
Impact of Neck Dissection in Head and Neck Squamous Cell Carcinomas of Unknown Primary

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Waltonen, J.D.; Ozer, E.; Hall, N.C.; Schuller, D.E.; Agrawal, A. Metastatic Carcinoma of the Neck of Unknown Primary Origin: Evolution and Efficacy of the Modern Workup. Arch. Otolaryngol. Head Neck Surg. 2009, 135, 1024–1029. [Google Scholar] [CrossRef] [Green Version]
- NCCN Clinical Pratice Guidelines in Oncology -Head and Neck Cancers 2018.
- Maghami, E.; Ismaila, N.; Alvarez, A.; Chernock, R.; Duvvuri, U.; Geiger, J.; Gross, N.; Haughey, B.; Paul, D.; Rodriguez, C.; et al. Diagnosis and Management of Squamous Cell Carcinoma of Unknown Primary in the Head and Neck: ASCO Guideline. J. Clin. Oncol. 2020, 38, 2570–2596. [Google Scholar] [CrossRef]
- Bugat, R.; Bataillard, A.; Lesimple, T.; Voigt, J.-J.; Culine, S.; Lortholary, A.; Merrouche, Y.; Ganem, G.; Kaminsky, M.C.; Negrier, S.; et al. Standards, Options and Recommendations for the management of patient with carcinoma of unknown primary site. Bull. Cancer 2002, 89, 869–875. [Google Scholar]
- Mackenzie, K.; Watson, M.; Jankowska, P.; Bhide, S.; Simo, R. Investigation and management of the unknown primary with metastatic neck disease: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S170–S175. [Google Scholar] [CrossRef] [Green Version]
- Troussier, I.; Klausner, G.; Blais, E.; Giraud, P.; Lahmi, L.; Pflumio, C.; Faivre, J.C.; Geoffrois, L.; Babin, E.; Morinière, S.; et al. Évolutions dans la prise en charge des métastases ganglionnaires cervicales sans cancer primitif retrouvé: Doses et volumes cibles de la radiothérapie avec modulation d’intensité. Cancer/Radiothérapie 2018, 22, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Arosio, A.D.; Pignataro, L.; Gaini, R.M.; Garavello, W. Neck lymph node metastases from unknown primary. Cancer Treat. Rev. 2017, 53, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Li, B.-Q.; Farwell, D.G.; Marsano, J.; Vijayakumar, S.; Purdy, J.A. Improved Dosimetric and Clinical Outcomes with Intensity-Modulated Radiotherapy for Head-and-Neck Cancer of Unknown Primary Origin. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 756–762. [Google Scholar] [CrossRef]
- Balaker, A.E.; Abemayor, E.; Elashoff, D.; St John, M.A. Cancer of unknown primary: Does treatment modality make a difference? Laryngoscope 2012, 122, 1279–1282. [Google Scholar] [CrossRef] [PubMed]
