
On-Treatment Albumin-Bilirubin Grade: Predictor of Response and Outcome of Sorafenib-Regorafenib Sequential Therapy in Patients with Unresectable Hepatocellular Carcinoma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Recruitment and Definitions
2.2. Statistical Analysis
3. Results
3.1. Baseline and On-Treatment Characteristics
3.2. Response to Sequential Therapy with Regorafenib
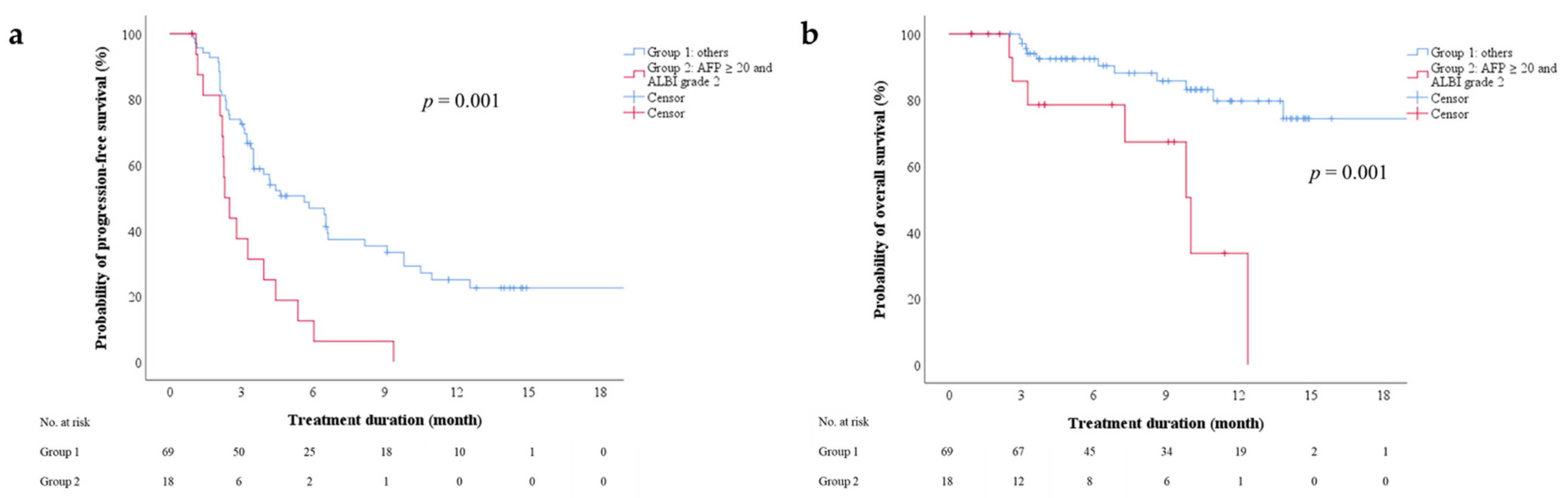
3.3. On-Treatment Factors Associated with PFS after Regorafenib Therapy
3.4. On-Treatment Factors Associated with Overall Survival (OS) after Regorafenib Therapy
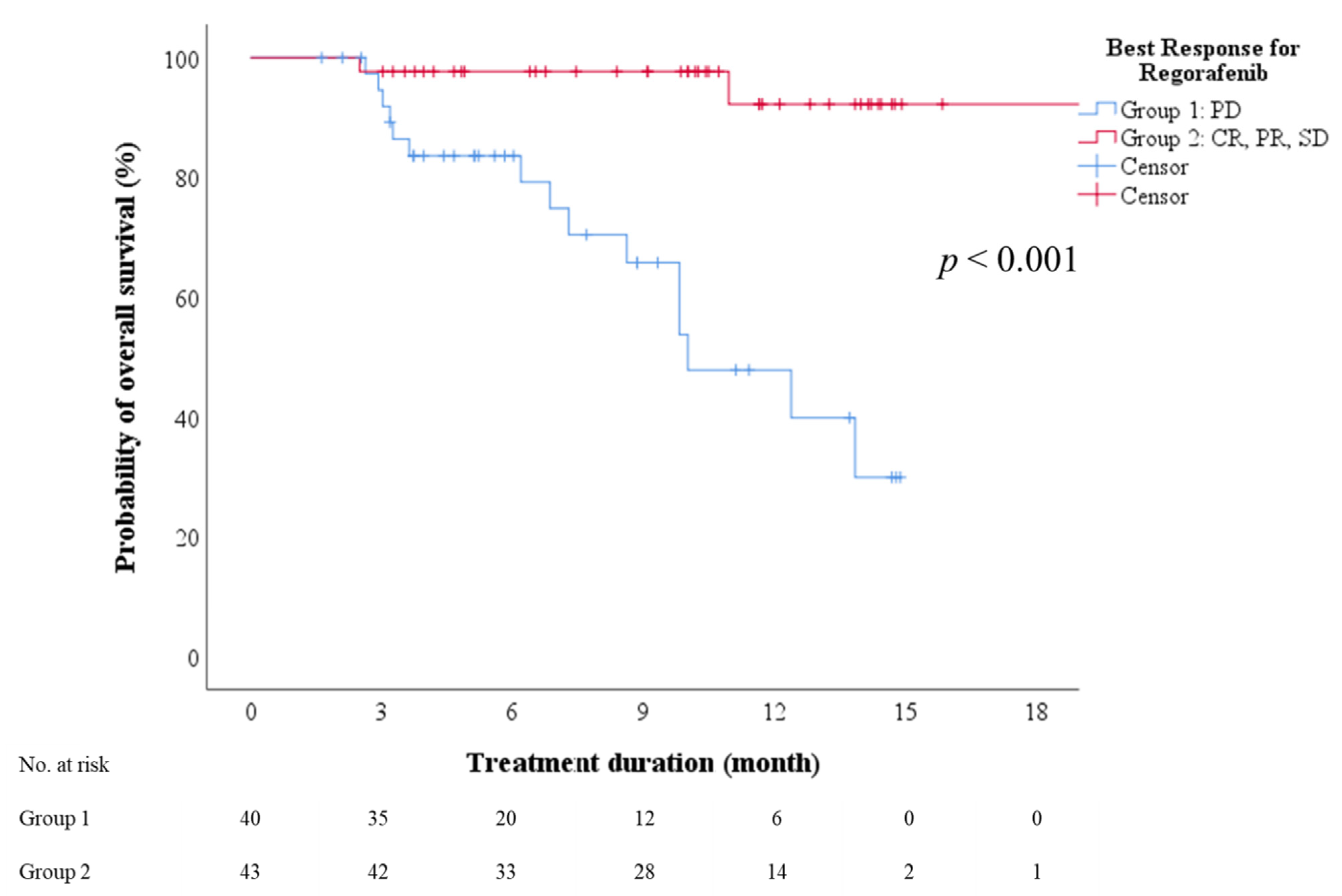
3.5. On-Treatment Factors Associated with OS after Sorafenib-Regorafenib Sequential Therapy
3.6. On-Treatment Factors Associated with Response to Regorafenib Therapy
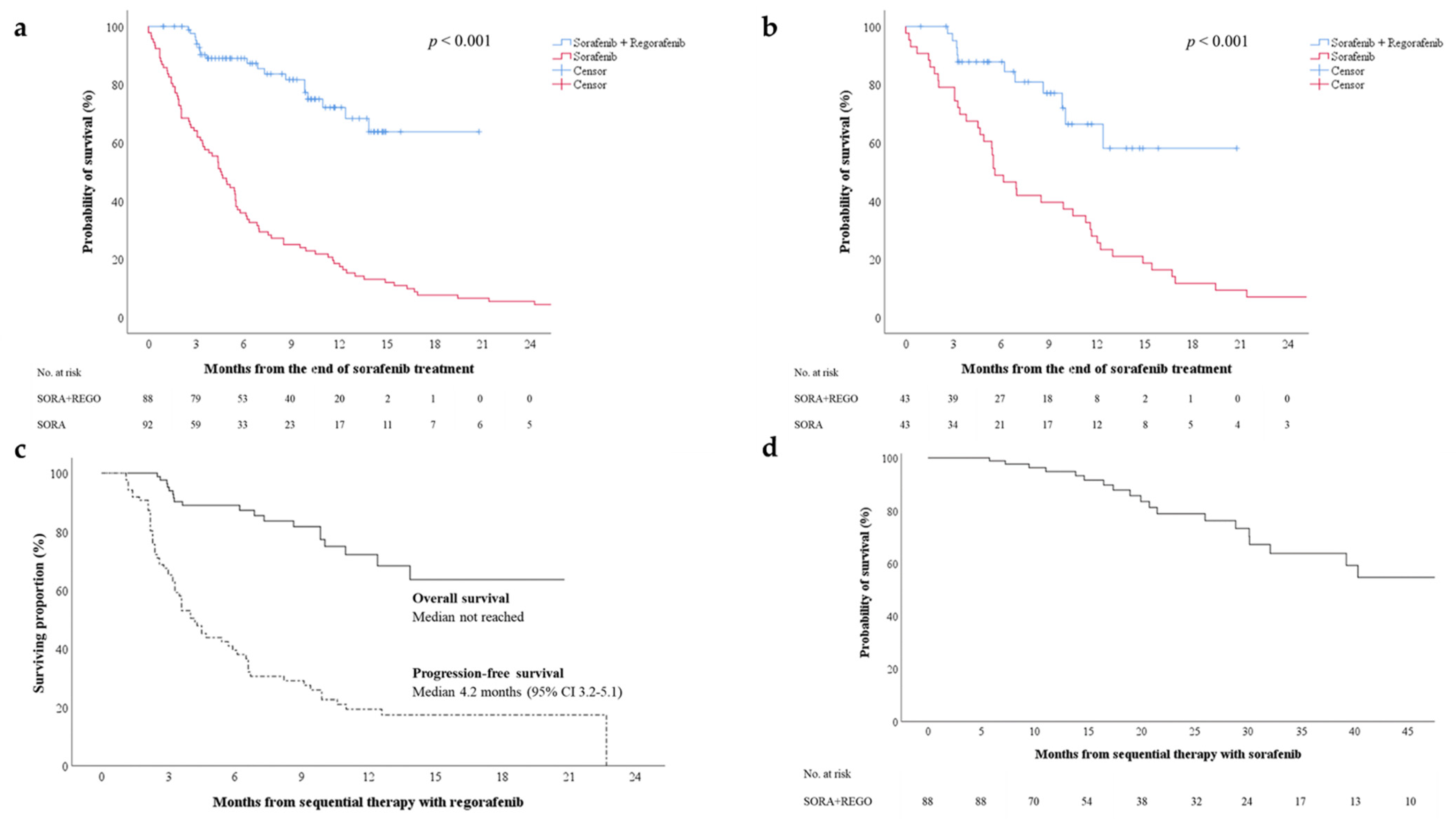
3.7. Effect of Sorafenib–Regorafenib Sequential Therapy on OS
3.8. Association of Adverse Event Profile with Sorafenib-Regorafenib Sequential Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kudo, M.; Venook, A.P.; Ye, S.L.; Bronowicki, J.P.; Chen, X.P.; Dagher, L.; Furuse, J.; Geschwind, J.H.; de Guevara, L.L.; et al. Observational registry of sorafenib use in clinical practice across Child-Pugh subgroups: The GIDEON study. J. Hepatol. 2016, 65, 1140–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirstein, M.M.; Scheiner, B.; Marwede, T.; Wolf, C.; Voigtlander, T.; Semmler, G.; Wacker, F.; Manns, M.P.; Hinrichs, J.B.; Pinter, M.; et al. Sequential systemic treatment in patients with hepatocellular carcinoma. Aliment. Pharm. Ther. 2020, 52, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): A non-randomised, open-label phase 2 trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- Yau, T.; Hsu, C.; Kim, T.Y.; Choo, S.P.; Kang, Y.K.; Hou, M.M.; Numata, K.; Yeo, W.; Chopra, A.; Ikeda, M.; et al. Nivolumab in advanced hepatocellular carcinoma: Sorafenib-experienced Asian cohort analysis. J. Hepatol. 