
Radical Resection for Locally Advanced Pancreatic Cancers in the Era of New Neoadjuvant Therapy—Arterial Resection, Arterial Divestment and Total Pancreatectomy


Abstract
:Simple Summary
Abstract
1. Introduction
2. Arterial Resections
2.1. Overview
2.2. Management for the Involvement of the Superior Mesenteric Artery
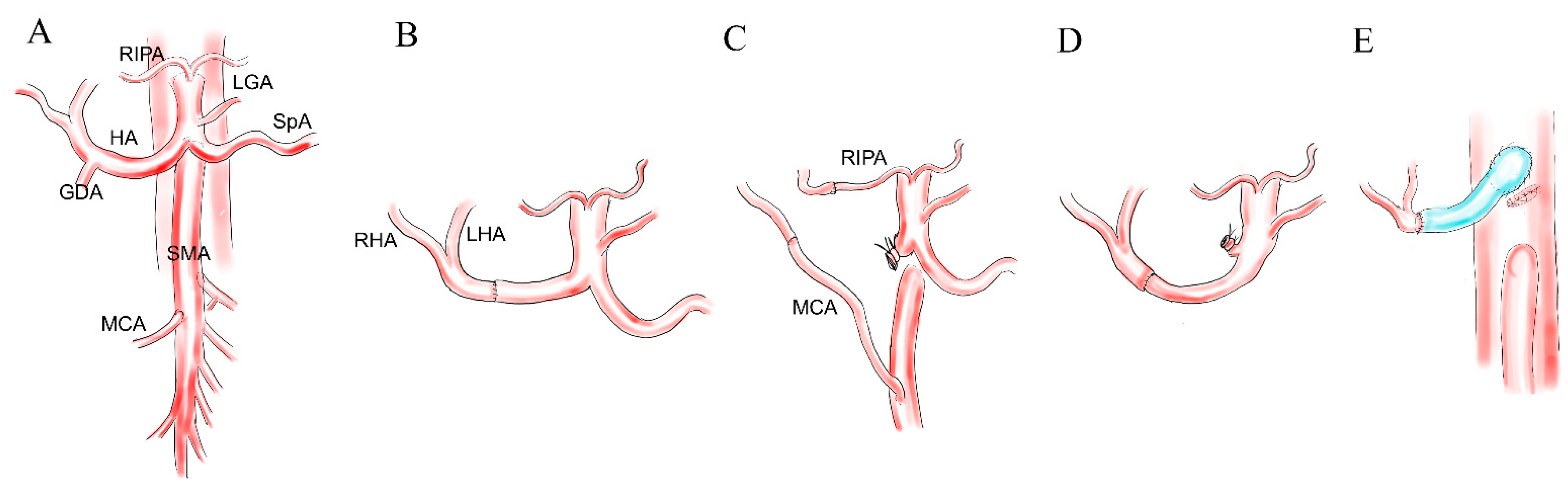
2.3. Resection of the Hepatic Artery
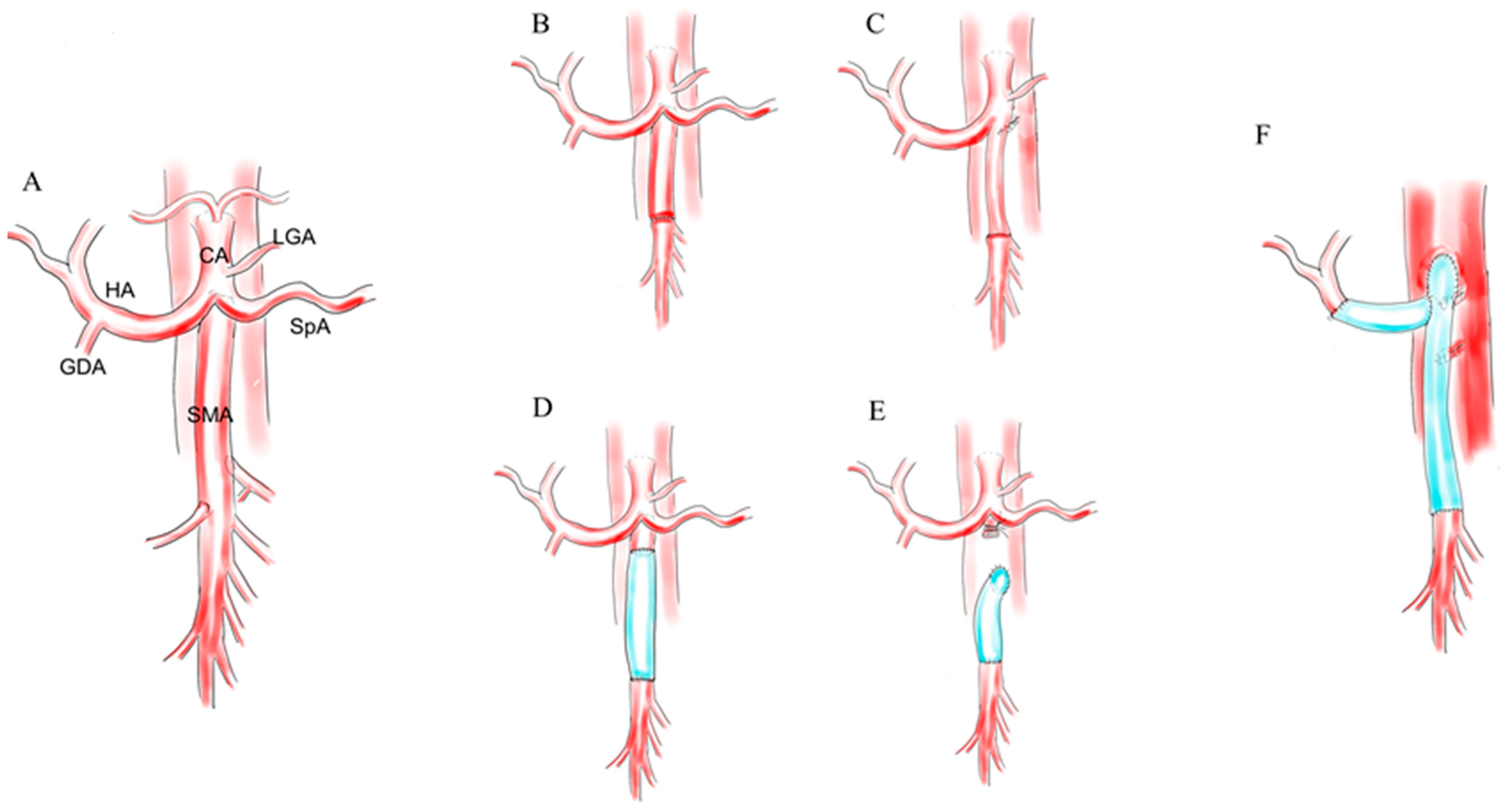
2.4. Resection of the Celiac Axis
3. Total Pancreatectomy
4. Recent Evolution of Radical Pancreatectomies in the Era of New Regimens and Future Perspective
4.1. Recent Reports of Extremely Radical Pancreatectomy
4.2. En-Bloc Arterial Resection or Arterial Divestment?
4.3. Rationale of Total Neoadjuvant Therapy
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortner, J.G. Regional pancreatectomy for cancer of the pancreas, ampulla, and other related sites. Tumor staging and results. Ann. Surg. 1984, 199, 418–425. [Google Scholar] [CrossRef]
- Mollberg, N.; Rahbari, N.N.; Koch, M.; Hartwig, W.; Hoeger, Y.; Büchler, M.W.; Weitz, J. Arterial resection during pancreatectomy for pancreatic cancer: A systematic review and meta-analysis. Ann. Surg. 2011, 254, 882–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karpoff, H.M.; Klimstra, D.S.; Brennan, M.F.; Conlon, K.C. Results of total pancreatectomy for adenocarcinoma of the pancreas. Arch. Surg. 2001, 136, 44–47; discussion 48. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Becouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardiere, C.; et al. Folfirinox versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortner, J.G.; Kim, D.K.; Cubilla, A.; Turnbull, A.; Pahnke, L.D.; Shils, M.E. Regional pancreatectomy: En bloc pancreatic, portal vein and lymph node resection. Ann. Surg. 1977, 186, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.B.; Farnell, M.B.; Lillemoe, K.D.; Vollmer, C., Jr.; Strasberg, S.M.; Schulick, R.D. Surgical treatment of resectable and borderline resectable pancreas cancer: Expert consensus statement. Ann. Surg. Oncol. 2009, 16, 1736–1744. [Google Scholar] [CrossRef] [PubMed]
- Tseng, J.F.; Tamm, E.P.; Lee, J.E.; Pisters, P.W.; Evans, D.B. Venous resection in pancreatic cancer surgery. Best Pract. Res. Clin. Gastroenterol. 2006, 20, 349–364. [Google Scholar] [CrossRef]
- Nakao, A.; Takeda, S.; Inoue, S.; Nomoto, S.; Kanazumi, N.; Sugimoto, H.; Fujii, T. Indications and techniques of extended resection for pancreatic cancer. World J. Surg. 2006, 30, 976–982. [Google Scholar] [CrossRef]
- Tseng, J.F.; Raut, C.P.; Lee, J.E.; Pisters, P.W.; Vauthey, J.N.; Abdalla, E.K.; Gomez, H.F.; Sun, C.C.; Crane, C.H.; Wolff, R.A.; et al. Pancreaticoduodenectomy with vascular resection: Margin status and survival duration. J. Gastrointest. Surg. 2004, 8, 935–949; discussion 949–950. [Google Scholar] [CrossRef]
- Esposito, I.; Kleeff, J.; Bergmann, F.; Reiser, C.; Herpel, E.; Friess, H.; Schirmacher, P.; Buchler, M.W. Most pancreatic cancer resections are r1 resections. Ann. Surg. Oncol. 2008, 15, 1651–1660. [Google Scholar] [CrossRef]
- Verbeke, C.S.; Leitch, D.; Menon, K.V.; McMahon, M.J.; Guillou, P.J.; Anthoney, A. Redefining the r1 resection in pancreatic cancer. Br. J. Surg. 2006, 93, 1232–1237. [Google Scholar] [CrossRef] [PubMed]
- Rebelo, A.; Büdeyri, I.; Heckler, M.; Partsakhashvili, J.; Ukkat, J.; Ronellenfitsch, U.; Michalski, C.W.; Kleeff, J. Systematic review and meta-analysis of contemporary pancreas surgery with arterial resection. Langenbeck’s Arch. Surg. 2020, 405, 903–919. [Google Scholar] [CrossRef]
- Małczak, P.; Sierżęga, M.; Stefura, T.; Kacprzyk, A.; Droś, J.; Skomarovska, O.; Krzysztofik, M.; Major, P.; Pędziwiatr, M. Arterial resections in pancreatic cancer—Systematic review and meta-analysis. HPB 2020, 22, 961–968. [Google Scholar] [CrossRef]
- Inoue, Y.; Saiura, A.; Oba, A.; Kawakatsu, S.; Ono, Y.; Sato, T.; Mise, Y.; Ishizawa, T.; Takahashi, Y.; Ito, H. Optimal extent of superior mesenteric artery dissection during pancreaticoduodenectomy for pancreatic cancer: Balancing surgical and oncological safety. J. Gastrointest. Surg. 2019, 23, 1373–1383. [Google Scholar] [CrossRef] [PubMed]