- Demiroz, C.; Vainshtein, J.M.; Koukourakis, G.V.; Gutfeld, O.; Prince, M.E.; Bradford, C.R.; Wolf, G.T.; McLean, S.; Worden, F.P.; Chepeha, D.B.; et al. Head and neck squamous cell carcinoma of unknown primary: Neck dissection and radiotherapy or definitive radiotherapy. Head Neck 2014, 36, 1589–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehanna, H.; Kong, A.; Ahmed, S. Recurrent head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S181–S190. [Google Scholar] [CrossRef]
- Patel, R.S.; Clark, J.; Wyten, R.; Gao, K.; O’Brien, C.J. Squamous cell carcinoma from an unknown head and neck primary site: A “selective treatment” approach. Arch. Otolaryngol. Head Neck Surg. 2007, 133, 1282–1287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pflumio, C.; Troussier, I.; Sun, X.S.; Salleron, J.; Petit, C.; Caubet, M.; Beddok, A.; Calugaru, V.; Servagi-Vernat, S.; Castelli, J.; et al. Unilateral or bilateral irradiation in cervical lymph node metastases of unknown primary? A retrospective cohort study. Eur. J. Cancer 2019, 111, 69–81. [Google Scholar] [CrossRef] [PubMed]
- Robbins, K.T.; Shaha, A.R.; Medina, J.E.; Califano, J.A.; Wolf, G.T.; Ferlito, A.; Som, P.M.; Day, T.A.; Committee for Neck Dissection Classification, American Head and Neck Society. Consensus Statement on the Classification and Terminology of Neck Dissection. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 536. [Google Scholar] [CrossRef] [Green Version]
- Blanchard, D.; Barry, B.; De Raucourt, D.; Choussy, O.; Dessard-Diana, B.; Hans, S.; Lafarge, D.; SFORL Work-Group. Guidelines update: Post-treatment follow-up of adult head and neck squamous cell carcinoma: Screening for metastasis and metachronous esophageal and bronchial locations. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2015, 132, 217–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehanna, H.; Wong, W.-L.; McConkey, C.C.; Rahman, J.K.; Robinson, M.; Hartley, A.G.J.; Nutting, C.; Powell, N.; Al-Booz, H.; Robinson, M.; et al. PET-CT Surveillance versus Neck Dissection in Advanced Head and Neck Cancer. N. Engl. J. Med. 2016, 374, 1444–1454. [Google Scholar] [CrossRef]
- Massa, S.T.; Osazuwa-Peters, N.; Christopher, K.M.; Arnold, L.D.; Schootman, M.; Varvares, R.J.W.M.A. Competing causes of death in the head and neck cancer population. Oral Oncol. 2017, 65, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.R. Optimal matching for observational studies. J. Am. Stat. Assoc. 1989, 84, 1024–1032. [Google Scholar] [CrossRef]
- Galloway, T.J.; Ridge, J.A. Management of squamous cancer metastatic to cervical nodes with an unknown primary site. J. Clin. Oncol. 2015, 33, 3328–3337. [Google Scholar] [CrossRef] [PubMed]
