
Surgical Management of the Axilla in Clinically Node-Positive Breast Cancer Patients Converting to Clinical Node Negativity through Neoadjuvant Chemotherapy: Current Status, Knowledge Gaps, and Rationale for the EUBREAST-03 AXSANA Study


 , , , , , , ,
, , , , , , ,  , , , , , , ,
, , , , , , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Targeted Axillary Dissection: More Questions Open Than Answered
2.1. Which Marking Technique Is Optimal?
2.2. How Many Nodes Should Be Marked?
2.3. When Should Lymph Nodes Be Marked?
2.4. What to Do in Case of a “Lost Marker”?
2.5. Is TAD Safe for All Patients?
2.6. Beyond Surgical Therapy: Which Fields Should Be Irradiated after TAD?
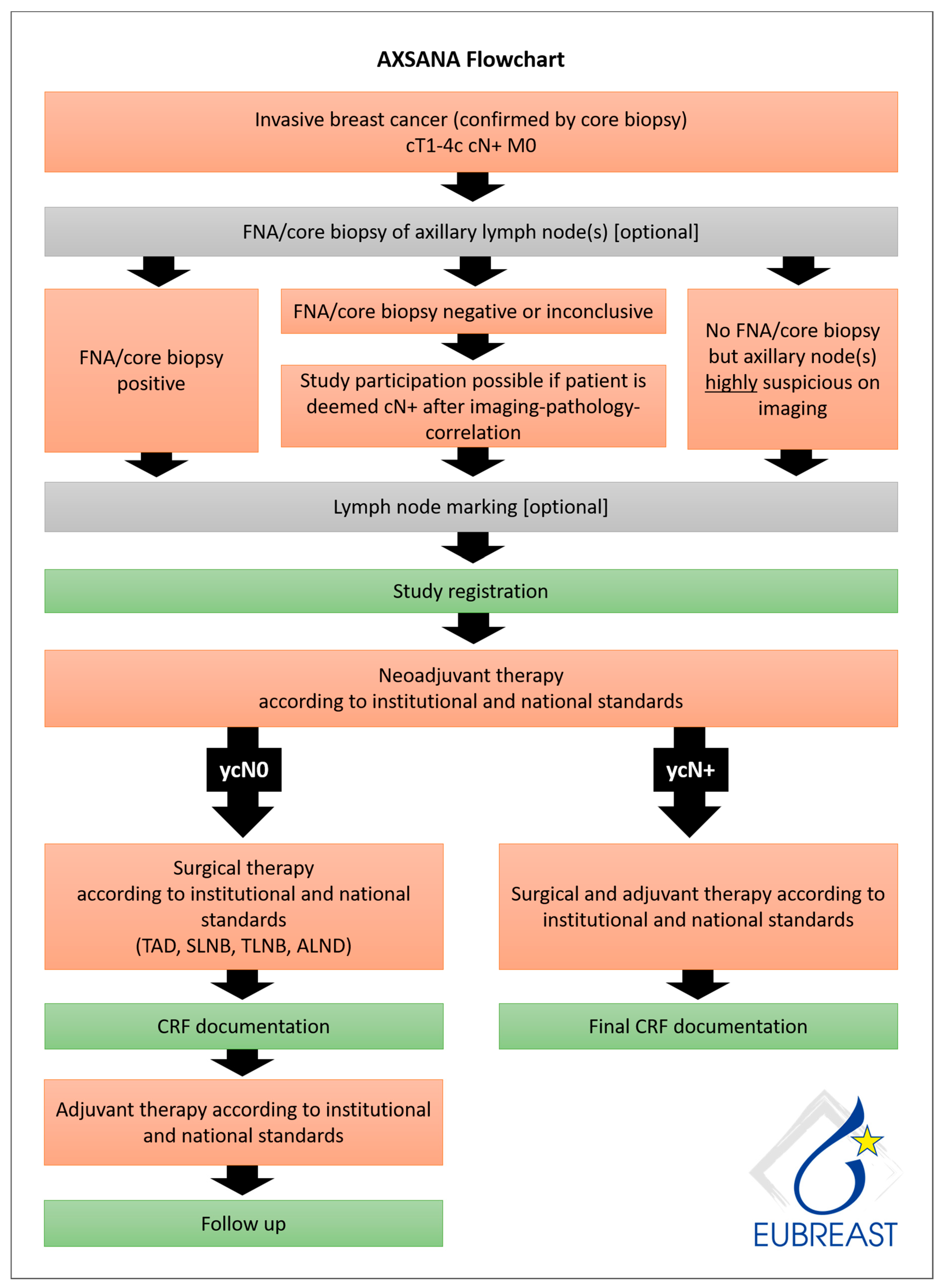
3. The AXSANA Study: Which Axillary Strategy Is Optimal in the cN+ → ycN0 Setting?
- 5-year invasive disease-free survival (iDFS)
- 3-year axillary recurrence rate
- Quality of life and arm morbidity
- Feasibility of different axillary staging strategies assessed by detection rates for SLN and/or TLN
- Success rate of nodal staging using different axillary staging techniques
- Number of removed lymph nodes and their association to complications, arm morbidity, and quality of life
- Operating time as a surrogate parameter for surgical resources
- Proportion of node-positive patients according to the strategy used (as a surrogate parameter for FNR)
- Factors associated with successful detection of the TLN
- Impact of learning curve on success rates of TAD
- Surgical standards of care in different European countries
- Treatment decisions in case of ypN+ status following NACT (ALND vs. radiation therapy)
- iDFS in patients with ypN+ status who received ALND or radiotherapy or both
- Analysis of factors contributing to a decreased quality of life and subjective symptoms of arm morbidity, i.e., baseline quality of life and sense of coherence, extent of axillary surgery, and other locoregional and systemic therapies received
- Economic resources required for different axillary staging strategies and techniques (material costs, operating time, etc.)