2019, 71, 543–552. [Google Scholar] [CrossRef] [Green Version]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased alpha-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Bangaru, S.; Marrero, J.A.; Singal, A.G. Review article: New therapeutic interventions for advanced hepatocellular carcinoma. Aliment. Pharm. Ther. 2020, 51, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 389, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O′Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Kudo, M. Newly Proposed ALBI Grade and ALBI-T Score as Tools for Assessment of Hepatic Function and Prognosis in Hepatocellular Carcinoma Patients. Liver Cancer 2019, 8, 312–325. [Google Scholar] [CrossRef]
- Kariyama, K.; Nouso, K.; Hiraoka, A.; Wakuta, A.; Oonishi, A.; Kuzuya, T.; Toyoda, H.; Tada, T.; Tsuji, K.; Itobayashi, E.; et al. EZ-ALBI Score for Predicting Hepatocellular Carcinoma Prognosis. Liver Cancer 2020, 9, 734–743. [Google Scholar] [CrossRef]
- Takada, H.; Kurosaki, M.; Tsuchiya, K.; Komiyama, Y.; Itakura, J.; Takahashi, Y.; Nakanishi, H.; Yasui, Y.; Tamaki, N.; Maeyashiki, C.; et al. Baseline and Early Predictors of Good Patient Candidates for Second-Line after Sorafenib Treatment in Unresectable Hepatocellular Carcinoma. Cancers 2019, 11, 1256. [Google Scholar] [CrossRef] [Green Version]
- Tokunaga, T.; Tanaka, M.; Tanaka, K.; Narahara, S.; Kawasaki, T.; Yoshimaru, Y.; Nagaoka, K.; Watanabe, T.; Tateyama, M.; Naoe, H.; et al. Modified albumin-bilirubin grade to predict eligibility for second-line therapies at progression on sorafenib therapy in hepatocellular carcinoma patients. Int. J. Clin. Oncol. 2021, 26, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Finn, R.S.; Kang, Y.K.; Yen, C.J.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Motomura, K.; Ohno, I.; et al. Serum alpha-fetoprotein and clinical outcomes in patients with advanced hepatocellular carcinoma treated with ramucirumab. Br. J. Cancer 2021, 124, 1388–1397. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Di Bisceglie, A.M.; Bruix, J.; Kramer, B.S.; Lencioni, R.; Zhu, A.X.; Sherman, M.; Schwartz, M.; Lotze, M.; Talwalkar, J.; et al. Design and endpoints of clinical trials in hepatocellular carcinoma. J. Natl. Cancer Inst. 2008, 100, 698–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.Y.; Merle, P.; Finn, R.S.; Frenette, C.; Masi, G.; Ikeda, M.; Zebger-Gong, H.; Fiala-Buskies, S.; Ozgurdal, K.; Kudo, M.; et al. Regorafenib in patients with unresectable hepatocellular carcinoma (uHCC) in routine clinical practice: Interim analysis of the prospective, observational REFINE trial. J. Clin. Oncol. 2020, 38, 542. [Google Scholar] [CrossRef]
- Wang, W.; Tsuchiya, K.; Kurosaki, M.; Yasui, Y.; Inada, K.; Kirino, S.; Yamashita, K.; Sekiguchi, S.; Hayakawa, Y.; Osawa, L.; et al. Sorafenib-Regorafenib Sequential Therapy in Japanese Patients with Unresectable Hepatocellular Carcinoma-Relative Dose Intensity and Post-Regorafenib Therapies in Real World Practice. Cancers 2019, 11, 1517. [Google Scholar] [CrossRef] [Green Version]
- Ogasawara, S.; Ooka, Y.; Itokawa, N.; Inoue, M.; Okabe, S.; Seki, A.; Haga, Y.; Obu, M.; Atsukawa, M.; Itobayashi, E.; et al. Sequential therapy with sorafenib and regorafenib for advanced hepatocellular carcinoma: A multicenter retrospective study in Japan. Investig. New Drugs 2020, 38, 172–180. [Google Scholar] [CrossRef]
- Yoo, C.; Byeon, S.; Bang, Y.; Cheon, J.; Kim, J.W.; Kim, J.H.; Chon, H.J.; Kang, B.; Kang, M.J.; Kim, I.; et al. Regorafenib in previously treated advanced hepatocellular carcinoma: Impact of prior immunotherapy and adverse events. Liver Int. 2020, 40, 2263–2271. [Google Scholar] [CrossRef]
- Lee, S.; Kim, B.K.; Kim, S.U.; Park, S.Y.; Kim, J.K.; Lee, H.W.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Tak, W.Y.; et al. Clinical outcomes and prognostic factors of patients with advanced hepatocellular carcinoma treated with sorafenib as first-line therapy: A Korean multicenter study. J. Gastroenterol. Hepatol. 2014, 29, 1463–1469. [Google Scholar] [CrossRef]
- Chan, S.L.; Mo, F.K.; Johnson, P.J.; Hui, E.P.; Ma, B.B.; Ho, W.M.; Lam, K.C.; Chan, A.T.; Mok, T.S.; Yeo, W. New utility of an old marker: Serial alpha-fetoprotein measurement in predicting radiologic response and survival of patients with hepatocellular carcinoma undergoing systemic chemotherapy. J. Clin. Oncol. 2009, 27, 446–452. [Google Scholar] [CrossRef]
