
Reappraising the Role of Trans-Sphenoidal Surgery in Prolactin-Secreting Pituitary Tumors

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
- Patients carrying giant prolactinomas (diameter > 4 cm);
- Patients with a follow-up shorter than 12 months.
2.2. Clinical Management of Patients
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Impact of Surgery as the First-Line Treatment
3.3. Impact of Surgery as the Second-Line Treatment
3.4. Adjustment for Other Factors Impacting the Rate of a Cure
3.5. Validation of Results in Long-Term Follow-Up Patients
3.6. Surgical Complications
3.7. Selection Biases
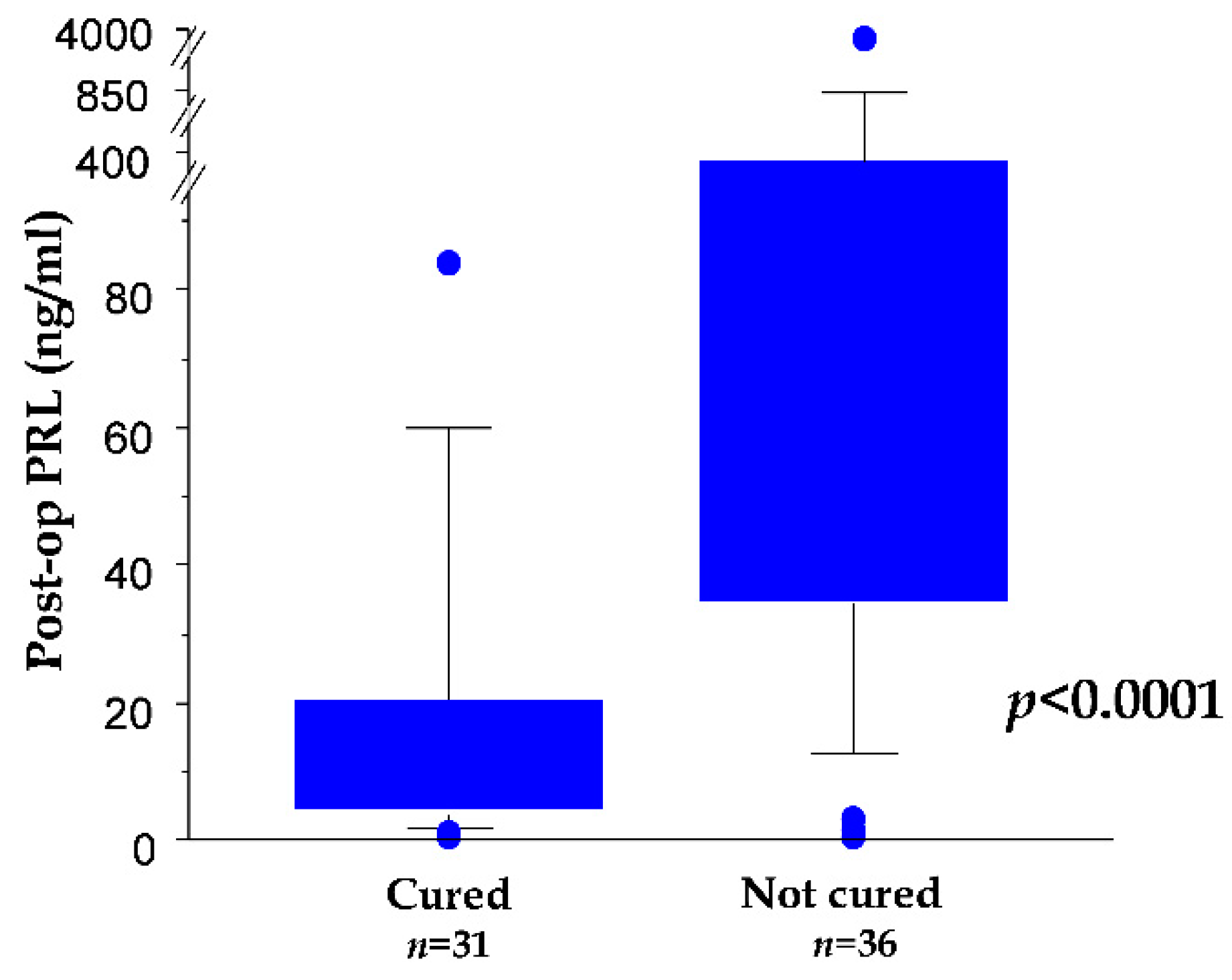
3.8. First Day Postoperative Serum PRL as Biomarker for a Cure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ezzat, S.; Asa, S.L.; Couldwell, W.T.; Barr, C.E.; Dodge, W.E.; Vance, M.L.; McCutcheon, I.E. The prevalence of pituitary adenomas: A systematic review. Cancer 2004, 101, 613–619. [Google Scholar] [CrossRef]
- Colao, A.; Di Sarno, A.; Guerra, E.; Pivonello, R.; Cappabianca, P.; Caranci, F.; Elefante, A.; Cavallo, L.M.; Briganti, F.; Cirillo, S.; et al. Predictors of remission of hyperprolactinaemia after long-term withdrawal of cabergoline therapy. Clin. Endocrinol. 2007, 673, 426–433. [Google Scholar] [CrossRef]
- Watanabe, S.; Takano, S.; Akutsu, H.; Sato, H.; Matsumura, A. Prolactinoma treatment status in the cabergoline era. No Shinkei Geka. 2011, 39, 1045–1054. [Google Scholar]
- Melmed, S.; Casanueva, F.F.; Hoffman, A.R.; Kleinberg, D.L.; Montori, V.M.; Schlechte, J.A.; Wass, J.A.; Endocrine Society. Diagnosis and treatment of hyperprolactinemia: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 273–288. [Google Scholar] [CrossRef]
- Akin, S.; Isikay, I.; Soylemezoglu, F.; Yucel, T.; Gurlek, A.; Berker, M. Reasons and results of endoscopic surgery for prolactinomas: 142 surgical cases. Acta Neurochir. 2016, 158, 933–934. [Google Scholar] [CrossRef]
- Song, Y.-J.; Chen, M.-T.; Lian, W.; Xing, B.; Yao, Y.; Feng, M.; Wang, R.-Z. Surgical treatment for male prolactinoma: A retrospective study of 184 cases. Medicine 2017, 96, e5833. [Google Scholar] [CrossRef] [PubMed]
- Menucci, M.; Quiñones-Hinojosa, A.; Burger, P.; Salvatori, R. Effect of dopaminergic drug treatment on surgical findings in prolactinomas. Pituitary 2011, 14, 68–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamanipoor Najafabadi, A.H.; Zandbergen, I.M.; de Vries, F.; Broersen, L.H.; van den Akker-van Marle, M.E.; Pereira, A.M.; Peul, W.C.; Dekkers, O.M.; van Furth, W.R.; Biermasz, N.R. Surgery as a Viable Alternative First-Line Treatment for Prolactinoma Patients. A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2020, 105, e32–e41. [Google Scholar] [CrossRef]
