
Sustained Complete Response after Biological Downstaging in Patients with Hepatocellular Carcinoma: XXL-Like Prioritization for Liver Transplantation or “Wait and See” Strategy?

 ,
,  , , , , and
, , , , and
Abstract
:Simple Summary
Abstract

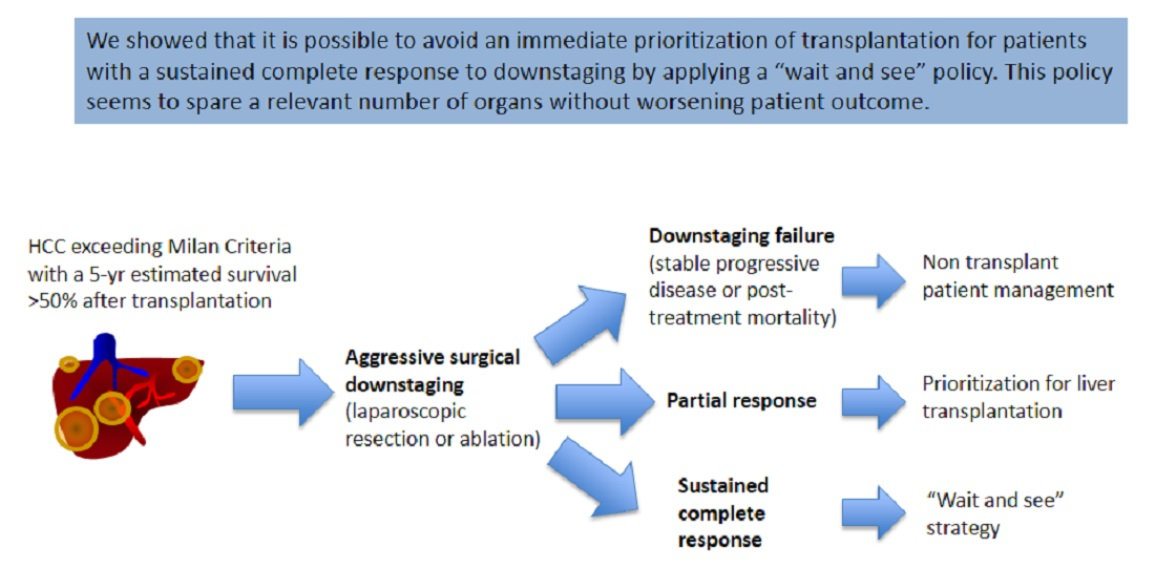
1. Introduction
2. Materials and Methods
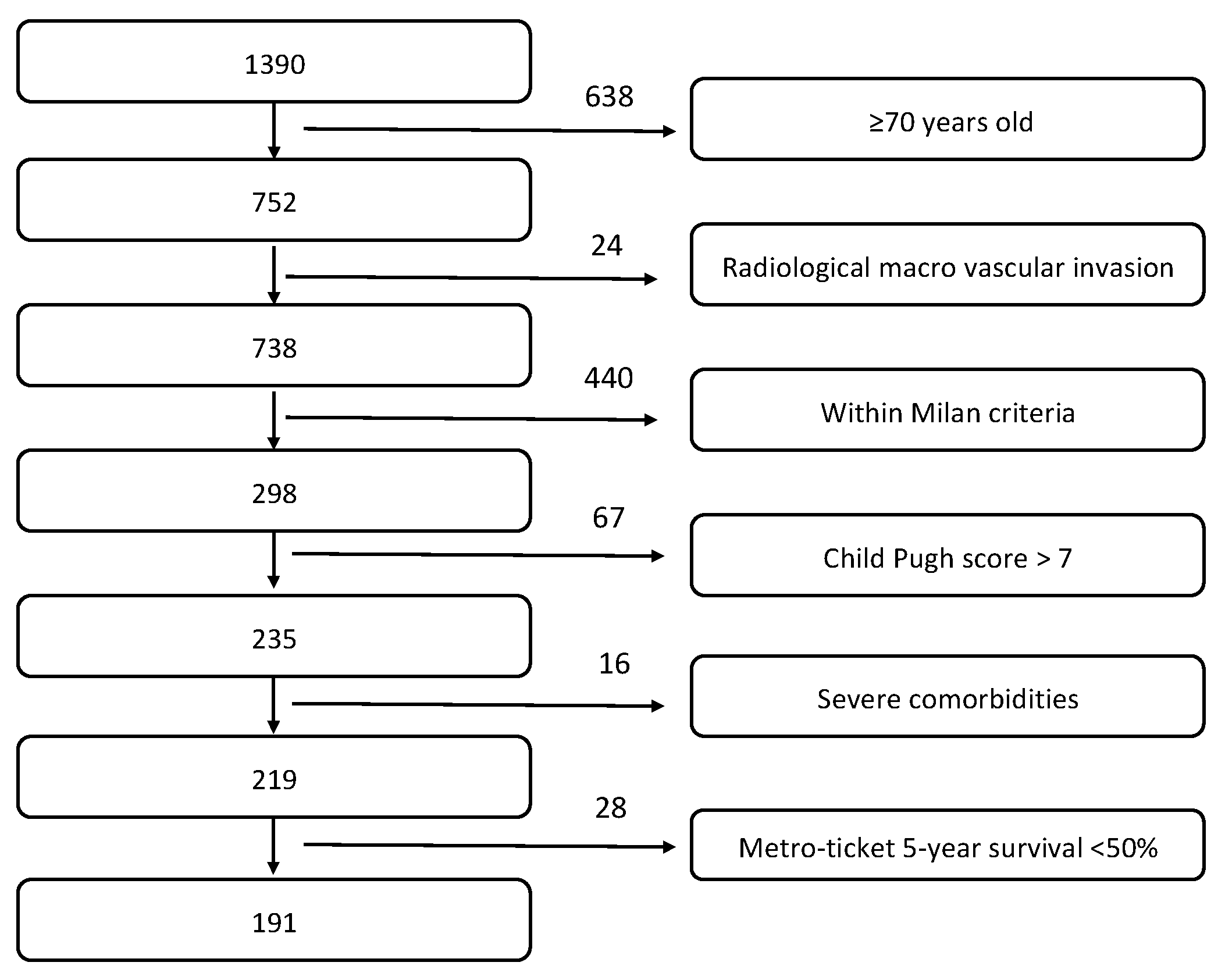
2.1. Patient Enrollment
2.2. Downstaging Protocol
2.3. Study Objectives
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
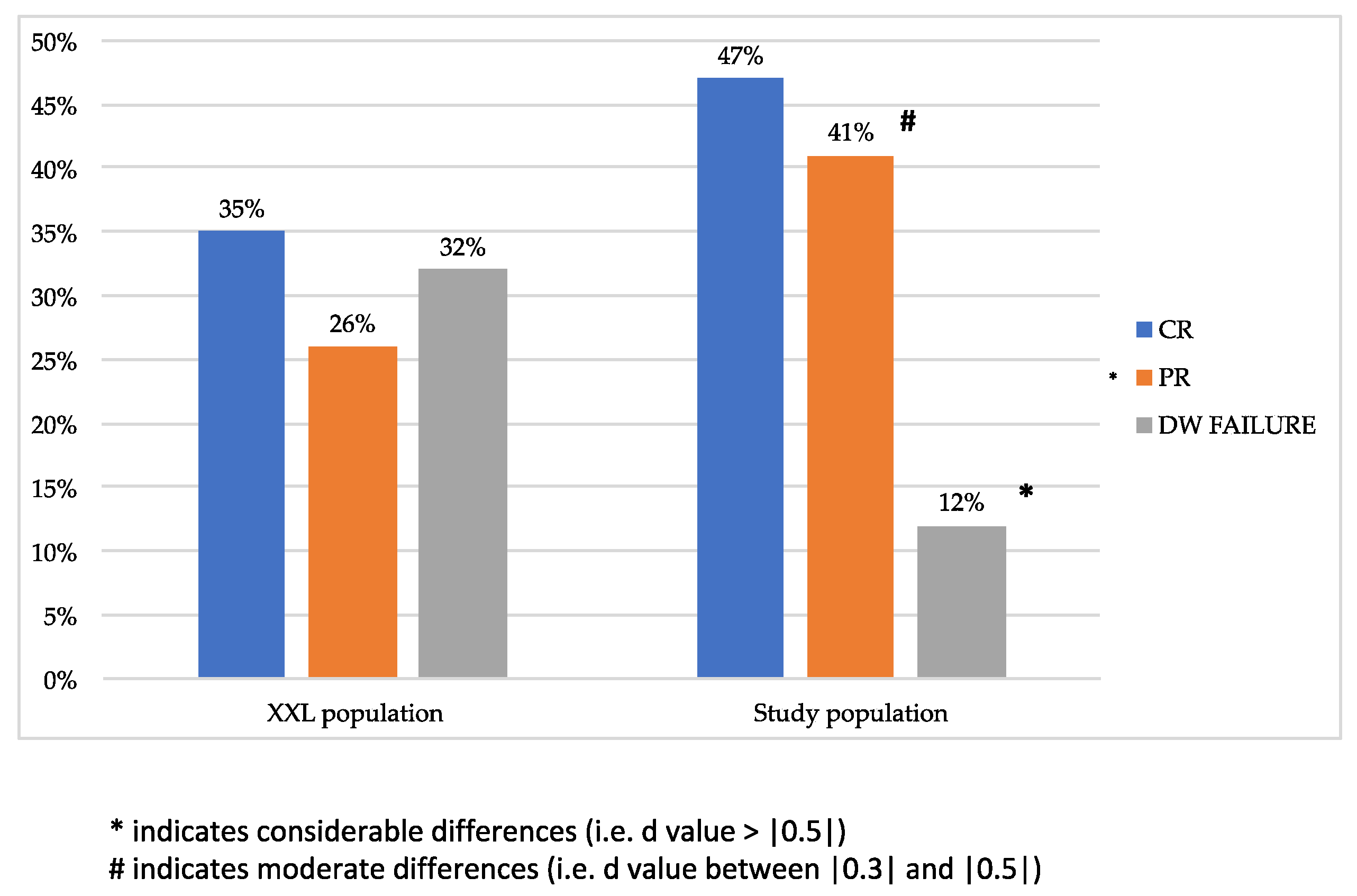
3.2. Effectiveness of Surgical Downstaging
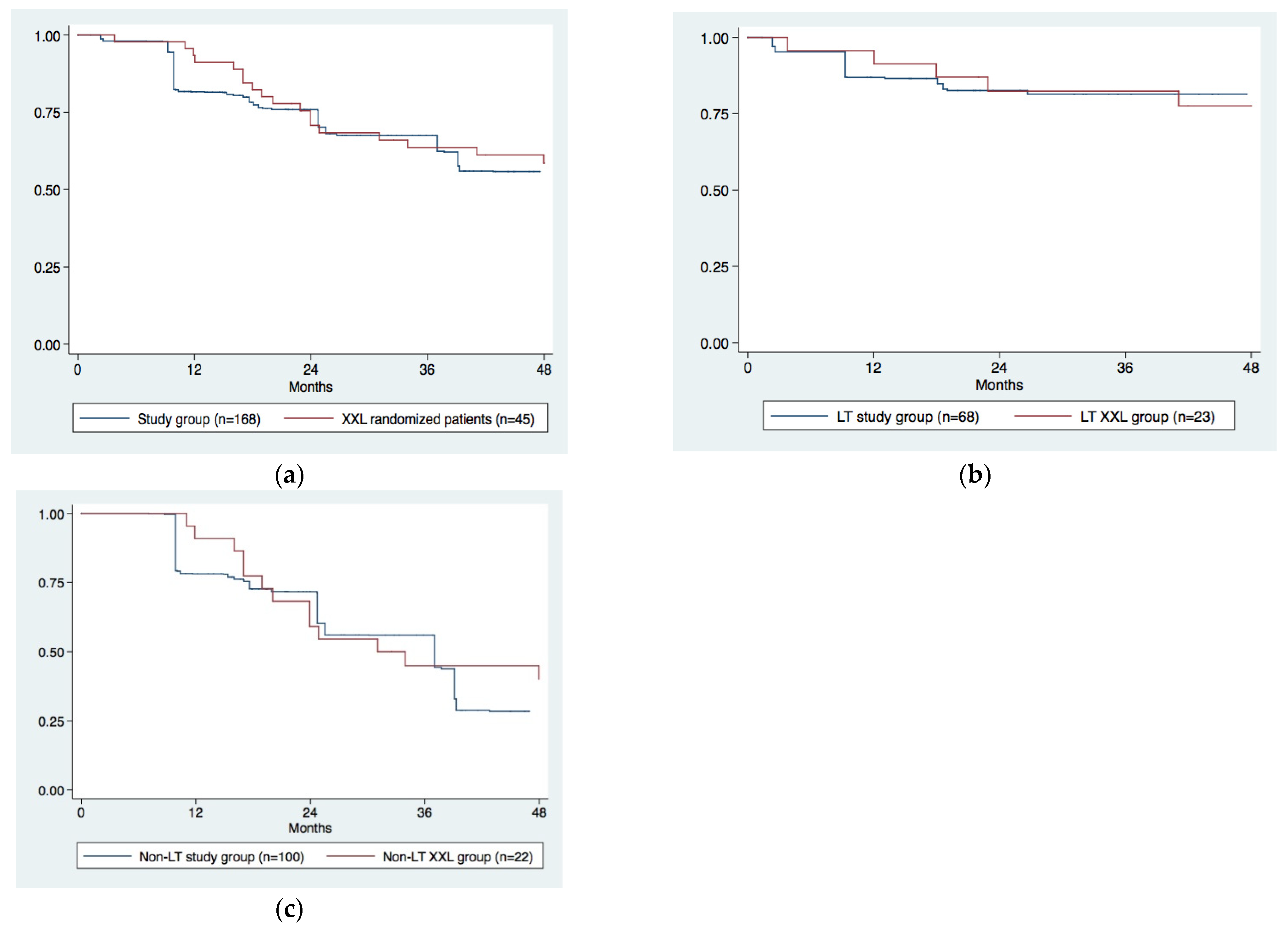
3.3. Survival Analysis
4. Discussion
- Our population was older (61 vs. 56 years): this can be explained by the fact that only patients with age ≤ 65 years were enrolled in the XXL trial [13], although, in the appendix of the same paper (https://ars.els-cdn.com/content/image/1-s2.0-S1470204520302242-mmc1.pdf (accessed on 13 January 2021)), an upper age limit of 69 years was described as the first inclusion criterion (Supplementary Materials);
- There was a higher number of patients undergoing downstaging for a recurrent HCC (51% vs. 14%). This aspect is probably justified by the fact that ours is a tertiary referral center, and a large part of our case history is made up of patients already undergoing nonsurgical loco-regional therapies (intra-arterial therapy and percutaneous ablation) at other centers for which they are no longer eligible.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vitale, A.; Trevisani, F.; Farinati, F.; Cillo, U. Treatment of Hepatocellular Carcinoma in the Precision Medicine Era: From Treatment Stage Migration to Therapeutic Hierarchy. Hepatology 2020, 72, 2206–2218. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Vitale, A.; Volk, M.L.; Frigo, A.C.; Grigoletto, F.; Brolese, A.; Zanus, G.; D’Amico, F.; Farinati, F.; Burra, P.; et al. The survival benefit of liver transplantation in hepatocellular carcinoma patients. Dig. Liver Dis. 2010, 42, 642–649. [Google Scholar] [CrossRef]