- Mani, N.; George, M.M.; Nash, L.; Anwar, B.; Homer, J.J. Role of 18-Fludeoxyglucose positron emission tomography-computed tomography and subsequent panendoscopy in head and neck squamous cell carcinoma of unknown primary. Laryngoscope 2016, 126, 1354–1358. [Google Scholar] [CrossRef]
- Colletier, P.J.; Garden, A.S.; Morrison, W.H.; Goepfert, H.; Geara, F.; Ang, K.K. Postoperative radiation for squamous cell carcinoma metastatic to cervical lymph nodes from an unknown primary site: Outcomes and patterns of failure. Head Neck 1998, 20, 674–681. [Google Scholar] [CrossRef]
- Lou, J.; Wang, S.; Wang, K.; Chen, C.; Zhao, J.; Guo, L. Squamous cell carcinoma of cervical lymph nodes from an unknown primary site: The impact of neck dissection. J. Cancer Res. Ther. 2015, 11 (Suppl. 2), C161–C167. [Google Scholar]
- Amsbaugh, M.J.; Yusuf, M.; Gaskins, J.; Silverman, C.; Potts, K.; Bumpous, J.; Redman, R.; Perez, C.; Dunlap, N. Neck dissection for unknown cancer of the head and neck in the era of chemoradiation. Am. J. Otolaryngol. 2017, 38, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Carsuzaa, F.; Gorphe, P.; Vergez, S.; Malard, O.; Fakhry, N.; Righini, C.; Philouze, P.; Lasne-Cardon, A.; Gallet, P.; Tonnerre, D.; et al. Consensus on resectability in N3 head and neck squamous cell carcinomas: GETTEC recommendations. Oral Oncol. 2020, 106, 104733. [Google Scholar] [CrossRef] [PubMed]
- Aslani, M.; Sultanem, K.; Voung, T.; Hier, M.; Niazi, T.; Shenouda, G. Metastatic carcinoma to the cervical nodes from an unknown head and neck primary site: Is there a need for neck dissection? Head Neck 2007, 29, 585–590. [Google Scholar] [CrossRef]
- Beldì, D.; Jereczek-Fossa, B.A.; D’Onofrio, A.; Gambaro, G.; Fiore, M.R.; Pia, F.; Chiesa, F.; Orecchia, R.; Krengli, M. Role of radiotherapy in the treatment of cervical lymph node metastases from an unknown primary site: Retrospective analysis of 113 patients. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Hauswald, H.; Lindel, K.; Rochet, N.; Debus, J.; Harms, W. Surgery with complete resection improves survival in radiooncologically treated patients with cervical lymph node metastases from cancer of unknown primary. Strahlenther. Onkol. Organ Dtsch. Röntgenges. 2008, 184, 150–156. [Google Scholar] [CrossRef]
- Zhou, M.J.; van Zante, A.; Lazar, A.A.; Groppo, E.R.; Garsa, A.A.; Ryan, W.R.; El-Sayed, I.H.; Eisele, D.W.; Yom, S.S. Squamous cell carcinoma of unknown primary of the head and neck: Favorable prognostic factors comparable to those in oropharyngeal cancer. Head Neck 2017, 40, 904–916. [Google Scholar] [CrossRef]
