
Etiology and Outcomes of Hepatocellular Carcinoma in an Ethnically Diverse Population: The Multiethnic Cohort

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. HCC Identification and Tumor Characteristics
2.3. Statistical Analysis
3. Results
3.1. Cohort Characteristics by Race/Ethnicity
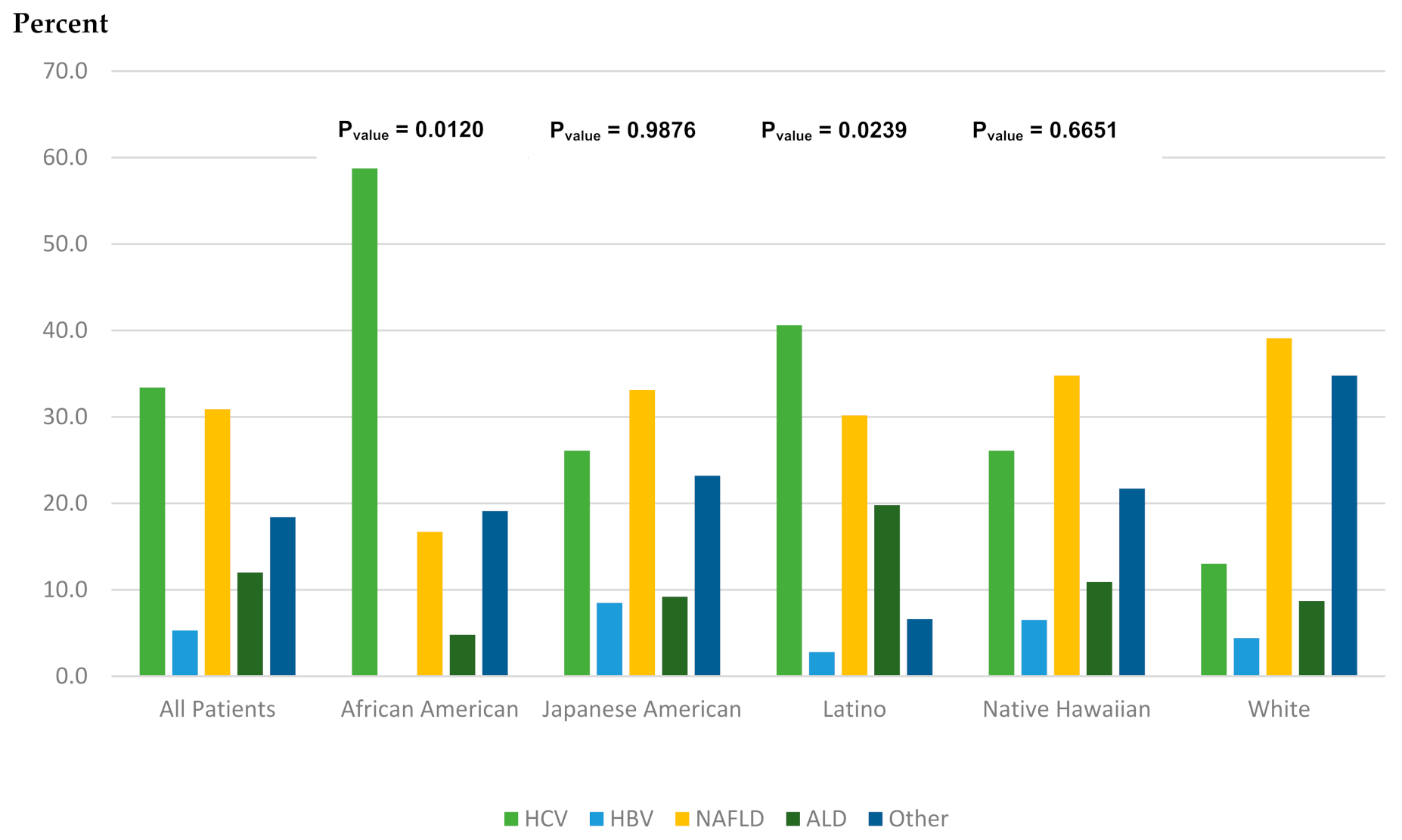
3.2. HCC Characteristics and Underlying Etiology by Race/Ethnicity
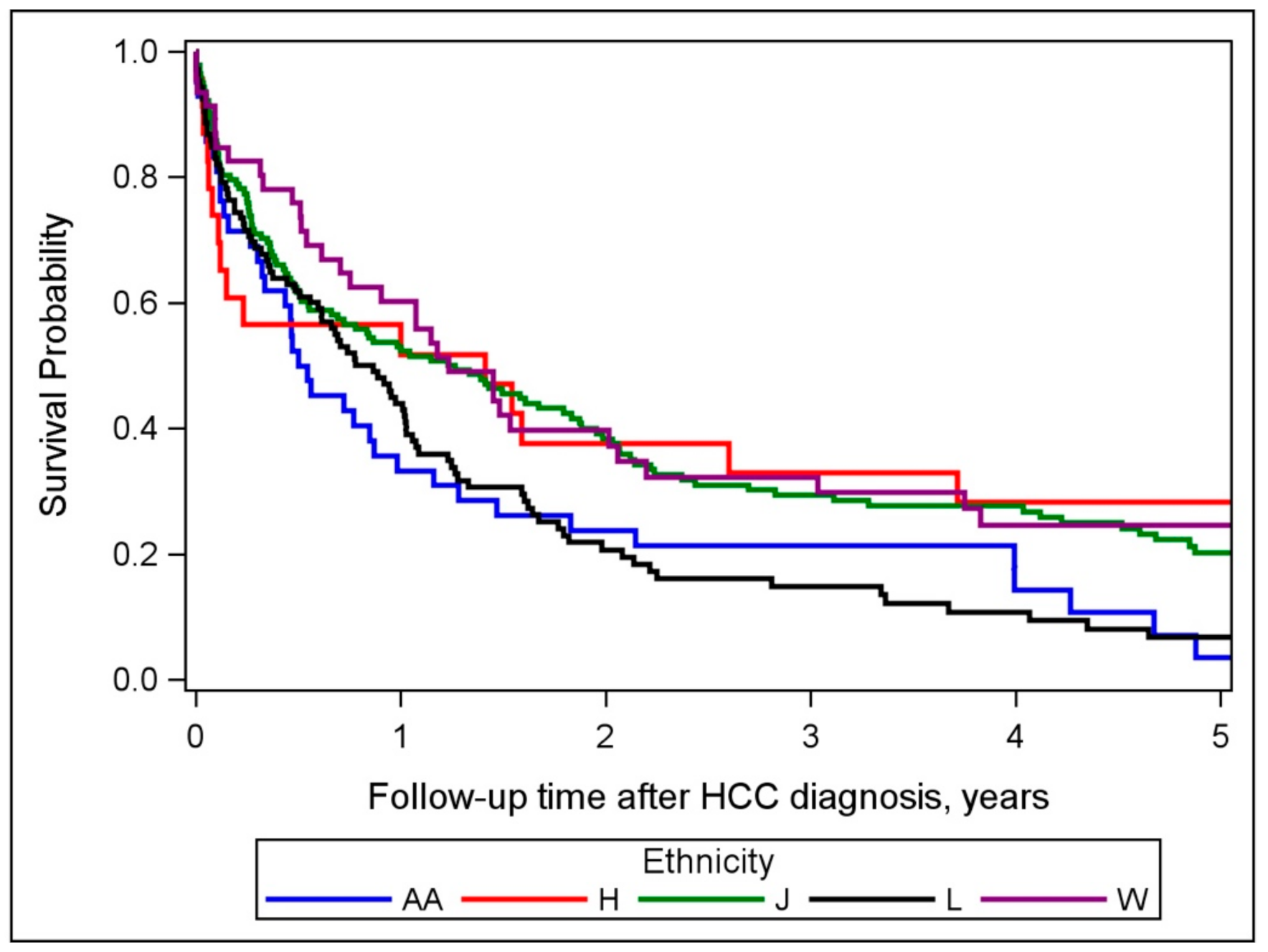
3.3. Relationship between Race/Ethnicity, Risk Factor, and Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Akinyemiju, T.; Abera, S.; Ahmed, M.; Alam, N.; Alemayohu, M.A.; Allen, C.; Al-Raddadi, R.; Alvis-Guzman, N.; Amoako, Y.; Global Burden of Disease Liver Cancer Collaboration; et al. The Burden of Primary Liver Cancer and Underlying Etiologies From 1990 to 2015 at the Global, Regional, and National Level: Results From the Global Burden of Disease Study 2015. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Hashim, D.; Boffetta, P.; La Vecchia, C.; Rota, M.; Bertuccio, P.; Malvezzi, M.; Negri, E. The global decrease in cancer mortality: Trends and disparities. Ann. Oncol. 2016, 27, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Pham, C.; Fong, T.L.; Zhang, J.; Liu, L. Striking Racial/Ethnic Disparities in Liver Cancer Incidence Rates and Temporal Trends in California, 1988–2012. J. Natl. Cancer Inst. 2018, 110, 1259–1269. [Google Scholar] [CrossRef] [PubMed]
- Ryerson, A.B.; Eheman, C.R.; Altekruse, S.F.; Ward, J.W.; Jemal, A.; Sherman, R.L.; Henley, S.J.; Holtzman, D.; Lake, A.; Noone, A.M.; et al. Annual Report to the Nation on the Status of Cancer, 1975–2012, featuring the increasing incidence of liver cancer. Cancer 2016, 122, 1312–1337. [Google Scholar] [CrossRef] [PubMed]
- Tapper, E.B.; Parikh, N.D. Mortality due to cirrhosis and liver cancer in the United States, 1999–2016: Observational study. BMJ 2018, 362, k2817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, S.L.; Kwong, S.L.; Bowlus, C.L.; Nguyen, T.T.; Maxwell, A.E.; Bastani, R.; Chak, E.W.; Chen, M.S., Jr. Racial/ethnic disparities in hepatocellular carcinoma treatment and survival in California, 1988-2012. World J. Gastroenterol. 2016, 22, 8584–8595. