
The Role of Pathological Method and Clearance Definition for the Evaluation of Margin Status after Pancreatoduodenectomy for Periampullary Cancer. Results of a Multicenter Prospective Randomized Trial

 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
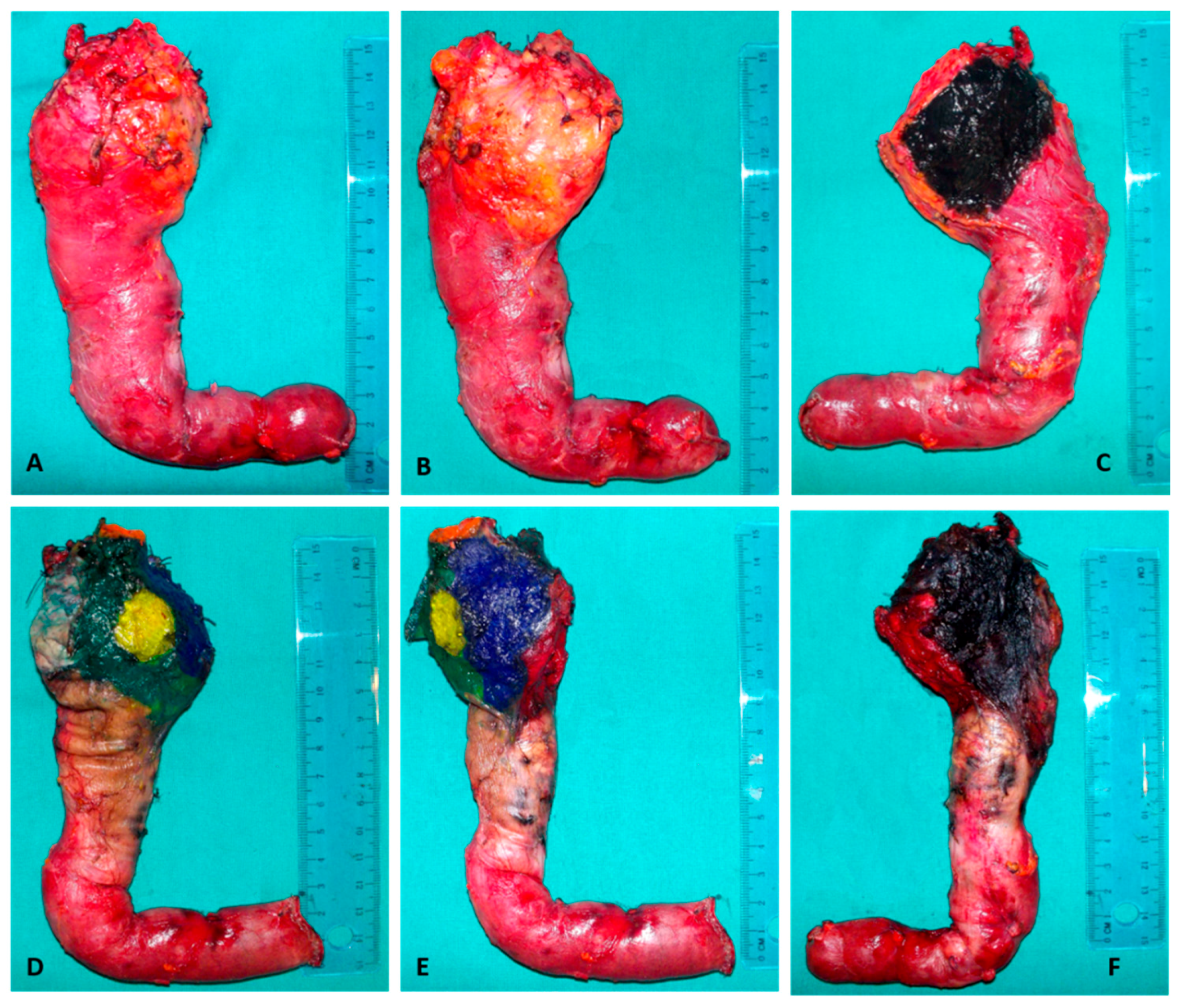
2.1. Randomization and Methods of Pathological Evaluation
2.2. Study End-Points and Data Collection
2.3. Sample Size Calculation and Statistical Analysis
3. Results
3.1. Impact of Method of Pathological Evaluation and Clearance on R1 Rate
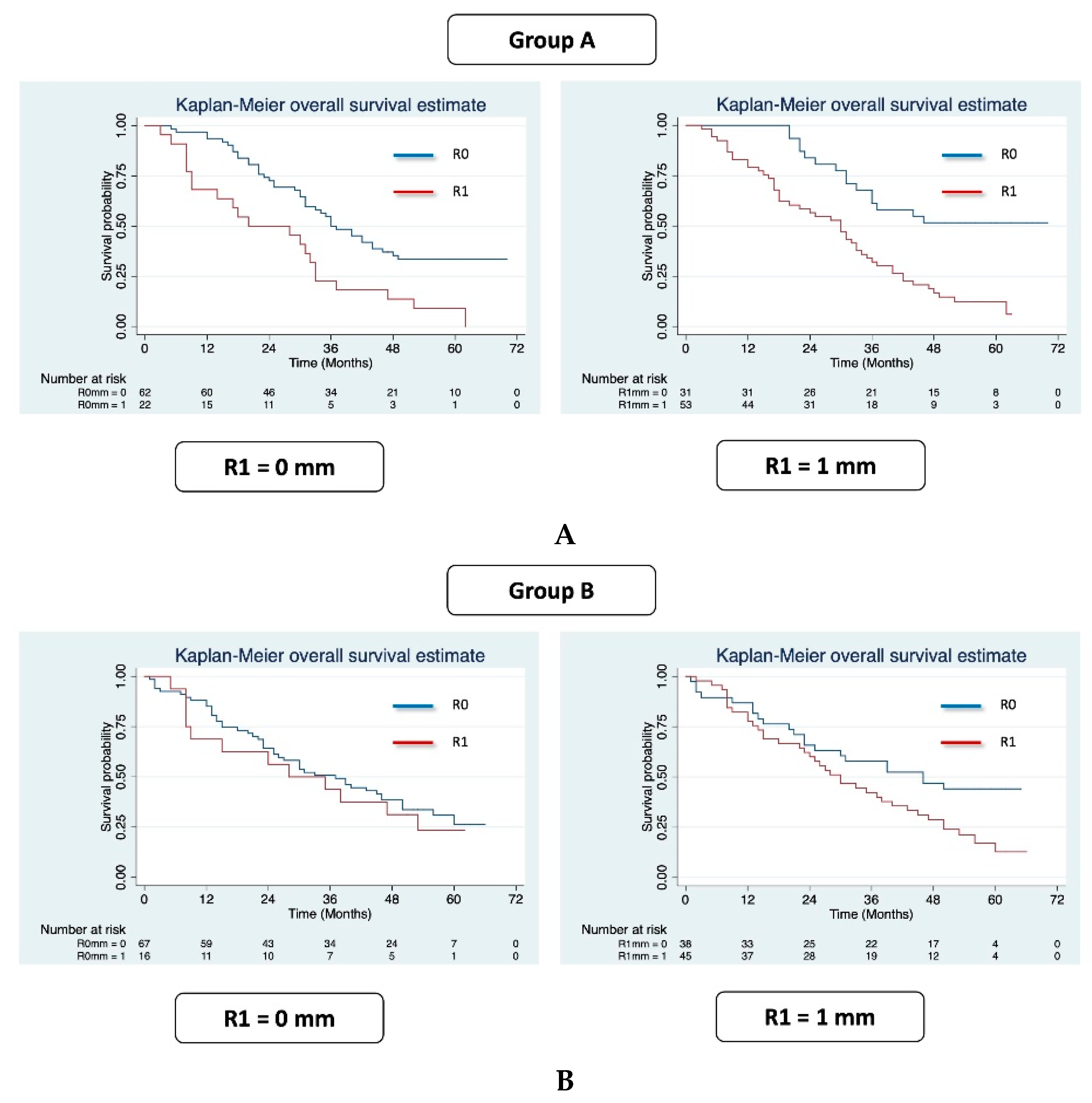
3.2. Prognostic Role of R1 Resection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rau, B.M.; Moritz, K.; Schuschan, S.; Alsfasser, G.; Prall, F.; Klar, E. R1 resection in pancreatic cancer has significant impact on long-term outcome in standardized pathology modified for routine use. Surgery 2012, 152, S103–S111. [Google Scholar] [CrossRef]
- Fatima, J.; Schnelldorfer, T.; Barton, J.; Wood, C.M.; Wiste, H.J.; Smyrk, T.C.; Zhang, L.; Sarr, M.G.; Nagorney, D.M.; Farnell, M.B. Pancreatoduodenectomy for ductal adenocarcinoma: Implications of positive margin on survival. Arch. Surg. 2010, 145, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamieson, N.B.; Denley, S.M.; Logue, J.; MacKenzie, D.J.; Foulis, A.K.; Dickson, E.J.; Imrie, C.W.; Carter, R.; McKay, C.J.; McMillan, D.C. A Prospective Comparison of the Prognostic Value of Tumor-and Patient-Related Factors in Patients Undergoing Potentially Curative Surgery for Pancreatic Ductal Adenocarcinoma. Ann. Surg. Oncol. 2011, 18, 2318–2328. [Google Scholar] [CrossRef] [PubMed]
- Richter, A.; Niedergethmann, M.; Sturm, J.W.; Lorenz, D.; Post, S.; Trede, M. Long-term results of partial pancreaticoduodenectomy for ductal adeno-carcinoma of the pancreatic head: 25-year experience. World J. Surg. 2003, 27, 324–329. [Google Scholar] [CrossRef]
- Sperti, C.; Pasquali, C.; Piccoli, A.; Pedrazzoli, S. Recurrence after resection for ductal adenocarcinoma of the pancreas. World J. Surg. 1997, 21, 195–200. [Google Scholar] [CrossRef]
- Verbeke, C.S.; Leitch, D.; Menon, K.V.; McMahon, M.J.; Guillou, P.J.; Anthoney, A. Redefining the R1 resection in pancreatic cancer. BJS 2006, 93, 1232–1237. [Google Scholar] [CrossRef] [PubMed]