- Boros, A.; Blanchard, P.; Dade, A.; Gorphe, P.; Breuskin, I.; Even, C.; Nguyen, F.; Deutsch, E.; Bidault, F.; Janot, F.; et al. Outcomes in N3 Head and Neck Squamous Cell Carcinoma and Role of Upfront Neck Dissection. Laryngoscope 2020. [Google Scholar] [CrossRef]
- Thariat, J.; Ang, K.K.; Allen, P.K.; Ahamad, A.; Williams, M.D.; Myers, J.N.; El-Naggar, A.K.; Ginsberg, L.E.; Rosenthal, D.I.; Glisson, B.S.; et al. Prediction of neck dissection requirement after definitive radiotherapy for head-and-neck squamous cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e367–e374. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Barbera, L.; Brouwers, M.; Browman, G.; Mackillop, W.J. Does delay in starting treatment affect the outcomes of radiotherapy? A systematic review. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2003, 21, 555–563. [Google Scholar] [CrossRef]
- Elicin, O.; Albrecht, T.; Haynes, A.G.; Bojaxhiu, B.; Nisa, L.; Caversaccio, M.; Dal Pra, A.; Schmücking, M.; Aebersold, D.M.; Giger, R.; et al. Outcomes in Advanced Head and Neck Cancer Treated with Up-front Neck Dissection prior to (Chemo)Radiotherapy. Otolaryngol. Head Neck Surg. 2016, 154, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, H.; McConkey, C.C.; Rahman, J.K.; Wong, W.L.; Smith, A.F.; Nutting, C.; Hartley, A.G.; Hall, P.; Hulme, C.; Patel, D.K.; et al. PET-NECK: A multicentre randomised Phase III non-inferiority trial comparing a positron emission tomography-computerised tomography-guided watch-and-wait policy with planned neck dissection in the management of locally advanced (N2/N3) nodal metastases in. Health Technol. Assess. 2017, 21, 1–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sokoya, M.; Chowdhury, F.; Kadakia, S.; Ducic, Y. Combination of panendoscopy and positron emission tomography/computed tomography increases detection of unknown primary head and neck carcinoma. Laryngoscope 2018. [Google Scholar] [CrossRef]
- Noij, D.P.; Martens, R.M.; Zwezerijnen, B.; Koopman, T.; de Bree, R.; Hoekstra, O.S.; de Graaf, P.; Castelijns, J.A. Diagnostic value of diffusion-weighted imaging and 18F-FDG-PET/CT for the detection of unknown primary head and neck cancer in patients presenting with cervical metastasis. Eur. J. Radiol. 2018, 107, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Wallis, S.; O’Toole, L.; Karsai, L.; Jose, J. Transoral endoscopic base of tongue mucosectomy for investigation of unknown primary cancers of head and neck. Clin. Otolaryngol. 2018, 43, 1139–1143. [Google Scholar] [CrossRef]