- Amano, H.; Miura, F.; Toyota, N.; Wada, K.; Katoh, K.; Hayano, K.; Kadowaki, S.; Shibuya, M.; Maeno, S.; Eguchi, T.; et al. Is pancreatectomy with arterial reconstruction a safe and useful procedure for locally advanced pancreatic cancer? J. Hepato-Biliary-Pancreat. Surg. 2009, 16, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Jegatheeswaran, S.; Baltatzis, M.; Jamdar, S.; Siriwardena, A.K. Superior mesenteric artery (sma) resection during pancreatectomy for malignant disease of the pancreas: A systematic review. HPB 2017, 19, 483–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitagawa, H.; Ohta, T.; Tajima, H.; Nakagawara, H.; Makino, I.; Takamura, H.; Tani, T.; Kayahara, M. En bloc resection including the superior mesenteric artery and vein of locally advanced pancreatic carcinomas. Nihon Geka Gakkai Zasshi 2011, 112, 164–169. [Google Scholar]
- Yekebas, E.F.; Bogoevski, D.; Cataldegirmen, G.; Kunze, C.; Marx, A.; Vashist, Y.K.; Schurr, P.G.; Liebl, L.; Thieltges, S.; Gawad, K.A.; et al. En bloc vascular resection for locally advanced pancreatic malignancies infiltrating major blood vessels: Perioperative outcome and long-term survival in 136 patients. Ann. Surg. 2008, 247, 300–309. [Google Scholar] [CrossRef]
- Inoue, Y.; Saiura, A.; Yoshioka, R.; Ono, Y.; Takahashi, M.; Arita, J.; Takahashi, Y.; Koga, R. Pancreatoduodenectomy with systematic mesopancreas dissection using a supracolic anterior artery-first approach. Ann. Surg. 2015, 262, 1092–1101. [Google Scholar] [CrossRef]
- Bachellier, P.; Addeo, P.; Faitot, F.; Nappo, G.; Dufour, P. Pancreatectomy with arterial resection for pancreatic adenocarcinoma: How can it be done safely and with which outcomes?: A single institution’s experience with 118 patients. Ann. Surg. 2020, 271, 932–940. [Google Scholar] [CrossRef]
- Loos, M.; Kester, T.; Klaiber, U.; Mihaljevic, A.L.; Mehrabi, A.; Muller-Stich, B.M.; Diener, M.K.; Schneider, M.A.; Berchtold, C.; Hinz, U.; et al. Arterial resection in pancreatic cancer surgery: Effective after a learning curve. Ann. Surg. 2020. Jun 12. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Chen, F.Z.; Ge, X.H.; Cai, M.Z.; Jiang, J.S.; Li, J.P.; Lu, S.H. Pancreatoduodenectomy with vascular reconstruction in treating carcinoma of the pancreatic head. Hepatobiliary Pancreat. Dis. Int. 2004, 3, 612–615. [Google Scholar] [PubMed]
- Boggi, U.; Del Chiaro, M.; Croce, C.; Vistoli, F.; Signori, S.; Moretto, C.; Amorese, G.; Mazzeo, S.; Cappelli, C.; Campani, D.; et al. Prognostic implications of tumor invasion or adhesion to peripancreatic vessels in resected pancreatic cancer. Surgery 2009, 146, 869–881. [Google Scholar] [CrossRef]
- Martin, R.C., 2nd; Scoggins, C.R.; Egnatashvili, V.; Staley, C.A.; McMasters, K.M.; Kooby, D.A. Arterial and venous resection for pancreatic adenocarcinoma: Operative and long-term outcomes. Arch. Surg. 2009, 144, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Bockhorn, M.; Burdelski, C.; Bogoevski, D.; Sgourakis, G.; Yekebas, E.F.; Izbicki, J.R. Arterial en bloc resection for pancreatic carcinoma. Br. J. Surg. 2011, 98, 86–92. [Google Scholar] [CrossRef]
- Rehders, A.; Stoecklein, N.H.; Güray, A.; Riediger, R.; Alexander, A.; Knoefel, W.T. Vascular invasion in pancreatic cancer: Tumor biology or tumor topography? Surgery 2012, 152, S143–S151. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Zhang, L.; He, T.; Ding, J.; Zhang, H.; Chen, G.; Zhang, D.; Wu, Z.; Chen, Q.; Fan, H.; et al. Pancreaticoduodenectomy combined with vascular resection and reconstruction for patients with locally advanced pancreatic cancer: A multicenter, retrospective analysis. PLoS ONE 2013, 8, e70340. [Google Scholar]
- Sgroi, M.D.; Narayan, R.R.; Lane, J.S.; Demirjian, A.; Kabutey, N.K.; Fujitani, R.M.; Imagawa, D.K. Vascular reconstruction plays an important role in the treatment of pancreatic adenocarcinoma. J. Vasc. Surg. 2015, 61, 475–480. [Google Scholar] [CrossRef] [Green Version]
- Glebova, N.O.; Hicks, C.W.; Tosoian, J.J.; Piazza, K.M.; Abularrage, C.J.; Schulick, R.D.; Wolfgang, C.L.; Black, J.H., 3rd. Outcomes of arterial resection during pancreatectomy for tumor. J. Vasc. Surg. 2016, 63, 722–729.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perinel, J.; Nappo, G.; El Bechwaty, M.; Walter, T.; Hervieu, V.; Valette, P.J.; Feugier, P.; Adham, M. Locally advanced pancreatic duct adenocarcinoma: Pancreatectomy with planned arterial resection based on axial arterial encasement. Langenbeck’s Arch. Surg. 2016, 401, 1131–1142. [Google Scholar] [CrossRef] [PubMed]
- Tee, M.C.; Krajewski, A.C.; Groeschl, R.T.; Farnell, M.B.; Nagorney, D.M.; Kendrick, M.L.; Cleary, S.P.; Smoot, R.L.; Croome, K.P.; Truty, M.J. Indications and perioperative outcomes for pancreatectomy with arterial resection. J. Am. Coll. Surg. 2018, 227, 255–269. [Google Scholar] [CrossRef]
- Loveday, B.P.T.; Zilbert, N.; Serrano, P.E.; Tomiyama, K.; Tremblay, A.; Fox, A.M.; Segedi, M.; O’Malley, M.; Borgida, A.; Bianco, T.; et al. Neoadjuvant therapy and major arterial resection for potentially reconstructable arterial involvement by stage 3 adenocarcinoma of the pancreas. HPB 2019, 21, 643–652. [Google Scholar] [CrossRef]
