
Impact of Surgical Resection and Reasons for Poor Prognosis of Pelvic Osteosarcoma Based on the Bone Tumor Registry in Japan

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Statistical Analyses
3. Results
3.1. Patient and Treatment Demographics for Femoral and Pelvic Osteosarcoma
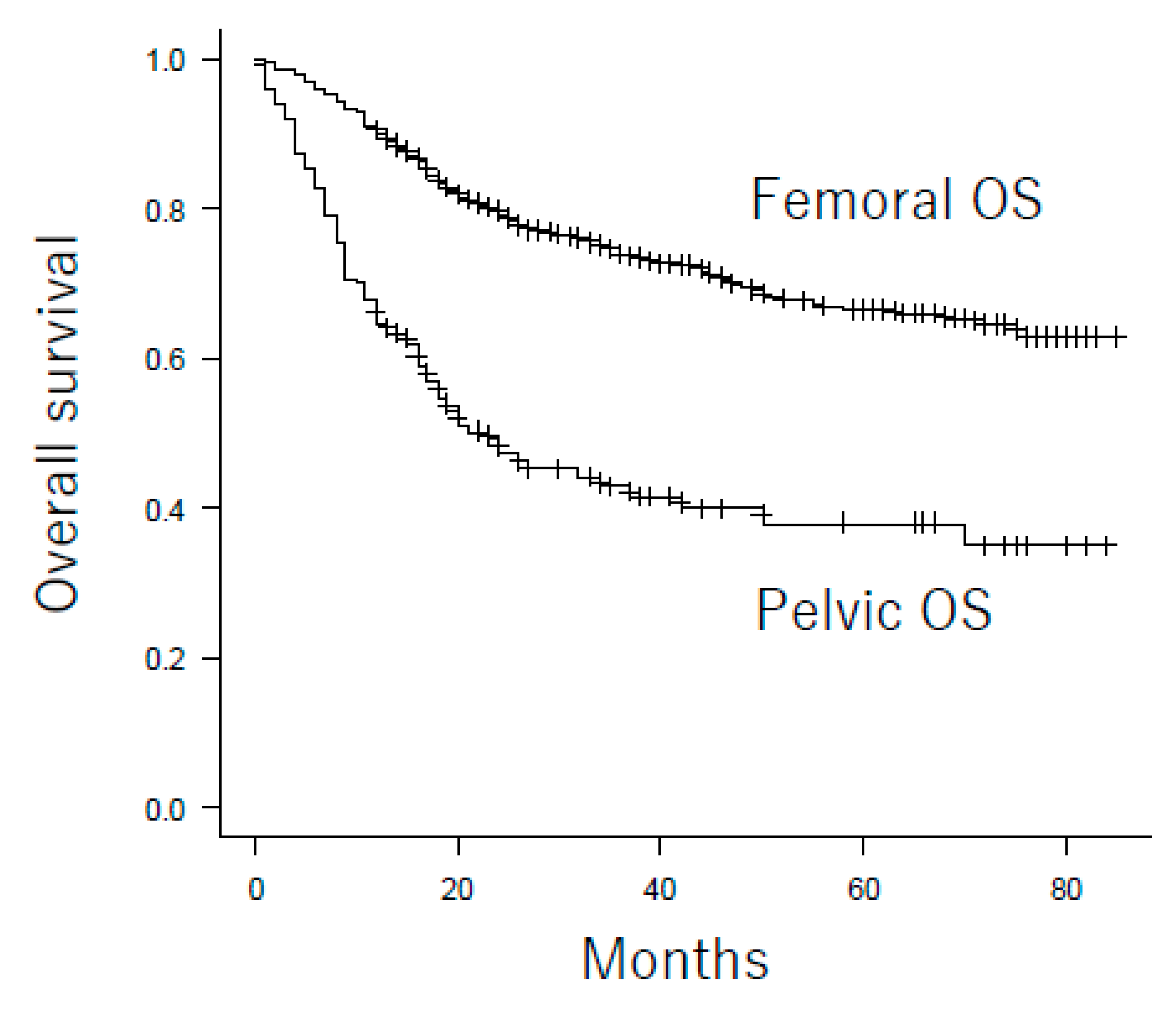
3.2. Overall Survival of Patients with Femoral and Pelvic Osteosarcoma
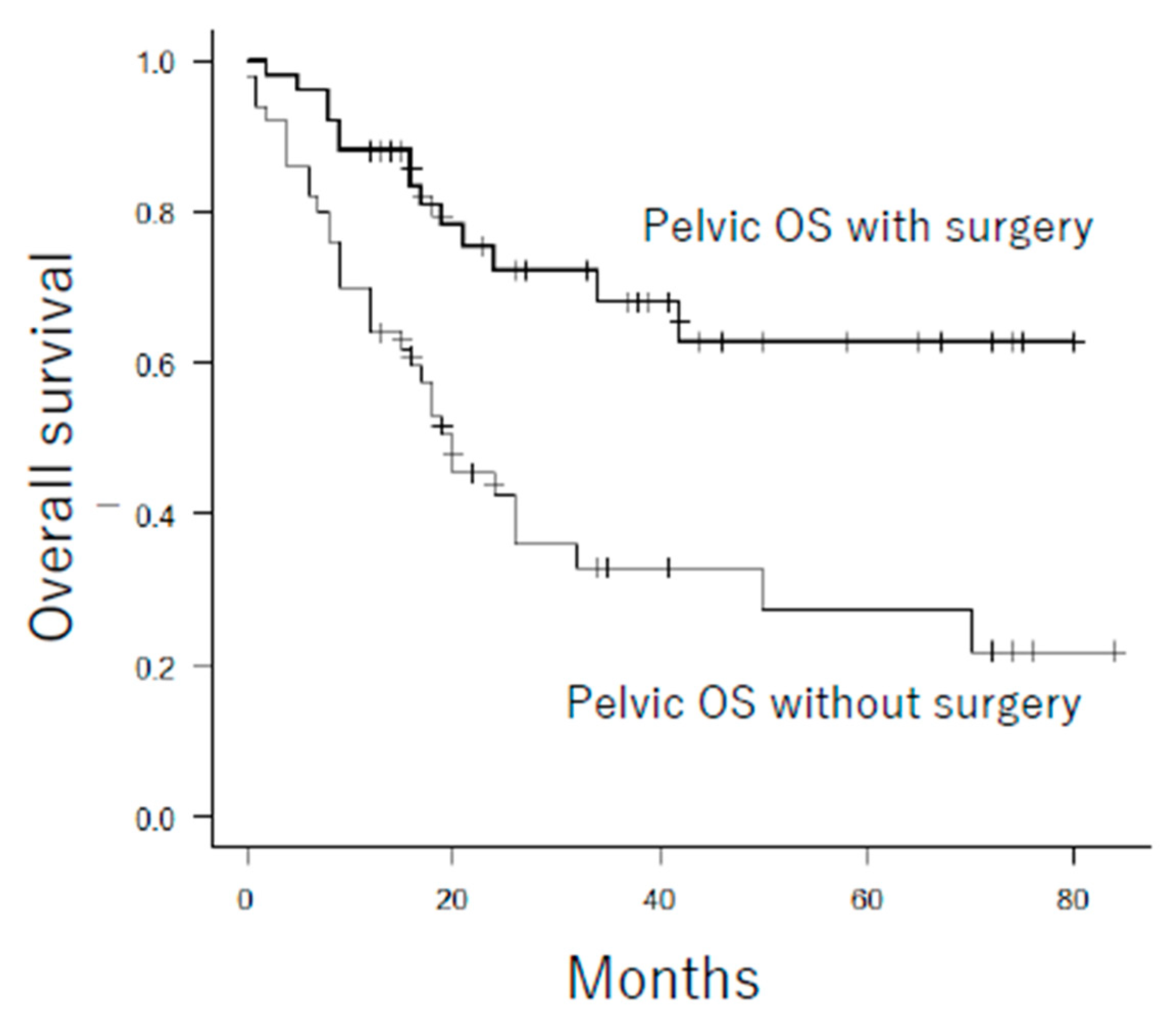
3.3. Characteristics of Pelvic Osteosarcoma Patients Treated with or without Surgical Resection
3.3.1. Propensity Score Analysis of Surgical Resection of Pelvic Osteosarcoma
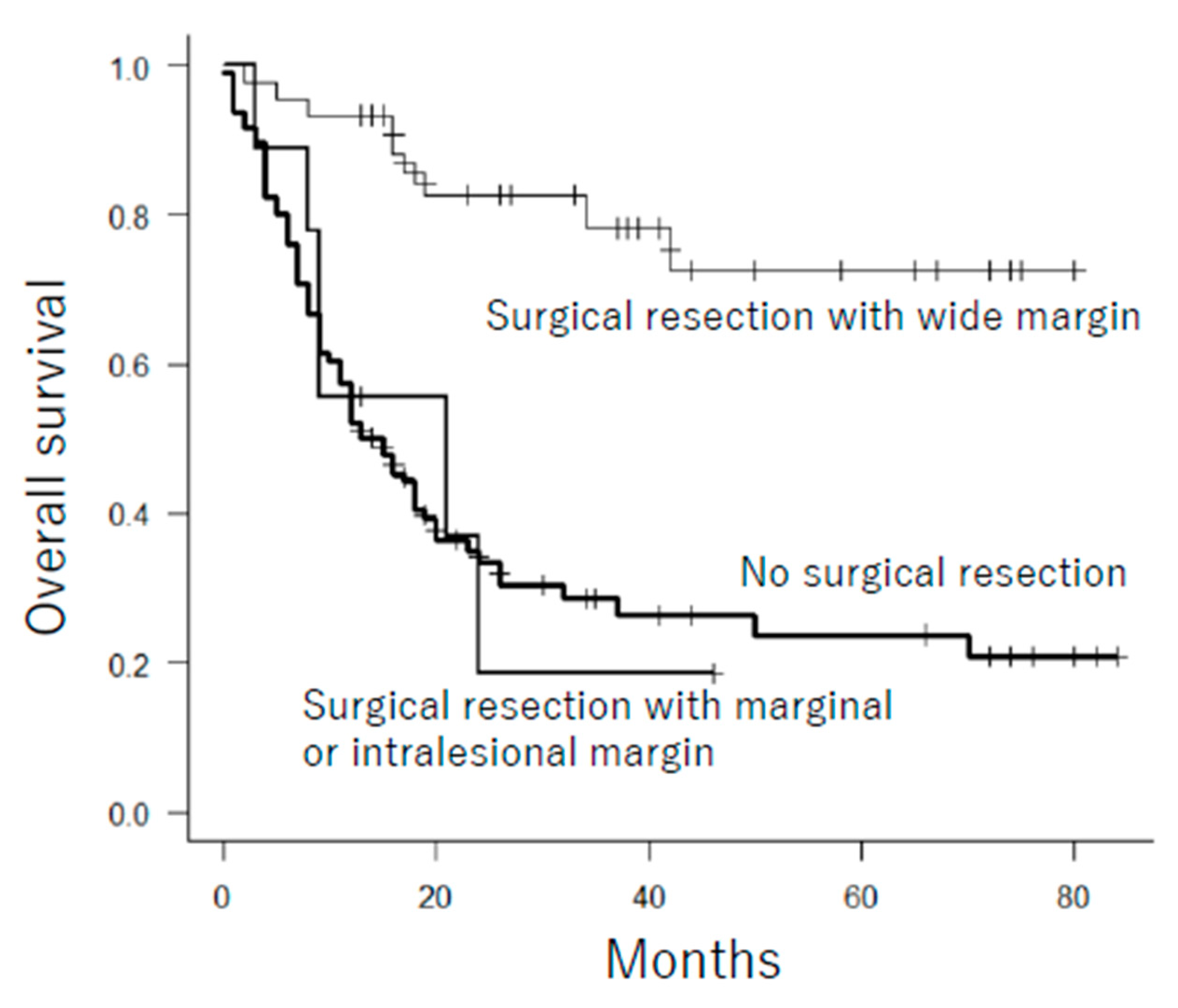
3.3.2. Indication for Surgical Resection of Pelvic Osteosarcoma
4. Discussion
4.1. Reasons for the Poor Prognosis of Pelvic Osteosarcoma Based on the Comparison of Pelvic and Femoral Osteosarcoma
4.2. Impact and Indication of Surgical Resection of Pelvic Osteosarcoma
4.3. Additional/Other Treatment Options
4.4. Future Direction
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meyers, P.A.; Schwartz, C.L.; Krailo, M.; Kleinerman, E.S.; Betcher, D.; Bernstein, M.L.; Conrad, E.; Ferguson, W.; Gebhardt, M.; Goorin, A.M.; et al. Osteosarcoma: A Randomized, Prospective Trial of the Addition of Ifosfamide and/or Muramyl Tripeptide to Cisplatin, Doxorubicin, and High-Dose Methotrexate. J. Clin. Oncol. 2005, 23, 2004–2011. [Google Scholar] [CrossRef] [PubMed]
- Mirabello, L.; Troisi, R.J.; Savage, S.A. Osteosarcoma incidence and survival rates from 1973 to 2004: Data from the Surveillance, Epidemiology, and End Results Program. Cancer 2009, 115, 1531–1543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuda, Y.; Ogura, K.; Shinoda, Y.; Kobayashi, H.; Tanaka, S.; Kawai, A. The outcomes and prognostic factors in patients with osteosarcoma according to age: A Japanese nationwide study with focusing on the age differences. BMC Cancer 2018, 18, 614. [Google Scholar] [CrossRef] [PubMed]