- Vitale, A.; Volk, M.; Cillo, U. Transplant benefit for patients with hepatocellular carcinoma. World J. Gastroenterol. 2013, 19, 9183–9188. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Vitale, A.; Polacco, M.; Fasolo, E. Liver transplantation for hepatocellular carcinoma through the lens of transplant benefit. Hepatology 2017, 65, 1741–1748. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, G.N. Transplant -related survival benefit should influence prioritization for liver transplantation especially in patients with hepatocellular carcinoma. Liver Transpl. 2017, 23, 652–662. [Google Scholar] [CrossRef] [Green Version]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Watson, J.J.; Bacchetti, P.; Venook, A.; Ascher, N.L.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: Expansion of the tumor size limits does not adversely impact survival. Hepatology 2001, 33, 1394–1403. [Google Scholar] [CrossRef]
- Sasaki, K.; Firl, D.J.; Hashimoto, K.; Fujiki, M.; Diago-Uso, T.; Quintini, C.; Eghtesad, B.; Fung, J.J.; Aucejo, F.N.; Miller, C.M. Development and validation of the HALT-HCC score to predict mortality in liver transplant recipients with hepatocellular carcinoma: A retrospective cohort analysis. Lancet Gastroenterol. Hepatol. 2017, 2, 595–603. [Google Scholar] [CrossRef]
- León Díaz, F.J.; Pérez Daga, J.A.; Sánchez Pérez, B.; Fernández Aguilar, J.L.; Montiel Casado, C.; Aranda Narváez, J.M.; Suárez Muñoz, M.A.; Romacho López, L.; Santoyo Villalba, J.; Santoyo Santoyo, J. Up-to-7 Criteria for Hepatocellular Carcinoma Liver Transplantation: A Retrospective Analysis of Experiences. Transplant. Proc. 2016, 48, 2969–2972. [Google Scholar] [CrossRef] [PubMed]