- Westermark, S.; Rangelova, E.; Ansorge, C.; Lundell, L.; Segersvärd, R.; Del Chiaro, M. Cattell-braasch maneuver combined with local hypothermia during superior mesenteric artery resection in pancreatectomy. Langenbeck’s Arch. Surg. 2016, 401, 1241–1247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tempero, M.A.; Malafa, M.P.; Chiorean, E.G.; Czito, B.; Scaife, C.; Narang, A.K.; Fountzilas, C.; Wolpin, B.M.; Al-Hawary, M.; Asbun, H.; et al. Pancreatic adenocarcinoma, version 1. 2019. J. Natl. Compr. Cancer Netw. 2019, 17, 202–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amano, R.; Kimura, K.; Nakata, B.; Yamazoe, S.; Motomura, H.; Yamamoto, A.; Tanaka, S.; Hirakawa, K. Pancreatectomy with major arterial resection after neoadjuvant chemoradiotherapy gemcitabine and s-1 and concurrent radiotherapy for locally advanced unresectable pancreatic cancer. Surgery 2015, 158, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, M.; Yoshitomi, H.; Takano, S.; Shimizu, H.; Kato, A.; Yoshidome, H.; Furukawa, K.; Takayashiki, T.; Kuboki, S.; Suzuki, D.; et al. Combined hepatic arterial resection in pancreatic resections for locally advanced pancreatic cancer. Langenbeck’s Arch. Surg. 2017, 402, 447–456. [Google Scholar] [CrossRef]
- Wang, C.; Wu, H.; Xiong, J.; Zhou, F.; Tao, J.; Liu, T.; Zhao, G.; Gou, S. Pancreaticoduodenectomy with vascular resection for local advanced pancreatic head cancer: A single center retrospective study. J. Gastrointest. Surg. 2008, 12, 2183–2190. [Google Scholar] [CrossRef]
- Desaki, R.; Mizuno, S.; Tanemura, A.; Kishiwada, M.; Murata, Y.; Azumi, Y.; Kuriyama, N.; Usui, M.; Sakurai, H.; Tabata, M.; et al. A new surgical technique of pancreaticoduodenectomy with splenic artery resection for ductal adenocarcinoma of the pancreatic head and/or body invading splenic artery: Impact of the balance between surgical radicality and qol to avoid total pancreatectomy. Biomed. Res. Int. 2014, 2014, 219038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appleby, L.H. The coeliac axis in the expansion of the operation for gastric carcinoma. Cancer 1953, 6, 704–707. [Google Scholar] [CrossRef]
- Hishinuma, S.; Ogata, Y.; Matsui, J.; Ozawa, I.; Inada, T.; Shimizu, H.; Eckhauser, F. Two cases of cancer of the pancreatic body undergoing gastric preservation with distal pancreatectomy combined with resection of the celiac axis. Jpn. J. Gastroenterol. Surg. 1991, 24, 2782–2786. [Google Scholar] [CrossRef] [Green Version]
- Kondo, S.; Katoh, H.; Hirano, S.; Ambo, Y.; Tanaka, E.; Okushiba, S.; Morikawa, T. Results of radical distal pancreatectomy with en bloc resection of the celiac artery for locally advanced cancer of the pancreatic body. Langenbeck’s Arch. Surg. 2003, 388, 101–106. [Google Scholar]
- Konishi, M.; Kinoshita, T.; Nakagori, T.; Inoue, K.; Oda, T.; Kimata, T.; Kikuchi, H.; Ryu, M. Distal pancreatectomy with resection of the celiac axis and reconstruction of the hepatic artery for carcinoma of the body and tail of the pancreas. J. Hepato-Biliary-Pancreat. Surg. 2000, 7, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Kimura, W.; Han, I.; Furukawa, Y.; Sunami, E.; Futakawa, N.; Inoue, T.; Shinkai, H.; Zhao, B.; Muto, T.; Makuuchi, M.; et al. Appleby operation for carcinoma of the body and tail of the pancreas. Hepato-Gastroenterol. 1997, 44, 387–393. [Google Scholar]
- Ozaki, H.; Kinoshita, T.; Kosuge, T.; Yamamoto, J.; Shimada, K.; Inoue, K.; Koyama, Y.; Mukai, K. An aggressive therapeutic approach to carcinoma of the body and tail of the pancreas. Cancer 1996, 77, 2240–2245. [Google Scholar] [CrossRef]
- Mayumi, T.; Nimura, Y.; Kamiya, J.; Kondo, S.; Nagino, M.; Kanai, M.; Miyachi, M.; Hamaguchi, K.; Hayakawa, N. Distal pancreatectomy with en bloc resection of the celiac artery for carcinoma of the body and tail of the pancreas. Int. J. Pancreatol. 1997, 22, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Hirano, S.; Kondo, S.; Hara, T.; Ambo, Y.; Tanaka, E.; Shichinohe, T.; Suzuki, O.; Hazama, K. Distal pancreatectomy with en bloc celiac axis resection for locally advanced pancreatic body cancer: Long-term results. Ann. Surg. 2007, 246, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Klompmaker, S.; Peters, N.A.; van Hilst, J.; Bassi, C.; Boggi, U.; Busch, O.R.; Niesen, W.; Van Gulik, T.M.; Javed, A.A.; Kleeff, J.; et al. Outcomes and risk score for distal pancreatectomy with celiac axis resection (dp-car): An international multicenter analysis. Ann. Surg. Oncol. 