- The Royal College of Pathologists. Standards and Minimun Datasets for Reporting Cancers. Minimum Dataset for the Histopathological Reporting of Pancreatic, Ampulla of Vater and Bile Duct Carcinoma; The Royal College of Pathologists: London, UK, 2002. [Google Scholar]
- Liszka, Ł.; Pająk, J.; Zielińska-Pająk, E.; Gołka, D.; Mrowiec, S.; Lampe, P. Different approaches to assessment of lymph nodes and surgical margin status in patients with ductal adenocarcinoma of the pancreas treated with pancreaticoduodenectomy. Pathology 2010, 42, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, M.A.; Maksymov, V.; Rowsell, C.H.; Hanna, S. A novel approach to the intraoperative assessment of the uncinate margin of the pancreaticoduodenectomy specimen. HPB 2007, 9, 146–149. [Google Scholar] [CrossRef] [Green Version]
- Esposito, I.; Kleej, J.; Bergmann, F.; Reiser, C.; Herpel, E.; Friess, H.; Schirmacher, P.; Büchler, M.V. Most pancreatic cancer resections are R1 resections. Ann. Surg. Oncol. 2008, 15, 1651–1660. [Google Scholar] [CrossRef]
- Adsay, N.V.; Basturk, O.; Saka, B.; Bagci, P.; Ozdemir, D.; Balci, S.; Sarmiento, J.M.; Kooby, D.A.; Staley, C.; Maithel, S.K.; et al. Whipple Made Simple For Surgical Pathologists. Am. J. Surg. Pathol. 2014, 38, 480–493. [Google Scholar] [CrossRef] [Green Version]
- Rosai, J. Rosai and Ackerman’s Surgical Pathology, 9th ed.; Mosby: Edinburgh, UK, 2004. [Google Scholar]
- Soer, E.; Brosens, L.; Van De Vijver, M.; Dijk, F.; Van Velthuysen, M.L.; Fariña-Sarasqueta, A.; Morreau, H.; Offerhaus, J.; Koens, L.; Verheij, J. Dilemmas for the pathologist in the oncologic assessment of pancreatoduodenectomy specimens. Virchows Arch. Pathol. Anat. Physiol. Klin. Med. 2018, 472, 533–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konstantinidis, I.T.; Warshaw, A.L.; Allen, J.N.; Blaszkowsky, L.S.; Castillo, C.F.; Deshpande, V.; Hong, T.S.; Kwak, E.L.; Lauwers, G.Y.; Ryan, D.P.; et al. Pancreatic ductal adenocarcinoma: Is there a survival difference for R1 resections versus locally advanced unresectable tumors? What is a ‘True’ R0 resection? Ann. Surg. 2013, 257, 731–736. [Google Scholar] [CrossRef]