- Duvoux, C.; Roudot-Thoraval, F.; Decaens, T.; Pessione, F.; Badran, H.; Piardi, T.; Francoz, C.; Compagnon, P.; Vanlemmens, C.; Dumortier, J.; et al. Liver transplantation for hepatocellular carcinoma: A model including α-fetoprotein improves the performance of Milan criteria. Gastroenterology 2012, 143, 986–994. [Google Scholar] [CrossRef]
- Toso, C.; Mentha, G.; Kneteman, N.M.; Majno, P. The place of downstaging for hepatocellular carcinoma. J. Hepatol. 2010, 52, 930–936. [Google Scholar] [CrossRef]
- Yao, F.Y.; Kerlan, R.K., Jr.; Hirose, R.; Davern, T.J., III; Bass, N.M.; Feng, S.; Peters, M.; Terrault, N.; Freise, C.E.; Ascher, N.L.; et al. Excellent outcome following down-staging of hepatocellular carcinoma prior to liver transplantation: An intention-to-treat analysis. Hepatology 2008, 48, 819–827. [Google Scholar] [CrossRef] [Green Version]
- Ravaioli, M.; Grazi, G.L.; Piscaglia, F.; Trevisani, F.; Cescon, M.; Ercolani, G.; Vivarelli, M.; Golfieri, R.; D’Errico Grigioni, A.; Panzini, I.; et al. Liver transplantation for hepatocellular carcinoma: Results of down-staging in patients initially outside the Milan selection criteria. Am. J. Transplant. 2008, 8, 2547–2557. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Citterio, D.; Bhoori, S.; Bongini, M.; Miceli, R.; De Carlis, L.; Colledan, M.; Salizzoni, M.; Romagnoli, R.; Antonelli, B.; et al. Liver transplantation in hepatocellular carcinoma after tumour downstaging (XXL): A randomised, controlled, phase 2b/3 trial. Lancet Oncol. 2020, 21, 947–956, Erratum in: 2020, 21, e373. [Google Scholar] [CrossRef] [PubMed]
- Farinati, F.; Vanin, V.; Giacomin, A.; Pozzan, C.; Cillo, U.; Vitale, A.; Di Nolfo, A.M.; Del Poggio, P.; Benvegnu’, L.; Rapaccini, G.; et al. BCLC stage B hepatocellular carcinoma and transcatheter arterial chemoembolization: A 20-year survey by the Italian Liver Cancer group. Liver Int. 2015, 35, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Vitale, A.; Dupuis, D.; Corso, S.; Neri, D.; D’Amico, F.; Gringeri, E.; Farinati, F.; Vincenzi, V.; Zanus, G. Laparoscopic ablation of hepatocellular carcinoma in cirrhotic patients unsuitable for liver resection or percutaneous treatment: A cohort study. PLoS ONE 2013, 8, e57249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cillo, U.; Bertacco, A.; Fasolo, E.; Carandina, R.; Vitale, A.; Zanus, G.; Gringeri, E.; D’Amico, F.; Bassi, D.; Neri, D.; et al. Videolaparoscopic microwave ablation in patients with HCC at a European high-volume center: Results of 815 procedures. J. Surg. Oncol. 2019, 120, 956–965. [Google Scholar] [CrossRef] [PubMed]
- Cillo, U.; Noaro, G.; Vitale, A.; Neri, D.; D’Amico, F.; Gringeri, E.; Farinati, F.; Vincenzi, V.; Vigo, M.; Zanus, G.; et al. Laparoscopic microwave ablation in patients with hepatocellular carcinoma: A prospective cohort study. HPB 2014, 16, 979–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cillo, U.; Vitale, A.; Grigoletto, F.; Gringeri, E.; D’Amico, F.; Valmasoni, M.; Brolese, A.; Zanus, G.; Srsen, N.; Carraro, A.; et al. Intention-to-treat analysis of liver transplantation in selected, aggressively treated HCC patients exceeding the Milan criteria. Am J Transplant. 2007, 7, 972–981. [Google Scholar] [CrossRef] [PubMed]
- Vitale, A.; D’Amico, F.; Frigo, A.C.; Grigoletto, F.; Brolese, A.; Zanus, G.; Neri, D.; Carraro, A.; D’Amico, F.E.; Burra, P.; et al. Response to therapy as a criterion for awarding priority to patients with hepatocellular carcinoma awaiting liver transplantation. Ann. Surg. Oncol. 2010, 17, 2290–2302. [Google Scholar] [CrossRef]
- Cillo, U.; Burra, P.; Mazzaferro, V.; Belli, L.; Pinna, A.D.; Spada, M.; Nanni Costa, A.; Toniutto, P.; I-BELT (Italian Board of Experts in the Field of Liver Transplantation). A Multistep, Consensus-Based Approach to Organ Allocation in Liver Transplantation: Toward a “Blended Principle Model”. Am. J. Transplant. 2015, 15, 2552–2561. [Google Scholar] [CrossRef]