- Which staging technique should be recommended to cN+ patients converting to ycN0?
- Is imaging helpful in identifying patients most likely to achieve pCR in the axilla? If yes, which method should be recommended?
- Should cN1 and cN2/3 patients be offered different surgical strategies for axillary staging?
- Which lymph node marking technique offers highest rates of successful TAD/TLNB?
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Members of the AXSANA Study Group
| Achim Rody | Lelia Bauer |
| Agnieszka Lawnicka | Manfred Hofmann |
| Alexander Emelyanov | Manuela Seixas |
| Alexander Miller | Maria Hufnagel |
| Anastasia Fleuster | Maria Joao Cardoso |
| Andrea Hasse | Marina Mangold |
| Andrea Papadia | Marjut Leidenius |
| Andrea Stefek | Markus Hahn |
| Andreas Rempen | Markus Keller |
| Andreas Schnelzer | Martin C. Koch |
| Andree Faridi | Matthias Frank |
| Angelika Jursik | Michael Berghorn |
| Anja Graf | Michael Burkhardt |
| Anke Klein-Tebbe | Michael David Mueller |
| Antje Nixdorf | Michael Schrauder |
| Antonio Jesus Esgueva Colmenarejo | Michael Untch |
| Arzu Akan | Michael Weigel |
| Atakan Sezer | Michal Bak |
| Aysegul Aktas | Muneer Mansour |
| Barbara Schlesinger | Mustafa Aydogdu |
| Beatrix Janke | Mustafa Celalettin Ugur |
| Benno Lex | Nana Bündgen |
| Carina Paschold | Natalia Krawczyk |
| Carolin Nestle-Krämling | Natalija Deuerling |
| Cem Yilmaz | Nicole Rotmensz |
| Christine Ankel | Nicoleta Zenovia Antone |
| Christoph Anthuber | Nina Ditsch |
| Christoph Großmann | Ninette Scharle |
| Cihan Uras | Oliver Behrens |
| Claudia Rauh | Oliver Hoffmann |
| Cordula Müller | Oumar Camara |
| Cornelia Meisel | Pavlina Diem |
| Cumhur Arici | Petra Bolkenius |
| Daniela Dieterle | Prodromos Kanavidis |
| Daniele Bolla | Renu Buss-Steidle |
| Dirk G. Kieback | Ricardo Felberbaum |
| Dirk-Michael Watermann | Richard Berger |
| Dorothea Fischer | Roberto Rodriguez |
| Eike Simon | Rodoniki Iosifidou |
| Ekkehard von Abel | Roland Csorba |
| Elisabeth Thiemann | Sabine Lemster |
| Elke Faust | Sabine Riemer |
| Elke Keil | Sandra Rauen |
| Elvira Schomann | Sarah Fröhlich |
| Emmanuel Barranger | Sebastian Wojcinski |
| Enes Arikan | Semra Gunay |
| Eva-Maria Jahn | Sibel Ozkan Gurdal |
| Felix Hilpert | Sibylle Perez |
| Florian Ebner | Silke Mattes |
| Francesco Meani | Sonja Cárdenas-Ovalle |
| Frank Beldermann | Stefan Hupfer |
| Gabriele Feisel-Schwickardi | Stefan Paepke |
| Gabriele Kaltenecker | Stefan Renner |
| Gunay Gurleyik | Stefanie Buchen |
| Hanna Barmettler | Stefanie Strobel |
| Hanna Karlsson | Steffen Liebers |
| Hans-Christian Kolberg | Stephan Hasmüller |
| Hans-Joachim Strittmatter | Stephan Seitz |
| Hasan Karanlik | Sudip Kundu |
| Heiko Graf | Susanne Albrecht |
| Helena Ikonomidis Sackey | Susanne Bucher |
| Henning Eichler | Susanne Kraudelt |
| Inga Bekes | Susanne Steer |
| Ingo Bauerfeind | Susen Schirrmeister |
| Ingo Thalmann | Sven-Thomas Graßhoff |
| Ingrid Buck | Tanja Fehm |
| Ioannis Natsiopoulos | Tanja Wanik |
| Isabelle Himsl | Telja Pursche |
| Isabelle Utz-Billing | Thomas Hawighorst |
| Jana Shabbir | Thomas Müller |
| Jeanette Zeppenfeld | Thomas Papathemilis |
| Jenci Palatty | Tuomo Meretoja |
| Jens Paul Seldte | Umit Ugurlu |
| Jens Schnabel | Ursula Makowiec |
| Joachim Rom | Ursula Scholz |
| Jose Ignacio Sanchez Mendez | Ute-Susann Albert |
| Jürgen Schuster | Vasileios Sevas |
| Jutta Lefarth | Veli Vural |
| Karen Wimmer | Visnja Fink |
| Kathrin Engelken | Vlad Alexandru Gata |
| Katja Vassilev | Volker Hanf |
| Katrin Sawitzki | Wencke Ruhwedel |
| Kerstin Hilmer | Wolfram Seifert |
| Kerstin Ramaker | Yvonne Wengström |
| Kilian Pankert |
Appendix A.2. Active Study Sites
| Klinikum Esslingen |
| UFK Rostock |
| Leopoldina-Krankenhaus |
| Städtisches Klinikum Karlsruhe Frauenklinik |
| Klinikum Aschaffenburg-Alzenau |
| Klinikum Stuttgart-Frauenklinik |
| MVZ Klinik Dr. Hancken GmbH |
| Marienhospital Bottrop gGmbH |
| Kreiskrankenhaus Bergstraße GmbH |
| Klinikum Memmingen |
| Brustzentrum Pinneberg |