- Smeland, S.; Bielack, S.S.; Whelan, J.; Bernstein, M.; Hogendoorn, P.; Krailo, M.D.; Gorlick, R.; Janeway, K.A.; Ingleby, F.C.; Anninga, J.; et al. Survival and prognosis with osteosarcoma: Outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur. J. Cancer 2019, 109, 36–50. [Google Scholar] [CrossRef] [Green Version]
- Kawai, A.; Huvos, A.G.; Meyers, P.A.; Healey, J. Osteosarcoma of the pelvis. Oncologic results of 40 patients. Clin. Orthop. Relat. Res. 1998, 1998, 196–207. [Google Scholar]
- Grimer, R.J.; Carter, S.R.; Tillman, R.M.; Spooner, D.; Mangham, D.C.; Kabukcuoglu, Y. Osteosarcoma of the pelvis. J. Bone Jt. Surg. Br. 1999, 81, 796–802. [Google Scholar] [CrossRef]
- Ozaki, T.; Flege, S.; Kevric, M.; Lindner, N.; Maas, R.; Delling, G.; Schwarz, R.; Von Hochstetter, A.R.; Salzer-Kuntschik, M.; Berdel, W.E.; et al. Osteosarcoma of the Pelvis: Experience of the Cooperative Osteosarcoma Study Group. J. Clin. Oncol. 2003, 21, 334–341. [Google Scholar] [CrossRef]
- Ferrari, S.; Palmerini, E.; Fabbri, N.; Staals, E.; Ferrari, C.; Alberghini, M.; Picci, P. Osteosarcoma of the pelvis: A monoinstitutional experience in patients younger than 41 years. Tumori. J. 2012, 98, 702–708. [Google Scholar] [CrossRef]
- Parry, M.C.; Laitinen, M.; Albergo, J.; Jeys, L.; Carter, S.; Gaston, C.L.; Sumathi, V.; Grimer, R.J. Osteosarcoma of the pelvis. Bone Jt. J. 2016, 98, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Angelini, A.; Drago, G.; Trovarelli, G.; Calabrò, T.; Ruggieri, P. Infection after Surgical Resection for Pelvic Bone Tumors: An Analysis of 270 Patients from One Institution. Clin. Orthop. Relat. Res. 2014, 472, 349–359. [Google Scholar] [CrossRef] [Green Version]
