
Characteristics and Lenvatinib Treatment Response of Unresectable Hepatocellular Carcinoma with Iso-High Intensity in the Hepatobiliary Phase of EOB-MRI

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
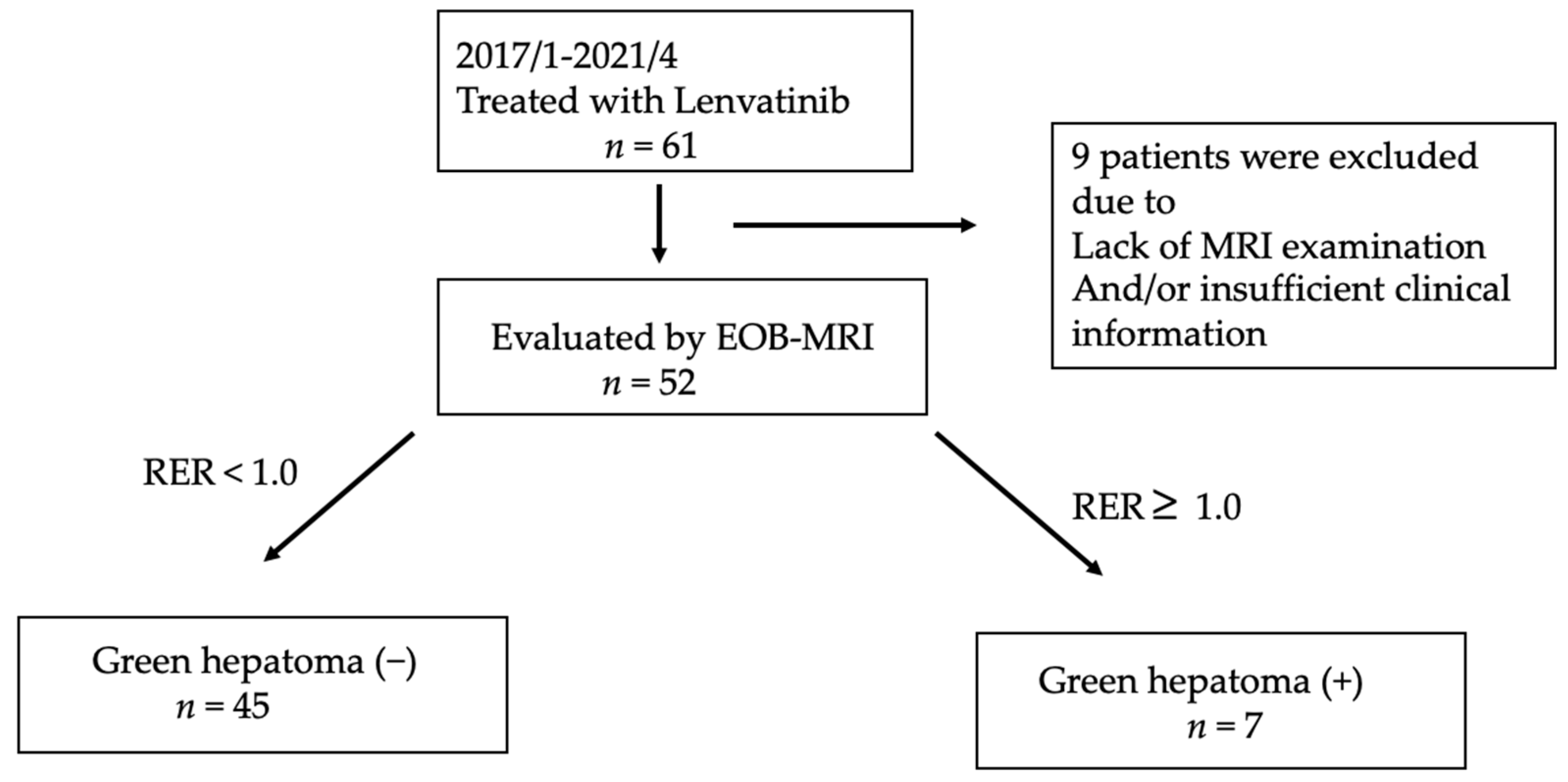
2.1. Patients and Study Design
2.2. Treatment Protocol
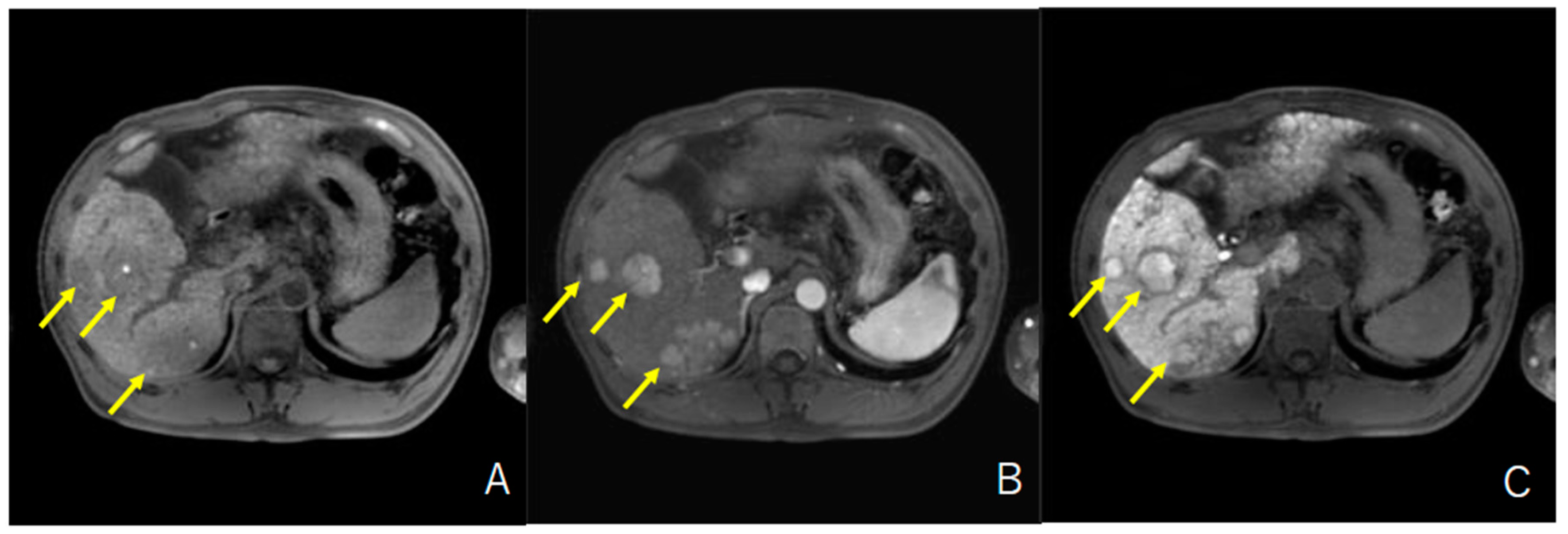
2.3. Evaluation of HCC with Iso-High Intensity in the Hepatobiliary Phase of EOB-MRI
2.4. Evaluation of the Response to Lenvatinib
2.5. CTNNB1 Mutation Detection in Cell-Free DNA
2.6. Statistical Analysis
3. Results
3.1. Enrolled Patients and Baseline Characteristics
3.2. Prevalence and Characteristics of HCC with Iso-High Intensity in the Hepatobiliary Phase of EOB-MRI in Patients with Unresectable HCC Who Were Treated with Lenvatinib
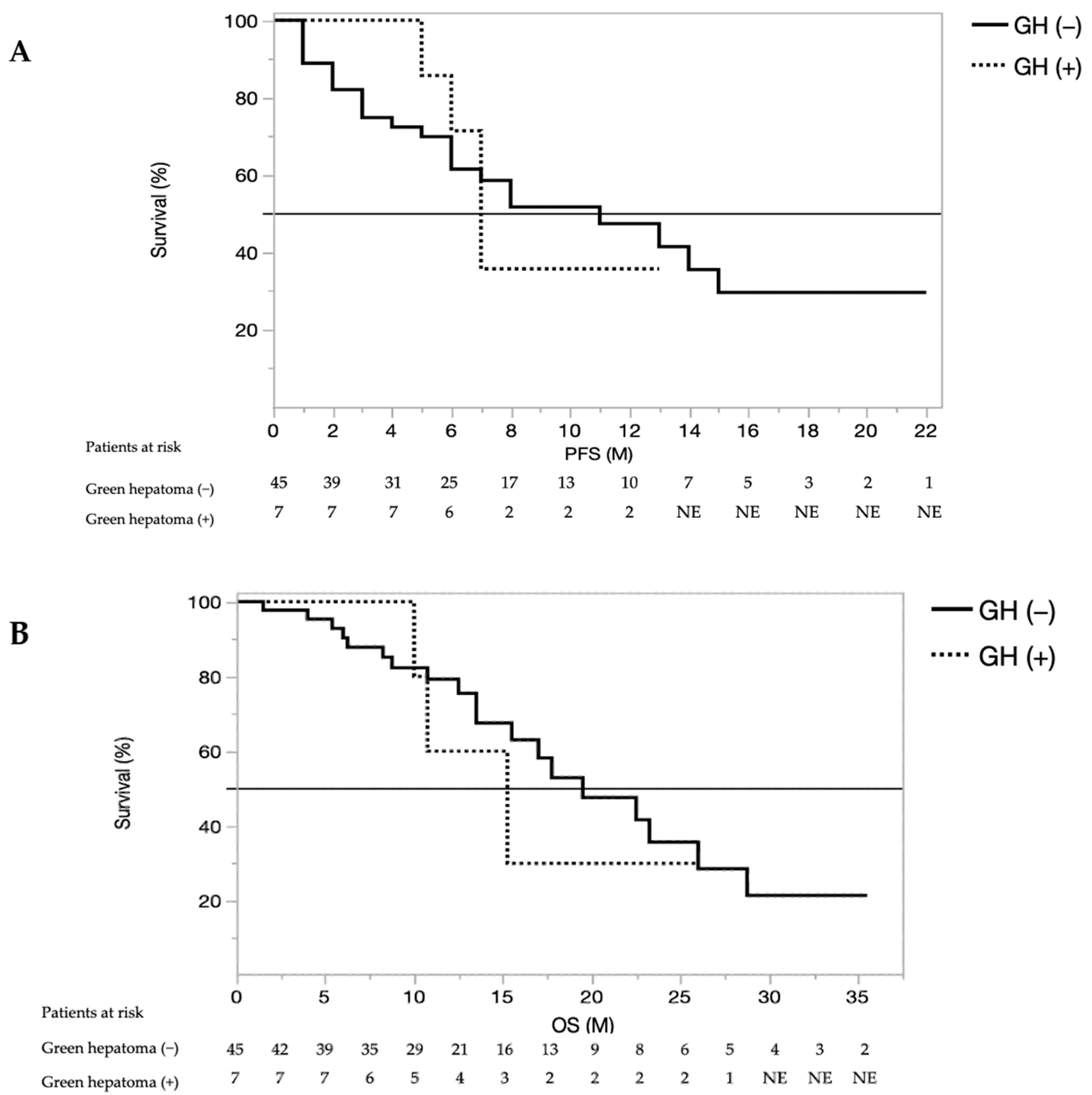
3.3. Treatment Response, Overall Survival, and Progression-Free Survival
3.4. Relationship between HCC with Iso-High Intensity in the Hepatobiliary Phase of EOB-MRI and WNT/β-Catenin Mutations Diagnosed by Cell-Free DNA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, D.; Nelson, D.R.; Bruchfeld, A.; Liapakis, A.; Silva, M.; Monsour, H., Jr.; Martin, P.; Pol, S.; Londono, M.C.; Hassanein, T.; et al. Grazoprevir plus elbasvir in treatment-naive and treatment-experienced patients with hepatitis C virus genotype 1 infection and stage 4–5 chronic kidney disease (the C-SURFER study): A combination phase 3 study. Lancet 2015, 386, 1537–1545. [Google Scholar] [CrossRef]
- Mazza, C.; Escudier, B.; Albiges, L. Nivolumab in renal cell carcinoma: Latest evidence and clinical potential. Ther. Adv. Med. Oncol. 