2019, 26, 772–781. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, T.; Hirano, S.; Noji, T.; Asano, T.; Okamura, K.; Tsuchikawa, T.; Murakami, S.; Kurashima, Y.; Ebihara, Y.; Nakanishi, Y.; et al. Distal pancreatectomy with en bloc celiac axis resection (modified appleby procedure) for locally advanced pancreatic body cancer: A single-center review of 80 consecutive patients. Ann. Surg. Oncol. 2016, 23, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Ocuin, L.M.; Miller-Ocuin, J.L.; Novak, S.M.; Bartlett, D.L.; Marsh, J.W.; Tsung, A.; Lee, K.K.; Hogg, M.E.; Zeh, H.J.; Zureikat, A.H. Robotic and open distal pancreatectomy with celiac axis resection for locally advanced pancreatic body tumors: A single institutional assessment of perioperative outcomes and survival. HPB 2016, 18, 835–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshiya, S.; Fukuzawa, K.; Inokuchi, S.; Kosai-Fujimoto, Y.; Sanefuji, K.; Iwaki, K.; Motohiro, A.; Itoh, S.; Harada, N.; Ikegami, T.; et al. Efficacy of neoadjuvant chemotherapy in distal pancreatectomy with en bloc celiac axis resection (dp-car) for locally advanced pancreatic cancer. J. Gastrointest. Surg. 2019, 24, 1605–1611. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T.; Satoi, S.; Kawai, M.; Motoi, F.; Sho, M.; Uemura, K.I.; Matsumoto, I.; Honda, G.; Okada, K.I.; Akahori, T.; et al. Is distal pancreatectomy with en-bloc celiac axis resection effective for patients with locally advanced pancreatic ductal adenocarcinoma? -multicenter surgical group study. Pancreatology 2018, 18, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Beane, J.D.; House, M.G.; Pitt, S.C.; Kilbane, E.M.; Hall, B.L.; Parmar, A.D.; Riall, T.S.; Pitt, H.A. Distal pancreatectomy with celiac axis resection: What are the added risks? HPB 2015, 17, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, K.I.; Kawai, M.; Hirono, S.; Miyazawa, M.; Kitahata, Y.; Ueno, M.; Hayami, S.; Shimokawa, T.; Yamaue, H. Ischemic gastropathy after distal pancreatectomy with en bloc celiac axis resection for pancreatic body cancer. Langenbeck’s Arch. Surg. 2018, 403, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Ueda, A.; Sakai, N.; Yoshitomi, H.; Furukawa, K.; Takayashiki, T.; Kuboki, S.; Takano, S.; Suzuki, D.; Kagawa, S.; Mishima, T.; et al. Is hepatic artery coil embolization useful in distal pancreatectomy with en bloc celiac axis resection for locally advanced pancreatic cancer? World J. Surg. Oncol. 2019, 17, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Truty, M.J.; Colglazier, J.J.; Mendes, B.C.; Nagorney, D.M.; Bower, T.C.; Smoot, R.L.; DeMartino, R.R.; Cleary, S.P.; Oderich, G.S.; Kendrick, M.L. En bloc celiac axis resection for pancreatic cancer: Classification of anatomical variants based on tumor extent. J. Am. Coll. Surg. 2020, 231, 8–29. [Google Scholar] [CrossRef] [PubMed]
- Yoshitomi, H.; Sakai, N.; Kagawa, S.; Takano, S.; Ueda, A.; Kato, A.; Furukawa, K.; Takayashiki, T.; Kuboki, S.; Miyzaki, M.; et al. Feasibility and safety of distal pancreatectomy with en bloc celiac axis resection (dp-car) combined with neoadjuvant therapy for borderline resectable and unresectable pancreatic body/tail cancer. Langenbeck’s Arch. Surg. 2019, 404, 451–458. [Google Scholar] [CrossRef]
- Sato, T.; Inoue, Y.; Takahashi, Y.; Mise, Y.; Ishizawa, T.; Tanakura, K.; Ito, H.; Saiura, A. Distal pancreatectomy with celiac axis resection combined with reconstruction of the left gastric artery. J. Gastrointest. Surg. 2017, 21, 910–917. [Google Scholar] [CrossRef]
- Oba, A.; Inoue, Y.; Sato, T.; Ono, Y.; Mise, Y.; Ito, H.; Ishizawa, T.; Takahashi, Y.; Saiura, A. Impact of indocyanine green-fluorescence imaging on distal pancreatectomy with celiac axis resection combined with reconstruction of the left gastric artery. HPB 2019, 21, 619–625. [Google Scholar] [CrossRef]
- Rockey, E.W. Total pancreatectomy for carcinoma: Case report. Ann. Surg. 1943, 118, 603–611. [Google Scholar] [CrossRef] [PubMed]
- ReMine, W.H.; Priestley, J.T.; Judd, E.S.; King, J.N. Total pancreatectomy. Ann. Surg. 1970, 172, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Ross, D.E. Cancer of the pancreas; a plea for total pancreatectomy. Am. J. Surg. 1954, 87, 20–33. [Google Scholar] [CrossRef]
- Warren, K.W.; Poulantzas, J.K.; Kune, G.A. Life after total pancreatectomy for chronic pancreatitis: Clinical study of eight cases. Ann. Surg. 1966, 164, 830–834. [Google Scholar] [CrossRef]
- Nakao, A.; Ichihara, T.; Nonami, T.; Harada, A.; Koshikawa, T.; Nakashima, N.; Nagura, H.; Takagi, H. Clinicohistopathologic and immunohistochemical studies of intrapancreatic development of carcinoma of the head of the pancreas. Ann. Surg. 1989, 209, 181–187. [Google Scholar] [CrossRef]