| Ortenau Klinikum Offenburg-Kehl |
| Klinikum Fichtelgebierge |
| Klinikum Ansbach |
| Brustzentrum, Sana Klinikum Berlin Lichtenberg |
| RWTH Uniklinik Aachen |
| Medius Klinik Nürtingen |
| Klinikum St. Marien Amberg |
| Klinikum Landkreis Tuttlingen |
| Brustzentrum Diakonieklinikum Stuttgart |
| Brustzentrum Südbaden |
| WKK Westküstenkliniken Heide |
| Marienhospital Stuttgart |
| AKH Celle |
| Vidia Christliche Kliniken Karlsruhe Diakonissenkrankenhaus |
| Agaplesion Krankenhaus Frankfurt |
| Klinikum Gütersloh |
| Siloah St Trudpert Klinikum |
| Brustzentrum Donau-Riß, Alb-Donau-Klinikum Ehingen |
| Franziskus Hospital Bielefeld |
| Brustzentrum Gelnhausen |
| München Klinik Harlaching Frauenklinik |
| Kreiskrankenhaus Torgau |
| Imland gGmbH Rendsburg |
| Friedrich-Ebert-Krankenhaus |
| Brustzentrum Sömmerda |
| Klinikum Hanau GmbH |
| Brustzentrum Osnabrück/Niels-Stensen-Kliniken |
| Klinikum Darmstadt |
| Agaplesion Ev. Klinikum Schaumburg |
| Diakoneo Diakonie-Klinikum Schwäbisch Hall |
| Rems-Murr-Kliniken-Winnenden |
| Brustzentrum Oberhavel |
| GRN Klinikum Weinheim |
| Kreisklinik Ebersberg |
| RKH Krankenhaus Bietigheim-Vaihingen |
| Asklepios Klinik Wiesbaden |
| Kliniken Heidenheim |
| Klinikum Dortmund gGmbh, Frauenklinik |
| KRH Robert-Koch-Klinikum Gehrden |
| SLK-Kliniken Heilbronn |
| Martin-Luther-KH Berlin |
| Brustzentrum Fürth |
| Frauenklinik Ulm |
| Sana Kliniken Ostholstein Eutin |
| Brustkrebszentrum Kaufbeuren |
| Klinikum Kulmbach |
| Klinikum Fulda |
| Helios Klinikum Pforzheim |
| Brustzentrum Nordsachsen Borna, Sana Klinikum Leipziger Land |
| Klinikverbund Allgäu gGmbH |
| Helios Klinikum Berlin-Buch |
| Klinikum Passau |
| Klinikum Dritter Orden, München |
| Euregio Brustzentrum Eschweiler |
| DRK Krankenhaus Chemnitz Rabenstein |
| Diako Flensburg |
| Klinikum Ernst von Bergmann |
| Brustzentrum Helios Klinikum Meiningen |
| Stauferklonikum Mutlangen |
| Helios Klinikum Rottweil |
| Frauenklinik Böblingen |
| Sana Klinikum Biberach |
| Klinikum rechts der Isar |
| Klinikum Starnberg Frauenklinik |
| DRK Kliniken Berlin |
| Städtisches Klinikum Solingen |
| Evangelisches KH Wesel |
| Brustzentrum Elisabeth Krankenhaus Kassel |
| Laiko Hospital, National and Kapodistrian University of Athens, Athens |
| Interbalkan Medical Center of Thessaloniki |
| Anticancer Hospital Theageneio |
| Clinica Universidad de Navarra, Madrid |
| Hospital Clinic Barcelona |
| Hospital Universitario La Paz-Unidad de Mama |
| University of the University of the Italian Switzerland, Ente Ospedaliero Cantonale, Ospedale Regionale di Lugano |
| Luzerner Kantonsspital, Luzern |
| Spital Region Oberaargau |
| Zonguldak Bulent Ecevit University, The School of Medicine |
| Trakya University Te School of Medicine |
| Ministry of Health Istanbul Provincial Health Directorate Prof. Dr. Cemil Taşcioğlu City Hospital |
| Marmara University, The School of Medicine |
| Ministry of Health Istanbul Provincial Health Directorate Istanbul Haydarpasa Numune Research and Training Hospital |
| Akdeniz University, The School of Medicine |
| Namik Kemal University, The School of Medicine |
| Istanbul University Oncology Institute |
| Istanbul Oncology Hospital |
| Acibadem University Research Institute of Senology |
References
- Classe, J.M.; Loaec, C.; Gimbergues, P.; Alran, S.; de Lara, C.T.; Dupre, P.F.; Rouzier, R.; Faure, C.; Paillocher, N.; Chauvet, M.P.; et al. Sentinel lymph node biopsy without axillary lymphadenectomy after neoadjuvant chemotherapy is accurate and safe for selected patients: The GANEA 2 study. Breast Cancer Res. Treat. 2019, 173, 343–352. [Google Scholar] [CrossRef]