2017, 9, 171–181. [Google Scholar] [CrossRef]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C.; et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Aren Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthelemy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Nakamura, Y. Biomarkers for Immune Checkpoint Inhibitor-Mediated Tumor Response and Adverse Events. Front. Med. 2019, 6, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harding, J.J.; Nandakumar, S.; Armenia, J.; Khalil, D.N.; Albano, M.; Ly, M.; Shia, J.; Hechtman, J.F.; Kundra, R.; El Dika, I.; et al. Prospective Genotyping of Hepatocellular Carcinoma: Clinical Implications of Next-Generation Sequencing for Matching Patients to Targeted and Immune Therapies. Clin. Cancer Res. 2019, 25, 2116–2126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitao, A.; Matsui, O.; Yoneda, N.; Kozaka, K.; Kobayashi, S.; Sanada, J.; Koda, W.; Minami, T.; Inoue, D.; Yoshida, K.; et al. Hepatocellular Carcinoma with beta-Catenin Mutation: Imaging and Pathologic Characteristics. Radiology 2015, 275, 708–717. [Google Scholar] [CrossRef]
- Ueno, A.; Masugi, Y.; Yamazaki, K.; Komuta, M.; Effendi, K.; Tanami, Y.; Tsujikawa, H.; Tanimoto, A.; Okuda, S.; Itano, O.; et al. OATP1B3 expression is strongly associated with Wnt/beta-catenin signalling and represents the transporter of gadoxetic acid in hepatocellular carcinoma. J. Hepatol. 2014, 61, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M. Gd-EOB-DTPA-MRI Could Predict WNT/beta-Catenin Mutation and Resistance to Immune Checkpoint Inhibitor Therapy in Hepatocellular Carcinoma. Liver Cancer 2020, 9, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Narita, M.; Hatano, E.; Arizono, S.; Miyagawa-Hayashino, A.; Isoda, H.; Kitamura, K.; Taura, K.; Yasuchika, K.; Nitta, T.; Ikai, I.; et al. Expression of OATP1B3 determines uptake of Gd-EOB-DTPA in hepatocellular carcinoma. J. Gastroenterol. 2009, 44, 793–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitao, A.; Zen, Y.; Matsui, O.; Gabata, T.; Kobayashi, S.; Koda, W.; Kozaka, K.; Yoneda, N.; Yamashita, T.; Kaneko, S.; et al. Hepatocellular carcinoma: Signal intensity at gadoxetic acid-enhanced MR Imaging—correlation with molecular transporters and histopathologic features. Radiology 2010, 256, 817–826. [Google Scholar] [CrossRef] [Green Version]