- Ihse, I.; Anderson, H.; Andrén, S. Total pancreatectomy for cancer of the pancreas: Is it appropriate? World J. Surg. 1996, 20, 288–293; discussion 294. [Google Scholar] [CrossRef]
- Scholten, L.; Stoop, T.F.; Del Chiaro, M.; Busch, O.R.; van Eijck, C.; Molenaar, I.Q.; de Vries, J.H.; Besselink, M.G. Dutch Pancreatic Cancer, G. Systematic review of functional outcome and quality of life after total pancreatectomy. Br. J. Surg. 2019, 106, 1735–1746. [Google Scholar] [CrossRef]
- Dresler, C.M.; Fortner, J.G.; McDermott, K.; Bajorunas, D.R. Metabolic consequences of (regional) total pancreatectomy. Ann. Surg. 1991, 214, 131–140. [Google Scholar] [CrossRef]
- Hata, T.; Ishida, M.; Motoi, F.; Sakata, N.; Yoshimatsu, G.; Naitoh, T.; Katayose, Y.; Egawa, S.; Unno, M. Clinical characteristics and risk factors for the development of postoperative hepatic steatosis after total pancreatectomy. Pancreas 2016, 45, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.; Wolfgang, C.L.; Cameron, J.L.; Eckhauser, F.; Choti, M.A.; Schulick, R.D.; Edil, B.H.; Pawlik, T.M. Total pancreatectomy for pancreatic adenocarcinoma: Evaluation of morbidity and long-term survival. Ann. Surg. 2009, 250, 282–287. [Google Scholar] [CrossRef]
- Hartwig, W.; Gluth, A.; Hinz, U.; Koliogiannis, D.; Strobel, O.; Hackert, T.; Werner, J.; Büchler, M.W. Outcomes after extended pancreatectomy in patients with borderline resectable and locally advanced pancreatic cancer. Br J Surg. 2016, 103, 1683–1694. [Google Scholar] [CrossRef]
- Hartwig, W.; Gluth, A.; Hinz, U.; Bergmann, F.; Spronk, P.E.; Hackert, T.; Werner, J.; Büchler, M.W. Total pancreatectomy for primary pancreatic neoplasms: Renaissance of an unpopular operation. Ann. Surg. 2015, 261, 537–546. [Google Scholar] [CrossRef] [Green Version]
- Müller, M.W.; Friess, H.; Kleeff, J.; Dahmen, R.; Wagner, M.; Hinz, U.; Breisch-Girbig, D.; Ceyhan, G.O.; Büchler, M.W. Is there still a role for total pancreatectomy? Ann. Surg. 2007, 246, 966–974, discussion 974–965. [Google Scholar] [CrossRef]
- Brooks, J.R.; Brooks, D.C.; Levine, J.D. Total pancreatectomy for ductal cell carcinoma of the pancreas. An update. Ann. Surg. 1989, 209, 405–410. [Google Scholar] [CrossRef]
- Launois, B.; Franci, J.; Bardaxoglou, E.; Ramee, M.P.; Paul, J.L.; Malledant, Y.; Campion, J.P. Total pancreatectomy for ductal adenocarcinoma of the pancreas with special reference to resection of the portal vein and multicentric cancer. World J. Surg. 1993, 17, 122–126, discussion 126–127. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, C.M.; Glant, J.; Winter, J.M.; Kennard, J.; Dixon, J.; Zhao, Q.; Howard, T.J.; Madura, J.A.; Nakeeb, A.; Pitt, H.A.; et al. Total pancreatectomy (r0 resection) improves survival over subtotal pancreatectomy in isolated neck margin positive pancreatic adenocarcinoma. Surgery 2007, 142, 572–578; discussion 578–580. [Google Scholar] [CrossRef] [PubMed]
- Nathan, H.; Wolfgang, C.L.; Edil, B.H.; Choti, M.A.; Herman, J.M.; Schulick, R.D.; Cameron, J.L.; Pawlik, T.M. Peri-operative mortality and long-term survival after total pancreatectomy for pancreatic adenocarcinoma: A population-based perspective. J. Surg. Oncol. 2009, 99, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Satoi, S.; Murakami, Y.; Motoi, F.; Sho, M.; Matsumoto, I.; Uemura, K.; Kawai, M.; Kurata, M.; Yanagimoto, H.; Yamamoto, T.; et al. Reappraisal of total pancreatectomy in 45 patients with pancreatic ductal adenocarcinoma in the modern era using matched-pairs analysis: Multicenter study group of pancreatobiliary surgery in japan. Pancreas 2016, 45, 1003–1009. [Google Scholar] [CrossRef]
- Johnston, W.C.; Hoen, H.M.; Cassera, M.A.; Newell, P.H.; Hammill, C.W.; Hansen, P.D.; Wolf, R.F. Total pancreatectomy for pancreatic ductal adenocarcinoma: Review of the national cancer data base. HPB 2016, 18, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Xiong, J.; Wei, A.; Ke, N.; He, D.; Chian, S.K.; Wei, Y.; Hu, W.; Liu, X. A case-matched comparison study of total pancreatectomy versus pancreaticoduodenectomy for patients with pancreatic ductal adenocarcinoma. Int. J. Surg. 2017, 48, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Passeri, M.J.; Baker, E.H.; Siddiqui, I.A.; Templin, M.A.; Martinie, J.B.; Vrochides, D.; Iannitti, D.A. Total compared with partial pancreatectomy for pancreatic adenocarcinoma: Assessment of resection margin, readmission rate, and survival from the U.S. National cancer database. Curr. Oncol. 2019, 26, e346–e356. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, D.; Mizuma, M.; Kumamaru, H.; Miyata, H.; Chikamoto, A.; Igarashi, H.; Itoi, T.; Egawa, S.; Kodama, Y.; Satoi, S.; et al. Risk model for severe postoperative complications after total pancreatectomy based on a nationwide clinical database. Br. J. Surg. 2020, 107, 734–742. [Google Scholar] [CrossRef]