- Strobel, O.; Hank, T.; Hinz, U.; Bergmann, F.; Schneider, L.; Springfeld, C.; Jäger, D.; Schirmacher, P.; Hackert, T.; Büchler, M.W. Pancreatic cancer surgery: The new R-status counts. Pancreatology 2016, 16, S75. [Google Scholar] [CrossRef]
- Jamieson, N.B.; Chan, N.I.J.; Foulis, A.K.; Dickson, E.J.; McKay, C.J.; Carter, C.R. The prognostic influence of resection margin clearance following pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. J. Gastrointest. Surg. 2013, 17, 511–521. [Google Scholar] [CrossRef]
- Butturini, G.; Stocken, D.D.; Wente, M.N.; Jeekel, H.; Klinkenbijl, J.H.G.; Bakkevold, K.E.; Takada, T.; Amano, H.; Dervenis, C.; Bassi, C.; et al. Influence of resection margins and treatment on survival in patients with pancreatic cancer: Meta-analysis of randomized controlled trials. Arch. Surg. 2008, 143, 75–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delpero, J.R.; Jeune, F.; Bachellier, P.; Regenet, N.; Le Treut, Y.P.; Paye, F.; Carrere, N.; Sauvanet, A.; Adham, M.; Autret, A.; et al. Prognostic Value of Resection Margin Involvement After Pancreaticoduodenectomy for Ductal Adenocarcinoma Updates from a French Prospective Multicenter Study. Ann. Surg. 2017, 266, 787–796. [Google Scholar] [CrossRef]
- World Health Organization Classification of Tumor Editorial Board. WHO Classification of Tumors: Digestive System Tumor, 5th ed.; World Health Organization: Geneva, Switzerland, 2019; Volume 1. [Google Scholar]
- Amin, M.B.; Edge, S.B. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- National Comprehensive Cancer Network. NCCN Guidelines. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx (accessed on 18 March 2021).
- Eckel, F.; Jelic, S. Biliary cancer: ESMO Clinical Recommendation for diagnosis, treatment and follow-up. Ann. Oncol. 2009, 20, iv46–iv48. [Google Scholar] [CrossRef]
- Pine, J.K.; Haugk, B.; Robinson, S.M.; Darne, A.; Wilson, C.; Sen, G.; French, J.J.; White, S.A.; Manas, D.M.; Charnley, R.M. Prospective assessment of resection margin status following pancreaticoduodenectomy for pancreatic ductal adenocarcinoma after standardization of margin definitions. Pancreatology 2020, 20, 537–544. [Google Scholar] [CrossRef]
