
Intersection of DNA Repair Pathways and the Immune Landscape Identifies PD-L2 as a Prognostic Marker in Epithelial Ovarian Cancer


 , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Tissue Microarrays
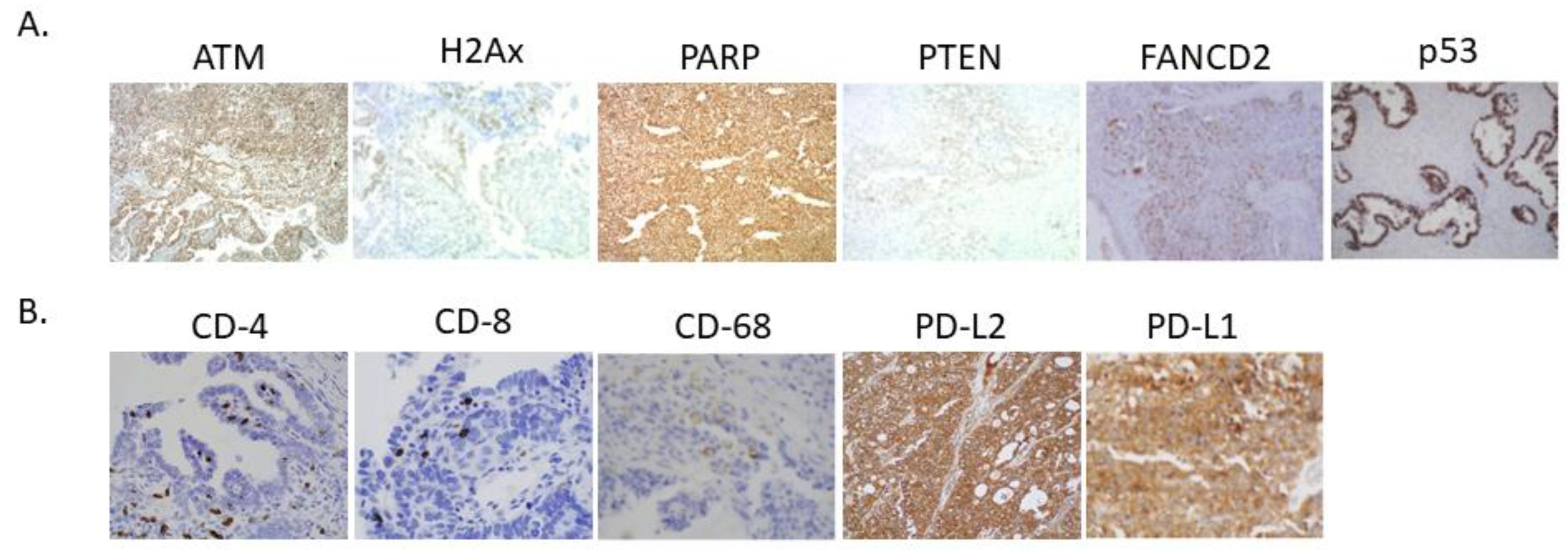
2.3. Immunohistochemistry Assay and Scoring Criteria
2.4. Study Definition
2.5. Statistical Analyses