- Lauretti, L.; D’Alessandris, Q.G.; Rigante, M.; Ricciardi, L.; Mattogno, P.P.; Olivi, A. O-arm in Endonasal Endoscopic Cranial Base Surgery: Technical Note on Initial Feasibility. World Neurosurg. 2018, 117, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Behan, L.A.; Moyles, P.; Cuesta, M.; Rogers, B.; Crowley, R.K.; Ryan, J.; Brennan, P.; Smith, D.; Tormey, W.; Sherlock, M.; et al. The incidence of anterior pituitary hormone deficiencies in patients with microprolactinoma and idiopathic hyperprolactinaemia. Clin. Endocrinol. 2017, 87, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Micko, A.; Vila, G.; Höftberger, R.; Knosp, E.; Wolfsberger, S. Endoscopic Transsphenoidal Surgery of Microprolactinomas: A Reappraisal of Cure Rate Based on Radiological Criteria. Neurosurgery 2019, 85, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Klibanski, A. Clinical practice. Prolactinomas. N. Engl. J. Med. 2010, 362, 1219–1226. [Google Scholar] [CrossRef]
- Sala, E.; Bellaviti Buttoni, P.; Malchiodi, E.; Verrua, E.; Carosi, G.; Profka, E.; Rodari, G.; Filopanti, M.; Ferrante, E.; Spada, A.; et al. Recurrence of hyperprolactinemia following dopamine agonist withdrawal and possible predictive factors of recurrence in prolactinomas. J. Endocrinol. Investig. 2016, 29, 1377–1381. [Google Scholar] [CrossRef] [PubMed]
- Chanson, P.; Maiter, D. Prolactinoma. In The Pituitary, 4th ed.; Melmed, S., Ed.; Elsevier: Cambridge, MA, USA, 2017; pp. 467–514. [Google Scholar]
- Ji, M.J.; Kim, J.H.; Lee, J.H.; Lee, J.H.; Kim, Y.H.; Paek, S.H.; Shin, C.S.; Kim, S.Y. Best candidates for dopamine agonist withdrawal in patients with prolactinomas. Pituitary 2017, 20, 578–584. [Google Scholar] [CrossRef]
- Babey, M.; Sahli, R.; Vajtai, I.; Andres, R.H.; Seiler, R.W. Pituitary Surgery for Small Prolactinomas as an Alternative to Treatment with Dopamine Agonists. Pituitary 2011, 14, 222–230. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, D.K.; Vance, M.L.; Boulos, P.T.; Laws, E.R. Surgical Outcomes in Hyporesponsive Prolactinomas: Analysis of Patients with Resistance or Intolerance to Dopamine Agonists. Pituitary 2005, 8, 53–60. [Google Scholar] [CrossRef]
- Ikeda, H.; Watanabe, K.; Tominaga, T.; Yoshimoto, T. Transsphenoidal Microsurgical Results of Female Patients with Prolactinomas. Clin. Neurol. Neurosurg. 2013, 115, 1621–1625. [Google Scholar] [CrossRef] [PubMed]
- Kreutzer, J.; Buslei, R.; Wallaschofski, H.; Hofmann, B.; Nimsky, C.; Fahlbusch, R.; Buchfelder, M. Operative Treatment of Prolactinomas: Indications and Results in a Current Consecutive Series of 212 Patients. Eur. J. Endocrinol. 2008, 158, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Loyo-Varela, M.; Herrada-Pineda, T.; Revilla-Pacheco, F.; Manrique-Guzman, S. Pituitary Tumor Surgery: Review of 3004 Cases. World Neurosurg. 2013, 79, 331–336. [Google Scholar] [CrossRef]