- Takahashi, D.; Kojima, M.; Sugimoto, M.; Kobayashi, S.; Takahashi, S.; Konishi, M.; Gotohda, N.; Nagino, M. Pathologic Evaluation of Surgical Margins in Pancreatic Cancer Specimens Using Color Coding with Tissue Marking Dyes. Pancreas 2018, 47, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Hartwig, W.; Hackert, T.; Hinz, U.; Gluth, A.; Bergmann, F.; Strobel, O.; Büchler, M.W.; Werner, J. Pancreatic cancer surgery in the new millennium: Better prediction of outcome. Ann. Surg. 2011, 254, 311–319. [Google Scholar] [CrossRef] [Green Version]
- Royal College of Pathologists of Australasia. Cancer of the Exocrine Pancreas, Ampulla of Vater and Distal Common Bile Duct. Structured Reporting Protocol, 1st ed.; Royal College of Pathologists of Australasia: Surry Hills, Australia, 2014. [Google Scholar]
- Chang, D.K.; Johns, A.L.; Merrett, N.D.; Gill, A.J.; Colvin, E.K.; Scarlett, C.J.; Nguyen, N.Q.; Leong, R.W.; Cosman, P.H.; Kelly, M.I.; et al. Margin Clearance and Outcome in Resected Pancreatic Cancer. J. Clin. Oncol. 2009, 27, 2855–2862. [Google Scholar] [CrossRef]
- Bockhorn, M.; Uzunoglu, F.G.; Adham, M.; Imrie, C.; Milicevic, M.; Sandberg, A.A.; Asbun, H.J.; Bassi, C.; Büchler, M.; Charnley, R.M.; et al. Borderline resectable pancreatic cancer: A consensus statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2014, 1556, 977–988. [Google Scholar] [CrossRef] [PubMed]
- Demir, I.E.; Jäger, C.; Schlitter, A.M.; Konukiewitz, B.; Stecher, L.; Schorn, S.; Tieftrunk, E.; Scheufele, F.; Calavrezos, L.; Schirren, R.; et al. R0 Versus R1 Resection Matters after Pancreaticoduodenectomy, and Less after Distal or Total Pancreatectomy for Pancreatic Cancer. Ann. Surg. 2018, 268, 1058–1068. [Google Scholar] [CrossRef] [PubMed]
- Van Roessel, S.; Soer, E.C.; Van Dieren, S.; Koens, L.; van Velthuysen, M.L.F.; Doukas, M.; Koerkamp, B.G.; Sarasqueta, A.F.; Bronkhorst, C.M.; Raicu, G.M.; et al. Axial slicing versus bivalving in the pathological examination of pancre-atoduodenectomy specimens (APOLLO): A multicentre randomized controlled trial. HPB Oxf 2021. Online Ahead of Print. [Google Scholar] [CrossRef] [PubMed]
- Borzomati, D.; Perrone, G.; Nappo, G.; Valeri, S.; Amato, M.; Petitti, T.; Muda, A.O.; Coppola, R. Microscopic residual tumour after pancreaticoduodenectomy: Is standardization of pathological examination worthwhile? Pancreas 2016, 45, 748–754. [Google Scholar] [CrossRef]