- Cottias, P.; Vinh, T.S.; Tomeno, B.; Anract, P. Complications and functional evaluation of 17 saddle prostheses for resection of periacetabular tumors. J. Surg. Oncol. 2001, 78, 90–100. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, C.; Gosheger, G.; Gebert, C.; Jürgens, H.; Winkelmann, W. Functional results and quality of life after treatment of pelvic sarcomas involving the acetabulum. J. Bone Jt. Surg. Am. 2006, 88, 575–582. [Google Scholar]
- Fuchs, B.; Hoekzema, N.; Larson, D.R.; Inwards, C.Y.; Sim, F.H. Osteosarcoma of the pelvis: Outcome analysis of surgical treatment. Clin. Orthop. Relat. Res. 2009, 467, 510–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsunobu, A.; Imai, R.; Kamada, T.; Imaizumi, T.; Tsuji, H.; Tsujii, H.; Shioyama, Y.; Honda, H.; Tatezaki, S.-I.; for the Working Group for Bone and Soft Tissue Sarcomas. Impact of carbon ion radiotherapy for unresectable osteosarcoma of the trunk. Cancer 2012, 118, 4555–4563. [Google Scholar] [CrossRef]
- Nishida, Y.; Isu, K.; Ueda, T.; Nishimoto, Y.; Tsuchiya, H.; Wada, T.; Sato, K.; Tsukushi, S.; Sugiura, H. Osteosarcoma in the elderly over 60 years: A multicenter study by the Japanese musculoskeletal oncology group. J. Surg. Oncol. 2009, 100, 48–54. [Google Scholar] [CrossRef]
- Imura, Y.; Takenaka, S.; Kakunaga, S.; Nakai, T.; Wakamatsu, T.; Outani, H.; Tanaka, T.; Tamiya, H.; Oshima, K.; Hamada, K.; et al. Survival analysis of elderly patients with osteosarcoma. Int. Orthop. 2019, 43, 1741–1747. [Google Scholar] [CrossRef]