3. Results
3.1. Study Population and Cohort Characteristics
3.2. Biomarker Correlations
3.3. Survival Statistics
3.4. Prognostic Biomarkers
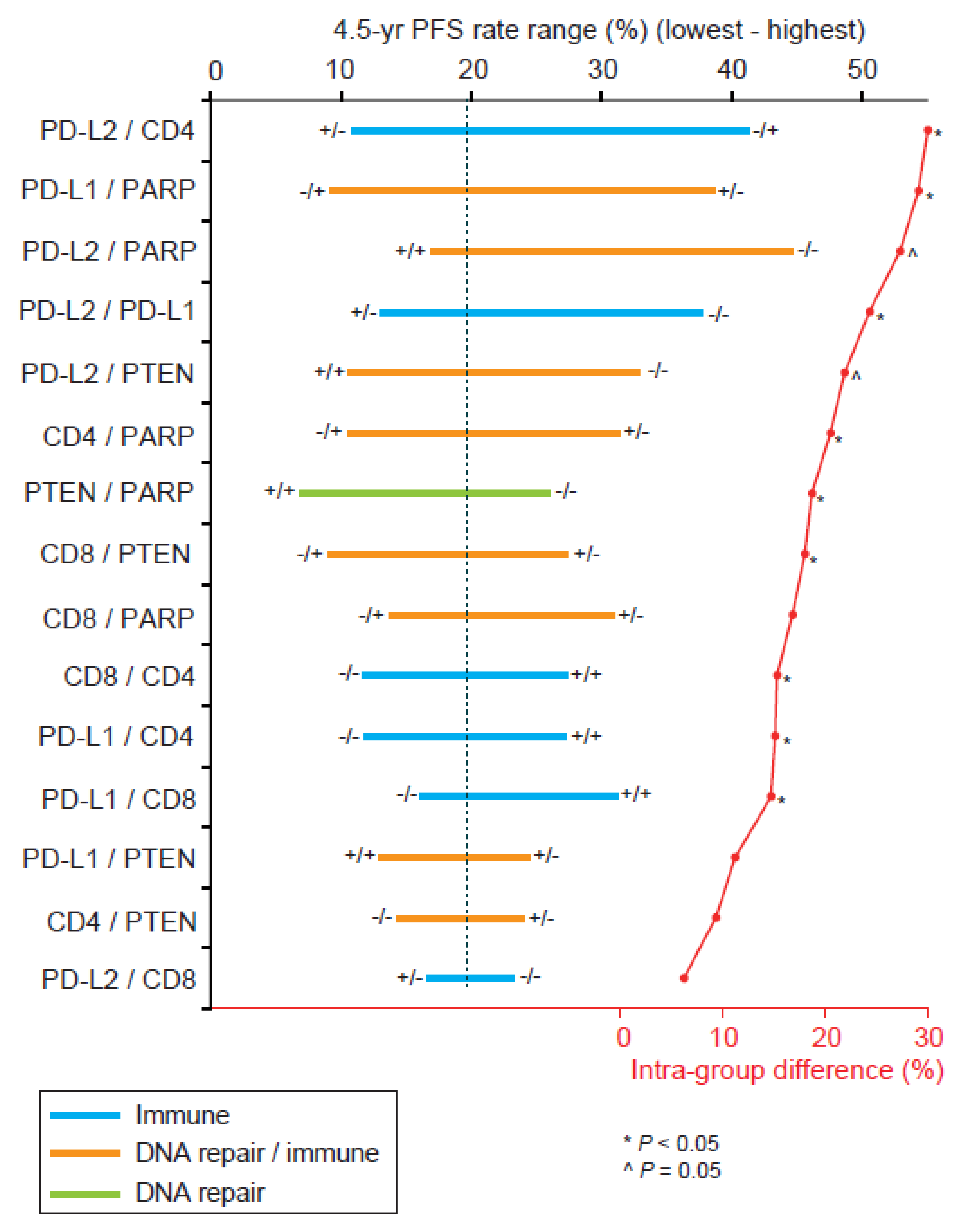
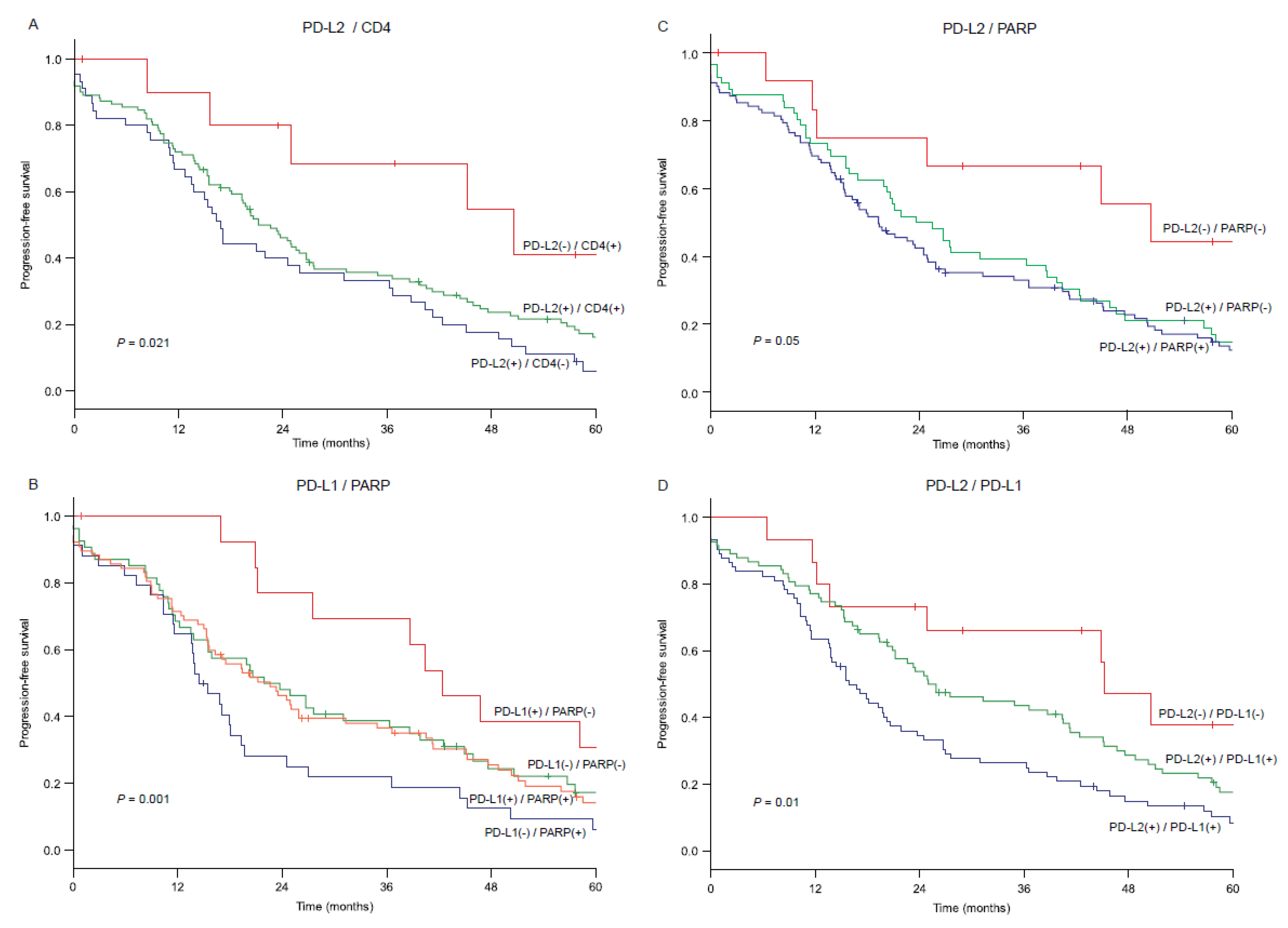
3.5. Biomarker Combination Patterns and Survival Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aoki, D.; Chiyoda, T. PARP inhibitors and quality of life in ovarian cancer. Lancet Oncol. 2018, 19, 1012–1014. [Google Scholar] [CrossRef]
- FDA Approves Niraparib for First-Line Maintenance of Advanced Ovarian Cancer. Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-niraparib-first-line-maintenance-advanced-ovarian-cancer (accessed on 15 April 2021).