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Liu, J.B.; So, S.K.; Han, S.S.; Wang, S.S.; Hertz, A.; Shariff-Marco, S.; Lin Gomez, S.; Rosenberg, P.S.; Nguyen, M.H.; et al. Disparities in hepatocellular carcinoma incidence by race/ethnicity and geographic area in California: Implications for prevention. Cancer 2018, 124, 3551–3559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Setiawan, V.W.; Hernandez, B.Y.; Lu, S.C.; Stram, D.O.; Wilkens, L.R.; Le Marchand, L.; Henderson, B.E. Diabetes and racial/ethnic differences in hepatocellular carcinoma risk: The multiethnic cohort. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolonel, L.N.; Henderson, B.E.; Hankin, J.H.; Nomura, A.M.; Wilkens, L.R.; Pike, M.C.; Stram, D.O.; Monroe, K.R.; Earle, M.E.; Nagamine, F.S. A multiethnic cohort in Hawaii and Los Angeles: Baseline characteristics. Am. J. Epidemiol. 2000, 151, 346–357. [Google Scholar] [CrossRef] [PubMed]
- Artinyan, A.; Mailey, B.; Sanchez-Luege, N.; Khalili, J.; Sun, C.L.; Bhatia, S.; Wagman, L.D.; Nissen, N.; Colquhoun, S.D.; Kim, J. Race, ethnicity, and socioeconomic status influence the survival of patients with hepatocellular carcinoma in the United States. Cancer 2010, 116, 1367–1377. [Google Scholar] [CrossRef]
- Mathur, A.K.; Osborne, N.H.; Lynch, R.J.; Ghaferi, A.A.; Dimick, J.B.; Sonnenday, C.J. Racial/ethnic disparities in access to care and survival for patients with early-stage hepatocellular carcinoma. Arch. Surg. 2010, 145, 1158–1163. [Google Scholar] [CrossRef] [Green Version]
- Rich, N.E.; Hester, C.; Odewole, M.; Murphy, C.C.; Parikh, N.D.; Marrero, J.A.; Yopp, A.C.; Singal, A.G. Racial and Ethnic Differences in Presentation and Outcomes of Hepatocellular Carcinoma. Clin. Gastroenterol. Hepatol. 2019, 17, 551–559. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.D.; Diaz, C.; Wang, D.; Gonzalez-Diaz, J.; Martin, P.; Kobetz, E. The Impact of Race on Survival After Hepatocellular Carcinoma in a Diverse American Population. Dig. Dis. Sci. 2018, 63, 515–528. [Google Scholar] [CrossRef]
- Younossi, Z.; Stepanova, M.; Ong, J.P.; Jacobson, I.M.; Bugianesi, E.; Duseja, A.; Eguchi, Y.; Wong, V.W.; Negro, F.; Yilmaz, Y.; et al. Nonalcoholic Steatohepatitis Is the Fastest Growing Cause of Hepatocellular Carcinoma in Liver Transplant Candidates. Clin. Gastroenterol. Hepatol. 2019, 17, 748–755 e743. [Google Scholar] [CrossRef] [Green Version]
