoreduction, and Ascites at Diagnosis. Obstet. Gynecol. Int. 2020, 2020, 2374716. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Name Author, Year [Ref] | Study Population, Number | Regimen | mPFS (Months) p Value | mOS (Months) p Value | VTE n/N (%) | ATE n/N (%) |
|---|---|---|---|---|---|---|
| GOG-0218 Tewari, 2018 [16] | Frontline stage III (incomplete resection) and stage IV (all) N = 1873 | A: C + P + pbo x6 B: C + P + bev x6 C: C + P + bev x6 → bev x16 | A: 10.3 m B: 11.3 m C: 14.1 m | A: 41.1 m B: 40.8 m C: 43.3 m | A: 35/601 (5.8%) B: 36/607 (5.9%) C: 42/608 (6.9%) | A: 5/601 (0.7%) B: 4/607 (0.7%) C: 4/608 (0.7%) |
| ICON-7 Perren, 2011 [17] | Frontline stage I-IIa (high risk) OR stage IIb-IV N = 1498 | A: C + P + pbo x6 → pbo x10 B: C + P + bev1 x6 → bev1 x10 | A: 17.5 m B: 19.9 m | A: 58.6 m B: 58.0 m | A: 31/753 (4.1%) B: 50/745 (6.7%) | A: 11/753 (1.4%) B: 27/745 (3.6%) |
| ANTHALYA Joly, 2017 [33] | Frontline stage IIIc-IV neoadjuvant N = 99 | A: C + P x4 → IDS → C + P + bev x1 → bev x16 B:(C + P) x4 + bev x3 →IDS →(C + P) x2 + bev x1 → bev x16 | A: 21.2 m [14.5–26.7] B: 23.5 m [18.5–30.6] | NA | A: 2/37 (5%) B: 6/58 (11%) | NA |
| GEICO-1205 Garcia-Garcia, 2019 [34] | Frontline FIGO IIIc-IV OC neoadjuvant N = 68 | A: C + P x4 → IDS →C + P + bev x3 → bev x15 B: C + P + bev x4 → IDS → C + P + bev x3 → bev x15 | A: 20.1 m B: 20.4 m | NA | A: 0/33 (0%) * B: 2/35 (5.7%) * | NA |
| mEOC/GOG0421 Gore, 2019 [35] | Frontline mucinous stage II-IV or relapsed stage I N = 50 | A: C + P x6 vs. B: Ox + Cap x6 vs. C: C + P + Bev x6 → bev x12 vs. D: Ox + Cap + Bev x6 → bev x12 | A&B: 8.1 m C&D: 18.1 m | A&B: 32.7 m C&D: 27.7 m | A&B: 0/26 (0%) * C&D:1/24 (4.1%) * | NA |
| Zhang, 2020 [36] | Frontline stage I-III N = 100 | A: C B: Npl85 + bev1 | A: NA B: NA | A: NA B: NA | A: NA B: NA | A: NA B: NA |
| OCEANS Aghajanian, 2015 [20] | Relapsed platinum-sensitive N = 484 | A: C + G + pbo x6 B: C + G + bev x6 → bev maintenance | A: 8.4 m B: 12.4 m | A: 32.9 m B: 33.6 m | A: 6/233 (2.6%) * B:11/247 (4.5%) * | A: 1/233 (0.4%) B: 6/247 (2.4%) |
| GOG-0213 Coleman, 2017 [21] | Relapsed platinum-sensitive N = 674 | A: C + P B: C + P + bev x6 → bev maintenance *** | A: 10.4 m B: 13.8 m | A: 37.3 m B: 42.2 m | A: 0/327 (0%) B: 0/330 (0%) | A: 6/327 (1.8%) B: 22/330 (6.6%) |
| MITO16B-MaNGO OV2B-ENGOT OV17 Pignata, 2021 [37] | Relapsed platinum sensitive, prior bevacizumab N = 406 | A: C + P or C + G or C + PLD B: C + P or C + G or C + PLD + bev2 | A: 8.8 m B: 11.8 m | A: 27.1 m B: 26.7 m | NA ** | NA ** |
| NSGO-AVANOVA2/ ENGOT-OV24 Mirza, 2019 [38] | Relapsed platinum sensitive N = 97 | A: niraparib B: niraparib + bev | A: 5.5 m B: 11.9 m | NA | A: 1/48 (2.2%) B: 2/49 (4.2%) | NA |