- Kitao, A.; Matsui, O.; Yoneda, N.; Kozaka, K.; Kobayashi, S.; Koda, W.; Gabata, T.; Yamashita, T.; Kaneko, S.; Nakanuma, Y.; et al. Hypervascular hepatocellular carcinoma: Correlation between biologic features and signal intensity on gadoxetic acid-enhanced MR images. Radiology 2012, 265, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Tsuboyama, T.; Onishi, H.; Kim, T.; Akita, H.; Hori, M.; Tatsumi, M.; Nakamoto, A.; Nagano, H.; Matsuura, N.; Wakasa, K.; et al. Hepatocellular carcinoma: Hepatocyte-selective enhancement at gadoxetic acid-enhanced MR imaging--correlation with expression of sinusoidal and canalicular transporters and bile accumulation. Radiology 2010, 255, 824–833. [Google Scholar] [CrossRef]
- Chen, V.L.; Xu, D.; Wicha, M.S.; Lok, A.S.; Parikh, N.D. Utility of Liquid Biopsy Analysis in Detection of Hepatocellular Carcinoma, Determination of Prognosis, and Disease Monitoring: A Systematic Review. Clin. Gastroenterol. Hepatol. 2020, 18, 2879–2902.e2879. [Google Scholar] [CrossRef]
- Cai, Z.; Chen, G.; Zeng, Y.; Dong, X.; Li, Z.; Huang, Y.; Xin, F.; Qiu, L.; Xu, H.; Zhang, W.; et al. Comprehensive Liquid Profiling of Circulating Tumor DNA and Protein Biomarkers in Long-Term Follow-Up Patients with Hepatocellular Carcinoma. Clin. Cancer Res. 2019, 25, 5284–5294. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Matsui, J.; Matsushima, T.; Obaishi, H.; Miyazaki, K.; Nakamura, K.; Tohyama, O.; Semba, T.; Yamaguchi, A.; Hoshi, S.S.; et al. Lenvatinib, an angiogenesis inhibitor targeting VEGFR/FGFR, shows broad antitumor activity in human tumor xenograft models associated with microvessel density and pericyte coverage. Vasc. Cell 2014, 6, 18. [Google Scholar] [CrossRef] [Green Version]