- Paluzzi, A.; Fernandez-Miranda, J.C.; Stefko, S.T.; Challinor, S.; Snyderman, C.H.; Gardner, P.A. Endoscopic Endonasal Approach for Pituitary Adenomas: A Series of 555 Patients. Pituitary 2014, 17, 307–319. [Google Scholar] [CrossRef]
- Primeau, V.; Raftopoulos, C.; Maiter, D. Outcomes of Transsphenoidal Surgery in Prolactinomas: Improvement of Hormonal Control in Dopamine Agonist-Resistant Patients. Eur. J. Endocrinol. 2012, 166, 779–786. [Google Scholar] [CrossRef]
- Qu, X.; Wang, M.; Wang, G.; Han, T.; Mou, C.; Han, L.; Jiang, M.; Qu, Y.; Zhang, M.; Pang, Q.; et al. Surgical Outcomes and Prognostic Factors of Transsphenoidal Surgery for Prolactinoma in Men: A Single-Center Experience with 87 Consecutive Cases. Eur. J. Endocrinol. 2011, 164, 499–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raverot, G.; Wierinckx, A.; Dantony, E.; Auger, C.; Chapas, G.; Villeneuve, L.; Brue, T.; Figarella-Branger, D.; Roy, P.; Jouanneau, E.; et al. Prognostic Factors in Prolactin Pituitary Tumors: Clinical, Histological, and Molecular Data From a Series of 94 Patients With a Long Postoperative Follow-Up. J. Clin. Endocrinol. Metab. 2010, 95, 1708–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinha, S.; Sharma, B.S.; Mahapatra, A.K. Microsurgical Management of Prolactinomas-Clinical and Hormonal Outcome in a Series of 172 Cases. Neurol. India 2011, 59, 532–536. [Google Scholar] [CrossRef]
- Sinkūnas, K.; Rastenyte, D.; Deltuva, V.P.; Knispelis, R.; Tamasauskas, A. Transsphenoidal Surgery for Prolactinomas: Results and Prognosis. Medicina 2007, 43, 691–697. [Google Scholar] [CrossRef] [Green Version]
- Tamasauskas, A.; Sinkunas, K.; Bunevicius, A.; Radziunas, A.; Skiriute, D.; Deltuva, V.P. Transsphenoidal Surgery for Microprolactinomas in Women: Results and Prognosis. Acta Neurochir. 2012, 154, 1889–1893. [Google Scholar] [CrossRef] [PubMed]
- Andereggen, L.; Frey, J.; Andres, R.H.; El-Koussy, M.; Beck, J.; Seiler, R.W.; Christ, E. 10-year follow-up study comparing primary medical vs. surgical therapy in women with prolactinomas. Endocrine 2017, 55, 223–230. [Google Scholar] [CrossRef]
- Rutkowski, M.J.; Aghi, M.K. Medical versus surgical treatment of prolactinoma: An analysis of treatment outcomes. Expert Rev. Endocrinol. Metab. 2018, 13, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Chiloiro, S.; Bianchi, A.; Doglietto, F.; de Waure, C.; Giampietro, A.; Fusco, A.; Iacovazzo, D.; Tartaglione, L.; Di Nardo, F.; Signorelli, F.; et al. Radically resected pituitary adenomas: Prognostic role of Ki 67 labeling index in a monocentric retrospective series and literature review. Pituitary 2014, 17, 267–276. [Google Scholar] [CrossRef]