- Stoop, T.F.; Ateeb, Z.; Ghorbani, P.; Scholten, L.; Arnelo, U.; Besselink, M.G.; Del Chiaro, M. Surgical outcomes after total pancreatectomy: A high-volume center experience. Ann. Surg. Oncol. 2020, 28, 1543–1551. [Google Scholar] [CrossRef]
- Stoop, T.F.; Ateeb, Z.; Ghorbani, P.; Scholten, L.; Arnelo, U.; Besselink, M.G.; Del Chiaro, M. Impact of endocrine and exocrine insufficiency on quality of life after total pancreatectomy. Ann. Surg. Oncol. 2020, 27, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Dodson, R.; Makary, M.A.; Weiss, M.J.; Hirose, K.; Cameron, J.L.; Ahuja, N.; Pawlik, T.M.; Wolfgang, C.L.; He, J. A contemporary evaluation of the cause of death and long-term quality of life after total pancreatectomy. World J. Surg. 2016, 40, 2513–2518. [Google Scholar] [CrossRef] [PubMed]
- Pulvirenti, A.; Pea, A.; Rezaee, N.; Gasparini, C.; Malleo, G.; Weiss, M.J.; Cameron, J.L.; Wolfgang, C.L.; He, J.; Salvia, R. Perioperative outcomes and long-term quality of life after total pancreatectomy. Br. J. Surg. 2019, 106, 1819–1828. [Google Scholar] [CrossRef] [PubMed]
- Truty, M.J.; Kendrick, M.L.; Nagorney, D.M.; Smoot, R.L.; Cleary, S.P.; Graham, R.P.; Goenka, A.H.; Hallemeier, C.L.; Haddock, M.G.; Harmsen, W.S.; et al. Factors predicting response, perioperative outcomes, and survival following total neoadjuvant therapy for borderline/locally advanced pancreatic cancer. Ann. Surg. 2021, 273, 341–349. [Google Scholar] [CrossRef]
- Diener, M.K.; Mihaljevic, A.L.; Strobel, O.; Loos, M.; Schmidt, T.; Schneider, M.; Berchtold, C.; Mehrabi, A.; Muller-Stich, B.P.; Jiang, K.; et al. Periarterial divestment in pancreatic cancer surgery. Surgery 2020. Oct 5. [Google Scholar] [CrossRef] [PubMed]
- Cai, B.; Lu, Z.; Neoptolemos, J.P.; Diener, M.K.; Li, M.; Yin, L.; Gao, Y.; Wei, J.; Chen, J.; Guo, F.; et al. Sub-adventitial divestment technique for resecting artery-involved pancreatic cancer: A retrospective cohort study. Langenbeck’s Arch. Surg. 2021. [Google Scholar] [CrossRef]
- Sabater, L.; Cugat, E.; Serrablo, A.; Suarez-Artacho, G.; Diez-Valladares, L.; Santoyo-Santoyo, J.; Martín-Pérez, E.; Ausania, F.; Lopez-Ben, S.; Jover-Navalon, J.M.; et al. Does the artery-first approach improve the rate of r0 resection in pancreatoduodenectomy?: A multicenter, randomized, controlled trial. Annals of surgery 2019, 270, 738–746. [Google Scholar] [CrossRef]
- Habib, J.R.; Kinny-Köster, B.; van Oosten, F.; Javed, A.A.; Cameron, J.L.; Lafaro, K.J.; Burkhart, R.A.; Burns, W.R.; He, J.; Thompson, E.D.; et al. Periadventitial dissection of the superior mesenteric artery for locally advanced pancreatic cancer: Surgical planning with the "halo sign" and "string sign". Surgery 2020. [Google Scholar] [CrossRef] [PubMed]
- Del Chiaro, M.; Schulick, R.D. Commentary on: Divestment or skeletonization of the SMA or the hepatic artery for locally advanced pancreatic ductal cancer after neoadjuvant therapy. Surgery 2020. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.T.; Wei, A.C.; Atenafu, E.G.; Cavallucci, D.; Cleary, S.P.; Moulton, C.A.; Greig, P.D.; Gallinger, S.; Serra, S.; McGilvray, I.D. Planned versus unplanned portal vein resections during pancreaticoduodenectomy for adenocarcinoma. Br. J. Surg. 2013, 100, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Oba, A.; Ito, H.; Ono, Y.; Sato, T.; Mise, Y.; Inoue, Y.; Takahashi, Y.; Saiura, A. Regional pancreatoduodenectomy versus standard pancreatoduodenectomy with portal vein resection for pancreatic ductal adenocarcinoma with portal vein invasion. BJS Open 2020, 4, 438–448. [Google Scholar] [CrossRef] [Green Version]
- Del Chiaro, M.; Schulick, R.D. Use of total pancreatectomy and preoperative radiotherapy in patients undergoing pancreatectomy with artery resection. J. Am. Coll. Surg. 2019, 228, 131. [Google Scholar] [CrossRef] [PubMed]
- Del Chiaro, M.; Rangelova, E.; Segersvärd, R.; Arnelo, U. Are there still indications for total pancreatectomy? Updates Surg. 2016, 68, 257–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ando, N.; Kato, H.; Igaki, H.; Shinoda, M.; Ozawa, S.; Shimizu, H.; Nakamura, T.; Yabusaki, H.; Aoyama, N.; Kurita, A.; et al. A randomized trial comparing postoperative adjuvant chemotherapy with cisplatin and 5-fluorouracil versus preoperative chemotherapy for localized advanced squamous cell carcinoma of the thoracic esophagus (jcog9907). Ann. Surg. Oncol. 2012, 19, 68–74. [Google Scholar] [CrossRef]