- Kuzuya, T.; Asahina, Y.; Tsuchiya, K.; Tanaka, K.; Suzuki, Y.; Hoshioka, T.; Tamaki, S.; Kato, T.; Yasui, Y.; Hosokawa, T.; et al. Early decrease in alpha-fetoprotein, but not des-gamma-carboxy prothrombin, predicts sorafenib efficacy in patients with advanced hepatocellular carcinoma. Oncology 2011, 81, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Personeni, N.; Bozzarelli, S.; Pressiani, T.; Rimassa, L.; Tronconi, M.C.; Sclafani, F.; Carnaghi, C.; Pedicini, V.; Giordano, L.; Santoro, A. Usefulness of alpha-fetoprotein response in patients treated with sorafenib for advanced hepatocellular carcinoma. J. Hepatol. 2012, 57, 101–107. [Google Scholar] [CrossRef]
- Finn, R.S.; Merle, P.; Granito, A.; Huang, Y.H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Gerolami, R.; Caparello, C.; et al. Outcomes of sequential treatment with sorafenib followed by regorafenib for HCC: Additional analyses from the phase III RESORCE trial. J. Hepatol. 2018, 69, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Gonzalez, A.; Sanduzzi-Zamparelli, M.; Sapena, V.; Torres, F.; Llarch, N.; Iserte, G.; Forner, A.; da Fonseca, L.; Rios, J.; Bruix, J.; et al. Systematic review with meta-analysis: The critical role of dermatological events in patients with hepatocellular carcinoma treated with sorafenib. Aliment. Pharm. Ther. 2019, 49, 482–491. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, A.R.; Sosin, D.M.; Wells, C.K. The Will Rogers phenomenon. Stage migration and new diagnostic techniques as a source of misleading statistics for survival in cancer. N. Engl. J. Med. 1985, 312, 1604–1608. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables Median ± IQR or n (%) | All Patients (n = 88) | Baseline (Before SORA) | On-Treatment (Before REGO) |
|---|---|---|---|
| Age (year) | 65 ± 15 | 66 ± 14 | |
| Sex | Male/female | 69/19 | |
| Etiology | HBV/HCV/ HBV+HCV/NBNC | 45/28/2/13 | |
| ECOG PS | 0/1/2 | 84/4/0 | 75/10/3 |
| Child–Pugh score | 5/6/≥7 | 74/11/3 | 59/24/5 |