- Eso, Y.; Marusawa, H. Novel approaches for molecular targeted therapy against hepatocellular carcinoma. Hepatol. Res. 2018, 48, 597–607. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Sho, T.; Suda, G.; Ogawa, K.; Shigesawa, T.; Suzuki, K.; Nakamura, A.; Ohara, M.; Umemura, M.; Kawagishi, N.; Natsuizaka, M.; et al. Lenvatinib in patients with unresectable hepatocellular carcinoma who do not meet the REFLECT trial eligibility criteria. Hepatol. Res. 2020, 50, 966–977. [Google Scholar] [CrossRef] [PubMed]
- Sho, T.; Suda, G.; Ogawa, K.; Kimura, M.; Shimazaki, T.; Maehara, O.; Shigesawa, T.; Suzuki, K.; Nakamura, A.; Ohara, M.; et al. Early response and safety of lenvatinib for patients with advanced hepatocellular carcinoma in a real-world setting. JGH Open 2020, 4, 54–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoshida, Y.; Nijman, S.M.; Kobayashi, M.; Chan, J.A.; Brunet, J.P.; Chiang, D.Y.; Villanueva, A.; Newell, P.; Ikeda, K.; Hashimoto, M.; et al. Integrative transcriptome analysis reveals common molecular subclasses of human hepatocellular carcinoma. Cancer Res. 2009, 69, 7385–7392. [Google Scholar] [CrossRef] [Green Version]
- Calderaro, J.; Couchy, G.; Imbeaud, S.; Amaddeo, G.; Letouze, E.; Blanc, J.F.; Laurent, C.; Hajji, Y.; Azoulay, D.; Bioulac-Sage, P.; et al. Histological subtypes of hepatocellular carcinoma are related to gene mutations and molecular tumour classification. J. Hepatol. 2017, 67, 727–738. [Google Scholar] [CrossRef]
- Llovet, J.M.; Montal, R.; Sia, D.; Finn, R.S. Molecular therapies and precision medicine for hepatocellular carcinoma. Nat. Rev. Clin. Oncol. 2018, 15, 599–616. [Google Scholar] [CrossRef]
