
Skeletal Muscle Loss and Octogenarian Status Are Associated with S-1 Adjuvant Therapy Discontinuation and Poor Prognosis after Pancreatectomy

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Treatment and Data Collection
2.3. Definition and Determination of Skeletal Muscle Loss
2.4. Evaluation of Inflammatory and Nutritional Factors
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.2. Prognostic Factors Associated with OS
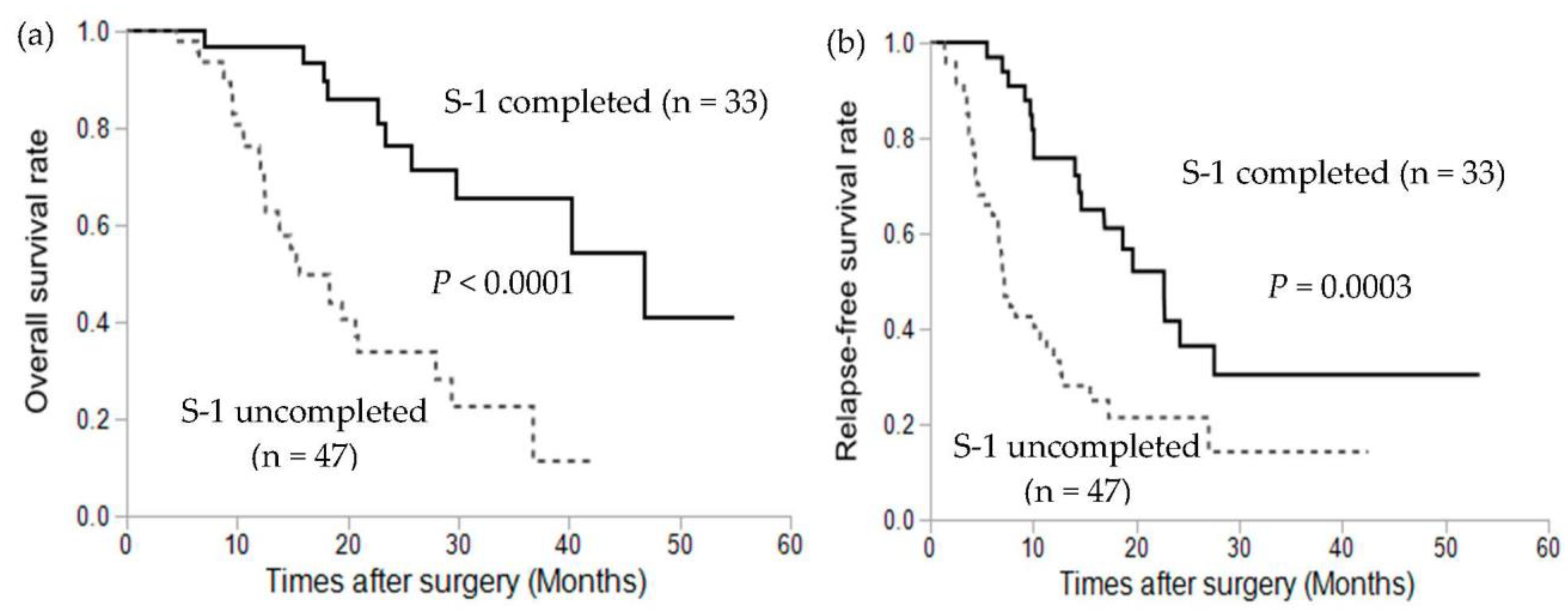
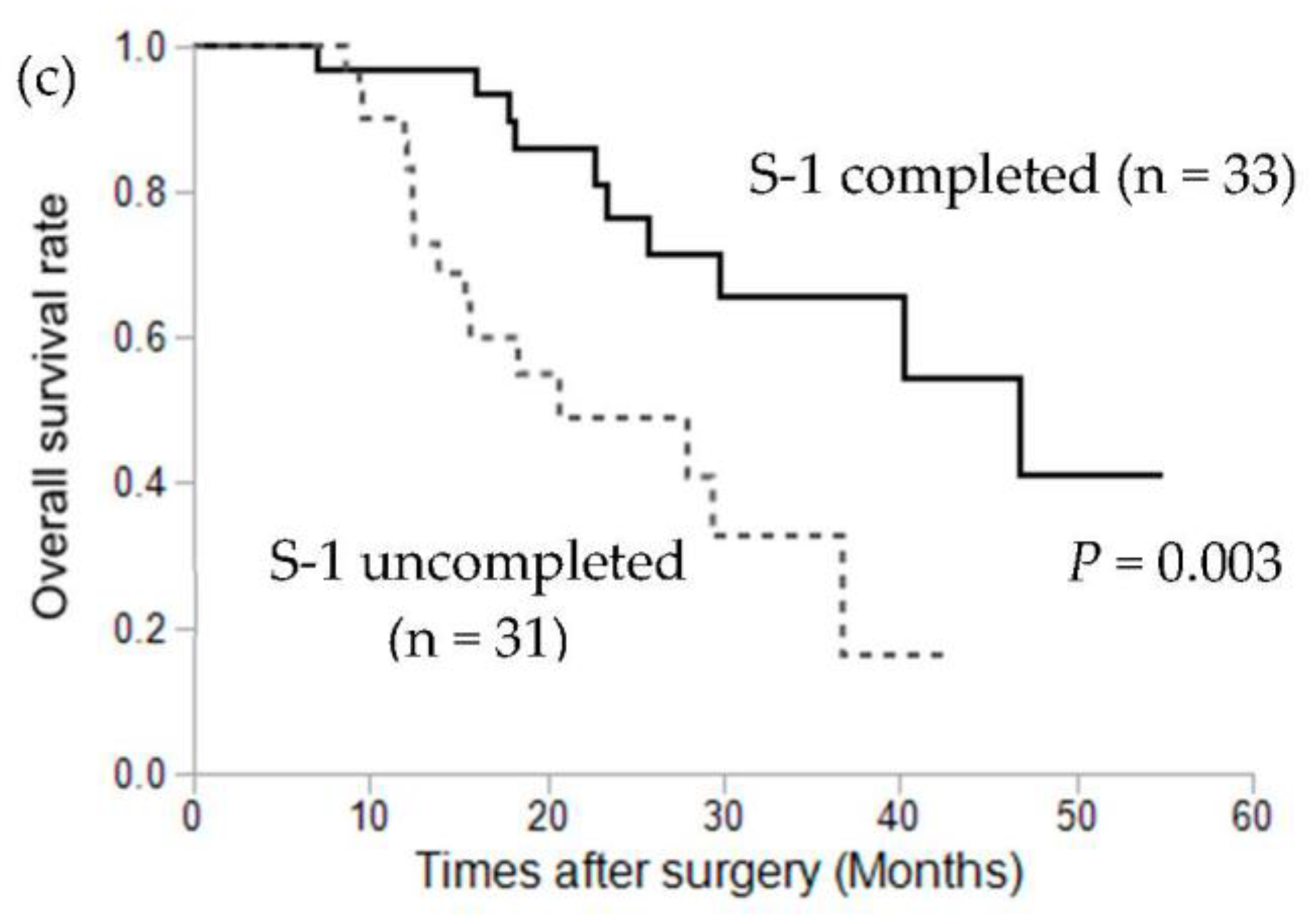
3.3. Association between S-1 Adjuvant Chemotherapy Completion and Prognosis