| Child–Pugh class | A/B/C | 85/3/0 | 83/5/0 |
| ALBI score | −2.71 ± 0.60 | −2.64 ± 0.57 | |
| ALBI grade | 1/2/3 | 54/33/0 | 48/40/0 |
| FIB-4 | 2.54 ± 2.07 | 3.59 ± 3.13 | |
| FIB-4 | <3.25/≥3.25 | 45/29 | 31/45 |
| BCLC stage | A/B/C | 1/23/64 | 1/23/64 |
| MVI | presence | 24 (27.3) | 28 (31.8) |
| EHS | presence | 44 (50) | 51 (58) |
| AFP (ng/mL) | 10.7 ± 118.5 | 17.3 ± 292.4 | |
| AFP (ng/mL) | <400/≥400 | 72/13 | 66/21 |
| Albumin (g/dL) | 4.1 ± 0.7 | 4.0 ± 0.7 | |
| AST (U/L) | 40 ± 34 | 39 ± 21 | |
| ALT (U/L) | 36 ± 32 | 31 ± 22 | |
| Total bilirubin (mg/dL) | 0.8 ± 0.4 | 0.8 ± 0.5 | |
| INR | 1.04 ± 0.10 | 1.05 ± 0.10 | |
| TKI duration (months) | 5.2 ± 9.8 | 2.8 ± 3.4 | |
| Evaluable Response | All Patients (n = 88) | Child–Pugh A5 (n = 59) | Child–Pugh A6 (n = 24) | ALBI Grade 1 (n = 48) | ALBI Grade 2 (n = 40) |
|---|---|---|---|---|---|
| Best Response, n (%) | |||||
| CR | 3 (3.4) | 2 (3.4) | 1 (4.2) | 3 (6.3) | 0 (0) |
| PR | 14 (15.9) | 11 (18.6) | 2 (8.3) | 8 (16.7) | 6 (15) |
| SD | 26 (29.5) | 20 (33.9) | 5 (20.8) | 20 (41.7) | 6 (15) |
| PD | 40 (45.5) | 24 (40.7) | 14 (58.3) | 16 (33.3) | 24 (60) |
| Non-assessable | 5 | 2 | 2 | 1 | 4 |
| ORR | 17 (19.3) | 13 (22.0) | 3 (12.5) | 11 (22.9) | 6 (15) |
| DCR | 43 (48.9) | 33 (55.9) | 8 (33.3) | 31 (64.6) | 12 (30) |
| For Responders | |||||
| Time to response (days) | 75 (7–357) | 94 (7–357) | 49 (49–59) | 117 (7–357) | 64 (14–94) |
| ALBI Grade-Based Model | Combined ALBI and AFP-Based Model | |||
|---|---|---|---|---|
| Variables | Multivariate Hazard Ratio (95% CI) | p Value | Multivariate
Hazard Ratio (95% CI) | p Value |
| Age (year) | ||||
| Male vs. female | 2.046 (1.050–3.984) | 0.035 | 1.870 (0.965–3.624) | 0.064 |
| ALBI grade 1 vs. 2 | 0.432 (0.258–0.722) | 0.001 | ||
| FIB-4 < 3.25 vs. ≥3.25 | ||||
| BCLC stage B vs. C | ||||
| MVI (no vs. yes) | ||||
| EHS (no vs. yes) | ||||
| AFP (ng/mL) <20 vs. ≥20 (ng/mL) | 0.556 (0.337–0.919) | 0.022 | ||
| ALBI grade 2 and AFP ≥ 20 ng/mL (yes vs. no) | 3.088 (1.704–5.595) | <0.001 | ||
| Albumin (g/dL) | ||||
| AST (U/L) | ||||
| ALT (U/L) | ||||
| Total bilirubin (mg/dL) | ||||