| Cong, 2019 [39] | Relapsed platinum sensitive N = 164 | A: C + P B: C + P + bev2 | A: 6.7 m B: 9.3 m | A: 12.5 m B: 18.5 m | NA | NA |
| AURELIA Pujade-Lauraine, 2014 [22] | Relapsed platinum resistant N = 360 | A: wP or Tp or PLD B: wP or Tp or PLD + bev | A: 3.4 m B: 6.7 m | A: 13.3 m B: 16.6 m | A: 8/181 (4.4%) * B: 5/179 (2.8%) * | A: 0/181 (0%) B: 4/179 (2.2%) |
| Liu, 2019 [41] | Relapsed platinum resistant N = 86 | A: ABP B: ABP + bev1 | A: 6.7 m B: 8.9 m | A: 12.7 m B: 16.3 m | NA | NA |
| Zhang, 2019 [40] | Relapsed platinum sensitive N = 160 | A: DTx + Npl80 B: DTx + Npl80 + bev1 | A: 8.6 m B: 12.2 m | A: 17.7 m B: 22.5 m | NA | NA |
| Study Name Author, Year [Ref] | Domain 1 Randomization Bias | Domain 2 Intervention Bias | Domain 3 Bias in Missing Outcome Data | Domain 4 Bias in Measurement of Outcome | Domain 5 Bias in Selection of the Reported Result | Overall Bias |
|---|---|---|---|---|---|---|
| GOG-0218 Tewari, 2018 [16] | Low risk | Low risk | Low risk | low risk | Low risk | Low risk |
| ICON-7 Perren, 2011 [17] | Low risk | Low risk | Low risk | low risk | Low risk | Low risk |
| ANTHALYA Joly, 2017 [33] | Some concerns | Some concerns | Low risk | Some concerns | Low risk | Some concerns |
| GEICO-1205 Garcia-Garcia, 2019 [34] | Some concerns | Some concerns | Low risk | Some concerns | Low risk | Some concerns |
| mEOC/GOG0421 Gore, 2019 [35] | Some concerns | Low risk | Low risk | low risk | Low risk | Low risk |
| Zhang, 2020 [36] | Some concerns | High risk | Low risk | High risk | Low risk | High risk |
| OCEANS Aghajanian, 2015 [20] | Low risk | Low risk | Low risk | low risk | Low risk | Low risk |
| GOG-0213 Coleman, 2017 [21] | Low risk | Low risk | Some concerns | Some concerns | Some concerns | Some concerns |
| MITO16B-MaNGO OV2B-ENGOT OV17 Pignata, 2021 [37] | Some concerns | Low risk | Low risk | Some concerns | Low risk | Some concerns |
| NSGO-AVANOVA2/ ENGOT-OV24 Mirza, 2019 [38] | Some concerns | Low risk | Low risk | Some concerns | Low risk | Some concerns |
| Cong, 2019 [39] | Some concerns | High risk | Low risk | High risk | Low risk | High risk |
| AURELIA Pujade-Lauraine, 2014 [22] | Some concerns | Low risk | Low risk | Some concerns | Low risk | Some concerns |
| Liu, 2019 [41] | Low risk | Some concerns | Low risk | Some concerns | Low risk | Some concerns |
| Zhang, 2019 [40] | Low risk | Some concerns | Low risk | Some concerns | Low risk | Some concerns |
| Author, Year [Ref] | Tumor Types | Total Included Patients | All TE RR (95% CI) | VTE RR (95% CI) | ATE RR (95% CI) |