- McGlynn, K.A.; Petrick, J.L.; London, W.T. Global epidemiology of hepatocellular carcinoma: An emphasis on demographic and regional variability. Clin. Liver Dis. 2015, 19, 223–238. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, P.S.; Medina, H.N.; Callahan, K.E.; Jones, P.D.; Brown, C.P.; Altekruse, S.F.; McGlynn, K.A.; Kobetz, E.N. The association between etiology of hepatocellular carcinoma and race-ethnicity in Florida. Liver Int. 2020, 40, 1201–1210. [Google Scholar] [CrossRef]
- Kowdley, K.V.; Wang, C.C.; Welch, S.; Roberts, H.; Brosgart, C.L. Prevalence of chronic hepatitis B among foreign-born persons living in the United States by country of origin. Hepatology 2012, 56, 422–433. [Google Scholar] [CrossRef]
- Yatsuhashi, H. Past, Present, and Future of Viral Hepatitis C in Japan. Euroasian J. Hepatogastroenterol. 2016, 6, 49–51. [Google Scholar] [CrossRef] [Green Version]
- Hall, E.W.; Rosenberg, E.S.; Sullivan, P.S. Estimates of state-level chronic hepatitis C virus infection, stratified by race and sex, United States, 2010. BMC Infect. Dis. 2018, 18, 224. [Google Scholar] [CrossRef]
- Hester, D.; Golabi, P.; Paik, J.; Younossi, I.; Mishra, A.; Younossi, Z.M. Among Medicare Patients With Hepatocellular Carcinoma, Non-alcoholic Fatty Liver Disease is the Most Common Etiology and Cause of Mortality. J. Clin. Gastroenterol. 2019. [Google Scholar] [CrossRef]
- Chang, E.T.; Yang, J.; Alfaro-Velcamp, T.; So, S.K.; Glaser, S.L.; Gomez, S.L. Disparities in liver cancer incidence by nativity, acculturation, and socioeconomic status in California Hispanics and Asians. Cancer Epidemiol. Prev. Biomark. 2010, 19, 3106–3118. [Google Scholar] [CrossRef] [Green Version]
- Rich, N.E.; Oji, S.; Mufti, A.R.; Browning, J.D.; Parikh, N.D.; Odewole, M.; Mayo, H.; Singal, A.G. Racial and Ethnic Disparities in Nonalcoholic Fatty Liver Disease Prevalence, Severity, and Outcomes in the United States: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 198–210. [Google Scholar] [CrossRef] [Green Version]
- Setiawan, V.W.; Stram, D.O.; Porcel, J.; Lu, S.C.; Le Marchand, L.; Noureddin, M. Prevalence of chronic liver disease and cirrhosis by underlying cause in understudied ethnic groups: The multiethnic cohort. Hepatology 2016, 64, 1969–1977. [Google Scholar] [CrossRef] [Green Version]