- Iwata, S.; Ishii, T.; Kawai, A.; Hiruma, T.; Yonemoto, T.; Kamoda, H.; Asano, N.; Takeyama, M. Prognostic Factors in Elderly Osteosarcoma Patients: A Multi-institutional Retrospective Study of 86 Cases. Ann. Surg. Oncol. 2014, 21, 263–268. [Google Scholar] [CrossRef]
- Kumar, R.; Kumar, M.; Malhotra, K.; Patel, S. Primary Osteosarcoma in the Elderly Revisited: Current Concepts in Diagnosis and Treatment. Curr. Oncol. Rep. 2018, 20, 13. [Google Scholar] [CrossRef]
- Grimer, R.J.; Cannon, S.R.; Taminiau, A.M.; Bielack, S.; Kempf-Bielack, B.; Windhager, R.; Dominkus, M.; Saeter, G.; Bauer, H.; Meller, I.; et al. Osteosarcoma over the age of forty. Eur. J. Cancer 2003, 39, 157–163. [Google Scholar] [CrossRef]
- Manoso, M.W.; Healey, J.H.; Boland, P.J.; Athanasian, E.A.; Maki, R.G.; Huvos, A.G.; Morris, C.D. De novo osteogenic sarcoma in patients older than forty: Benefit of multimodality therapy. Clin. Orthop. Relat. Res. 2005, 438, 110–115. [Google Scholar] [CrossRef]
- Griesser, M.J.; Gillette, B.; Crist, M.; Pan, X.; Muscarella, P.; Scharschmidt, T.; Mayerson, J. Internal and external hemipelvectomy or flail hip in patients with sarcomas: Quality-of-life and functional outcomes. Am. J. Phys. Med. Rehabil. 2012, 91, 24–32. [Google Scholar] [CrossRef]
- Takenaka, S.; Araki, N.; Outani, H.; Hamada, K.; Yoshikawa, H.; Kamada, T.; Imai, R. Complication rate, functional outcomes, and risk factors associated with carbon ion radiotherapy for patients with unresectable pelvic bone sarcoma. Cancer 2020, 126, 4188–4196. [Google Scholar] [CrossRef] [PubMed]
- Bacci, G.; Rocca, M.; Salone, M.; Balladelli, A.; Ferrari, S.; Palmerini, E.; Forni, C.; Briccoli, A. High grade osteosarcoma of the extremities with lung metastases at presentation: Treatment with neoadjuvant chemotherapy and simultaneous resection of primary and metastatic lesions. J. Surg. Oncol. 2008, 98, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, T.; Hillmann, A.; Winkelmann, W. Treatment Outcome of Pelvic Sarcomas in Young Children: Orthopaedic and Oncologic Analysis. J. Pediatr. Orthop. 1998, 18, 350–355. [Google Scholar] [CrossRef]