- Winter, S.C.; Ofo, E.; Meikle, D.; Silva, P.; Fraser, L.; O’Hara, J.; Kim, D.; Robinson, M.; Paleri, V. Trans-oral robotic assisted tongue base mucosectomy for investigation of cancer of unknown primary in the head and neck region. UK Exp. Clin. Otolaryngol. 2017, 42, 1247–1251. [Google Scholar] [CrossRef] [Green Version]
- Axelsson, L.; Nyman, J.; Haugen-Cange, H.; Bove, M.; Johansson, L.; de Lara, S.; Kovacs, A.; Hammerlid, E. Prognostic factors for head and neck cancer of unknown primary including the impact of human papilloma virus infection. J. Otolaryngol. Head Neck Surg. 2017, 46, 45. [Google Scholar] [CrossRef]
- Motz, K.; Qualliotine, J.R.; Rettig, E.; Richmon, J.D.; Eisele, D.W.; Fakhry, C. Changes in Unknown Primary Squamous Cell Carcinoma of the Head and Neck at Initial Presentation in the Era of Human Papillomavirus. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 223. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, L.; Boscolo-Rizzo, P.; Dal Cin, E.; Romeo, S.; Baboci, L.; Dyckhoff, G.; Hess, J.; Lucena-Porcel, C.; Byl, A.; Becker, N.; et al. Human papillomavirus as prognostic marker with rising prevalence in neck squamous cell carcinoma of unknown primary: A retrospective multicentre study. Eur. J. Cancer 2017, 74, 73–81. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Neck Dissection Extent | All Patients N = 322 | No ND N = 53 | Adenectomy N = 33 | Selective ND N = 116 | Modified Radical/Radical ND N = 120 | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Patients | ||||||||
| Male | 271 (84.2%) | 48 (90.6%) | 26 (78.8%) | 95 (81.9%) | 102 (85.0%) | 0.414 | ||
| Female | 51 (15.8%) | 5 (9.4%) | 7 (21.2%) | 21 (18.1%) | 18 (15.0%) | |||
| Age (years) | 61.5; 62.3 +/− 10.3 | 62.6; 64.4 +/− 11.4 | 65.6; 64.8 +/− 12.2 | 61.2; 61.0 +/− 9.5 | 61.4; 62.1 +/− 9.9 | 0.330 | ||
| Tumors | ||||||||
| Extension staging, including: | ||||||||
| Head and neck CT | ||||||||
| Head and neck MRI | 303 (94.1%) | 51 (96.3%) | 33 (100.0%) | 108 (93.1%) | 111 (92.5%) | 0.353 | ||
| Chest-abdomn-pelvic | 45 (14%) | 6 (11.3%) | 0 | 24 (20.9%) | 15 (12.5%) | 0.015 | ||
| CT | 175 (56.6%) | 32 (64.0%) | 21 (75.0%) | 62 (54.9%) | 60 (50.9%) | 0.082 | ||
| 18-FDG PET-CT | 265 (82.6%) | 44 (83.0%) | 29 (87.8%) | 99 (85.3%) | 93 (78.2%) | 0.409 | ||
| Nodal stage: | <0.001 | |||||||
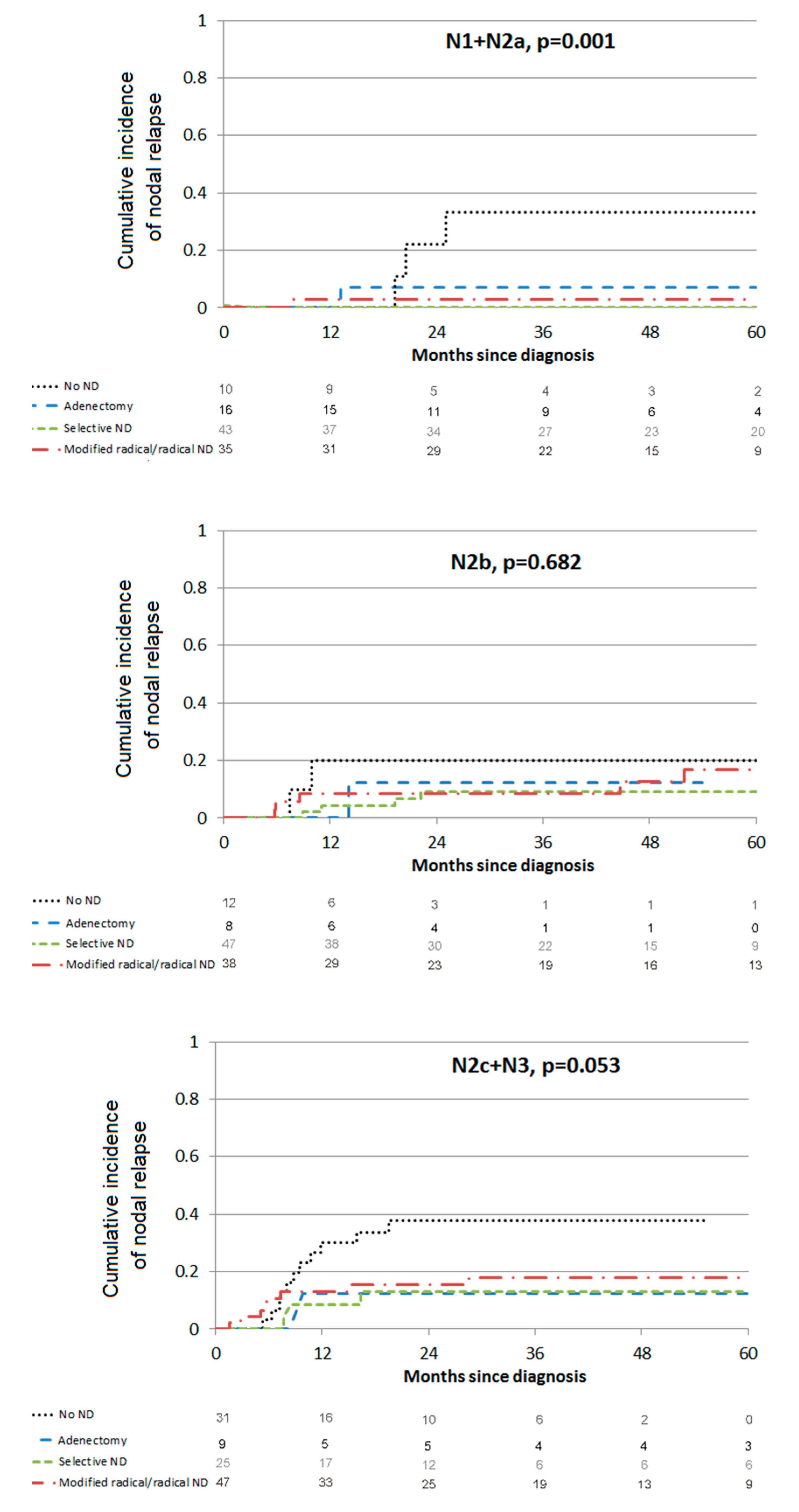
| N1 + N2a | 104 (32.3%) | 10 (18.9%) | 16 (48.5%) | 43 (37.1%) | 35 (29.2%) | |||
| N2b | 106 (32.9%) | 12 (22.6%) | 8 (24.2%) | 48 (41.4%) | 38 (31.7%) | |||
| N2c + N3 | 112 (34.8%) | 31 (58.5%) | 9 (27.3%) | 25 (21.6%) | 47 (39.2%) | |||
| Diameter of largest cervical node (cm) | 4.5; 5.7 +/− 6.1 | 6; 6.5 +/− 3.6 | 4; 8.2 +/− 11.2 | 3.5; 5.6 +/− 7.8 | 5.0; 4.8 +/− 2.0 | <0.001 | ||