- Sia, D.; Jiao, Y.; Martinez-Quetglas, I.; Kuchuk, O.; Villacorta-Martin, C.; Castro de Moura, M.; Putra, J.; Camprecios, G.; Bassaganyas, L.; Akers, N.; et al. Identification of an Immune-specific Class of Hepatocellular Carcinoma, Based on Molecular Features. Gastroenterology 2017, 153, 812–826. [Google Scholar] [CrossRef] [Green Version]
- Zucman-Rossi, J.; Villanueva, A.; Nault, J.C.; Llovet, J.M. Genetic Landscape and Biomarkers of Hepatocellular Carcinoma. Gastroenterology 2015, 149, 1226–1239.e1224. [Google Scholar] [CrossRef] [Green Version]
- Jiao, J.; Watt, G.P.; Stevenson, H.L.; Calderone, T.L.; Fisher-Hoch, S.P.; Ye, Y.; Wu, X.; Vierling, J.M.; Beretta, L. Telomerase reverse transcriptase mutations in plasma DNA in patients with hepatocellular carcinoma or cirrhosis: Prevalence and risk factors. Hepatol. Commun. 2018, 2, 718–731. [Google Scholar] [CrossRef]
- Xu, R.H.; Wei, W.; Krawczyk, M.; Wang, W.; Luo, H.; Flagg, K.; Yi, S.; Shi, W.; Quan, Q.; Li, K.; et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat. Mater. 2017, 16, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Dhayat, S.A.; Yang, Z. Impact of circulating tumor DNA in hepatocellular and pancreatic carcinomas. J. Cancer Res. Clin. Oncol. 2020, 146, 1625–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimoto, A.; Totoki, Y.; Abe, T.; Boroevich, K.A.; Hosoda, F.; Nguyen, H.H.; Aoki, M.; Hosono, N.; Kubo, M.; Miya, F.; et al. Whole-genome sequencing of liver cancers identifies etiological influences on mutation patterns and recurrent mutations in chromatin regulators. Nat. Genet. 2012, 44, 760–764. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, H.; Shibata, T. Comprehensive genome sequencing of the liver cancer genome. Cancer Lett. 2013, 340, 234–240. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Patients with HCC Treated by Lenvatinib (n = 52) | Green Hepatoma (n = 7) | Green Hepatoma (−) (n = 45) | p-Value |
|---|---|---|---|---|
| Baseline characteristics | ||||