- Hunt, K.K.; Yi, M.; Mittendorf, E.A.; Guerrero, C.; Babiera, G.V.; Bedrosian, I.; Hwang, R.F.; Kuerer, H.M.; Ross, M.I.; Meric-Bernstam, F. Sentinel lymph node surgery after neoadjuvant chemotherapy is accurate and reduces the need for axillary dissection in breast cancer patients. Ann. Surg. 2009, 250, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Kahler-Ribeiro-Fontana, S.; Pagan, E.; Magnoni, F.; Vicini, E.; Morigi, C.; Corso, G.; Intra, M.; Canegallo, F.; Ratini, S.; Leonardi, M.C.; et al. Long-term standard sentinel node biopsy after neoadjuvant treatment in breast cancer: A single institution ten-year follow-up. Eur. J. Surg. Oncol. 2021, 47, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, T.; Bauerfeind, I.; Fehm, T.; Fleige, B.; Hausschild, M.; Helms, G.; Lebeau, A.; Liedtke, C.; von Minckwitz, G.; Nekljudova, V.; et al. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): A prospective, multicentre cohort study. Lancet Oncol. 2013, 14, 609–618. [Google Scholar] [CrossRef]
- Boughey, J.C.; Suman, V.J.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Leitch, A.M.; Kuerer, H.M.; Bowling, M.; Flippo-Morton, T.S.; et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: The ACOSOG Z1071 (Alliance) clinical trial. JAMA 2013, 310, 1455–1461. [Google Scholar] [CrossRef] [Green Version]
- Chehade, H.E.H.; Headon, H.; El Tokhy, O.; Heeney, J.; Kasem, A.; Mokbel, K. Is sentinel lymph node biopsy a viable alternative to complete axillary dissection following neoadjuvant chemotherapy in women with node-positive breast cancer at diagnosis? An updated meta-analysis involving 3,398 patients. Am. J. Surg. 2016, 212, 969–981. [Google Scholar] [CrossRef]
- Boughey, J.C.; Ballman, K.V.; Le-Petross, H.T.; McCall, L.M.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Feliberti, E.C.; Hunt, K.K. Identification and Resection of Clipped Node Decreases the False-negative Rate of Sentinel Lymph Node Surgery in Patients Presenting With Node-positive Breast Cancer (T0-T4, N1-N2) Who Receive Neoadjuvant Chemotherapy: Results From ACOSOG Z1071 (Alliance). Ann. Surg. 2016, 263, 802–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caudle, A.S.; Yang, W.T.; Krishnamurthy, S.; Mittendorf, E.A.; Black, D.M.; Gilcrease, M.Z.; Bedrosian, I.; Hobbs, B.P.; DeSnyder, S.M.; Hwang, R.F.; et al. Improved Axillary Evaluation Following Neoadjuvant Therapy for Patients With Node-Positive Breast Cancer Using Selective Evaluation of Clipped Nodes: Implementation of Targeted Axillary Dissection. J. Clin. Oncol. 2016, 34, 1072–1078. [Google Scholar] [CrossRef] [Green Version]
- NCCN Clinical Practice Guidelines in Oncology, Breast Cancer, Version 1.2021—15 January 2021. NCCN.org. 2021. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx#breast (accessed on 27 March 2021).
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E.; Committee, E.G. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1674. [Google Scholar] [CrossRef] [Green Version]
- Recommendations of the AGO Breast Committee: Diagnosis and Treatment of Patients with early and advanced Breast Cancer. Available online: www.ago-online.de (accessed on 27 March 2021).
- Banys-Paluchowski, M.; Gruber, I.V.; Hartkopf, A.; Paluchowski, P.; Krawczyk, N.; Marx, M.; Brucker, S.; Hahn, M. Axillary ultrasound for prediction of response to neoadjuvant therapy in the context of surgical strategies to axillary dissection in primary breast cancer: A systematic review of the current literature. Arch. Gynecol. Obstet. 2020, 301, 341–353. [Google Scholar] [CrossRef]
- Consensus Guideline on the Management of the Axilla in Patients with Invasive/In-Situ Breast Cancer. The American Society of Breast Surgeons. 2019. Available online: https://www.breastsurgeons.org/docs/statements/Consensus-Guideline-on-the-Management-of-the-Axilla.pdf?v2 (accessed on 27 March 2021).
- Finnish Breast Cancer Group. Rintasyöpäryhmän Valtakunnallinen Diagnostiikka—Ja Hoitosuositus. Available online: https://1587667.167.directo.fi/@Bin/c554c241df494d864925e07ad6aa705e/1614023914/application/pdf/186425/SRSR_Suositus_2019%20Joulukuu.pdf (accessed on 1 December 2019).
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): S3-Leitlinie Früherkennung, Diagnose, Therapie und Nachsorge des Mammakarzinoms, Version 4.3, AWMF Registernummer: 032-045OL. Available online: http://www.leitlinienprogramm-onkologie.de/leitlinien/mammakarzinom/ (accessed on 10 June 2020).