- Peng, Y.; Liu, F.; Xu, H.; Wei, Y.; Li, B. Is laparoscopic liver resection suitable for selected patients with BCLC stage B HCC? A propensity score-matched analysis. HPB 2020, 22, 595–602. [Google Scholar] [CrossRef]
- Signorovitch, J.E.; Sikirica, V.; Erder, M.H.; Xie, J.; Lu, M.; Hodgkins, P.S.; Betts, K.A.; Wu, E.Q. Matching-adjusted indirect comparisons: A new tool for timely comparative effectiveness research. Value Health 2012, 15, 940–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnand, B.; Kernan, W.N.; Feinstein, A.R. Indexes and boundaries for “quantitative significance” in statistical decisions. J. Clin. Epidemiol. 1990, 43, 1273–1284. [Google Scholar] [CrossRef]
- Guyot, P.; Ades, A.E.; Ouwens, M.J.; Welton, N.J. Enhanced secondary analysis of survival data: Reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef] [Green Version]
- Ioannou, G.N.; Green, P.K.; Berry, K. HCV eradication induced by direct-acting antiviral agents reduces the risk of hepatocellular carcinoma. J. Hepatol. 2018, 68, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Brancaccio, G.; Vitale, A.; Signoriello, G.; Gaeta, G.B.; Cillo, U. Changing indications for liver transplant: Slow decline of hepatitis viruses in Italy. Infect. Dis. 2020, 52, 557–562. [Google Scholar] [CrossRef]
- Zanetto, A.; Shalaby, S.; Vitale, A.; Mescoli, C.; Ferrarese, A.; Gambato, M.; Franceschet, E.; Germani, G.; Senzolo, M.; Romano, A.; et al. Dropout rate from the liver transplant waiting list because of hepatocellular carcinoma progression in hepatitis C virus–infected patients treated with direct-acting antivirals. Liver Transplant. 2017, 23, 1103–1112. [Google Scholar] [CrossRef]