| PLT (109/L) | ||||
| INR |
| ALBI Grade-Based Model | Combined ALBI and AFP-Based Model | |||
|---|---|---|---|---|
| Variables | Multivariate Hazard Ratio (95% CI) | p Value | Multivariate Hazard Ratio (95% CI) | p Value |
| Age (year) | ||||
| Male vs. female | 2.643 (0.584–11.95) | 0.207 | 2.488 (0.558–11.09) | 0.232 |
| ALBI grade 1 vs. 2 | 0.543 (0.190–1.556) | 0.256 | ||
| FIB-4 < 3.25 vs. ≥3.25 | 0.514 (0.158–1.671) | 0.269 | 0.638 (0.197–2.066) | 0.453 |
| BCLC stage B vs. C | ||||
| MVI (no vs. yes) | ||||
| EHS (no vs. yes) | ||||
| AFP (ng/mL) <20 vs. ≥20 (ng/mL) | 0.322 (0.109–0.946) | 0.039 | ||
| ALBI grade 2 and AFP ≥ 20 ng/mL (yes vs. no) | 3.783 (1.316–10.88) | 0.014 | ||
| Albumin (g/dL) | ||||
| AST (U/L) | ||||
| ALT (U/L) | ||||
| Total bilirubin (mg/dL) | ||||
| PLT (109/L) | ||||
| INR |
| ALBI Grade-Based Model | Combined ALBI and AFP-Based Model | |||
|---|---|---|---|---|
| Variables | Multivariate Hazard Ratio (95% CI) | p Value | Multivariate Hazard Ratio (95% CI) | p Value |
| Age (year) | ||||
| Male vs. female | ||||
| ALBI grade 1 vs. 2 | 0.303 (0.112–0.821) | 0.019 | ||
| FIB-4 < 3.25 vs. ≥3.25 | 0.548 (0.161–1.864) | 0.335 | 0.648 (0.181–2.316) | 0.504 |
| BCLC stage B vs. C | 0.612 (0.133–2.814) | 0.528 | 0.790 (0.139–4.485) | 0.790 |
| MVI (no vs. yes) | ||||
| EHS (no vs. yes) | 0.705 (0.205–2.421) | 0.579 | 0.569 (0.129–2.513) | 0.457 |
| AFP (ng/mL) <20 vs. ≥20 (ng/mL) | 0.335 (0.122–0.919) | 0.034 | ||
| ALBI grade 2 and AFP ≥ 20 ng/mL (yes vs. no) | 4.603 (1.386–15.29) | 0.013 | ||
| Albumin (g/dL) | ||||
| AST (U/L) | ||||
| ALT (U/L) | ||||
| Total bilirubin (mg/dL) | ||||
| PLT (109/L) | ||||
| INR |
| AEs, n (%) | Sorafenib(n = 88) | Regorafenib(n = 88) | ||||
| Any | Gr 3 | Gr 4 | Any | Gr 3 | Gr 4 | |
| All TEAE | 56 (63.6) | 26 (29.5) | 1 (1.1) | 78 (88.6) | 13 (14.8) | 1 (1.1) |
| Drug-related TEAE | ||||||
| Hand-foot skin reaction | 52 (59.1) | 19 (21.6) | 0 | 28 (31.8) | 9 (10.2) | 0 |
| Diarrhea | 32 (36.4) | 7 (8.0) | 1 (1.1) | 34 (38.6) | 5 (5.7) | 0 |
| Hypertension | 13 (14.8) | 1 (1.1) | 0 | 4 (4.5) | 0 | 0 |