|---|---|---|---|---|---|
| Scappaticci, 2007 [44] | Lung, colorectal, breast | 1745 | NA | 0.89 (0.66–1.20) p = 0.44 | 1.8 (0.94–3.33) p = 0.076 |
| Nalluri, 2008 [45] | Lung, colorectal, breast, renal, pancreatic | 7956 | NA | 1.33 (1.13–1.56) p < 0.001 | NA |
| Ranpura, 2010 [49] | Lung, colorectal, breast, renal, pancreatic | 12,617 | NA | NA | 1.44 (1.08–1.91) p = 0.013 |
| Azzi, 2010 [50] | not specified | 13,026 | NA | NA | 1.46 (1.11–1.93) p = 0.007 |
| Hurwitz, 2011 [54] | Lung, colorectal, breast, renal, pancreatic | 6055 | NA | 0.91 (0.77–1.06) p = 0.23 | NA |
| Cortes, 2012 [51] | breast | 3784 | NA | 1.02 (0.70–1.61) p = 0.78 | 1.49 (0.70–3.19) p = 0.30 |
| Totzeck, 2017 [52] | Lung, colorectal, breast, renal, ovarian, gastric | 20,500 | NA | 1.29 (1.13–1.48) p = 0.0001 | 1.37 (1.10–1.70) p = 0.004 |
| Li, 2018 [53] | lung | 3555 | 1.74 (1.15–2.62) p = 0.008 | NA | NA |
| Author, Year [Ref] | Therapeutic Agents Included | Total Included Patients | All TE RR (95% CI) | VTE RR (95% CI) | ATE RR (95% CI) |
|---|---|---|---|---|---|
| Zhou, 2013 [55] | bevacizumab | 3621 | NA | 1.32 (0.99–1.75) p = 0.054 | 2.29 (1.33–3.75) p < 0.03 |
| Wang, 2014 [60] | bevacizumab | 3608 | 1.85 (1.18–2.91) | NA | NA |
| Li, 2015 [56] | bevacizumab | 3621 | NA | NA | 2.33 (1.34–4.03) p = 0.003 |
| Yi, 2017 [57] | bevacizumab | 3211 | NA | NA | 4.84 (1.24–12.98) p = 0.03 |
| Wu, 2017 [59] | bevacizumab | 4994 | NA | 1.43 (1.04–1.96) p = 0.03 | 2.39 (1.39–4.10) p = 0.002 |
| Wang, 2018 [58] | Bevacizumab, sorafenib, nintedanib, pazopanib, aflibercept | 8721 | NA | 1.08 (0.79–1.48) | 2.27 (1.34–3.84) |
| Our analysis | bevacizumab | 6119 | NA | 1.32 (1.02–1.78) p = 0.04 | 2.45 (1.27–4.72) p = 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saerens, M.; De Jaeghere, E.A.; Kanervo, H.; Vandemaele, N.; Denys, H.; Naert, E. Risk of Thrombo-Embolic Events in Ovarian Cancer: Does Bevacizumab Tilt the Scale? A Systematic Review and Meta-Analysis. Cancers 2021, 13, 4603. https://doi.org/10.3390/cancers13184603
Saerens M, De Jaeghere EA, Kanervo H, Vandemaele N, Denys H, Naert E. Risk of Thrombo-Embolic Events in Ovarian Cancer: Does Bevacizumab Tilt the Scale? A Systematic Review and Meta-Analysis. Cancers. 2021; 13(18):4603. https://doi.org/10.3390/cancers13184603
Chicago/Turabian StyleSaerens, Michael, Emiel A. De Jaeghere, Heini Kanervo, Nele Vandemaele, Hannelore Denys, and Eline Naert. 2021. "Risk of Thrombo-Embolic Events in Ovarian Cancer: Does Bevacizumab Tilt the Scale? A Systematic Review and Meta-Analysis" Cancers 13, no. 18: 4603. https://doi.org/10.3390/cancers13184603