- Roayaie, S.; Jibara, G.; Tabrizian, P.; Park, J.-W.; Yang, J.; Yan, L.; Schwartz, M.; Han, G.; Izzo, F.; Chen, M.; et al. The role of hepatic resection in the treatment of hepatocellular cancer. Hepatology 2015, 62, 440–451. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Sinn, D.H.; Jung, S.H.; Gwak, G.-Y.; Paik, Y.-H.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Paik, S.W. The recommended treatment algorithms of the BCLC and HKLC staging systems: Does following these always improve survival rates for HCC patients? Liver Int. 2016, 36, 1490–1497. [Google Scholar] [CrossRef] [PubMed]
- Pecorelli, A.; Lenzi, B.; Gramenzi, A.; Garuti, F.; Farinati, F.; Giannini, E.G.; Ciccarese, F.; Piscaglia, F.; Rapaccini, G.L.; Di Marco, M.; et al. Italian Liver Cancer (ITA.LI.CA) group. Curative therapies are superior to standard of care (transarterial chemoembolization) for intermediate stage hepatocellular carcinoma. Liver Int. 2017, 37, 423–433. [Google Scholar] [CrossRef]
- Belli, G.; Fantini, C.; D’Agostino, A.; Cioffi, L.; Langella, S.; Russolillo, N.; Belli, A. Laparoscopic versus open liver resection for hepatocellular carcinoma in patients with histologically proven cirrhosis: Short- and middle-term results. Surg. Endosc. 2017, 21, 2004–2011. [Google Scholar] [CrossRef]
- Kardashian, A.; Florman, S.S.; Haydel, B.; Ruiz, R.M.; Klintmalm, G.B.; Lee, D.D.; Taner, C.B.; Aucejo, F.; Tevar, A.D.; Humar, A.; et al. Liver Transplantation Outcomes in a U.S. Multicenter Cohort of 789 Patients with Hepatocellular Carcinoma Presenting Beyond Milan Criteria. Hepatology 2020, 72, 2014–2028. [Google Scholar] [CrossRef]
- Mehta, N.; Dodge, J.L.; Grab, J.D.; Yao, F.Y. National Experience on Down-Staging of Hepatocellular Carcinoma Before Liver Transplant: Influence of Tumor Burden, Alpha-Fetoprotein, and Wait Time. Hepatology 2020, 71, 943–954. [Google Scholar] [CrossRef] [PubMed]