- Tummers, W.S.; Groen, J.V.; Mulder, B.G.S.; Farina-Sarasqueta, A.; Morreau, J.; Putter, H.; Van De Velde, C.J.; Vahrmeijer, A.L.; Bonsing, B.A.; Mieog, J.S.; et al. Impact of resection margin status on recurrence and survival in pancreatic cancer surgery. BJS 2019, 106, 1055–1065. [Google Scholar] [CrossRef] [Green Version]
- McIntyre, C.A.; Zambrinis, C.P.; Pulvirenti, A.; Chou, J.F.; Gonen, M.; Balachandran, V.P.; Kingham, T.P.; D’Angelica, M.I.; Brennan, M.F.; Drebin, J.A.; et al. Detailed analysis of margin positivity and the site of local recurrence after pancreaticoduodenectomy. Ann. Surg. Oncol. 2020. Epub Ahead of Print. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LEEPP (Group A) (N. 84) | “Conventional” Protocol (Group B) (N. 84) | p | |
|---|---|---|---|
| Gender: | 0.21 | ||
| (a) male, n. (%) | 48 (57%) | 40 (52%) | |
| (b) female, n. (%) | 36 (42%) | 44 (47%) | |
| Age, mean years (range) | 67.5 (33–84) | 67.3 (38–85) | 0.87 |
| Neo-adjuvant treatment, n. (%) | 7 (8.3%) | 5 (5.9%) | 0.38 |
| Type of surgery: | 0.83 | ||
| (a) Classical Whipple, n. (%) | 13 (15%) | 14 (17%) | |
| (b) PPPD, n. (%) | 71 (85%) | 70 (83%) | |
| Vascular resection, n. (%) | 16 (19%) | 17 (20%) | 0.84 |
| Histological type: | 0.06 | ||
| (a) PDAC, n. (%) | 55 (66%) | 68 (81%) | |
| (b) AC, n. (%) | 20 (23%) | 9 (10%) | |
| (c) DC, n. (%) | 9 (11%) | 7 (8%) | |
| Histological grade: | 0.62 | ||
| (a) Gx, n. (%) | 6 (7.14%) | 6 (7.14%) | |
| (b) G1, n. (%) | 2 (2.38%) | 6 (7.14%) | |
| (c) G2, n. (%) | 40 (47.62%) | 39 (46.43%) | |
| (d) G3, n. (%) | 35 (41.67%) | 31 (36.90%) | |
| (e) G4, n. (%) | 1 (1.19%) | 2 (2.38%) | |
| Tumor size, mean cm (range) | 2.67 (0.4–5.5) | 2.97 (1–7) | 0.04 |
| T staging: | 0.12 | ||
| (a) Tis, n. (%) | 1 (1.2%) | 0 (0%) | |
| (b) T1, n. (%) | 2 (2.4%) | 2 (3.6%) | |
| (c) T2, n. (%) | 10 (11.9%) | 2 (2.4%) | |
| (d) T3, n. (%) | 65 (77.5%) | 75 (88.1%) | |
| (e) T4, n. (%) | 6 (7.1%) | 5 (5.9%) | |
| N staging: | 0.25 | ||
| (a) N0, n. (%) | 15 (17.9%) | 21 (25.0%) | |
| (b) N+, n. (%) | 69 (82.1%) | 63 (75.0%) | |
| Vascular invasion, n. (%) | 44 (52.4%) | 48 (57.1%) | 0.53 |
| Lymphatic invasion, n. (%) | 32 (38.1%) | 32 (38.1%) | 0.99 |
| Perineural invasion, n. (%) | 67 (79.8%) | 66 (78.6%) | 0.84 |