- Chatterjee, J.; Dai, W.; Aziz, N.H.A.; Teo, P.Y.; Wahba, J.; Phelps, D.L.; Maine, C.J.; Whilding, L.M.; Dina, R.; Trevisan, G.; et al. Clinical use of programmed cell death-1 and its ligand expression as discriminatory and predictive markers in ovarian cancer. Clin. Cancer Res. 2017, 23, 3453–3460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.; Wei, S.; Hurt, E.M.; Green, M.D.; Zhao, L.; Vatan, L.; Szeliga, W.; Herbst, R.; Harms, P.W.; Fecher, L.A.; et al. Host expression of PD-L1 determines efficacy of PD-L1 pathway blockade-mediated tumor regression. J. Clin. Investig. 2018, 128, 1708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Flies, D.B. Molecular mechanisms of T cell co-stimulation and co-inhibition. Nat. Rev. Immunol. 2013, 13, 227–242. [Google Scholar] [CrossRef]
- Latchman, Y.; Wood, C.R.; Chernova, T.; Chaudhary, D.; Borde, M.; Chernova, I.; Iwai, Y.; Long, A.J.; Brown, J.A.; Nunes, R.; et al. PD-L2 is a second ligand for PD-1 and inhibits T cell activation. Nat. Immunol. 2001, 2, 261–268. [Google Scholar] [CrossRef]
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef] [Green Version]
- Liang, S.C.; Latchman, Y.E.; Buhlmann, J.E.; Tomczak, M.F.; Horwitz, B.H.; Freeman, G.J.; Sharpe, A.H. Regulation of PD-1, PD-L1, and PD-L2 expression during normal and autoimmune responses. Eur. J. Immunol. 2003, 33, 2706–2716. [Google Scholar] [CrossRef]
- Rozali, E.N.; Hato, S.V.; Robinson, B.W.; Lake, R.A.; Lesterhuis, W.J. Programmed death ligand 2 in cancer-induced immune suppression. Clin. Dev. Immunol. 2012, 2012, 656340. [Google Scholar] [CrossRef] [PubMed]
- Odunsi, K.; Pejovic, T. Immune checkpoint and poly(ADP-Ribose) polymerase inhibition for recurrent platinum-resistant ovarian and metastatic triple-negative breast cancers. JAMA Oncol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Meinhold-Heerlein, I.; Fotopoulou, C.; Harter, P.; Kurzeder, C.; Mustea, A.; Wimberger, P.; Hauptmann, S.; Sehouli, J. The new WHO classification of ovarian, fallopian tube, and primary peritoneal cancer and its clinical implications. Arch. Gynecol. Obstet. 2016, 293, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Kononen, J.; Bubendorf, L.; Kallioniemi, A.; Barlund, M.; Schraml, P.; Leighton, S.; Torhorst, J.; Mihatsch, M.J.; Sauter, G.; Kallioniemi, O.P. Tissue microarrays for high-throughput molecular profiling of tumor specimens. Nat. Med. 1998, 4, 844–847. [Google Scholar] [CrossRef]
- Hope, E.R.; Mhawech-Fauceglia, P.; Pejovic, T.; Zahn, C.M.; Wang, G.; Conrads, T.P.; Larry Maxwell, G.; Hamilton, C.A.; Darcy, K.M.; Syed, V. Nestin: A biomarker of aggressive uterine cancers. Gynecol. Oncol. 2016, 140, 503–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wysham, W.Z.; Mhawech-Fauceglia, P.; Li, H.; Hays, L.; Syriac, S.; Skrepnik, T.; Wright, J.; Pande, N.; Hoatlin, M.; Pejovic, T. BRCAness profile of sporadic ovarian cancer predicts disease recurrence. PLoS ONE 2012, 7, e30042. [Google Scholar] [CrossRef] [Green Version]