- Liang, H.; Ji, T.; Zhang, Y.; Wang, Y.; Guo, W. Reconstruction with 3D-printed pelvic endoprostheses after resection of a pelvic tumour. Bone Jt. J. 2017, 99, 267–275. [Google Scholar] [CrossRef]
- Gouin, F.; Paul, L.; Odri, G.-A.; Cartiaux, O. Computer-Assisted Planning and Patient-Specific Instruments for Bone Tumor Resection within the Pelvis: A Series of 11 Patients. Sarcoma 2014, 2014, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.C.; Kumta, S.M.; Chiu, K.H.; Antonio, G.E.; Unwin, P.; Leung, K.S. Precision tumour resection and reconstruction using image-guided computer navigation. J. Bone Jt. Surgery. Br. Vol. 2007, 89, 943–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suehara, Y.; Alex, D.; Bowman, A.S.; Middha, S.; Zehir, A.; Chakravarty, D.; Wang, L.; Jour, G.; Nafa, K.; Hayashi, T.; et al. Clinical Genomic Sequencing of Pediatric and Adult Osteosarcoma Reveals Distinct Molecular Subsets with Potentially Targetable Alterations. Clin. Cancer Res. 2019, 25, 6346–6356. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Patient Number (%) | p | ||
|---|---|---|---|---|
| Femoral OS | Pelvic OS | |||
| Gender | Male | 338 (53.5%) | 73 (48.7%) | 0.332 |
| Female | 294 (46.5%) | 77 (51.3%) | ||
| Metastasis at presentation | M0 | 531 (84.7%) | 109 (73.2%) | 0.001 |
| M1 | 96 (15.3%) | 40 (26.8%) | ||
| Age | mean | 27.58 years | 50.63 years | <0.001 |
| <40 years | 473 (74.8%) | 45 (30.0%) | <0.001 | |
| ≥40 years | 159 (25.2%) | 105 (70.0%) | ||
| <60 years | 542 (80.1%) | 90 (60.0%) | <0.001 | |