| Skin rash | 11 (12.5) | 1 (1.1) | 0 | 5 (5.7) | 0 | 0 |
| Fatigue | 8 (9.1) | 0 | 0 | 5 (5.7) | 0 | 0 |
| Hair loss | 5 (5.7) | 0 | 0 | 0 | 0 | 0 |
| Decreased appetite | 4 (4.5) | 0 | 0 | 4 (4.5) | 0 | 0 |
| Abdominal pain | 2 (2.3) | 0 | 0 | 5 (5.7) | 0 | 0 |
| Abnormal LFTs | 1 (1.1) | 0 | 0 | 4 (4.5) | 0 | 1 (1.1) |
| AE, n (%) | Hand-foot Skin Reaction (During Regorafenib Therapy) (n = 88) | |||||
| Gr 0 | Any AE | Gr 1 | Gr 2 | Gr 3 | Gr 4 | |
| Hand-foot skin reaction (during sorafenib therapy) | ||||||
| Gr 0, n = 36 (100) | 29 (80.6) | 7 (19.4) | 2 (5.6) | 1 (2.8) | 4 (11.1) | 0 |
| Any AE, n = 52 (100) | 31 (59.6) | 21 (40.4) | 6 (11.5) | 10 (19.2) | 5 (9.6) | 0 |
| Gr 1, n = 10 (100) | 9 (90) | 1 (10) | 1 (10) | 0 | 0 | 0 |
| Gr 2, n = 23 (100) | 13 (56.5) | 10 (43.5) | 3 (13.0) | 5 (21.7) | 2 (8.7) | 0 |
| Gr 3, n = 19 (100) | 9 (47.4) | 10 (52.6) | 2 (10.5) | 5 (26.3) | 3 (15.8) | 0 |
| Gr 4, n = 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.-W.; Chuang, P.-H.; Su, W.-P.; Kao, J.-T.; Hsu, W.-F.; Lin, C.-C.; Huang, G.-T.; Lin, J.-T.; Lai, H.-C.; Peng, C.-Y. On-Treatment Albumin-Bilirubin Grade: Predictor of Response and Outcome of Sorafenib-Regorafenib Sequential Therapy in Patients with Unresectable Hepatocellular Carcinoma. Cancers 2021, 13, 3758. https://doi.org/10.3390/cancers13153758
Wang H-W, Chuang P-H, Su W-P, Kao J-T, Hsu W-F, Lin C-C, Huang G-T, Lin J-T, Lai H-C, Peng C-Y. On-Treatment Albumin-Bilirubin Grade: Predictor of Response and Outcome of Sorafenib-Regorafenib Sequential Therapy in Patients with Unresectable Hepatocellular Carcinoma. Cancers. 2021; 13(15):3758. https://doi.org/10.3390/cancers13153758
Chicago/Turabian StyleWang, Hung-Wei, Po-Heng Chuang, Wen-Pang Su, Jung-Ta Kao, Wei-Fan Hsu, Chun-Che Lin, Guan-Tarn Huang, Jaw-Town Lin, Hsueh-Chou Lai, and Cheng-Yuan Peng. 2021. "On-Treatment Albumin-Bilirubin Grade: Predictor of Response and Outcome of Sorafenib-Regorafenib Sequential Therapy in Patients with Unresectable Hepatocellular Carcinoma" Cancers 13, no. 15: 3758. https://doi.org/10.3390/cancers13153758