- Lazar, G.; Kelemen, P.; Kosa, C.; Maraz, R.; Paszt, A.; Pavlovics, G.; Savolt, A.; Simonka, Z.; Toth, D.; Matrai, Z. Modern surgical treatment of breast cancer. 4th Breast Cancer Consensus Conference. Magy Onkol. 2020, 64, 329–346. [Google Scholar] [PubMed]
- Indian Council of Medical Research Consensus Document for Management of Breast Cancer; Department of Health Research MoHFW: New Delhi, India, 2016.
- Recommendations of the Polish Society of Surgical Oncology (Surgical Treatment in Breast Neoplasms: Second Consensus). 2019. Available online: https://journals.viamedica.pl/oncology_in_clinical_practice/article/view/OCP.2017.0015/43197 (accessed on 27 March 2021).
- Ghid de Management al Cancerului Mamar. Available online: http://old.ms.ro/index.php?pag=181&pg=5 (accessed on 1 December 2009).
- Peltecu, G.; Median, D.; Vlad, Ș.; Tuinea, L.; Iancu, G.; Gică, N.; Nedelea, F.; Cigăran, R.; Chirculescu, R.; Lesaru, M.; et al. Cancerul Mamar. Societatea de Obstetrica si Ginecologie. Available online: https://sogr.ro/wp-content/uploads/2019/06/30.-Cancerul-mamar.pdf (accessed on 26 February 2021).
- Bröstcancer-Nationellt Vårdprogram-SweBCG, 2020-02-11 Version: 3.0. Available online: http://www.swebcg.se/wp-content/uploads/2016/10/nationellt-vardprogram-brostcancer_200211.pdf (accessed on 1 December 2020).
- Neoadjuverende Kemoterapi ved Brystkræft mhp. Down-Sizing og Down-Staging. In Danish Breast Cancer Group Guidelines; Danish Breast Cancer Group: Aarhus, Denmark, 2016. [Google Scholar]
- Associazione Italiana di Oncologia Medica (AIOM). Breast Neoplasms Guidelines, 2018 ed.; Associazione Italiana di Oncologia Medica (AIOM): Milan, Italy, 2019. [Google Scholar]
- IX Consenso Nacional de Cancro de Mama; Sociedade Portuguesa de Senologia: Coimbra, Portugal, 2017.
- Clinical Guidelines Mammary Cancer; Прoфессиoнальные Aссoциации: Ассoциация oнкoлoгoв Рoссии Рoссийскoе oбществo клиническoй oнкoлoгии: Moscow, Russia, 2018.
- De La Peña, F.A.; Andrés, R.; Garcia-Sáenz, J.A.; Manso, L.; Margelí, M.; Dalmau, E.; Pernas, S.; Prat, A.; Servitja, S.; Ciruelos, E. SEOM clinical guidelines in early stage breast cancer (2018). Clin. Transl. Oncol. 2019, 21, 18–30. [Google Scholar] [CrossRef] [Green Version]
- Boileau, J.F.; Poirier, B.; Basik, M.; Holloway, C.M.; Gaboury, L.; Sideris, L.; Meterissian, S.; Arnaout, A.; Brackstone, M.; McCready, D.R.; et al. Sentinel node biopsy after neoadjuvant chemotherapy in biopsy-proven node-positive breast cancer: The SN FNAC study. J. Clin. Oncol. 2015, 33, 258–264. [Google Scholar] [CrossRef]
- Reinisch, M.; Heil, J.; Rüland, A.; Seiberling, C.; Harrach, H.; Schindowski, D.; Lubitz, J.; Ankel, C.; Grasshoff, S.T.; Deuschle, P.; et al. Prospective, multicenter registry trial to evaluate the clinical feasibility of targeted axillary dissection (TAD) in patients (pts) with breast cancer (BC) and core biopsy proven axillary involvement (cN+). Ann. Oncol. 2019, 30, v56. [Google Scholar] [CrossRef]
- Kuemmel, S.; Heil, J.; Rueland, A.; Seiberling, C.; Harrach, H.; Schindowski, D.; Lubitz, J.; Hellerhoff, K.; Ankel, C.; Grasshoff, S.T.; et al. A Prospective, Multicenter Registry Study to Evaluate the Clinical Feasibility of Targeted Axillary Dissection (TAD) in Node-Positive Breast Cancer Patients. Ann. Surg. 2020, 4. [Google Scholar] [CrossRef] [PubMed]
- Plecha, D.; Bai, S.; Patterson, H.; Thompson, C.; Shenk, R. Improving the Accuracy of Axillary Lymph Node Surgery in Breast Cancer with Ultrasound-Guided Wire Localization of Biopsy Proven Metastatic Lymph Nodes. Ann. Surg. Oncol. 2015, 22, 4241–4246. [Google Scholar] [CrossRef]
- Laws, A.; Dillon, K.; Kelly, B.N.; Kantor, O.; Hughes, K.S.; Gadd, M.A.; Smith, B.L.; Lamb, L.R.; Specht, M. Node-Positive Patients Treated with Neoadjuvant Chemotherapy Can Be Spared Axillary Lymph Node Dissection with Wireless Non-Radioactive Localizers. Ann. Surg. Oncol. 2020, 27, 4819–4827. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Hieken, T.J.; Glazebrook, K.N.; Boughey, J.C. Localizing the Clipped Node in Patients with Node-Positive Breast Cancer Treated with Neoadjuvant Chemotherapy: Early Learning Experience and Challenges. Ann. Surg. Oncol. 2017, 24, 3011–3016. [Google Scholar] [CrossRef] [PubMed]
- Simons, J.M.; Scoggins, M.E.; Kuerer, H.M.; Krishnamurthy, S.; Yang, W.T.; Sahin, A.A.; Shen, Y.; Lin, H.; Bedrosian, I.; Mittendorf, E.A.; et al. Prospective Registry Trial Assessing the Use of Magnetic Seeds to Locate Clipped Nodes After Neoadjuvant Chemotherapy for Breast Cancer Patients. Ann. Surg. Oncol. 2021, 8, 1–7. [Google Scholar] [CrossRef]