- Coli, A.; Asa, S.A.; Fadda, G.; Scannone, D.; Chiloiro, S.; De Marinis, L.; Lauretti, L.; Ranelletti, L.; Lauriola, L. Minichromosome Maintenance Protein 7 as Prognostic Marker of Tumor Aggressiveness in Pituitary Adenoma Patients. Eur. J. Endocrinol. 2016, 174, 307–314. [Google Scholar] [CrossRef] [Green Version]
- Li, C.Z.; Gui, S.B.; Zong, X.Y.; Zhang, Y.Z. The Expression of Estrogen Receptor Subtypes in Prolactinomas and Their Relationship to Tumor Biological Behavior. Biomed. Environ. Sci. 2015, 28, 820–822. [Google Scholar] [CrossRef]
- Shimazu, S.; Shimatsu, A.; Yamada, S.; Inoshita, N.; Nagamura, Y.; Usui, T.; Tsukada, T. Resistance to Dopamine Agonists in Prolactinoma Is Correlated with Reduction of Dopamine D2 Receptor Long Isoform mRNA Levels. Eur. J. Endocrinol. 2012, 166, 383–390. [Google Scholar] [CrossRef] [Green Version]
- Trouillas, J.; Delgrange, E.; Wierinckx, A.; Vasiljevic, A.; Jouanneau, E.; Burman, P.; Raverot, G. Clinical, Pathological, and Molecular Factors of Aggressiveness in Lactotroph Tumours. Neuroendocrinology 2019, 109, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Barbarino, A.; De Marinis, L.; Anile, C.; Menini, E.; Merlini, G.; Maira, G. Dopaminergic Mechanisms Regulating Prolactin Secretion in Patients With Prolactin-Secreting Pituitary Adenoma. Long-term Studies after Selective Transsphenoidal Surgery. Metabolism 1982, 31, 1100–1104. [Google Scholar] [CrossRef]
- Barbarino, A.; De Marinis, L.; Maira, G.; Menini, E.; Anile, C. Serum Prolactin Response to Thyrotropin-Releasing Hormone and Metoclopramide in Patients with Prolactin-Secreting Tumors Before and After Transsphenoidal Surgery. J. Clin. Endocrinol. Metab. 1978, 47, 1148–1151. [Google Scholar] [CrossRef] [PubMed]
- Barbarino, A.; De Marinis, L.; Mancini, A.; Menini, E.; D’Amico, C.; Passeri, M.; Sambo, P.; Anile, C.; Maira, G. Prolactin Dynamics in Patients with Non-Secretin Tumours of the Hypothalamic-Pituitary Region. Acta Endocrinol. 1985, 110, 10–16. [Google Scholar] [CrossRef]
- Barbarino, A.; De Marinis, L.; Menini, E.; Anile, C.; Maira, G. Prolactin-secreting Pituitary Adenomas: Prolactin Dynamics Before and After Transsphenoidal Surgery. Acta Endocrinol. 1979, 91, 397–409. [Google Scholar] [CrossRef]
- De Marinis, L.; Mancini, A.; Minnielli, S.; Masala, R.; Anile, C.; Maira, G.; Barbarino, A. Evaluation of Dopaminergic Tone in Hyperprolactinemia. III. Thyroid-stimulating Hormone Response to Metoclopramide in Differential Diagnosis and Postoperative Follow-Up of Prolactinoma Patients. Metabolism 1985, 34, 917–922. [Google Scholar] [CrossRef]
- Del Gatto, V.; Bima, C.; Chiloiro, S.; Giampietro, A.; Bianchi, A. Use of 111In-pentetreotide Scintigraphy for Diagnosis and Management of Resistant Macroprolactinoma. Endocrine 2018, 60, 532–534. [Google Scholar] [CrossRef]