- Lai, Q.; Vitale, A.; Halazun, K.; Iesari, S.; Viveiros, A.; Bhangui, P.; Mennini, G.; Wong, T.; Uemoto, S.; Lin, C.-C.; et al. Identification of an upper limit of tumor burden for downstaging in candidates with hepatocellular cancer waiting for liver transplantation: A west–east collaborative effort. Cancers 2020, 12, 452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cillo, U.; Giuliani, T.; Polacco, M.; Manley, L.M.H.; Crivellari, G.; Vitale, A. Prediction of hepatocellular carcinoma biological behavior in patient selection for liver transplantation. World J. Gastroenterol. 2016, 22, 232–252. [Google Scholar] [CrossRef] [PubMed]
- Giannini, E.G.; Aglitti, A.; Borzio, M.; Gambato, M.; Guarino, M.; Iavarone, M.; Lai, Q.; Sandri, G.B.L.; Melandro, F.; Morisco, F.; et al. Overview of immune checkpoint inhibitors therapy for hepatocellular carcinoma, and the ITA.LI.ca cohort derived estimate of amenability rate to immune checkpoint inhibitors in clinical practice. Cancers 2019, 11, 1689. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Procedure | First Treatment n (%) | Other Therapies n (%) |
|---|---|---|
| Resection ± laparoscopic ablation | 71 (37%) | 7 (4%) |
| Laparoscopic ablation | 113 (59%) | 12 (6%) |
| Laparotomic ablation | 4 (2%) | 2 (1%) |
| Percutaneus ablation | 3 (2%) | 10 (5%) |
| Intra-arterial therapies | - | 62 (32%) |
| Total | 191 | 93 |
| Characteristics | Raw Population (n = 191) | Study Population (n = 191) | XXL Population (n = 74) |
|---|---|---|---|
| Age >56 years old | 145 (76%) * | 95 (50%) | 37 (50%) |
| Female sex | 32 (17%) * | 13 (7%) | 5 (7%) |
| BMI | 26 (18–38) | 26 (18–38) | 26 (19–33) |
| HCV | 89 (47%) # | 125 (66%) | 49 (66%) |
| HBV | 41 (22%) | 31 (16%) | 12 (16%) |
| Alcohol/dysmetabolic | 42 (22%) | 20 (11%) | 11 (15%) |
| MELD score | 8 (6–21) | 8 (6–21) | 8 (6–17) |
| Child–Pugh class B | 50 (26%) * | 23 (12%) | 9 (12%) |
| CRPH * | 80 (42%) | 95 (50%) | 37 (50%) |