- Malpica, A.; Deavers, M.T.; Lu, K.; Bodurka, D.C.; Atkinson, E.N.; Gershenson, D.M.; Silva, E.G. Grading ovarian serous carcinoma using a two-tier system. Am. J. Surg. Pathol. 2004, 28, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Jiao, S.; Xia, W.; Yamaguchi, H.; Wei, Y.; Chen, M.K.; Hsu, J.M.; Hsu, J.L.; Yu, W.H.; Du, Y.; Lee, H.H.; et al. PARP Inhibitor Upregulates PD-L1 Expression and Enhances Cancer-Associated Immunosuppression. Clin. Cancer Res. 2017, 23, 3711–3720. [Google Scholar] [CrossRef] [Green Version]
- Shen, J.; Zhao, W.; Ju, Z.; Wang, L.; Peng, Y.; Labrie, M.; Yap, T.A.; Mills, G.B.; Peng, G. PARPi triggers the STING-dependent immune response and enhances the therapeutic efficacy of immune checkpoint blockade independent of BRCAness. Cancer Res. 2019, 79, 311–319. [Google Scholar] [CrossRef] [Green Version]
- Konstantinopoulos, P.A.; Waggoner, S.; Vidal, G.A.; Mita, M.; Moroney, J.W.; Holloway, R.; Van Le, L.; Sachdev, J.C.; Chapman-Davis, E.; Colon-Otero, G.; et al. Single-arm phases 1 and 2 trial of niraparib in combination with pembrolizumab in patients with recurrent platinum-resistant ovarian carcinoma. JAMA Oncol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Farkkila, A.; Gulhan, D.C.; Casado, J.; Jacobson, C.A.; Nguyen, H.; Kochupurakkal, B.; Maliga, Z.; Yapp, C.; Chen, Y.A.; Schapiro, D.; et al. Immunogenomic profiling determines responses to combined PARP and PD-1 inhibition in ovarian cancer. Nat. Commun. 2020, 11, 1459. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Conejo-Garcia, J.R.; Katsaros, D.; Gimotty, P.A.; Massobrio, M.; Regnani, G.; Makrigiannakis, A.; Gray, H.; Schlienger, K.; Liebman, M.N.; et al. Intratumoral T cells, recurrence, and survival in epithelial ovarian cancer. N. Engl. J. Med. 2003, 348, 203–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, E.; Olson, S.H.; Ahn, J.; Bundy, B.; Nishikawa, H.; Qian, F.; Jungbluth, A.A.; Frosina, D.; Gnjatic, S.; Ambrosone, C.; et al. Intraepithelial CD8+ tumor-infiltrating lymphocytes and a high CD8+/regulatory T cell ratio are associated with favorable prognosis in ovarian cancer. Proc. Natl. Acad. Sci. USA 2005, 102, 18538–18543. [Google Scholar] [CrossRef] [Green Version]
- Clarke, B.; Tinker, A.V.; Lee, C.H.; Subramanian, S.; van de Rijn, M.; Turbin, D.; Kalloger, S.; Han, G.; Ceballos, K.; Cadungog, M.G.; et al. Intraepithelial T cells and prognosis in ovarian carcinoma: Novel associations with stage, tumor type, and BRCA1 loss. Mod. Pathol. 2009, 22, 393–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, M.P.; Balmaceda, C.; Bravo, M.L.; Kato, S.; Villarroel, A.; Owen, G.I.; Roa, J.C.; Cuello, M.A.; Ibanez, C. Patient inflammatory status and CD4+/CD8+ intraepithelial tumor lymphocyte infiltration are predictors of outcomes in high-grade serous ovarian cancer. Gynecol. Oncol. 