- Siso, C.; de Torres, J.; Esgueva-Colmenarejo, A.; Espinosa-Bravo, M.; Rus, N.; Cordoba, O.; Rodriguez, R.; Peg, V.; Rubio, I.T. Intraoperative Ultrasound-Guided Excision of Axillary Clip in Patients with Node-Positive Breast Cancer Treated with Neoadjuvant Therapy (ILINA Trial): A New Tool to Guide the Excision of the Clipped Node After Neoadjuvant Treatment. Ann. Surg. Oncol. 2018, 25, 784–791. [Google Scholar] [CrossRef]
- Sun, J.; Henry, D.A.; Carr, M.J.; Yazdankhahkenary, A.; Laronga, C.; Lee, M.C.; Hoover, S.J.; Sun, W.; Czerniecki, B.J.; Khakpour, N.; et al. Feasibility of Axillary Lymph Node Localization and Excision Using Radar Reflector Localization. Clin. Breast Cancer 2020. In Press. [Google Scholar] [CrossRef]
- Hartmann, S.; Reimer, T.; Gerber, B.; Stubert, J.; Stengel, B.; Stachs, A. Wire localization of clip-marked axillary lymph nodes in breast cancer patients treated with primary systemic therapy. Eur. J. Surg. Oncol. 2018, 44, 1307–1311. [Google Scholar] [CrossRef]
- Diego, E.J.; McAuliffe, P.F.; Soran, A.; McGuire, K.P.; Johnson, R.R.; Bonaventura, M.; Ahrendt, G.M. Axillary Staging After Neoadjuvant Chemotherapy for Breast Cancer: A Pilot Study Combining Sentinel Lymph Node Biopsy with Radioactive Seed Localization of Pre-treatment Positive Axillary Lymph Nodes. Ann. Surg. Oncol. 2016, 23, 1549–1553. [Google Scholar] [CrossRef]
- Martínez, A.M.; Roselló, I.V.; Gómez, A.S.; Catanese, A.; Molina, M.P.; Suarez, M.S.; Miguel, I.P.; Aulina, L.B.; Gozálvez, C.R.; Ibáñez, J.F.J.; et al. Advantages of preoperative localization and surgical resection of metastatic axillary lymph nodes using magnetic seeds after neoadjuvant chemotherapy in breast cancer. Surg. Oncol. 2021, 36, 28–33. [Google Scholar] [CrossRef]
- Kim, W.H.; Kim, H.J.; Kim, S.H.; Jung, J.H.; Park, H.Y.; Lee, J.; Kim, W.W.; Park, J.Y.; Chae, Y.S.; Lee, S.J. Ultrasound-guided dual-localization for axillary nodes before and after neoadjuvant chemotherapy with clip and activated charcoal in breast cancer patients: A feasibility study. BMC Cancer 2019, 19, 859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balasubramanian, R.; Morgan, C.; Shaari, E.; Kovacs, T.; Pinder, S.E.; Hamed, H.; Sever, A.R.; Kothari, A. Wire guided localisation for targeted axillary node dissection is accurate in axillary staging in node positive breast cancer following neoadjuvant chemotherapy. Eur. J. Surg. Oncol. 2020, 46, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Lim, G.H.; Teo, S.Y.; Gudi, M.; Ng, R.P.; Pang, J.; Tan, Y.S.; Lee, Y.S.; Allen, J.C., Jr.; Leong, L.C.H. Initial results of a novel technique of clipped node localization in breast cancer patients postneoadjuvant chemotherapy: Skin Mark clipped Axillary nodes Removal Technique (SMART trial). Cancer Med. 2020, 9, 1978–1985. [Google Scholar] [CrossRef] [PubMed]
- Lim, G.H.; Gudi, M.; Teo, S.Y.; Ng, R.P.; Yan, Z.; Lee, Y.S.; Allen, J.C., Jr.; Leong, L.C.H. Would Removal of All Ultrasound Abnormal Metastatic Lymph Nodes Without Sentinel Lymph Node Biopsy Be Accurate in Patients with Breast Cancer with Neoadjuvant Chemotherapy? Oncologist 2020, 25, e1621–e1627. [Google Scholar] [CrossRef]
- Simons, J.; Nijnatten, T.J.V.; Koppert, L.B.; van der Pol, C.C.; Diest, P.J.V.; Jager, A.; Klaveren, D.V.; Kam, B.L.; Lobbes, M.B.; de Boer, M.; et al. Radioactive Iodine Seed placement in the Axilla with Sentinel lymph node biopsy after neoadjuvant chemotherapy in breast cancer: Results of the prospective multicenter RISAS trial. Gen. Sess. Abstr. 2021, 81, GS1-10. [Google Scholar]
- Donker, M.; Straver, M.E.; Wesseling, J.; Loo, C.E.; Schot, M.; Drukker, C.A.; van Tinteren, H.; Sonke, G.S.; Rutgers, E.J.; Peeters, M.J.V. Marking axillary lymph nodes with radioactive iodine seeds for axillary staging after neoadjuvant systemic treatment in breast cancer patients: The MARI procedure. Ann. Surg. 2015, 261, 378–382. [Google Scholar] [CrossRef] [Green Version]
- Thill, M.; Khandan, F.; Schnitzbauer, T. Magseed®-basierte Langzeitmarkierung von Target Lymphknoten bei Patientinnen mit einem Mammakarzinom im Frühstadium unter neoadjuvanter Therapie—Erste Erfahrungen und Perspektiven. GebFra 2020, 80. [Google Scholar] [CrossRef]