- Beste, L.A.; Leipertz, S.L.; Green, P.K.; Dominitz, J.A.; Ross, D.; Ioannou, G.N. Trends in Burden of Cirrhosis and Hepatocellular Carcinoma by Underlying Liver Disease in US Veterans, 2001–2013. Gastroenterology 2015, 149, 1471–1482. [Google Scholar] [CrossRef] [Green Version]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J.; American Gastroenterological, A.; American Association for the Study of Liver, D.; et al. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012, 142, 1592–1609. [Google Scholar] [CrossRef] [Green Version]
- Li, W.Q.; Park, Y.; McGlynn, K.A.; Hollenbeck, A.R.; Taylor, P.R.; Goldstein, A.M.; Freedman, N.D. Index-based dietary patterns and risk of incident hepatocellular carcinoma and mortality from chronic liver disease in a prospective study. Hepatology 2014, 60, 588–597. [Google Scholar] [CrossRef] [Green Version]
- Bogumil, D.; Park, S.Y.; Le Marchand, L.; Haiman, C.A.; Wilkens, L.R.; Boushey, C.J.; Setiawan, V.W. High-Quality Diets Are Associated With Reduced Risk of Hepatocellular Carcinoma and Chronic Liver Disease: The Multiethnic Cohort. Hepatol. Commun. 2019, 3, 437–447. [Google Scholar] [CrossRef] [Green Version]
- Setiawan, V.W.; Stram, D.O.; Porcel, J.; Chari, S.T.; Maskarinec, G.; Le Marchand, L.; Wilkens, L.R.; Haiman, C.A.; Pandol, S.J.; Monroe, K.R. Pancreatic Cancer Following Incident Diabetes in African Americans and Latinos: The Multiethnic Cohort. J. Natl. Cancer Inst. 2019, 111, 27–33. [Google Scholar] [CrossRef]
- Ha, J.; Yan, M.; Aguilar, M.; Bhuket, T.; Tana, M.M.; Liu, B.; Gish, R.G.; Wong, R.J. Race/ethnicity-specific disparities in cancer incidence, burden of disease, and overall survival among patients with hepatocellular carcinoma in the United States. Cancer 2016, 122, 2512–2523. [Google Scholar] [CrossRef]
- Brar, G.; Greten, T.F.; Graubard, B.I.; McNeel, T.S.; Petrick, J.L.; McGlynn, K.A.; Altekruse, S.F. Hepatocellular Carcinoma Survival by Etiology: A SEER-Medicare Database Analysis. Hepatol. Commun. 2020, 4, 1541–1551. [Google Scholar] [CrossRef]