2018, 151, 10–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanske, M.; Wienert, S.; Castillo-Tong, D.C.; Kreuzinger, C.; Vergote, I.; Lambrechts, S.; Gabra, H.; Gourley, C.; Ganapathi, R.N.; Kolaschinski, I.; et al. Dynamics of the intratumoral immune response during progression of high-grade serous ovarian cancer. Neoplasia 2018, 20, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Bachmayr-Heyda, A.; Aust, S.; Heinze, G.; Polterauer, S.; Grimm, C.; Braicu, E.I.; Sehouli, J.; Lambrechts, S.; Vergote, I.; Mahner, S.; et al. Prognostic impact of tumor infiltrating CD8+ T cells in association with cell proliferation in ovarian cancer patients--a study of the OVCAD consortium. BMC Cancer 2013, 13, 422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piao, J.; Lim, H.J.; Lee, M. Prognostic value of programmed cell death ligand-1 expression in ovarian cancer: An updated meta-analysis. Obstet. Gynecol. Sci. 2020, 63, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Ohigashi, Y.; Sho, M.; Yamada, Y.; Tsurui, Y.; Hamada, K.; Ikeda, N.; Mizuno, T.; Yoriki, R.; Kashizuka, H.; Yane, K.; et al. Clinical significance of programmed death-1 ligand-1 and programmed death-1 ligand-2 expression in human esophageal cancer. Clin. Cancer Res. 2005, 11, 2947–2953. [Google Scholar] [CrossRef] [Green Version]
- Nomi, T.; Sho, M.; Akahori, T.; Hamada, K.; Kubo, A.; Kanehiro, H.; Nakamura, S.; Enomoto, K.; Yagita, H.; Azuma, M.; et al. Clinical significance and therapeutic potential of the programmed death-1 ligand/programmed death-1 pathway in human pancreatic cancer. Clin. Cancer Res. 2007, 13, 2151–2157. [Google Scholar] [CrossRef] [Green Version]
- Gao, Q.; Wang, X.Y.; Qiu, S.J.; Yamato, I.; Sho, M.; Nakajima, Y.; Zhou, J.; Li, B.Z.; Shi, Y.H.; Xiao, Y.S.; et al. Overexpression of PD-L1 significantly associates with tumor aggressiveness and postoperative recurrence in human hepatocellular carcinoma. Clin. Cancer Res. 2009, 15, 971–979. [Google Scholar] [CrossRef] [Green Version]
- Hamanishi, J.; Mandai, M.; Iwasaki, M.; Okazaki, T.; Tanaka, Y.; Yamaguchi, K.; Higuchi, T.; Yagi, H.; Takakura, K.; Minato, N.; et al. Programmed cell death 1 ligand 1 and tumor-infiltrating CD8+ T lymphocytes are prognostic factors of human ovarian cancer. Proc. Natl. Acad. Sci. USA 2007, 104, 3360–3365. [Google Scholar] [CrossRef] [Green Version]
- Yearley, J.H.; Gibson, C.; Yu, N.; Moon, C.; Murphy, E.; Juco, J.; Lunceford, J.; Cheng, J.; Chow, L.Q.M.; Seiwert, T.Y.; et al. PD-L2 Expression in human tumors: Relevance to anti-PD-1 therapy in cancer. Clin. Cancer Res. 2017, 23, 3158–3167. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, S.M.; Martinenaite, E.; Holmstrom, M.; Jorgensen, M.A.; Met, O.; Nastasi, C.; Klausen, U.; Donia, M.; Pedersen, L.M.; Munksgaard, L.; et al. The inhibitory checkpoint, PD-L2, is a target for effector T cells: Novel possibilities for immune therapy. Oncoimmunology 2018, 7, e1390641. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Antibody | Company | Primary Antibody | Dilution | Antigen Retrieval | Incubation | Positive Control |