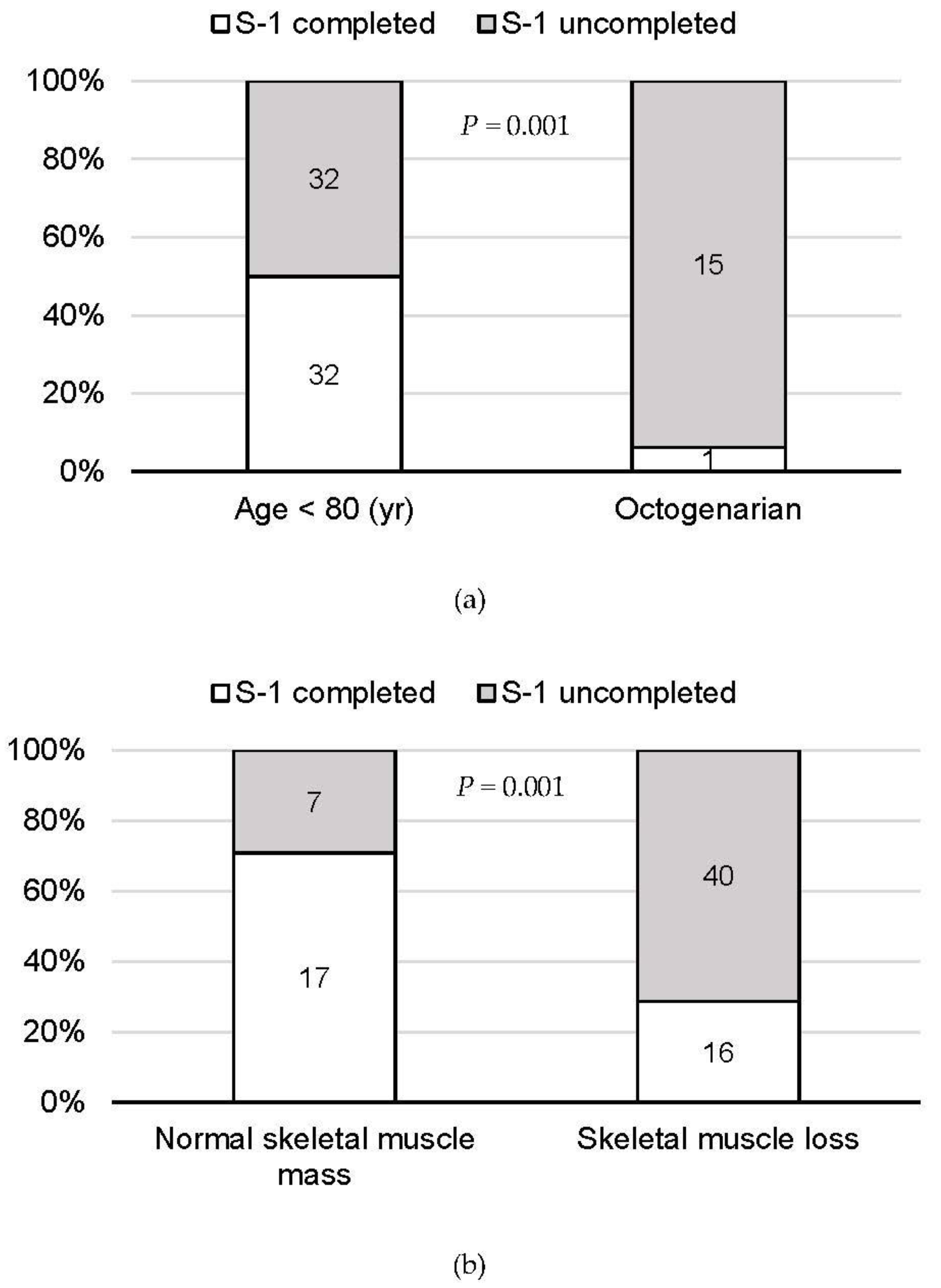
3.4. Factors Associated with S-1 Adjuvant Chemotherapy Completion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Statistics Bureau Ministry of Internal Affairs and Communications. Available online: https://www.stat.go.jp/data/topics/topi1211.html (accessed on 1 August 2021).