- Fokas, E.; Allgäuer, M.; Polat, B.; Klautke, G.; Grabenbauer, G.G.; Fietkau, R.; Kuhnt, T.; Staib, L.; Brunner, T.; Grosu, A.L.; et al. Randomized phase ii trial of chemoradiotherapy plus induction or consolidation chemotherapy as total neoadjuvant therapy for locally advanced rectal cancer: Cao/aro/aio-12. J. Clin. Oncol. 2019, 37, 3212–3222. [Google Scholar] [CrossRef]
- Kasi, A.; Abbasi, S.; Handa, S.; Al-Rajabi, R.; Saeed, A.; Baranda, J.; Sun, W. Total neoadjuvant therapy vs standard therapy in locally advanced rectal cancer: A systematic review and meta-analysis. JAMA Netw. Open 2020, 3, e2030097. [Google Scholar] [CrossRef]
- Murphy, J.E.; Wo, J.Y.; Ryan, D.P.; Clark, J.W.; Jiang, W.; Yeap, B.Y.; Drapek, L.C.; Ly, L.; Baglini, C.V.; Blaszkowsky, L.S.; et al. Total neoadjuvant therapy with folfirinox in combination with losartan followed by chemoradiotherapy for locally advanced pancreatic cancer: A phase 2 clinical trial. JAMA Oncol. 2019, 5, 1020–1027. [Google Scholar] [CrossRef]
- Jang, J.Y.; Han, Y.; Lee, H.; Kim, S.W.; Kwon, W.; Lee, K.H.; Oh, D.Y.; Chie, E.K.; Lee, J.M.; Heo, J.S.; et al. Oncological benefits of neoadjuvant chemoradiation with gemcitabine versus upfront surgery in patients with borderline resectable pancreatic cancer: A prospective, randomized, open-label, multicenter phase 2/3 trial. Ann. Surg. 2018, 268, 215–222. [Google Scholar] [CrossRef]
- Unno, M.; Motoi, F.; Matsuyama, Y.; Satoi, S.; Matsumoto, I.; Aosasa, S.; Shirakawa, H.; Wada, K.; Fujii, T.; Yoshitomi, H.; et al. Randomized phase ii/iii trial of neoadjuvant chemotherapy with gemcitabine and s-1 versus upfront surgery for resectable pancreatic cancer (prep-02/jsap-05). J. Clin. Oncol. 2019, 37, 189. [Google Scholar] [CrossRef]
- Uesaka, K.; Boku, N.; Fukutomi, A.; Okamura, Y.; Konishi, M.; Matsumoto, I.; Kaneoka, Y.; Shimizu, Y.; Nakamori, S.; Sakamoto, H.; et al. Adjuvant chemotherapy of s-1 versus gemcitabine for resected pancreatic cancer: A phase 3, open-label, randomised, non-inferiority trial (jaspac 01). Lancet 2016, 388, 248–257. [Google Scholar] [CrossRef]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Choné, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. Folfirinox or gemcitabine as adjuvant therapy for pancreatic cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef] [PubMed]
- Oettle, H.; Post, S.; Neuhaus, P.; Gellert, K.; Langrehr, J.; Ridwelski, K.; Schramm, H.; Fahlke, J.; Zuelke, C.; Burkart, C.; et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: A randomized controlled trial. JAMA 2007, 297, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Stocken, D.D.; Bassi, C.; Ghaneh, P.; Cunningham, D.; Goldstein, D.; Padbury, R.; Moore, M.J.; Gallinger, S.; Mariette, C.; et al. Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: A randomized controlled trial. JAMA 2010, 304, 1073–1081. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Year | Country | N | NAT (%) | Procedures | Reconstruction Method | Study Period | Mortality (%) |
|---|---|---|---|---|---|---|---|---|
| Li [24] | 2004 | China | 11 | ND | PD | Graft 8, interposition from the aorta 3 | 1994–2003 | ND |
| Nakao [10] | 2006 | Japan | 3 | ND | PD, TP | ND | 1981–2005 | 35.7 ** |
| Yekebas [20] | 2008 | Germany | 3 | ND | PD, DP | EEA 1, graft 2 | 1994–2005 | 33 |
| Amano [17] | 2009 | Japan | 12 | 13 ** | PD, TP | EEA 3, SpA transposition 7 *, graft 2 | 2005–2009 | 17 |
| Boggi [25] | 2009 | Italy | 6 | ND | PD | EEA 1, graft 5 | 1987–2004 | 4.0 ** |
| Martin [26] | 2009 | USA | 2 | 100 | PD, TP | Graft 2 | 1999–2007 | 0 |
| Kitagawa [19] | 2011 | Japan | 17 | ND | PD | EEA 1, graft 16 | 2002–2011 | 12 |
| Bockhorn [27] | 2011 | Germany | 3 | ND | PD, TP | Graft 3 | 1994–2004 | 14 ** |
| Rehders [28] | 2012 | Germany | 4 | ND | PD | EEA 3, graft 1 | 2004–2010 | ND |
| Gong [29] | 2013 | China | 10 | ND | PD | ND | 2006–2011 | 6.7 ** |
| Sgroi [30] | 2015 | USA | 4 | 38 ** | PD | EEA 4 | 2003–2013 | ND |
| Glebova [31] | 2016 | USA | 2 | 28 ** | PD | EEA 1, graft 1 | 1989–2014 | ND |
| Perinel [32] | 2016 | France | 6 | 67 | TP | SpA transposition 6 | 2008–2014 | 0 |
| Tee [33] | 2018 | USA | 15 | 75 ** | PD, DP, TP | EEA, graft, or reconstruction † | 1990–2017 | 7.0 |
| Loveday [34] | 2019 | Canada | 10 | 94 ** | PD, DP, TP | EEA, interposition from the aorta † | 2009–2016 | 3.2 ** |
| Bachellier [22] | 2020 | France | 34 | 75 ** | PD, DP, TP | EEA or graft 34 † | 1990–2017 | 5.7 |