| ≥60 years | 90 (14.2%) | 60 (40.0%) | ||
| Size | mean | 10.63 cm | 11.12 cm | 0.278 |
| <8 cm | 163 (27.0%) | 32 (21.9%) | 0.247 | |
| ≥8 cm | 440 (73.0%) | 114 (78.1%) | ||
| <12 cm | 408 (67.7%) | 84 (57.5%) | 0.027 | |
| ≥12 cm | 195 (32.3%) | 62 (42.5%) | ||
| Secondary | Primary | 624 (98.7%) | 144 (96.0%) | 0.054 |
| Secondary | 8 (1.3%) | 6 (4.0%) | ||
| Chemotherapy | No | 71 (11.3%) | 31 (20.7%) | 0.003 |
| Yes | 560 (88.7%) | 119 (79.3%) | ||
| Surgical resection | No | 26 (4.1%) | 95 (63.3%) | <0.001 |
| Yes | 606 (95.9%) | 55 (36.7%) | ||
| 3-Year OS Rate | 3-Year OS Rate | |||||
|---|---|---|---|---|---|---|
| Variables | All Cases | p | Femoral OS | Pelvic OS | p | |
| Location | Femoral | 73.7% | <0.001 | |||
| Pelvis | 42.8% | |||||
| Gender | Male | 68.3% | 0.818 | 72.9% | 45.7% | <0.001 |
| Female | 67.4% | 74.6% | 39.0% | <0.001 | ||
| Metastasis at presentation | M0 | 75.8% | <0.001 | 80.6% | 52.0% | <0.001 |
| M1 | 29.3% | 33.9% | 19.7% | 0.002 | ||
| Age at diagnosis | <40 years | 77.9% | <0.001 | 79.9% | 55.7% | <0.001 |
| ≥40 years | 48.5% | 55.8% | 37.3% | <0.001 | ||
| <60 years | 74.2% | <0.001 | 76.6% | 59.5% | <0.001 | |
| ≥60 years | 41.8% | 56.9% | 19.0% | <0.001 | ||
| Size | <12 cm | 73.2% | <0.001 | 77.6% | 51.5% | <0.001 |
| ≥12 cm | 56.7% | 64.4% | 32.2% | <0.001 | ||
| Secondary | Primary | 68.3% | 0.085 | 73.8% | 43.5% | <0.001 |
| Secondary | 48.2% | 62.5% | 25.0% | 0.163 | ||
| Chemotherapy | Yes | 70.2% | <0.001 | 74.9% | 48.0% | <0.001 |
| No | 52.1% | 64.0% | 22.4% | <0.001 | ||
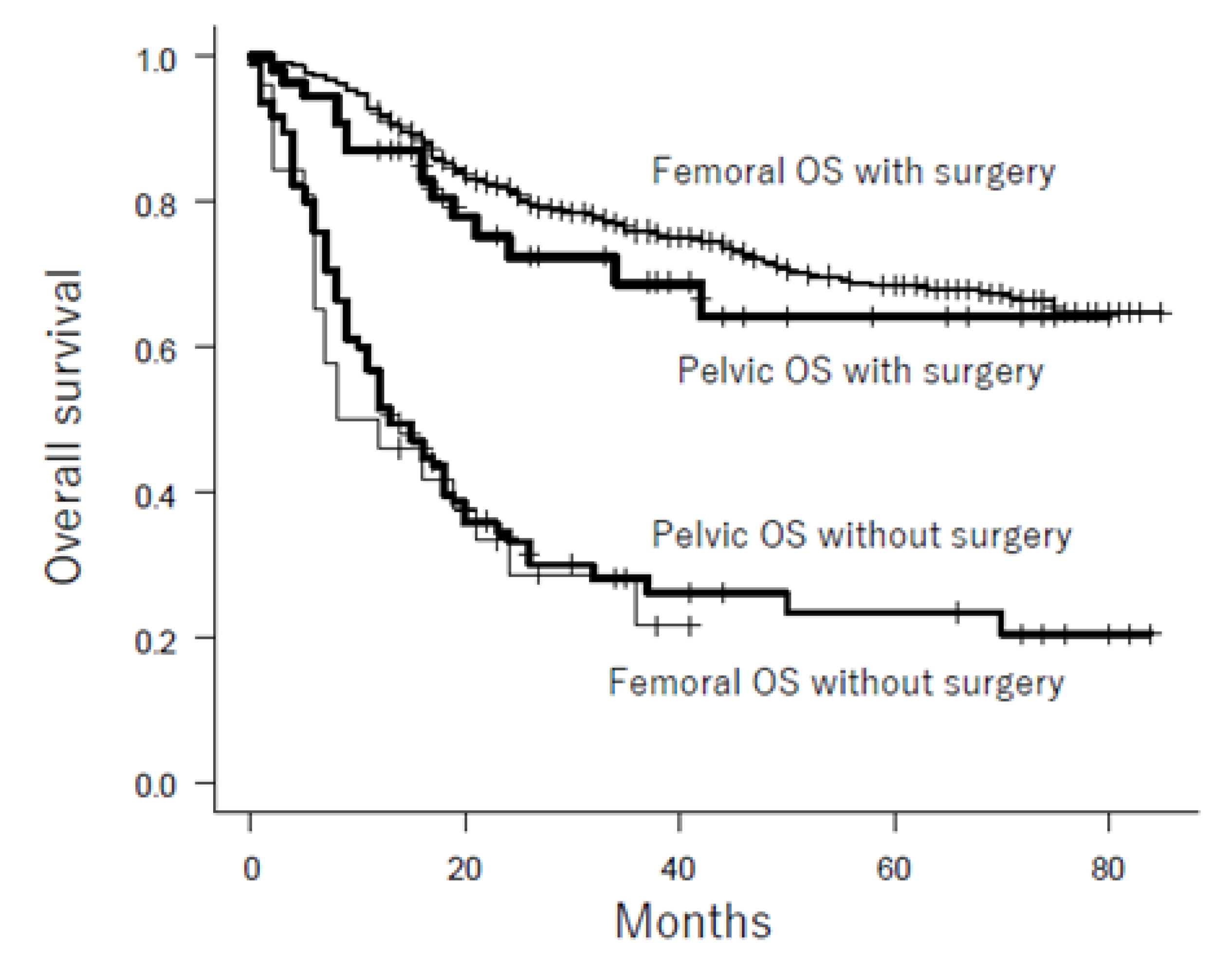
| Surgical resection | Yes | 75.5% | <0.001 | 76.0% | 68.9% | 0.329 |
| No | 26.6% | 21.6% | 28.2% | 0.644 | ||
| Variables | HR | 95% CI | p |
|---|---|---|---|