- Beltrame, V.; Gruppo, M.; Pastorelli, D.; Pedrazzoli, S.; Merigliano, S.; Sperti, C. Outcome of Pancreaticoduodenectomy in Octogenarians: Single Institution’s Experience and Review of the Literature. J. Visc. Surg. 2015, 152, 279–284. [Google Scholar] [CrossRef]
- Ansari, D.; Aronsson, L.; Fredriksson, J.; Andersson, B.; Andersson, R. Safety of Pancreatic Resection in the Elderly: A Retrospective Analysis of 556 Patients. Ann. Gastroenterol. 2016, 29, 221–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, Y.; Kenmochi, T.; Irino, T.; Egawa, T.; Hayashi, S.; Nagashima, A.; Kitagawa, Y. The Impact of Surgical Outcome After Pancreaticoduodenectomy in Elderly Patients. World J. Surg. Oncol. 2011, 9, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kow, A.W.; Sadayan, N.A.; Ernest, A.; Wang, B.; Chan, C.Y.; Ho, C.K.; Liau, K.H. Is Pancreaticoduodenectomy Justified in Elderly Patients? Surgeon 2012, 10, 128–136. [Google Scholar] [CrossRef]
- Lahat, G.; Sever, R.; Lubezky, N.; Nachmany, I.; Gerstenhaber, F.; Ben-Haim, M.; Nakache, R.; Koriansky, J.; Klausner, J.M. Pancreatic Cancer: Surgery is a Feasible Therapeutic Option for Elderly Patients. World J. Surg. Oncol. 2011, 9, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riall, T.S.; Reddy, D.M.; Nealon, W.H.; Goodwin, J.S. The Effect of Age on Short-Term Outcomes after Pancreatic Resection: A Population-Based Study. Ann. Surg. 2008, 248, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Sukharamwala, P.; Thoens, J.; Szuchmacher, M.; Smith, J.; DeVito, P. Advanced Age is a Risk Factor for Post-Operative Complications and Mortality After a Pancreaticoduodenectomy: A Meta-Analysis and Systematic Review. HPB 2012, 14, 649–657. [Google Scholar]
- Oguro, S.; Shimada, K.; Kishi, Y.; Nara, S.; Esaki, M.; Kosuge, T. Perioperative and Long-Term Outcomes after Pancreaticoduodenectomy in Elderly Patients 80 Years of Age and Older. Langenbecks Arch. Surg. 2013, 398, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Uesaka, K.; Boku, N.; Fukutomi, A.; Okamura, Y.; Konishi, M.; Matsumoto, I.; Kaneoka, Y.; Shimizu, Y.; Nakamori, S.; Sakamoto, H.; et al. JASPAC 01 Study Group. Adjuvant Chemotherapy of S-1 Versus Gemcitabine for Resected Pancreatic Cancer: A phase 3, Open-Label, Randomised, Non-Inferiority Trial (JASPAC 01). Lancet 2016, 388, 248–257. [Google Scholar] [CrossRef]
- Bundred, J.; Kamarajah, S.K.; Roberts, K.J. Body Composition Assessment and Sarcopenia in Patients with Pancreatic Cancer: A Systematic Review and Meta-Analysis. HPB 2019, 21, 1603–1612. [Google Scholar] [CrossRef]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Abellan van Kan, G.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An Undiagnosed Condition in Older Adults. Current Consensus Definition: Prevalence, Etiology, and Consequences. International Working Group on Sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Kurita, Y.; Kobayashi, N.; Tokuhisa, M.; Goto, A.; Kubota, K.; Endo, I.; Nakajima, A.; Ichikawa, Y. Sarcopenia Is a Reliable Prognostic Factor in Patients with Advanced Pancreatic Cancer Receiving FOLFIRINOX Chemotherapy. Pancreatology 2019, 19, 127–135. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of Surgical Complications: A New Proposal with Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; Wiley-Liss: New York, NY, USA, 2009. [Google Scholar]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. Japan Society of Hepatology guidelines for sarcopenia in liver disease (1st edition): Recommendation from the working group for creation of sarcopenia assessment criteria. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef]
- Kinoshita, A.; Onoda, H.; Imai, N.; Iwaku, A.; Oishi, M.; Fushiya, N.; Koike, K.; Nishino, H.; Tajiri, H. Comparison of the Prognostic Value of Inflammation-Based Prognostic Scores in Patients with Hepatocellular Carcinoma. Br. J. Cancer 2012, 107, 988–993. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.; Chan, S.L.; Wong, G.L.; Wong, V.W.; Chong, C.C.; Lai, P.B.; Chan, H.L.; To, K.F. Prognostic Nutritional Index (PNI) Predicts Tumor Recurrence of Very Early/Early Stage Hepatocellular Carcinoma After Surgical Resection. Ann. Surg. Oncol. 2015, 22, 4138–4148. [Google Scholar] [CrossRef] [PubMed]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. An Inflammation-Based Prognostic Score (mGPS) Predicts Cancer Survival Independent of Tumour Site: A Glasgow Inflammation Outcome Study. Br. J. Cancer 2011, 104, 726–734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papis, D.; Vagliasindi, A.; Maida, P. Hepatobiliary and Pancreatic Surgery in the Elderly: Current Status. Ann. Hepatobiliary Pancreat Surg. 2020, 24, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hardacre, J.M.; Simo, K.; McGee, M.F.; Stellato, T.A.; Schulak, J.A. Pancreatic Resection in Octogenarians. J. Surg. Res. 2009, 156, 129–132. [Google Scholar] [CrossRef]
- Hatzaras, I.; Schmidt, C.; Klemanski, D.; Muscarella, P.; Melvin, W.S.; Ellison, E.C.; Bloomston, M. Pancreatic Resection in the Octogenarian: A Safe Option for Pancreatic Malignancy. J. Am. Coll. Surg. 2011, 212, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.K.; Dinorcia, J.; Reavey, P.L.; Holden, M.M.; Genkinger, J.M.; Lee, J.A.; Schrope, B.A.; Chabot, J.A.; Allendorf, J.D. Pancreaticoduodenectomy Can Be Performed Safely in Patients Aged 80 Years and Older. J. Gastrointest. Surg. 2010, 14, 1838–1846. [Google Scholar] [CrossRef]
- Kim, J.H.; Min, S.K.; Lee, H.; Hong, G.; Lee, H.K. The Safety and Risk Factors of Major Hepatobiliary Pancreatic Surgery in Patients Older than 80 Years. Ann. Surg. Treat. Res. 2016, 91, 288–294. [Google Scholar] [CrossRef] [Green Version]
- Nagrial, A.M.; Chang, D.K.; Nguyen, N.Q.; Johns, A.L.; Chantrill, L.A.; Humphris, J.L.; Chin, V.T.; Samra, J.S.; Gill, A.J.; Pajic, M.; et al. Adjuvant Chemotherapy in Elderly Patients with Pancreatic Cancer. Br. J. Cancer 2014, 110, 313–319. [Google Scholar] [CrossRef] [Green Version]