- Fusco, A.; Lugli, F.; Sacco, E.; Tilaro, L.; Bianchi, A.; Angelini, F.; Tofani, A.; Barini, A.; Lauriola, L.; Maira, G.; et al. Efficacy of the Combined Cabergoline and Octreotide Treatment in a Case of a Dopamine-Agonist Resistant Macroprolactinoma. Pituitary 2011, 14, 351–357. [Google Scholar] [CrossRef]
- Maira, G.; Anile, C.; De Marinis, L.; Barbarino, A. Prolactin-secreting Adenomas: Surgical Results and Long-Term Follow-Up. Neurosurgery 1989, 24, 736–743. [Google Scholar] [CrossRef] [PubMed]
- Maira, G.; Anile, C.; De Marinis, L.; Barbarino, A. Prolactin-secreting Adenomas--Surgical Results. Can. J. Neurol. Sci. 1990, 17, 67–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Group | Whole Cohort | First-Line Treatment | Surgery | ||
|---|---|---|---|---|---|
| TSS | DA | Yes | No | ||
| n (%) | 259 (100) | 119 (45.9) | 140 (54.1) | 194 (74.9) | 65 (25.1) |
| Female, n (%) | 164 (63.3) | 56 (34.1) | 108 (65.9) | 113 (68.9) | 51 (31.1) |
| Male, n (%) | 95 (36.7) | 63 (66.3) | 32 (33.7) | 81 (85.3) | 14 (14.7) |
| Microadenomas, n (%) | 125 (48.3) | 41 (32.8) | 84 (67.2) | 78 (62.4) | 47 (37.6) |
| Macroadenomas, n (%) | 134 (51.7) | 78 (58.2) | 56 (41.8) | 116 (86.6) | 18 (13.4) |
| Female: microadenomas, n (%) | 105 (64.0) | 29 (27.6) | 76 (72.4) | 62 (59.0) | 43 (41.0) |
| Female: macroadenomas, n (%) | 59 (36.0) | 27 (45.8) | 32 (54.2) | 51 (86.4) | 8 (13.6) |
| Male: microadenomas, n (%) | 20 (21.1) | 12 (60) | 8 (40) | 16 (80) | 4 (20) |
| Male: macroadenomas, n (%) | 75 (78.9) | 51 (68) | 24 (32) | 65 (86.7) | 10 (13.3) |
| Age, mean (range) (years) | 35.2 (18–78) | 35.6 (18–78) | 34.8 (18–76) | 33.9 (18–78) | 38.9 (18–76) |
| Knosp: 0–II, n (%) | 227 (87.3) | 99 (83.2) | 127 (90.7) | 168 (74.3) | 58 (25.7) |
| Knosp: III and IV, n (%) | 33 (12.7) | 20 (16.8) | 13 (9.3) | 26 (78.8) | 7 (21.2) |
| Follow-up, mean (range) (months) | 102.2 (12–438) | 100.9 (12–438) | 103.2 (12–420) | 108.8 (12–438) | 82.7 (12–300) |
| Rate of Cure | ||||||
|---|---|---|---|---|---|---|
| Group | First-Line Treatment | p * | Surgery | p * | ||
| TSS, n (%) | DA, n (%) | yes | no | |||
| Whole Cohort | 56/119 (47.1) | 57/140 (40.7) | 0.3172 | 97/194 (50.0) | 16/65 (24.6) | 0.0005 |
| Female | 38/56 (67.9) | 49/108 (45.4) | 0.0081 | 72/113 (63.7) | 15/51 (29.4) | <0.0001 |
| Male | 18/63 (28.6) | 8/32 (25) | 0.8102 | 25/81 (30.9) | 1/14 (7.1) | 0.1026 |
| Microadenomas | 25/41 (61.0) | 41/84 (48.8) | 0.2530 | 52/78 (78.8) | 14/47 (21.2) | <0.0001 |
| Macroadenomas | 31/78 (39.7) | 16/56 (28.6) | 0.2028 | 45/116 (38.8) | 2/18 (11.1) | 0.0031 |
| Female: microadenomas | 20/29 (69.0) | 37/76 (48.7) | 0.0080 | 44/62 (71.0) | 13/43 (30.2) | <0.0001 |
| Female: macroadenomas | 18/27 (66.7) | 12/32 (37.5) | 0.0370 | 28/51 (54.9) | 2/8 (25) | 0.1455 |
| Male: microadenomas | 5/12 (41.7) | 4/8 (50) | >0.9999 | 8/16 (50) | 1/4 (25) | 0.5913 |
| Male: macroadenomas | 13/51 (25.5) | 4/24 (16.7) | 0.5566 | 17/65 (26.2) | 0/10 (0) | 0.1043 |