| N. of retrieved LN, mean (range) | 39.7 (12–97) | 29.5 (5–97) | 0.01 |
| N. of metastatic LN, mean (range) | 4.7 (0–29) | 4.3 (0–25) | 0.71 |
| N. of blocks, mean (range) | 49.8 (20–95) | 35.9 (13–109) | <0.01 |
| Adjuvant treatment, n. (%) | 67 (79.7%) | 58 (69.8%) | 0.12 |
| Minimum Clearance | R1 Resection (%) (Group A) | R1 Resection (%) (Group B) | p |
|---|---|---|---|
| Entire cohort: | |||
| (a) 0 mm, n. (%) | 22 (26.2%) | 17 (20.2%) | 0.36 |
| (b) 1 mm, n. (%) | 51 (60.7%) | 48 (57.1%) | 0.27 |
| PDAC * | |||
| (a) 0 mm, n. (%) | 18 (32.7%) | 16 (23.5%) | 0.25 |
| (b) 1 mm, n. (%) | 44 (80.0%) | 43 (63.2%) | 0.42 |
| DC: | |||
| (a) 0 mm, n. (%) | 1 (11.1%) | 1 (14.3%) | 0.84 |
| (b) 1 mm, n. (%) | 5 (55.5%) | 1 (14.3%) | 0.09 |
| AC: | |||
| (a) 0 mm, n. (%) | 3 (15.0%) | 0 (0%) | 0.22 |
| (b) 1 mm, n. (%) | 2 (20.0%) | 4 (22.2%) | 0.89 |
| Group A | Group B | |||||
|---|---|---|---|---|---|---|
| R0 Resection | R1 Resection | p | R0 Resection | R1 Resection | p | |
| LR * (0 mm), n. (%) | 15 (24.2%) | 7 (31.8%) | 0.48 | 18 (26.9%) | 4 (25.0%) | 0.87 |
| LR * (1 mm), n. (%) | 6 (19.2%) | 16 (30.1%) | 0.27 | 11 (28.9%) | 11 (24.4%) | 0.64 |
| A. Multivariate analyses for group A according to the different minimum clearance | ||||
| Group A (R1 Clearance = 0 mm) | Group A (R1 Clearance = 1 mm) | |||
| HR | p-Value | HR | p-Value | |
| Age | 1.00 (0.97–1.04) | 0.709 | 0.99 (0.96–1.03) | 0.749 |
| Sex female | 1.33 (0.78–2.27) | 0.297 | 1.44 (0.82–1.53) | 0.197 |
| PDAC vs.: | ||||
| DCC | 0.61 (0.22–1.68) | 0.340 | 0.72 (0.26–1.99) | 0.528 |
| AC | 0.44 (0.17–1.16) | 0.099 | 0.67 (0.24–1.79) | 0.421 |
| Neoadjuvant treatment | 0.31 (0.08–1.15) | 0.080 | 0.27 (0.78–1.12) | 0.074 |
| Adjuvant treatment | 0.15 (0.06–0.39) | 0.0001 | 0.17 (0.06–0.42) | 0.0001 |
| pT3–pT4 | 1.69 (0.26–10.99) | 0.581 | 1.70 (0.28–10.47) | 0.568 |
| N+ | 2.08 (0.93–4.68) | 0.076 | 1.62 (0.73–3.59) | 0.237 |
| G3–G4 | 1.09 (0.58–2.06) | 0.779 | 1.34 (0.72–2.51) | 0.356 |
| Vascular invasion | 2.16 (1.16–4.03) | 0.015 | 1.99 (1.06–3.71) | 0.031 |
| Perineural invasion | 1.31 (0.23–7.52) | 0.762 | 0.92 (0.16–5.32) | 0.929 |
| R1 | 2.19 (1.20–4.00) | 0.011 | 3.35 (1.40–8.00) | 0.007 |
| B. Multivariate analyses for group B according to the different minimum clearance. | ||||