- Aoyama, T.; Katayama, Y.; Murakawa, M.; Atsumi, Y.; Yamaoku, K.; Kanazawa, A.; Higuchi, A.; Shiozawa, M.; Kobayashi, S.; Ueno, M.; et al. Safety and Feasibility of S-1 Adjuvant Chemotherapy for Pancreatic Cancer in Elderly Patients. Cancer Chemother. Pharmacol. 2015, 75, 1115–1120. [Google Scholar] [CrossRef] [PubMed]
- Shimoda, M.; Kubota, K.; Shimizu, T.; Katoh, M. Randomized Clinical Trial of Adjuvant Chemotherapy with S-1 Versus Gemcitabine After Pancreatic Cancer Resection. Br. J. Surg. 2015, 102, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, I.H. Sarcopenia: Origins and Clinical Relevance. J. Nutr. 1997, 127, 990S–991S. [Google Scholar] [CrossRef] [Green Version]
- Chan, M.Y.; Chok, K.S.H. Sarcopenia in Pancreatic Cancer—Effects on Surgical Outcomes and Chemotherapy. World J. Gastrointest. Oncol. 2019, 11, 527–537. [Google Scholar] [CrossRef]
- Ozola Zalite, I.; Zykus, R.; Francisco Gonzalez, M.; Saygili, F.; Pukitis, A.; Gaujoux, S.; Charnley, R.M.; Lyadov, V. Influence of Cachexia and Sarcopenia on Survival in Pancreatic Ductal Adenocarcinoma: A Systematic Review. Pancreatology 2015, 15, 19–24. [Google Scholar] [CrossRef]
- Ishii, N.; Iwata, Y.; Nishikawa, H.; Enomoto, H.; Aizawa, N.; Ishii, A.; Miyamoto, Y.; Yuri, Y.; Hasegawa, K.; Nakano, C.; et al. Effect of Pretreatment Psoas Muscle Mass on Survival for Patients with Unresectable Pancreatic Cancer Undergoing Systemic Chemotherapy. Oncol. Lett. 2017, 14, 6059–6065. [Google Scholar] [CrossRef] [Green Version]
- Centonze, L.; Di Sandro, S.; Lauterio, A.; De Carlis, R.; Botta, F.; Mariani, A.; Bagnardi, V.; De Carlis, L. The Impact of Sarcopenia on Postoperative Course Following Pancreatoduodenectomy: Single-Center Experience of 110 Consecutive Cases. Dig. Surg. 2020, 37, 312–320. [Google Scholar] [CrossRef] [PubMed]
- Prado, C.M.; Baracos, V.E.; McCargar, L.J.; Mourtzakis, M.; Mulder, K.E.; Reiman, T.; Butts, C.A.; Scarfe, A.G.; Sawyer, M.B. Body Composition as an Independent Determinant of 5-Fluorouracil-Based Chemotherapy Toxicity. Clin. Cancer Res. 2007, 13, 3264–3268. [Google Scholar] [CrossRef] [Green Version]
- Cousin, S.; Hollebecque, A.; Koscielny, S.; Mir, O.; Varga, A.; Baracos, V.E.; Soria, J.C.; Antoun, S. Low Skeletal Muscle Is Associated with Toxicity in Patients Included in Phase I Trials. Investig. New Drugs 2014, 32, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Oh, D.Y.; Kim, T.Y.; Lee, K.H.; Han, S.W.; Im, S.A.; Kim, T.Y.; Bang, Y.J. Skeletal Muscle Depletion Predicts the Prognosis of Patients with Advanced Pancreatic Cancer Undergoing Palliative Chemotherapy, Independent of Body Mass Index. PLoS ONE 2015, 10, e0139749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinoshita, S.; Sho, M.; Yanagimoto, H.; Satoi, S.; Akahori, T.; Nagai, M.; Nishiwada, S.; Yamamoto, T.; Hirooka, S.; Yamaki, S.; et al. Potential Role of Surgical Resection for Pancreatic Cancer in the Very Elderly. Pancreatology 2015, 15, 240–246. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Factors | Patients (N = 80) |
|---|---|
| Age, years | 72 (42–88) |
| Octogenarian | 16 (20%) |
| Sex (male/female) | 43/37 |
| Skeletal muscle loss | 56 (70%) |