- Desai, A.; Sandhu, S.; Lai, J.P.; Sandhu, D.S. Hepatocellular carcinoma in non-cirrhotic liver: A comprehensive review. World J. Hepatol. 2019, 11, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Jemal, A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950–2014: Over Six Decades of Changing Patterns and Widening Inequalities. J. Environ. Public Health 2017, 2017, 2819372. [Google Scholar] [CrossRef] [PubMed]
- Halbert, C.H.; Weathers, B.; Delmoor, E.; Mahler, B.; Coyne, J.; Thompson, H.S.; Have, T.T.; Vaughn, D.; Malkowicz, S.B.; Lee, D. Racial differences in medical mistrust among men diagnosed with prostate cancer. Cancer 2009, 115, 2553–2561. [Google Scholar] [CrossRef] [PubMed]
- Penner, L.A.; Dovidio, J.F.; Gonzalez, R.; Albrecht, T.L.; Chapman, R.; Foster, T.; Harper, F.W.; Hagiwara, N.; Hamel, L.M.; Shields, A.F.; et al. The Effects of Oncologist Implicit Racial Bias in Racially Discordant Oncology Interactions. J. Clin. Oncol 2016, 34, 2874–2880. [Google Scholar] [CrossRef]
- Lin, Y.J.; Lin, C.N.; Sedghi, T.; Hsu, S.H.; Gross, C.P.; Wang, J.D.; Wang, S.Y. Treatment patterns and survival in hepatocellular carcinoma in the United States and Taiwan. PLoS ONE 2020, 15, e0240542. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | All Patients (N = 359) | African American (N = 42) | Japanese American (N = 142) | Latino (N = 106) | White (N = 46) | Native Hawaiian (N = 23) |
|---|---|---|---|---|---|---|
| Mean age at enrollment (SD), years | 61.5 ± 7.43 | 64.1 ± 7.65 | 62.5 ± 7.75 | 60.2 ± 5.94 | 59.6 ± 7.91 | 60.7 ± 8.61 |
| Sex (%) | ||||||
| Male | 235 (65.5) | 27 (64.3) | 71 (62.0) | 88 (67.0) | 32 (69.6) | 17 (73.9) |
| Female | 124 (34.5) | 15 (35.7) | 54 (38.0) | 35 (33.0) | 14 (30.4) | 6 (26.1) |
| BMI category (%) | ||||||
| <25.0 kg/m2 | 106 (29.5) | 12 (28.6) | 57 (40.1) | 19 (17.9) | 12 (26.1) | 17 (26.1) |
| 25.0–30.0 kg/m2 | 155 (43.2) | 19 (45.2) | 58 (40.9) | 51 (48.1) | 17 (37.0) | 10 (43.5) |
| ≥30.0 kg/m2 | 95 (26.5) | 9 (21.4) | 26 (18.3) | 36 (34.0) | 17 (37.0) | 7 (30.4) |
| Unknown | 3 (0.8) | 2 (4.8) | 1 (0.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Smoking status (%) | ||||||
| Never smoker | 96 (26.7) | 8 (19.1) | 38 (26.8) | 35 (33.0) | 12 (26.1) | 3 (13.0) |
| Ever smoker | 255 (71.1) | 34 (80.9) | 104 (73.2) | 66 (62.3) | 33 (71.7) | 18 (78.3) |
| Unknown | 8 (2.2) | 0 (0.0) | 0 (0.0) | 5 (4.7) | 1 (2.2) | 2 (8.7) |
| Education (%) | ||||||