| Group B (R1 Clearance) = 0 mm | Group B (R1 Clearance) = 1 mm | |||
| HR | p-Value | HR | p-Value | |
| Age | 1.02 (0.99–1.05) | 0.170 | 1.02 (0.99–1.05) | 0.223 |
| Sex female | 1.89 (1.03–3.46) | 0.039 | 1.88 (1.04–3.40) | 0.037 |
| PDAC vs.: | ||||
| DCC | 1.25 (0.44–3.55) | 0.672 | 1.81 (0.59–5.51) | 0.297 |
| AC | 0.13 (0.03–0.51) | 0.003 | 0.19 (0.05–0.78) | 0.021 |
| Neoadjuvant treatment | 1.47 (0.38–5.58) | 0.574 | 1.68 (0.44–6.42) | 0.760 |
| Adjuvant treatment | 0.21 (0.11–0.43) | 0.0001 | 0.21 (0.10–0.42) | 0.0001 |
| pT3–pT4 | 0.80 (0.10–6.39) | 0.838 | 1.05 (0.13–8.25) | 0.963 |
| N+ | 1.86 (0.66–5.17) | 0.238 | 1.53 (0.56–4.20) | 0.407 |
| G3–G4 | 1.11 (0.56–2.21) | 0.766 | 0.97 (0.49–1.90) | 0.929 |
| Vascular invasion | 1.51 (0.77–2.98) | 0.227 | 1.34 (0.68–2.64) | 0.392 |
| Perineural invasion | 0.41 (0.17–0.97) | 0.044 | 0.39 (0.16–0.95) | 0.039 |
| R1 | 0.88 (0.43–1.80) | 0.729 | 1.96 (0.96–4.01) | 0.066 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nappo, G.; Borzomati, D.; Zerbi, A.; Spaggiari, P.; Boggi, U.; Campani, D.; Mrowiec, S.; Liszka, Ł.; Coppola, A.; Amato, M.; et al. The Role of Pathological Method and Clearance Definition for the Evaluation of Margin Status after Pancreatoduodenectomy for Periampullary Cancer. Results of a Multicenter Prospective Randomized Trial. Cancers 2021, 13, 2097. https://doi.org/10.3390/cancers13092097
Nappo G, Borzomati D, Zerbi A, Spaggiari P, Boggi U, Campani D, Mrowiec S, Liszka Ł, Coppola A, Amato M, et al. The Role of Pathological Method and Clearance Definition for the Evaluation of Margin Status after Pancreatoduodenectomy for Periampullary Cancer. Results of a Multicenter Prospective Randomized Trial. Cancers. 2021; 13(9):2097. https://doi.org/10.3390/cancers13092097
Chicago/Turabian StyleNappo, Gennaro, Domenico Borzomati, Alessandro Zerbi, Paola Spaggiari, Ugo Boggi, Daniela Campani, Sławomir Mrowiec, Łukasz Liszka, Alessandro Coppola, Michela Amato, and et al. 2021. "The Role of Pathological Method and Clearance Definition for the Evaluation of Margin Status after Pancreatoduodenectomy for Periampullary Cancer. Results of a Multicenter Prospective Randomized Trial" Cancers 13, no. 9: 2097. https://doi.org/10.3390/cancers13092097