| ASA PS classification (I/II/III/IV/V/VI) | 1/67/12/0/0/0 |
| Operation | |
| pancreaticoduodenectomy | 52 |
| distal pancreatectomy | 26 |
| total pancreatectomy | 2 |
| Disease stage | |
| IA, IB, IIA | 28 |
| IIB, IV | 52 |
| R0 resection | 63 (79%) |
| Complications (Clavien–Dindo grade ≥III) | 19 (24%) |
| S-1 adjuvant therapy completion | 33 (41%) |
| Recurrence | 56 (70%) |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95%CI | p | Odds Ratio | 95%CI | p | |
| Octogenarian | 2.69 | 1.29–5.62 | 0.008 * | 1.19 | 0.50–2.81 | 0.698 |
| Female sex | 1.02 | 0.54–1.91 | 0.950 | |||
| BMI <18.5 kg/m2 | 1.18 | 0.45–3.06 | 0.740 | |||
| Skeletal muscle loss | 1.79 | 0.87–3.68 | 0.115 | |||
| ASA PS ≥3 | 0.90 | 0.35–2.31 | 0.898 | |||
| PNI <45 | 1.14 | 0.55–2.38 | 0.723 | |||
| mGPS ≥1 | 2.76 | 1.11–6.85 | 0.029 * | 2.30 | 0.85–6.19 | 0.100 |
| Operation (PD, TP vs. DP) | 1.14 | 0.58–2.24 | 0.710 | |||
| R1 resection | 0.97 | 0.44–2.10 | 0.929 | |||
| Tumor size ≥30 mm | 1.73 | 0.88–3.40 | 0.114 | |||
| Lymph node metastasis | 1.62 | 0.79–3.34 | 0.189 | |||
| Stage ≥IIB | 1.85 | 0.87–3.90 | 0.108 | |||
| Complications (Clavien–Dindo grade ≥III) | 0.84 | 0.38–1.82 | 0.652 | |||
| S-1 adjuvant therapy <6 months | 4.62 | 2.15–9.94 | <0.0001 * | 3.99 | 1.76–9.03 | 0.0009 * |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Odds Ratio | 95%CI | p | Odds Ratio | 95%CI | p | |
| Octogenarian | 15.00 | 1.87–120.39 | 0.011 * | 15.94 | 1.82–140.06 | 0.013 * |
| Female sex | 1.30 | 0.53–3.19 | 0.566 | |||
| BMI <18.5 kg/m2 | 1.27 | 0.34–4.74 | 0.723 | |||
| Skeletal muscle loss | 6.07 | 2.12–17.42 | 0.0008 * | 6.37 | 1.99–20.37 | 0.002 * |
| ASA PS ≥3 | 0.98 | 0.28–3.40 | 0.975 | |||
| PNI <45 | 1.42 | 0.49–4.14 | 0.517 | |||
| mGPS ≥1 | 2.27 | 0.43–12.11 | 0.337 | |||
| Operation (PD, TP vs. DP) | 1.35 | 0.52–3.47 | 0.537 | |||
| Complications (Clavien–Dindo grade ≥III) | 0.72 | 0.26–2.03 | 0.536 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsukagoshi, M.; Harimoto, N.; Araki, K.; Kubo, N.; Watanabe, A.; Igarashi, T.; Ishii, N.; Yamanaka, T.; Hagiwara, K.; Hoshino, K.; et al. Skeletal Muscle Loss and Octogenarian Status Are Associated with S-1 Adjuvant Therapy Discontinuation and Poor Prognosis after Pancreatectomy. Cancers 2021, 13, 4105. https://doi.org/10.3390/cancers13164105
Tsukagoshi M, Harimoto N, Araki K, Kubo N, Watanabe A, Igarashi T, Ishii N, Yamanaka T, Hagiwara K, Hoshino K, et al. Skeletal Muscle Loss and Octogenarian Status Are Associated with S-1 Adjuvant Therapy Discontinuation and Poor Prognosis after Pancreatectomy. Cancers. 2021; 13(16):4105. https://doi.org/10.3390/cancers13164105
Chicago/Turabian StyleTsukagoshi, Mariko, Norifumi Harimoto, Kenichiro Araki, Norio Kubo, Akira Watanabe, Takamichi Igarashi, Norihiro Ishii, Takahiro Yamanaka, Kei Hagiwara, Kouki Hoshino, and et al. 2021. "Skeletal Muscle Loss and Octogenarian Status Are Associated with S-1 Adjuvant Therapy Discontinuation and Poor Prognosis after Pancreatectomy" Cancers 13, no. 16: 4105. https://doi.org/10.3390/cancers13164105