| First HCC diagnosis | 95 (49%) * | 167 (88%) | 64 (86%) |
| No. of nodules | 3 (1–10) | 3 (1–10) | 3.5 (1–9) |
| Diameter of the largest nodule (mm) | 40 (10–80) | 40 (10–80) | 41.5 (12–80) |
| Sum of diameters (mm) | 70 (26–200) | 70 (26–200) | 75.5 (13–155) |
| Tumor burden | 7 (5–13) | 7 (5–13) | 7.3 (5.2–13) |
| AFP <13 ng/mL | 103 (54%) | 95 (50%) | 37 (50%) |
| BCLC stage B | 158 (83%) | 162 (85%) | 63 (85%) |
| Up-to-78 out | 101 (53%) | 104 (55%) | 41 (55%) |
| UCSF criteria out | 124 (65%) | 104 (55%) | 41 (55%) |
| French Model9 high risk (>2 points) | 109 (57%) | 97 (51%) | 38 (51%) |
| HALT-HCC score ≥17 | 60 (32%) * | 1 (1%) | 0 (0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitale, A.; Scolari, F.; Bertacco, A.; Gringeri, E.; D’Amico, F.; Bassi, D.; D’Amico, F.E.; Angeli, P.; Burra, P.; Lai, Q.; et al. Sustained Complete Response after Biological Downstaging in Patients with Hepatocellular Carcinoma: XXL-Like Prioritization for Liver Transplantation or “Wait and See” Strategy? Cancers 2021, 13, 2406. https://doi.org/10.3390/cancers13102406
Vitale A, Scolari F, Bertacco A, Gringeri E, D’Amico F, Bassi D, D’Amico FE, Angeli P, Burra P, Lai Q, et al. Sustained Complete Response after Biological Downstaging in Patients with Hepatocellular Carcinoma: XXL-Like Prioritization for Liver Transplantation or “Wait and See” Strategy? Cancers. 2021; 13(10):2406. https://doi.org/10.3390/cancers13102406
Chicago/Turabian StyleVitale, Alessandro, Federica Scolari, Alessandra Bertacco, Enrico Gringeri, Francesco D’Amico, Domenico Bassi, Francesco Enrico D’Amico, Paolo Angeli, Patrizia Burra, Quirino Lai, and et al. 2021. "Sustained Complete Response after Biological Downstaging in Patients with Hepatocellular Carcinoma: XXL-Like Prioritization for Liver Transplantation or “Wait and See” Strategy?" Cancers 13, no. 10: 2406. https://doi.org/10.3390/cancers13102406