| Extracapsular spread a | 209 (71.8%) | 25 (75.8%) | 21 (70.0%) | 74 (64.9%) | 89 (78.1%) | 0.158 | ||
| Conventional squamous cell carcinoma | 316 (98.1%) | 53 (100%) | 33 (100%) | 112 (96.6%) | 118 (98.3%) | 0.354 | ||
| Variant of squamous cell carcinoma | 6 (1.9%) | 0 | 0 | 4 (3.5%) | 2 (1.7%) | |||
| Histological differentiation a | 0.357 | |||||||
| Well differentiated | 120 (43.8%) | 25 (51.1%) | 13 (48.1%) | 46 (46%) | 39 (37.5%) | |||
| Keratinizing | 85 (31%) | 18 (41.9%) | 13 (48.1%) | 28 (28%) | 26 (24.8%) | |||
| Non-keratinizing | 24 (8.8%) | 2 (4.6%) | 0 | 12 (12%) | 10 (9.5%) | |||
| NOS | 11 (4%) | 5 (4.6%) | 0 | 6 (6%) | 3 (2.9%) | |||
| Moderately differentiated | 71 (25.9%) | 9 (20.9%) | 7 (25.9%) | 26 (26%) | 29 (27.9%) | |||
| Poorly differentiated | 76 (27.7%) | 10 (23.4%) | 7 (25.9%) | 25 (25%) | 34 (32.7%) | |||
| Undifferentiated | 7 (2.6%) | 2 (4.6%) | 0 | 3 (3%) | 2 (1.9%) | |||
| HPV status a | − | |||||||
| Positive | 14 (26.4%) | 0 | 1 (100%) | 8 (23.5%) | 5 (31.3%) | |||
| Negative | 39 (73.6%) | 2 (100%) | 0 | 26 (76.5%) | 11 (68.8%) | |||
| Prognostic Analysis by Event | Local Relapse | Nodal Relapse | Metastatic Relapse | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bivariate Analysis | Multivariate Analysis | Bivariate Analysis | Multivariate Analysis | Bivariate Analysis | Multivariate Analysis | |||||||
| HR 95% CI | p-Value | HR 95% CI | p-Value | HR 95% CI | p-Value | HR 95% CI | p-Value | HR 95% CI | p-Value | HR 95% CI | p-Value | |
| Patients | ||||||||||||
| Male gender | 2.34 [0.57; 9.59] | 0.238 | 1.74 [0.62; 4.89] | 0.292 | 1.14 [0.49; 2.67] | 0.755 | ||||||
| Age at diagnosis | 1.04 [0.99; 1.08] | 0.091 | 1.03 [1; 1.06] | 0.066 | 1.04 [1; 1.07] | 0.030 | ||||||
| Tumors | ||||||||||||
| Initial imaging 18-FDG PET-CT | 0.58 [0.25; 1.32] | 0.195 | 0.92 [0.42; 2.05] | 0.844 | 0.46 [0.24; 0.87] | 0.016 | 0.46 [0.24; 0.89] | 0.021 | ||||
| Diameter of largest node (cm) | 1.00 [0.96; 1.04] | 0.910 | 1.03 [0.99; 1.06] | 0.115 | 1.05 [1.03; 1.08] | <0.001 | 1.05 [1.02; 1.08] | <0.001 | ||||
| Nodal staging | ||||||||||||
| N1 + N2a | 1 | 1 | 1 | 1 | 1 | 1 | ||||||
| N2b | 0.79 [0.28; 2.25] | 0.659 | 0.81 [0.28; 2.30] | 0.689 | 2.13 [0.81; 5.57] | 0.124 | 1.90 [0.71; 5.11] | 0.200 | 1.13 [0.5; 2.52] | 0.772 | 0.76 [0.32; 1.80] | 0.536 |
| N2c + N3 | 1.38 [0.57; 3.35] | 0.483 | 1.41 [0.58; 3.43] | 0.448 | 3.89 [1.6; 9.44] | 0.003 | 2.62 [1.06; 6.48] | 0.037 | 1.87 [0.91; 3.84] | 0.089 | 1.57 [0.75; 3.30] | 0.231 |
| Extracapsular spread | 0.98 [0.39; 2.47] | 0.957 | 1.6 [0.7;3.66] | 0.270 | 2.74 [1.08; 6.99] | 0.034 | ||||||