- Malter, W.; Eichler, C.; Hanstein, B.; Mallmann, P.; Holtschmidt, J. First Reported Use of Radiofrequency Identification (RFID) Technique for Targeted Excision of Suspicious Axillary Lymph Nodes in Early Stage Breast Cancer—Evaluation of Feasibility and Review of Current Recommendations. Vivo 2020, 34, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, S.; Stachs, A.; Kühn, T.; Winckelmann, A.; De Boniface, J.; Gerber, B.; Reimer, T. Target Lymph Node Biopsy (TLNB) nach Kohlenstoffmarkierung bei Mammakarzinom-Patientinnen im Rahmen der primären Systemtherapie—Ergebnisse der TATTOO-Studie (DGGG-Kongress). GebFra 2020, 80, 61. [Google Scholar] [CrossRef]
- Natsiopoulos, I.; Intzes, S.; Liappis, T.; Zarampoukas, K.; Zarampoukas, T.; Zacharopoulou, V.; Papazisis, K. Axillary Lymph Node Tattooing and Targeted Axillary Dissection in Breast Cancer Patients Who Presented as cN+ Before Neoadjuvant Chemotherapy and Became cN0 After Treatment. Clin. Breast Cancer 2019, 19, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Allweis, T.M.; Menes, T.; Rotbart, N.; Rapson, Y.; Cernik, H.; Bokov, I.; Diment, J.; Magen, A.; Golan, O.; Levi-Bendet, N.; et al. Ultrasound guided tattooing of axillary lymph nodes in breast cancer patients prior to neoadjuvant therapy, and identification of tattooed nodes at the time of surgery. Eur. J. Surg. Oncol. 2020, 46, 1041–1045. [Google Scholar] [CrossRef]
- Khallaf, E.; Wessam, R.; Abdoon, M. Targeted axillary dissection of carbon-tattooed metastatic lymph nodes in combination with post-neo-adjuvant sentinel lymph node biopsy using 1% methylene blue in breast cancer patients. Breast J. 2020, 26, 1061–1063. [Google Scholar] [CrossRef] [PubMed]
- Gatek, J.; Petru, V.; Kosac, P.; Ratajsky, M.; Duben, J.; Dudesek, B.; Jancik, P.; Zabojnikova, M.; Katrusak, J.; Opelova, P.; et al. Targeted axillary dissection with preoperative tattooing of biopsied positive axillary lymph nodes in breast cancer. Neoplasma 2020, 67, 1329–1334. [Google Scholar] [CrossRef]
- Choy, N.; Lipson, J.; Porter, C.; Ozawa, M.; Kieryn, A.; Pal, S.; Kao, J.; Trinh, L.; Wheeler, A.; Ikeda, D.; et al. Initial results with preoperative tattooing of biopsied axillary lymph nodes and correlation to sentinel lymph nodes in breast cancer patients. Ann. Surg. Oncol. 2015, 22, 377–382. [Google Scholar] [CrossRef]
- Van Nijnatten, T.J.A.; Simons, J.M.; Smidt, M.L.; van der Pol, C.C.; van Diest, P.J.; Jager, A.; van Klaveren, D.; Kam, B.L.R.; Lobbes, M.B.I.; de Boer, M.; et al. A Novel Less-invasive Approach for Axillary Staging after Neoadjuvant Chemotherapy in Patients with Axillary Node-positive Breast Cancer by Combining Radioactive Iodine Seed Localization in the Axilla with the Sentinel Node Procedure (RISAS): A Dutch Prospective Multicenter Validation Study. Clin. Breast Cancer 2017, 17, 399–402. [Google Scholar] [CrossRef] [PubMed]
- Gera, R.; Tayeh, S.; Al-Reefy, S.; Mokbel, K. Evolving Role of Magseed in Wireless Localization of Breast Lesions: Systematic Review and Pooled Analysis of 1,559 Procedures. Anticancer Res. 2020, 40, 1809–1815. [Google Scholar] [CrossRef]
- Kasem, I.; Mokbel, K. Savi Scout(R) Radar Localisation of Non-palpable Breast Lesions: Systematic Review and Pooled Analysis of 842 Cases. Anticancer Res. 2020, 40, 3633–3643. [Google Scholar] [CrossRef]
- Lowes, S.; Bell, A.; Milligan, R.; Amonkar, S.; Leaver, A. Use of Hologic LOCalizer radiofrequency identification (RFID) tags to localise impalpable breast lesions and axillary nodes: Experience of the first 150 cases in a UK breast unit. Clin. Radiol. 2020, 75, 942–949. [Google Scholar] [CrossRef]
- McGugin, C.; Spivey, T.; Coopey, S.; Smith, B.; Kelly, B.; Gadd, M.; Hughes, K.; Dontchos, B.; Specht, M. Radiofrequency identification tag localization is comparable to wire localization for non-palpable breast lesions. Breast Cancer Res. Treat. 2019, 177, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Glaeser, A.; Sinn, H.P.; Garcia-Etienne, C.; Riedel, F.; Hug, S.; Schaefgen, B.; Golatta, M.; Hennigs, A.; Feisst, M.; Sohn, C.; et al. Heterogeneous Responses of Axillary Lymph Node Metastases to Neoadjuvant Chemotherapy are Common and Depend on Breast Cancer Subtype. Ann. Surg. Oncol. 2019, 26, 4381–4389. [Google Scholar] [CrossRef] [PubMed]
- United State Nuclear Regulatory Commission. Low Activity Radioactive Seeds Used for Localization of Non-Palpable Lesions and Lymph Nodes, Licensing Guidance, Revision 1. Available online: https://www.nrc.gov/docs/ML1619/ML16197A568.pdf (accessed on 1 December 2016).