| Location: pelvis | 1.01 | 0.67–1.51 | 0.976 |
| Gender: female | 1.06 | 0.82–1.36 | 0.679 |
| Metastasis at presentation: yes | 3.56 | 2.62–4.84 | <0.001 |
| Age ≥60 years | 2.96 | 2.15–4.06 | <0.001 |
| Size ≥12 cm | 1.38 | 1.05–1.81 | 0.021 |
| Secondary osteosarcoma | 0.96 | 0.42–2.21 | 0.919 |
| Chemotherapy: yes | 0.92 | 0.63–1.34 | 0.661 |
| Surgical resection: yes | 0.35 | 0.23–0.53 | <0.001 |
| Patient Number (%) (n = 150) | Patient Number (%) after Propensity Score Matching (n = 92) | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Resection | No Resection | p | Resection | No Resection | p | |
| Gender | Male | 26 (47.3%) | 47 (49.5%) | 0.928 | 22 (47.8%) | 22 (47.8%) | 1.00 |
| Female | 29 (52.7%) | 48 (50.5%) | 24 (52.2%) | 24 (52.2%) | |||
| Metastasis at presentation | M0 | 51 (92.7%) | 58 (61.7%) | <0.001 | 42 (91.3%) | 43 (93.5%) | 1.00 |
| M1 | 4 (7.3%) | 36 (38.3%) | 4 (8.7%) | 3 (6.5%) | |||
| Age | <40 years | 19 (34.5%) | 26 (27.4%) | 0.460 | 17 (37.0%) | 17 (37.0%) | 1.00 |
| ≥40 years | 36 (65.5%) | 69 (72.6%) | 29 (63.0%) | 29 (63.0%) | |||
| <60 years | 40 (72.7%) | 50 (52.6%) | 0.025 | 32 (69.6%) | 32 (69.6%) | 1.00 | |
| ≥60 years | 15 (27.3%) | 45 (47.4%) | 14 (30.4%) | 14 (30.4%) | |||
| Size | <12 cm | 40 (74.1%) | 44 (47.8%) | 0.003 | 33 (71.7%) | 31 (67.4%) | 0.82 |
| ≥12 cm | 14 (25.9%) | 48 (52.2%) | 13 (28.3%) | 15 (32.6%) | |||
| Secondary | Primary | 52 (94.5%) | 92 (96.8%) | 0.795 | 45 (97.8%) | 45 (97.8%) | 1.00 |
| Secondary | 3 (5.5%) | 3 (3.2%) | 1 (2.2%) | 1 (2.2%) | |||
| Chemotherapy | Yes | 44 (80.0%) | 75 (78.9%) | 1 | 39 (84.8%) | 40 (93.5%) | 1.00 |
| No | 11 (20.0%) | 20 (21.1%) | 7 (15.2%) | 6 (13.0%) | |||
| Variables | Odds Ratio | 95% CI | p |
|---|---|---|---|
| Gender: female | 1.24 | 0.57–2.69 | 0.583 |