| High school graduate or less | 170 (47.4) | 20 (47.6) | 58 (40.9) | 72 (67.9) | 10 (21.7) | 10 (43.5) |
| Some college/technical school | 112 (31.2) | 15 (35.7) | 47 (33.1) | 21 (19.8) | 20 (43.5) | 9 (39.1) |
| College graduate | 35 (9.8) | 5 (11.9) | 15 (10.6) | 5 (4.7) | 8 (17.4) | 2 (8.7) |
| Graduate/professional school | 34 (9.5) | 2 (4.8) | 21 (14.8) | 3 (2.8) | 7 (15.2) | 1 (4.4) |
| Unknown | 8 (2.2) | 0 (0.0) | 1 (0.7) | 5 (4.7) | 1 (2.2) | 1 (4.4) |
| Alcohol Intake (%) | ||||||
| 0 | 176 (49.0) | 19 (45.2) | 82 (57.8) | 49 (46.2) | 18 (39.1) | 8 (34.8) |
| <12 g/day | 83 (23.1) | 11 (26.2) | 30 (21.1) | 28 (26.4) | 12 (26.1) | 2 (8.7) |
| ≥12 g/day | 84 (23.4) | 11 (26.2) | 24 (16.9) | 23 (21.7) | 14 (30.4) | 12 (52.2) |
| Missing | 16 (4.5) | 1 (2.4) | 6 (4.2) | 6 (5.7) | 2 (4.4) | 1 (4.4) |
| Diabetes mellitus (%) | 223 (62.1) | 21 (50.0) | 89 (62.7) | 79 (74.5) | 22 (47.8) | 12 (52.2) |
| Healthy Eating Index 2010 | ||||||
| Median (range) | 64.5 (32.1–93.7) | 66.5 (32.1–85.6) | 64.6 (34.6–86.8) | 62.8 (45.0–92.3) | 69.5 (41.0–93.7) | 67.8 (51.0–78.8) |
| Characteristics | All Patients (N = 359) | African American (N = 42) | Japanese American (N = 142) | Latino (N = 106) | White (N = 46) | Native Hawaiian (N = 23) |
|---|---|---|---|---|---|---|
| Mean age at diagnosis (SD), years | 75.1 ± 7.16 | 76.7 ± 8.26 | 76.2 ± 7.40 | 74.0 ± 5.86 | 72.9 ± 7.27 | 74.7 ± 7.47 |
| Median follow-up time *, months | 10.6 | 6.4 | 12.4 | 8.8 | 14.7 | 12.2 |
| Stage at diagnosis (%) | ||||||
| Localized | 169 (47.1) | 18 (40.5) | 72 (50.7) | 51 (48.1) | 21 (45.7) | 8 (34.8) |
| Regional | 87 (24.2) | 11 (26.2) | 37 (26.1) | 24 (22.6) | 10 (21.7) | 5 (21.7) |
| Distant | 57 (15.9) | 7 (16.7) | 22 (15.5) | 15 (14.2) | 8 (17.4) | 5 (21.7) |
| Unknown | 46 (12.8) | 7 (16.7) | 11 (7.8) | 16 (15.1) | 7 (15.2) | 5 (21.7) |
| p-value ** | 0.7605 | 0.9495 | 0.4677 | 0.9645 | Reference | 0.7741 |
| Underlying Etiology | ||||||
| HCV | 120 (33.4) | 25 (59.5) | 37 (26.1) | 43 (40.6) | 12 (26.1) | 3 (13.0) |
| HBV | 19 (5.3) | 0 (0.0) | 12 (8.5) | 3 (2.8) | 3 (6.5) | 1 (4.4) |
| NAFLD | 111 (30.9) | 7 (16.7) | 47 (33.1) | 32 (30.2) | 16 (34.8) | 7 (39.1) |
| ALD | 43 (12.0) | 2 (4.8) | 13 (9.2) | 21 (19.8) | 5 (10.9) | 2 (8.7) |