| Loos [23] | 2020 | Germany | 30 | 49 ** | PD, DP, TP | EEA, graft, transposition † | 2003–2019 | 6.7 |
| Author | Year | Country | N | NAT (%) | Procedures | Reconstruction Method | Study Period | Mortality (%) |
|---|---|---|---|---|---|---|---|---|
| Li [24] | 2004 | China | 8 | ND | PD | EEA 5, graft 3 | 1994–2003 | ND |
| Nakao [10] | 2006 | Japan | 9 | ND | PD, TP | ND | 1981–2005 | ND |
| Yekebas [20] | 2008 | Germany | 10 | ND | PD, TP, DP | EEA 10 | 1994–2005 | 0 |
| Amano H [17] | 2009 | Japan | 15 | 13 † | PD, TP | EEA 3, GDA 4 *, SpA 6 **, Others 3 | 2005–2009 | 6.7 |
| Boggi [25] | 2009 | Italy | 12 | ND | PD | EEA 6, graft 5, no reconstruction 1 | 1987–2004 | 4 † |
| Martin [26] | 2009 | USA | 3 | 33 | PD, TP | EEA 3 | 1999–2007 | 0 |
| Bockhorn [27] | 2011 | Germany | 18 | ND | PD, TP | EEA 10, graft 8 | 1994–2004 | 14 † |
| Gong [29] | 2013 | China | 5 | ND | PD | ND | 2006–2011 | 6.7 † |
| Amano R [37] | 2015 | Japan | 7 | 100 | PD, TP | EEA 6, no reconstruction 1 | 2012–2013 | 0 |
| Sgroi [30] | 2015 | USA | 7 | 38 † | PD | EEA 7 | 2003–2013 | ND |
| Glebova [31] | 2016 | USA | 18 | 28 † | PD | EEA 15, graft 2, no reconstruction 1 | 1989–2014 | ND |
| Perinel [32] | 2016 | France | 6 | 0 | TP | SpA 3, no reconstruction 3 ‡ | 2008–2014 | 0 |
| Miyazaki [38] | 2017 | Japan | 21 | 43 | PD, TP | EEA1, no reconstruction 20 | 2019–2015 | 0 |
| Tee [33] | 2018 | USA | 60 | 75 † | PD, DP, TP | EEA or graft or reconstruction § | 1990–2017 | 13 |
| Loveday [34] | 2019 | Canada | 10 | 94 † | PD, DP, TP | EEA, interposition from the aorta † | 2009–2016 | 3.2 † |
| Bachellier [22] | 2020 | France | 29 | 75 † | PD, DP, TP | EEA or graft 20 §, no reconstruction 9 § | 1990–2017 | 5.1 † |
| Loos [23] | 2020 | Germany | 85 | 49 † | PD, DP, TP | EEA, graft, transposition § | 2003–2019 | 16.7 |
| Author | Year | Country | N | Study Period | Preoperative Embolization (%) | LGA Flow Preservation (%) | Ischemic Complication (%) | Mortality (%) | |
|---|---|---|---|---|---|---|---|---|---|
| Stomach | Liver | ||||||||
| Klompmaker [49] | 2019 | Europa | 191 | 2000–2016 | 38 | 12 | 11 | 23 | 9.5 |
| Nakamura [50] | 2016 | Japan | 80 | 1998–2015 | 100 | 6.3 | 29 | 6 | 5 |
| Yamamoto [53] | 2017 | Japan | 72 | 2001–2011 | ND | ND | ND | ND | 4.2 |
| Okada [55] | 2018 | Japan | 50 | 2004–2017 | 92 | 46 | 10 | 56 | 8 |
| Yoshitomi [58] | 2019 | Japan | 38 | 2010–2016 | 74 | 0 | 10 | 3 | 3 |
| Ocuin [48] | 2016 | USA | 30 | 2007–2015 | ND | 0 | 7 | ND | 14 |
| Yoshiya [49] | 2019 | Japan | 20 | 2008–2018 | 80 | 0 | 0 | ND | 0 |
| Beane [51] | 2015 | USA | 20 | 2011–2012 | ND | 0 | 0 | 0 | 10 |
| Oba [57] | 2019 | Japan | 18 | 2014–2017 | 0 | 89 | 11 | ND | 0 |
| Author | Year | Country | N | Study Period | Mortality (%) | R0 Resection Rate (%) | Median Survival Time (Months) |
|---|---|---|---|---|---|---|---|
| Brooks [74] | 1989 | USA | 48 | 1970–1986 | 8.3 | ND | 12 |
| Launois [75] | 1993 | France | 47 | 1968–1986 | 15 | ND | 8 |
| Karpoff [4] | 2001 | USA | 35 | 1983–1998 | 5.7 | 82 | 7.9 |
| Schmit [76] | 2007 | USA | 33 | 1992–2006 | 6 | 100 | 18 |
| Reddy [70] | 2009 | USA | 100 | 1970–2007 | 8 | 78 | 12 |
| Nathan [77] | 2009 | USA | 376 | 1998–2004 | 8.6 | ND | 15 |
| Hartwig [71] | 2015 | Germany | 289 | 2001–2012 | 7.8 | ND | 18 |
| Satoi [78] | 2016 | Japan | 45 | 2001–2011 | 0 | 76 | 17 |
| Johnston [79] | 2016 | USA | 2582 | 1998–2004 | 5.5 | 76 | 15 |
| Xiong [80] | 2017 | China | 50 | 2009–2015 | 6 | 90 | 18 |
| Passeri [81] | 2019 | USA | 807 | 1998–2006 | 5.6 | 76 | 17 |
| Hashimoto [82] | 2020 | Japan | 1393 | 2013–2016 | 1.1 | ND | ND |
| Stoop [83] | 2020 | Sweden | 90 | 2008–2017 | 3.4 | ND | ND |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, Y.; Oba, A.; Ono, Y.; Sato, T.; Ito, H.; Takahashi, Y. Radical Resection for Locally Advanced Pancreatic Cancers in the Era of New Neoadjuvant Therapy—Arterial Resection, Arterial Divestment and Total Pancreatectomy. Cancers 2021, 13, 1818. https://doi.org/10.3390/cancers13081818
Inoue Y, Oba A, Ono Y, Sato T, Ito H, Takahashi Y. Radical Resection for Locally Advanced Pancreatic Cancers in the Era of New Neoadjuvant Therapy—Arterial Resection, Arterial Divestment and Total Pancreatectomy. Cancers. 2021; 13(8):1818. https://doi.org/10.3390/cancers13081818
Chicago/Turabian StyleInoue, Yosuke, Atushi Oba, Yoshihiro Ono, Takafumi Sato, Hiromichi Ito, and Yu Takahashi. 2021. "Radical Resection for Locally Advanced Pancreatic Cancers in the Era of New Neoadjuvant Therapy—Arterial Resection, Arterial Divestment and Total Pancreatectomy" Cancers 13, no. 8: 1818. https://doi.org/10.3390/cancers13081818