| Age (yr) | 70 (45–83) | 70 (55–79) | 71 (45–83) | 0.9357 |
| Sex (Male/Female) | 46/6 | 7/0 | 39/6 | 0.3043 |
| Etiology, No. (%) | ||||
| HBV | 14 (26.9%) | 0 (0%) | 14 (31.1%) | 0.0702 |
| HCV | 8 (15.3%) | 1 (14.3%) | 7 (15.5%) | 0.9310 |
| NBNC | 30 (57.6%) | 6 (85.7%) | 24 (53.3%) | 0.0864 |
| Vascular invasion, No. (%) | 16 (30.7%) | 0 (0.0%) | 16 (35.5%) | 0.1006 |
| Extrahepatic extension, No. (%) | 16 (30.7%) | 0 (0.0%) | 16 (35.5%) | 0.0580 |
| BCLC stage, No. (%) | ||||
| B | 27 (51.9%) | 5 (71.4%) | 22 (48.8%) | 0.2669 |
| C | 25 (48.0%) | 2 (28.6.%) | 23 (51.1%) | |
| Child–Pugh class, No. (%) | ||||
| A | 41 (78.8%) | 4 (57.1%) | 37 (82.2%) | 0.1307 |
| B | 11 (21.1%) | 3 (42.8%) | 8 (17.7%) | |
| Biochemical analysis | ||||
| Albumin, g/dL | 3.7 (2.8–4.6) | 3.2 (2.9–4.6) | 3.8 (2.8–4.6) | 0.4354 |
| Total bilirubin, mg/dL | 0.7 (0.3–3.1) | 1.2 (0.9–3.1) | 0.7 (0.3–1.9) | 0.0197 |
| Prothrombin time, % | 88.3 (40.7–117.7) | 83.9 (46.6–107.6) | 88.4 (40.7–117.7) | 0.1637 |
| Platelet, ×104/μL | 16.1 (4.4–51.7) | 13.4 (4.4–51.7) | 17.3 (6.5–51.7) | 0.4448 |
| Alpha-fetoprotein, ng/mL | 78.3 (2.0–449,909) | 2.2 (2.2–852.5) | 78.3 (2.0–449,909) | 0.4759 |
| AFP, L3% | 19.2 (0–99.5) | 41.1 (0.5–80.4) | 19.2 (0–99.5) | 0.4273 |
| PIVKA-II, mAU/mL | 345 (13–93,644) | 266 (26–29,756) | 381 (13–93,644) | 0.3961 |
| RER | 0.785 (0.446–1.446) | 1.110 (1.018–1.446) | 0.7526 (0.446–0.969) | <0.001 |
| Pt No. | Age (years) | Sex | HCCs in Liver (n) | Green Hepatoma (n) | Size of Green Hepatoma (mm) | RER (Median) | Etiology |
|---|---|---|---|---|---|---|---|
| 1 | 55 | M | 6 | 3 | 12.6, 33.3, 32.5 | 1.155 | HCV |
| 2 | 79 | M | 5 | 2 | 11.1, 19.1 | 1.174 | NBNC |
| 3 | 70 | M | 3 | 2 | 16.6, 39.1 | 1.191 | NBNC |
| 4 | 73 | M | 3 | 1 | 10 | 1.073 | NBNC |
| 5 | 67 | M | 4 | 1 | 18.4 | 1.085 | NBNC |
| 6 | 83 | M | 5 | 1 | 19.8 | 1.105 | NBNC |
| 7 | 57 | M | 4 | 1 | 23.6 | 1.004 | NBNC |