| Treatments | ||||||||||||
| Interval of >10 weeks between diagnosis and start of RT | 2.22 [0.97; 5.05] | 0.058 | 2.04 [1.05; 3.95] | 0.034 | 0.89 [0.49; 1.61] | 0.693 | ||||||
| Interruption RT ≥ 4 days | 1.9 [0.54; 6.74] | 0.320 | 3.76 [1.58; 8.9] | 0.003 | 3.84 [1.71; 8.62] | 0.001 | 1.94 [0.74; 5.08] | 0.177 | ||||
| Neck dissection | ||||||||||||
| No ND | 1 | 1 | 1 | 1 | ||||||||
| Adenectomy | 0.28 [0.03; 2.36] | 0.243 | 0.17 [0.04; 0.75] | 0.019 | 0.20 [0.05; 0.85] | 0.029 | 0.60 [0.19; 1.87] | 0.381 | ||||
| Selective ND | 0.47 [0.163; 1.38] | 0.169 | 0.17 [0.07; 0.4] | <0.001 | 0.20 [0.08; 0.51] | <0.001 | 0.57 [0.27; 1.22] | 0.149 | ||||
| Modified radical/radical ND | 0.71 [0.26; 1.92] | 0.496 | 0.36 [0.18; 0.73] | 0.005 | 0.40 [0.19; 0.83] | 0.015 | 0.57 [0.26; 1.22] | 0.149 | ||||
| Mucosal RT | 0.32 [0.13; 0.76] | 0.010 | 0.32 [0.13; 0.76) | 0.010 | 0.65 [0.29; 1.46] | 0.309 | 0.52 [0.26; 1.07] | 0.076 | ||||
| Chemotherapy | 0.52 [0.24; 1.13] | 0.098 | 1.47 [0.73; 2.93] | 0.279 | 1.67 [0.84; 3.33] | 0.142 | ||||||
| Neoadjuvant chemotherapy | 1.26 [0.38; 4.19] | 0.712 | 2.74 [1.31; 5.7] | 0.007 | 0.87 [0.32; 2.41] | 0.791 | ||||||
| Concomitant chemotherapy | 0.5 [0.23; 1.1] | 0.085 | 1.02 [0.54; 1.94] | 0.941 | 1.49 [0.78; 2.86] | 0.230 | ||||||
| Prognostic Analysis by Event | Progression-Free Survival | HNCUP-Specific Death | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Bivariate Analysis | Multivariate Analysis | Bivariate Analysis | Multivariate Analysis | ||||||
| HR 95% CI | p-Value | HR 95% CI | p-Value | HR 95% CI | p-Value | HR 95% CI | p-Value | ||
| Patients | |||||||||
| Male gender | 1.46 [0.85; 2.51] | 0.174 | 3.82 [1.17;12.45] | 0.026 | |||||
| Age at diagnosis | 1.03 [1.01; 1.05] | 0.001 | 1 [0.98;1.03] | 0.880 | |||||
| Tumors | |||||||||
| Initial imaging including a 18-FDG PET-CT | 0.61 [0.4; 0.92] | 0.017 | 0.56 [0.36; 0.86] | 0.008 | 0.43 [0.25;0.74] | 0.002 | 0.44 [0.24; 0.83] | 0.010 | |
| Diameter of largest node (cm) | 1.03 [1.01;1.06] | 0.009 | 1.06 [1.03;1.08] | <0.001 | 1.06 [1.03; 1.09] | <.001 | |||
| Nodal stage | |||||||||
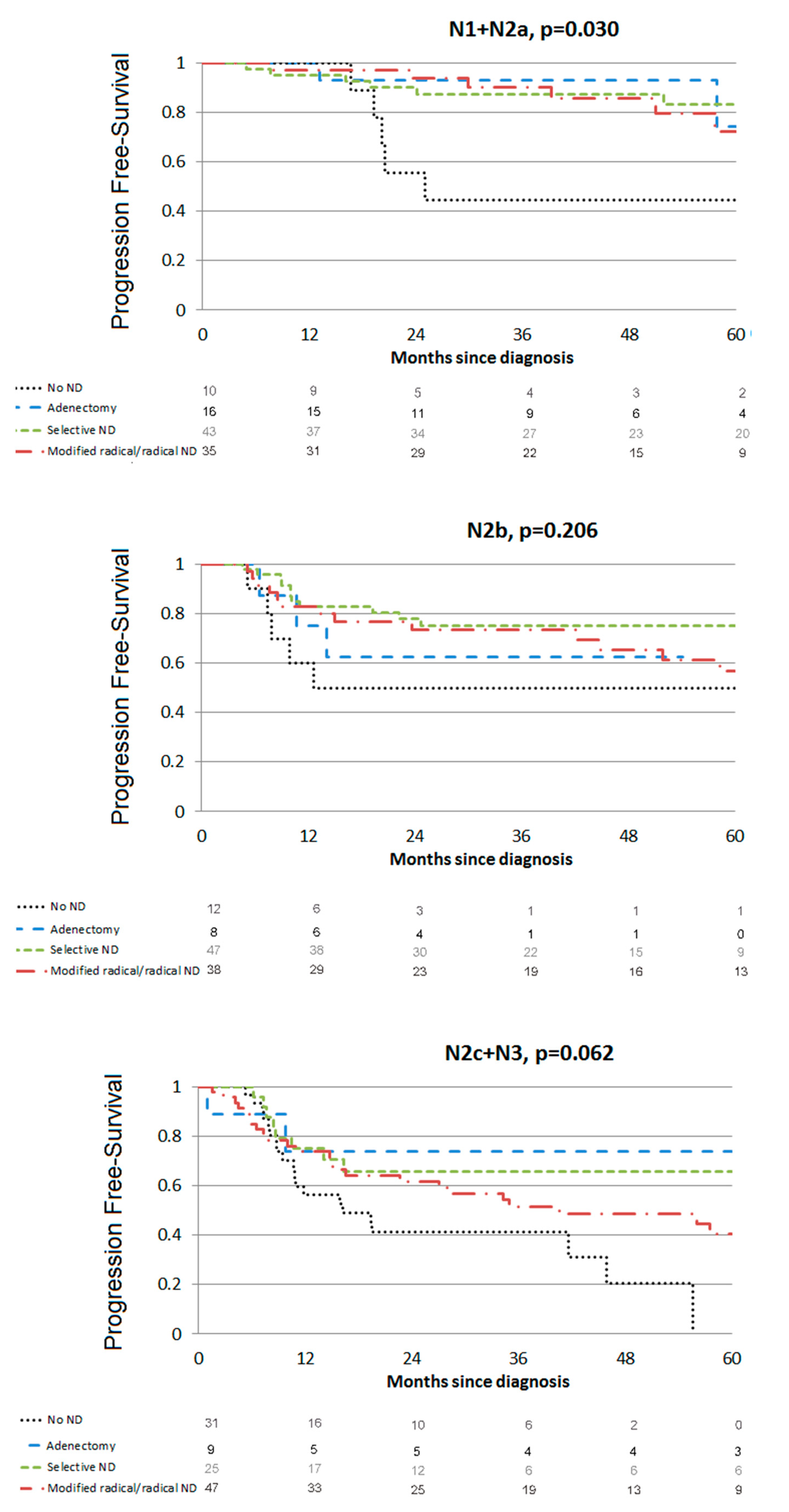
| N1+N2a | 1 | 1 | 1 | 1 | |||||
| N2b | 1.82 [1.09; 3.06] | 0.023 | 1.99 [1.18; 3.36] | 0.010 | 1.61 [0.77; 3.35] | 0.206 | 0.97 [0.41; 2.29] | 0.948 | |
| N2c+N3 | 3.26 [2.02; 5.25] | <0.001 | 3.00 [1.83; 4.92] | <0.001 | 3.65 [1.87; 7.13] | <0.001 | 2.55 [1.2; 5.15] | 0.009 | |
| Extracapsular spread | 2.13 [1.25; 3.63] | 0.006 | 2.18 [1.04; 4.56] | 0.0382 | |||||
| Treatments | |||||||||