| Other | 66 (18.4) | 8 (19.1) | 33 (23.2) | 7 (6.6) | 10 (21.7) | 8 (34.8) |
| p-value ** | <0.0001 | 0.0120 | 0.9876 | 0.0239 | Reference | 0.6651 |
| Treatment (%) | ||||||
| None | 119 (33.2) | 21 (50.0) | 37 (26.1) | 48 (45.3) | 7 (15.2) | 6 (26.1) |
| Treated | 218 (60.7) | 20 (47.6) | 97 (68.3) | 54 (50.9) | 33 (71.7) | 14 (60.9) |
| Unknown | 22 (6.1) | 1 (2.4) | 8 (5.6) | 4 (3.8) | 6 (13.0) | 3 (13.0) |
| p-value ** | 0.0005 | 0.0009 | 0.1128 | 0.0007 | Reference | 0.5387 |
| Conditions (%) *** | ||||||
| Yes | 51 (14.2) | 28 (4.8) | 21 (14.8) | 25 (23.6) | 1 (2.2) | 2 (8.7) |
| p-value ** | 0.0021 | 0.6039 | 0.0207 | 0.0013 | Reference | 0.2559 |
| Cause of death (%) | ||||||
| All death (n) | 295 | 38 | 111 | 93 | 35 | 18 |
| HCC-related | 213 (72.2) | 28 (73.7) | 77 (69.4) | 68 (73.1) | 25 (71.4) | 15 (83.3) |
| Liver-related | 22 (7.5) | 2 (5.3) | 6 (5.4) | 12 (12.9) | 2 (5.7) | 0 (0.0) |
| Non-liver-related | 58 (19.7) | 8 (21.1) | 27 (24.3) | 12 (12.9) | 8 (22.9) | 3 (16.7) |
| Unknown | 2 (0.7) | 0 (0.0) | 1 (0.9) | 1 (1.1) | 0 (0.0) | 0 (0.0) |
| No. Deaths | Univariate HR (95% CI) a | p-Value | Multivariate HR (95% CI) b | p-Value | |
|---|---|---|---|---|---|
| Race/ethnicity | |||||
| White | 35 | 1.00 | <0.0001 | 1.00 | 0.0067 |
| African American | 38 | 1.73 (1.08–2.78) | 1.87 (1.06–3.28) | ||
| Japanese American | 111 | 0.96 (0.65–1.41) | 1.02 (0.66–1.57) | ||
| Latino | 93 | 1.92 (1.29–2.85) | 1.47 (0.91–2.38) | ||
| Native Hawaiian | 18 | 0.75 (0.42–1.34) | 0.65 (0.34–1.23) | ||
| Sex | |||||
| Female | 105 | 1.00 | 0.5638 | ||
| Male | 190 | 1.08 (0.84–1.37) | |||
| Underlying etiology | |||||
| HCV | 96 | 1.00 | 0.0007 | 1.00 | 0.0030 |
| HBV | 14 | 0.90 (0.51–1.60) | 2.00 (1.03–3.86) | ||
| NAFLD | 90 | 1.53 (1.13–2.08) | 2.02 (1.40–2.91) | ||
| ALD | 40 | 2.11 (1.44–3.09) | 1.73 (1.11–2.72) | ||
| Other | 55 | 1.20 (0.86–1.68) | 1.32 (0.88–1.99) | ||
| Stage at diagnosis | |||||
| Localized | 121 | 1.00 | <0.0001 | 1.00 | <0.0001 |
| Regional | 76 | 2.33 (1.74–3.12) | 2.16 (1.57–2.98) | ||
| Distant | 56 | 3.79 (2.74–5.25) | 3.06 (2.13–4.39) | ||
| Unknown | 42 | 4.76 (3.29–6.87) | 1.76 (1.11–2.78) | ||
| First course of treatment | |||||
| None | 113 | 1.00 | <0.0001 | 1.00 | <0.0001 |
| Treated | 162 | 0.17 (0.13–0.22) | 0.22 (0.16–0.30) | ||