|---|---|---|---|---|---|---|
| PARP | Abcam | Monoclonal | 1/25 | Citrate buffer, 20 min steamer | 1 h | Breast carcinoma |
| PTEN | Millipore | Monoclonal | 1/100 | Citrate buffer, 20 min microwave | 2 h | Endometrial cancer |
| ATM | Abcam | Monoclonal | 1/50 | TRIS, 40 min steamer | 1 h | Normal testis |
| FANCD2 | Epitomics | Monoclonal | 1/100 | Citrate buffer, 20 min microwave | 1 h | Breast carcinoma |
| H2AX | Bethyl Lab | Monoclonal | 1/100 | Citrate buffer, 20 min microwave | 1 h | Ovarian cancer |
| p53 | Novocastra | Monoclonal | 1/50 | Citrate buffer, 40 min microwave | 1 h | Ovarian cancer |
| CD4 | Agilent | Monoclonal | ready to use | Automated | 30 min | Tonsil |
| CD8 | Agilent | Monoclonal | ready to use | Automated | 30 min | Tosnil |
| CD68 | Agilent | Monoclonal | 1/3000 | Automated | 30 min | Lymph node |
| FOXP3 | Biolegend | Polyclonal | 1/20 | Tris buffer | 30 min | Lymph node |
| PDL1 | Lifespan | Polyclonal | 1/250 | Alkaline buffer, 20 min | 30 min | Tonsil |
| PDL2 | Atlas | Polyclonal | 1/100 | Citrate buffer, 40 min microwave | 1 h | Tonsil |
| Characteristics | n = 181 |
|---|---|
| Age (yrs) * | 61.6 (±12.1) |
| <70 | (71.4%) |
| ≥70 | (28.6%) |
| Primary site | |
| Ovary | 136 (75.1%) |
| Fallopian | 1 (0.6%) |
| Peritoneal | 44 (24.3%) |
| Cancer Stage * | |
| I | 8 (4.4%) |
| II | 10 (5.6%) |
| III | 138 (76.7%) |
| IV | 24 (13.3%) |
| Histology type | |
| Serous * | 147 (81.2%) |
| Clear cell | 8 (4.4%) |
| Endometrioid | 9 (5.0%) |
| Mucinous | 5 (2.8%) |
| Mixed | 9 (5.0%) |
| Carcinosarcoma | 3 (1.7%) |
| Grade tumor differentiation | |
| 1 | 10 (5.5%) |
| 2 | 15 (8.3%) |
| 3 | 156 (86.2%) |
| Complete resection | |
| No | 118 (65.9%) |
| Yes | 61 (34.1%) |
| Progression of disease | |
| No | 24 (13.3%) |
| Yes ** | 157 (87.7%) |
| Death due to disease | |
| No | 30 (16.8%) |
| Yes | 149 (83.2%) |
| No. | p53 | PARP | ATM | H2Ax | PTEN | FANCD2 | CD4 | CD8 | CD68 | FOXp3 | PD-L1 | PD-L2 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p53 | 173 | 0.13 | 0.08 | 0.02 | 0.01 | 0.09 | 0.18 | 0.07 | 0.18 | 0.08 | 0.13 | 0.07 | |||||||||||||
| PARP | 181 | 0.08 | 0.41 | 0.04 | 0.06 | 0.40 | 0.24 | 0.07 | 0.07 | 0.09 | 0.59 | 0.07 | |||||||||||||
| ATM | 173 | 0.31 | <0.001 | 0.22 | 0.12 | 0.32 | 0.002 | 0.27 | 0.15 | 0.13 | 0.32 | 0.04 | |||||||||||||
| H2Ax | 178 | 0.76 | 0.57 | 0.004 | 0.15 | 0.05 | 0.04 | 0.02 | 0.02 | 0.05 | 0.01 | 0.03 | |||||||||||||
| PTEN | 179 | 0.89 | 0.44 | 0.13 | 0.044 | 0.02 | 0.08 | 0.01 | 0.09 | 0.05 | 0.14 | 0.04 | |||||||||||||
| FANCD2 | 179 | 0.25 | <0.001 | <0.001 | 0.50 | 0.80 | 0.09 | 0.07 | 0.08 | 0.03 | 0.37 | 0.07 | |||||||||||||
| CD4 | 179 | 0.02 | 0.001 | 0.98 | 0.62 | 0.31 | 0.21 | 0.45 | 0.49 | 0.46 | 0.08 | 0.01 | |||||||||||||
| CD8 | 176 | 0.40 | 0.33 | <0.001 | 0.80 | 0.90 | 0.38 | <0.001 | 0.49 | 0.55 | 0.12 | 0.18 | |||||||||||||
| CD68 | 173 | 0.02 | 0.34 | 0.046 | 0.79 | 0.23 | 0.30 | <0.001 | <0.001 | 0.57 | 0.10 | 0.17 | |||||||||||||