| Time lapse between diagnosis and irradiation | 1.25 [0.87; 1.8] | 0.236 | 1.03 [0.62; 1.68] | 0.923 | |||||
| Interruption RT ≥ 4 days | 1.59 [0.84; 3] | 0.155 | 3.31 [1.58; 6.96] | 0.002 | 3.86 [1.75; 8.53] | <0.001 | |||
| Neck dissection | |||||||||
| No ND | 1 | 1 | 1 | ||||||
| Lymphadenectomy | 0.26 [0.11; 0.58] | 0.001 | 0.29 [0.13;0.67] | <0.001 | 0.17 [0.04; 0.78] | 0.022 | |||
| Selective ND | 0.28 [0.17; 0.46] | <0.001 | 0.35 [0.21; 0.59] | <0.001 | 0.40 [0.20; 0.80] | 0.010 | |||
| Modified radical/radical ND | 0.45 [0.29; 0.71] | <0.001 | 0.43 [0.27; 0.69] | <0.001 | 0.50 [0.26; 0.96] | 0.037 | |||
| Mucosal radiotherapy | 0.5 [0.31; 0.81] | 0.005 | 0.41 [0.25; 0.67] | <0.001 | 0.62 [0.32; 1.21] | 0.161 | |||
| Chemotherapy | 1.04 [0.71; 1.52] | 0.838 | 1.11 [0.66; 1.86] | 0.690 | |||||
| Neoadjuvant | 2.01 [1.21; 3.33] | 0.007 | 2.42 [1.2; 4.84] | 0.013 | 2.45 [1.16; 5.18] | 0.018 | |||
| Concomitant | 0.84 [0.58; 1.21] | 0.348 | 0.84 [0.51; 1.39] | 0.502 | |||||
| Neck Dissection Extent | No ND | Adenectomy | Selective ND | Modified Radical ND | Radical ND | p-Value |
|---|---|---|---|---|---|---|
| Acute toxicities | ||||||
| Number of patients | 53 | 33 | 116 | 105 | 15 | |
| Dysphagia | 19(35.8%) | 6(18.2%) | 34 (29.3%) | 24 (22.9%) | 7 (46.7%) | 0.122 |
| Pain | 9(17.3%) | 4(12.1%) | 13 (11.3%) | 14 (13.5%) | 5 (33.3%) | 0.206 |
| Late toxicities | ||||||
| Number of patients | 50 | 31 | 115 | 99 | 15 | |
| Dysphagia | 5(10.0%) | 0 | 6 (5.2%) | 7 (7.1%) | 7 (46.7%) | <0.001 |
| Fibrosis | 0 | 1(3.2%) | 10 (8.7%) | 3 (3%) | 6 (40%) | <0.001 |
| Pain | 2(4.0%) | 0 | 2 (1.7%) | 1 (1%) | 2 (13.3%) | 0.068 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Shama, Y.; Salleron, J.; Carsuzaa, F.; Sun, X.-S.; Pflumio, C.; Troussier, I.; Petit, C.; Caubet, M.; Beddok, A.; Calugaru, V.; et al. Impact of Neck Dissection in Head and Neck Squamous Cell Carcinomas of Unknown Primary. Cancers 2021, 13, 2416. https://doi.org/10.3390/cancers13102416
Abu-Shama Y, Salleron J, Carsuzaa F, Sun X-S, Pflumio C, Troussier I, Petit C, Caubet M, Beddok A, Calugaru V, et al. Impact of Neck Dissection in Head and Neck Squamous Cell Carcinomas of Unknown Primary. Cancers. 2021; 13(10):2416. https://doi.org/10.3390/cancers13102416
Chicago/Turabian StyleAbu-Shama, Yazan, Julia Salleron, Florent Carsuzaa, Xu-Shan Sun, Carole Pflumio, Idriss Troussier, Claire Petit, Matthieu Caubet, Arnaud Beddok, Valentin Calugaru, and et al. 2021. "Impact of Neck Dissection in Head and Neck Squamous Cell Carcinomas of Unknown Primary" Cancers 13, no. 10: 2416. https://doi.org/10.3390/cancers13102416