| Unknown | 20 | 1.04 (0.62–1.77) | 1.06 (0.57–1.99) | ||
| Smoking status | |||||
| Never smoker | 75 | 1.00 | 0.0238 | 1.00 | 0.0021 |
| Ever smoker | 213 | 1.45 (1.11–1.90) | 1.72 (1.26–2.33) | ||
| Unknown | 7 | 1.44 (0.66–3.15) | 0.98 (0.38–2.51) | ||
| Education | |||||
| High school graduate or less | 149 | 1.00 | 0.0072 | 1.00 | 0.1614 |
| Some college/technical school | 91 | 0.82 (0.63–1.07) | 0.72 (0.52–0.98) | ||
| College graduate | 26 | 0.90 (0.59–1.38) | 0.90 (0.55–1.47) | ||
| Graduate/professional school | 22 | 0.43 (0.27–0.68) | 0.63 (0.36–1.09) | ||
| Unknown | 7 | 1.04 (0.48–2.25) | 1.43 (0.51–3.99) | ||
| Alcohol intake | |||||
| 0 | 145 | 1.00 | 0.2200 | ||
| <12 g/day | 72 | 1.21 (0.91–1.62) | |||
| ≥12 g/day | 66 | 0.93 (0.69–1.25) | |||
| Unknown | 12 | 1.56 (0.85–2.87) | |||
| BMI category (kg/m2) | |||||
| <25.0 | 87 | 1.00 | <0.0001 | 1.00 | 0.0011 |
| 25.0–30.0 | 124 | 1.43 (1.08–1.89) | 0.98 (0.71–1.36) | ||
| ≥30.0 | 81 | 2.55 (1.86–3.49) | 1.89 (1.29–2.75) | ||
| Unknown | 3 | 1.69 (0.51–5.64) | 0.82 (0.22–3.04) | ||
| Diabetes mellitus | |||||
| No | 112 | 1.00 | 0.4653 | ||
| Yes | 183 | 1.09 (0.86–1.39) | |||
| Healthy Eating Index 2010 | 283 | 0.98 (0.97–0.995) | 0.0029 | 1.00 (0.99–1.02) | 0.5470 |
| Year of diagnosis | 295 | 1.04 (1.01–1.07) | 0.0056 | 0.98 (0.95–1.01) | 0.2508 |
| Conditions c | |||||
| No | 252 | 1.00 | 0.4104 | ||
| Yes | 43 | 1.15 (0.83–1.60) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barzi, A.; Zhou, K.; Wang, S.; Dodge, J.L.; El-Khoueiry, A.; Setiawan, V.W. Etiology and Outcomes of Hepatocellular Carcinoma in an Ethnically Diverse Population: The Multiethnic Cohort. Cancers 2021, 13, 3476. https://doi.org/10.3390/cancers13143476
Barzi A, Zhou K, Wang S, Dodge JL, El-Khoueiry A, Setiawan VW. Etiology and Outcomes of Hepatocellular Carcinoma in an Ethnically Diverse Population: The Multiethnic Cohort. Cancers. 2021; 13(14):3476. https://doi.org/10.3390/cancers13143476
Chicago/Turabian StyleBarzi, Afsaneh, Kali Zhou, Songren Wang, Jennifer L. Dodge, Anthony El-Khoueiry, and Veronica Wendy Setiawan. 2021. "Etiology and Outcomes of Hepatocellular Carcinoma in an Ethnically Diverse Population: The Multiethnic Cohort" Cancers 13, no. 14: 3476. https://doi.org/10.3390/cancers13143476