| FOXp3 | 177 | 0.32 | 0.26 | 0.10 | 0.51 | 0.51 | 0.71 | <0.001 | <0.001 | <0.001 | 0.05 | 0.16 | |||||||||||||
| PD-L1 | 180 | 0.09 | <0.001 | <0.001 | 0.94 | 0.055 | <0.001 | 0.29 | 0.11 | 0.20 | 0.53 | 0.10 | |||||||||||||
| PD-L2 | 178 | 0.38 | 0.34 | 0.64 | 0.73 | 0.58 | 0.33 | 0.95 | 0.02 | 0.03 | 0.03 | 0.20 | |||||||||||||
| Characteristic | 4.5-yr (%) | Adjusted HR (95% CI) | p-Value |
|---|---|---|---|
| Stage | |||
| I–II | 66.7% | 1 | |
| III–IV | 15.8% | 2.28 (1.02–5.10) | 0.046 |
| Cytoreduction | |||
| Residual | 13.8% | 1 | |
| Complete | 32.0% | 0.64 (0.43–0.95) | 0.026 |
| PARP | |||
| 0/1+ | 25.6% | 1 | |
| 2+/3+ | 16.1% | 1.75 (1.19–2.59) | 0.005 |
| PTEN | |||
| 0/1+ | 21.1% | 1 | |
| 2+/3+ | 10.4% | 1.96 (1.13–3.41) | 0.017 |
| FANC | |||
| 0/1+/2+ | 17.3% | 1 | |
| 3+ | 25.9% | 0.82 (0.55–1.24) | 0.350 |
| PD-L1 | |||
| 0/1+ | 17.4% | 1 | |
| 2+/3+ | 22.0% | 0.49 (0.32–0.73) | <0.001 |
| PD-L2 | |||
| 0 | 32.8% | 1 | |
| 1+/2+/3+ | 18.4% | 1.89 (1.01–3.52) | 0.046 |
| CD4 | |||
| 0 | 12.5% | 1 | |
| 1+/2+/3+ | 22.9% | 0.67 (0.45–0.99) | 0.042 |
| CD8 | |||
| 0/1+/2+ | 17.6% | 1 | |
| 3+ | 24.9% | 0.68 (0.45–1.04) | 0.073 |
| Characteristic | 4.5-yr (%) | Adjusted-HR (95%CI) | p-Value |
|---|---|---|---|
| Age (years) | |||
| <70 | 34.3% | 1 | |
| ≥70 | 24.1% | 1.40 (0.96–2.05) | 0.079 |
| Stage | |||
| I–II | 69.3% | 1 | |
| III–IV | 28.4% | 2.12 (0.90–5.01) | 0.086 |
| Cytoreduction | |||
| Residual | 25.8% | 1 | |
| Complete | 39.9% | 0.61 (0.41–0.92) | 0.019 |
| H2Ax | |||
| 0 | 65.9% | 1 | |
| 1+/2+/3+ | 28.9% | 1.64 (0.82–3.30) | 0.163 |
| PD-L1 | |||
| 0/1+ | 27.3% | 1 | |
| 2+/3+ | 35.8% | 0.83 (0.59–1.16) | 0.273 |
| CD8 | |||
| 0 | 14.8% | 1 | |
| 1+/2+/3+ | 34.0% | 0.60 (0.36–0.99) | 0.045 |
| FOXp3 | |||
| 0/1+ | 28.9% | 1 | |
| 2+/3+ | 35.6% | 0.74 (0.51–1.08) | 0.115 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batman, S.; Matsuo, K.; Mhawech-Fauceglia, P.; Munro, E.; Weisenberger, M.; Allen, A.; Joshi, S.; Machida, H.; Matsuzaki, S.; Bozanovic, T.; et al. Intersection of DNA Repair Pathways and the Immune Landscape Identifies PD-L2 as a Prognostic Marker in Epithelial Ovarian Cancer. Cancers 2021, 13, 1972. https://doi.org/10.3390/cancers13081972
Batman S, Matsuo K, Mhawech-Fauceglia P, Munro E, Weisenberger M, Allen A, Joshi S, Machida H, Matsuzaki S, Bozanovic T, et al. Intersection of DNA Repair Pathways and the Immune Landscape Identifies PD-L2 as a Prognostic Marker in Epithelial Ovarian Cancer. Cancers. 2021; 13(8):1972. https://doi.org/10.3390/cancers13081972
Chicago/Turabian StyleBatman, Samantha, Koji Matsuo, Paulette Mhawech-Fauceglia, Elizabeth Munro, Mercedes Weisenberger, Allison Allen, Sonali Joshi, Hiroko Machida, Shinya Matsuzaki, Tatjana Bozanovic, and et al. 2021. "Intersection of DNA Repair Pathways and the Immune Landscape Identifies PD-L2 as a Prognostic Marker in Epithelial Ovarian Cancer" Cancers 13, no. 8: 1972. https://doi.org/10.3390/cancers13081972