| Metastasis at presentation: yes | 0.167 | 0.052–0.53 | 0.002 |
| Age ≥60 years | 0.299 | 0.12–0.75 | 0.010 |
| Size ≥12 cm | 0.46 | 0.20–1.05 | 0.065 |
| Secondary osteosarcoma | 3.25 | 0.46–23.0 | 0.238 |
| Chemotherapy: yes | 0.754 | 0.26–2.19 | 0.605 |
| Stage at Presentation | Age at Diagnosis | Surgical Resection | No. of Patients | 3-Year OS Rate | p |
|---|---|---|---|---|---|
| Localized | <60 years old | Yes | 36 | 83.0 | 0.005 |
| Localized | <60 years old | No | 32 | 50.9 | |
| Localized | ≥60 years old | Yes | 15 | 39.1 | 0.117 |
| Localized | ≥60 years old | No | 26 | 22.0 | |
| Metastatic | <60 years old | Yes | 4 | 75.0 | 0.251 |
| Metastatic | <60 years old | No | 18 | 29.2 | |
| Metastatic | ≥60 years old | Yes | 0 | N.A | N.A. |
| Metastatic | ≥60 years old | No | 18 | 0.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takenaka, S.; Tamiya, H.; Wakamatsu, T.; Nakai, S.; Imura, Y.; Outani, H.; Yagi, T.; Kawai, A. Impact of Surgical Resection and Reasons for Poor Prognosis of Pelvic Osteosarcoma Based on the Bone Tumor Registry in Japan. Cancers 2021, 13, 3320. https://doi.org/10.3390/cancers13133320
Takenaka S, Tamiya H, Wakamatsu T, Nakai S, Imura Y, Outani H, Yagi T, Kawai A. Impact of Surgical Resection and Reasons for Poor Prognosis of Pelvic Osteosarcoma Based on the Bone Tumor Registry in Japan. Cancers. 2021; 13(13):3320. https://doi.org/10.3390/cancers13133320
Chicago/Turabian StyleTakenaka, Satoshi, Hironari Tamiya, Toru Wakamatsu, Sho Nakai, Yoshinori Imura, Hidetatsu Outani, Toshinari Yagi, and Akira Kawai. 2021. "Impact of Surgical Resection and Reasons for Poor Prognosis of Pelvic Osteosarcoma Based on the Bone Tumor Registry in Japan" Cancers 13, no. 13: 3320. https://doi.org/10.3390/cancers13133320