| Rate of Cure | ||||||
|---|---|---|---|---|---|---|
| Group | First-Line Treatment | p * | Surgery | p * | ||
| TSS, n (%) | DA, n (%) | yes | no | |||
| Whole Cohort | 56/119 (47.1) | 57/140 (40.7) | 0.3172 | 97/194 (50.0) | 16/65 (24.6) | 0.0005 |
| Female | 38/56 (67.9) | 49/108 (45.4) | 0.0081 | 72/113 (63.7) | 15/51 (29.4) | <0.0001 |
| Male | 18/63 (28.6) | 8/32 (25) | 0.8102 | 25/81 (30.9) | 1/14 (7.1) | 0.1026 |
| Microadenomas | 25/41 (61.0) | 41/84 (48.8) | 0.2530 | 52/78 (78.8) | 14/47 (21.2) | <0.0001 |
| Macroadenomas | 31/78 (39.7) | 16/56 (28.6) | 0.2028 | 45/116 (38.8) | 2/18 (11.1) | 0.00313 |
| Female: microadenomas | 20/29 (69.0) | 37/76 (48.7) | 0.0080 | 44/62 (71.0) | 13/43 (30.2) | <0.0001 |
| Female: macroadenomas | 18/27 (66.7) | 12/32 (37.5) | 0.0370 | 28/51 (54.9) | 2/8 (25) | 0.1455 |
| Male: microadenomas | 5/12 (41.7) | 4/8 (50) | >0.9999 | 8/16 (50) | 1/4 (25) | 0.5913 |
| Male: macroadenomas | 13/51 (25.5) | 4/24 (16.7) | 0.5566 | 17/65 (26.2) | 0/10 (0) | 0.1043 |
| Whole Court | >5ys FU population | |||||||
|---|---|---|---|---|---|---|---|---|
| p-Value | Odds Ratio | 95% Lower | 95% Upper | p-Value | Odds Ratio | 95% Lower | 95% Upper | |
| Not cured: constant | 0.5143 | 0.751 | 0.318 | 1.776 | 0.5060 | 0.695 | 0.237 | 2.033 |
| Surgery: Yes | <0.0001 | 0.196 | 0.087 | 0.439 | 0.0005 | 0.158 | 0.056 | 0.445 |
| Age | 0.921 | 1.001 | 0.981 | 1.022 | 0.5640 | 1.007 | 0.982 | 1.033 |
| Sex: Female | 0.0009 | 0.323 | 0.166 | 0.627 | 0.0016 | 0.257 | 0.11 | 0.598 |
| Size: Micro-PRL-omas | 0.0182 | 0.469 | 0.250 | 0.879 | 0.0997 | 0.516 | 0.235 | 1.134 |
| I treatment: TSS | 0.6573 | 0.863 | 0.451 | 1.650 | 0.7586 | 1.131 | 0.516 | 2.475 |
| Knosp III and IV | 0.618 | 1.280 | 0.485 | 3.381 | 0.6406 | 0.758 | 0.237 | 2.427 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mattogno, P.P.; D’Alessandris, Q.G.; Chiloiro, S.; Bianchi, A.; Giampietro, A.; Pontecorvi, A.; De Marinis, L.; Olivi, A.; Anile, C.; Lauretti, L. Reappraising the Role of Trans-Sphenoidal Surgery in Prolactin-Secreting Pituitary Tumors. Cancers 2021, 13, 3252. https://doi.org/10.3390/cancers13133252
Mattogno PP, D’Alessandris QG, Chiloiro S, Bianchi A, Giampietro A, Pontecorvi A, De Marinis L, Olivi A, Anile C, Lauretti L. Reappraising the Role of Trans-Sphenoidal Surgery in Prolactin-Secreting Pituitary Tumors. Cancers. 2021; 13(13):3252. https://doi.org/10.3390/cancers13133252
Chicago/Turabian StyleMattogno, Pier Paolo, Quintino Giorgio D’Alessandris, Sabrina Chiloiro, Antonio Bianchi, Antonella Giampietro, Alfredo Pontecorvi, Laura De Marinis, Alessandro Olivi, Carmelo Anile, and Liverana Lauretti. 2021. "Reappraising the Role of Trans-Sphenoidal Surgery in Prolactin-Secreting Pituitary Tumors" Cancers 13, no. 13: 3252. https://doi.org/10.3390/cancers13133252