| Treatment Response | Green Hepatoma | Green Hepatoma (−) | p-Value |
|---|---|---|---|
| n = 7 | n = 45 | ||
| CR/PR/SD/PD | 0/3/4/0 | 4/19/16/6 | 0.5087 |
| ORR | 3 (42.8%) | 22 (48.8%) | 0.5901 |
| DCR | 7 (100%) | 39(86.6%) | 0.3416 |
| Case | Green Hepatoma | Age (Years) | Sex | Etiology | Child–Pugh | BCLC | CTNNB-1 | Mutation |
|---|---|---|---|---|---|---|---|---|
| 1 | + | 70 | M | NBNC | 6 | B | positive | T41AS45F |
| 2 | + | 72 | M | NBNC | 6 | B | positive | T41A |
| 3 | + | 83 | M | NBNC | 6 | B | negative | |
| 4 | − | 70 | M | NBNC | 5 | B | negative | |
| 5 | − | 62 | M | NBNC | 6 | B | negative | |
| 6 | − | 70 | M | NBNC | 7 | B | negative | |
| 7 | − | 70 | F | NBNC | 5 | B | negative |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kubo, A.; Suda, G.; Kimura, M.; Maehara, O.; Tokuchi, Y.; Kitagataya, T.; Ohara, M.; Yamada, R.; Shigesawa, T.; Suzuki, K.; et al. Characteristics and Lenvatinib Treatment Response of Unresectable Hepatocellular Carcinoma with Iso-High Intensity in the Hepatobiliary Phase of EOB-MRI. Cancers 2021, 13, 3633. https://doi.org/10.3390/cancers13143633
Kubo A, Suda G, Kimura M, Maehara O, Tokuchi Y, Kitagataya T, Ohara M, Yamada R, Shigesawa T, Suzuki K, et al. Characteristics and Lenvatinib Treatment Response of Unresectable Hepatocellular Carcinoma with Iso-High Intensity in the Hepatobiliary Phase of EOB-MRI. Cancers. 2021; 13(14):3633. https://doi.org/10.3390/cancers13143633
Chicago/Turabian StyleKubo, Akinori, Goki Suda, Megumi Kimura, Osamu Maehara, Yoshimasa Tokuchi, Takashi Kitagataya, Masatsugu Ohara, Ren Yamada, Taku Shigesawa, Kazuharu Suzuki, and et al. 2021. "Characteristics and Lenvatinib Treatment Response of Unresectable Hepatocellular Carcinoma with Iso-High Intensity in the Hepatobiliary Phase of EOB-MRI" Cancers 13, no. 14: 3633. https://doi.org/10.3390/cancers13143633