- Kirkilesis, G.; Constantinidou, A.; Kontos, M. False negativity of targeted axillary dissection in breast cancer. Breast Care 2021. In Press. [Google Scholar] [CrossRef]
- Kantor, O.; Sipsy, L.M.; Yao, K.; James, T.A. A Predictive Model for Axillary Node Pathologic Complete Response after Neoadjuvant Chemotherapy for Breast Cancer. Ann. Surg. Oncol. 2018, 25, 1304–1311. [Google Scholar] [CrossRef] [PubMed]
- Tadros, A.B.; Yang, W.T.; Krishnamurthy, S.; Rauch, G.M.; Smith, B.D.; Valero, V.; Black, D.M.; Lucci, A., Jr.; Caudle, A.S.; DeSnyder, S.M.; et al. Identification of Patients With Documented Pathologic Complete Response in the Breast After Neoadjuvant Chemotherapy for Omission of Axillary Surgery. JAMA Surg. 2017, 152, 665–670. [Google Scholar] [CrossRef]
- Barron, A.U.; Hoskin, T.L.; Day, C.N.; Hwang, E.S.; Kuerer, H.M.; Boughey, J.C. Association of Low Nodal Positivity Rate Among Patients With ERBB2-Positive or Triple-Negative Breast Cancer and Breast Pathologic Complete Response to Neoadjuvant Chemotherapy. JAMA Surg. 2018, 153, 1120–1126. [Google Scholar] [CrossRef] [Green Version]
- Esgueva, A.; Siso, C.; Espinosa-Bravo, M.; Sobrido, C.; Miranda, I.; Salazar, J.P.; Rubio, I.T. Leveraging the increased rates of pathologic complete response after neoadjuvant treatment in breast cancer to de-escalate surgical treatments. J. Surg. Oncol. 2021, 123, 71–79. [Google Scholar] [CrossRef]
- Koolen, B.B.; Donker, M.; Straver, M.E.; van der Noordaa, M.E.M.; Rutgers, E.J.T.; Olmos, R.A.V.; Peeters, M.V. Combined PET-CT and axillary lymph node marking with radioactive iodine seeds (MARI procedure) for tailored axillary treatment in node-positive breast cancer after neoadjuvant therapy. Br. J. Surg. 2017, 104, 1188–1196. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, S.; Stachs, A.; Kühn, T.; Winckelmann, A.; de Boniface, J.; Gerber, B.; Reimer, T. Abstract OT3-01-01: Feasibility of carbon tattooing for targeted lymph node biopsy in breast cancer patients treated by primary systemic therapy (TATTOO trial). Cancer Res. 2019, 80, OT3-01. [Google Scholar] [CrossRef]
- Henke, G.; Knauer, M.; Ribi, K.; Hayoz, S.; Gerard, M.A.; Ruhstaller, T.; Zwahlen, D.R.; Muenst, S.; Ackerknecht, M.; Hawle, H.; et al. Tailored axillary surgery with or without axillary lymph node dissection followed by radiotherapy in patients with clinically node-positive breast cancer (TAXIS): Study protocol for a multicenter, randomized phase-III trial. Trials 2018, 19, 667. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Type of Surgery | Description |
|---|---|
| Axillary lymph node dissection (ALND) | Systematic removal of lymph nodes from the axilla, usually level I and II, sometimes including also level III |
| Sentinel lymph node biopsy (SLNB) | Identification and removal of the sentinel lymph node, usually using radioactive tracer (Technetium-99) or blue dye |
| Targeted lymph node biopsy (TLNB) | Selective removal of metastatic lymph node(s) marked before neoadjuvant therapy |
| Targeted axillary dissection (TAD) | Combination of TLNB and SLNB |
| National/International: | Staging Recommendation for cN+ → ycN0 Patients | Level of Evidence/Grade of Recommendation |
|---|---|---|
| European Society for Medical Oncology (ESMO) [10] | Sentinel lymph node biopsy (SLNB) can be an option, as long as additional recommendations are followed (e.g., dual tracer, clipping/marking of positive nodes, minimum of three sentinel nodes removed) | III, B |
| National Comprehensive Cancer Network (NCCN) [9] | Consider SLNB. Relatively high false-negative rate (FNR) (>10%) can be improved by marking biopsied lymph nodes to document their removal, using dual tracer, and by removing more than 2 sentinel nodes | 2B |
| American Society of Breast Surgeons [13] | If SLNB after neoadjuvant therapy is attempted, dual tracer should be used. If a SLN and/or the clipped node (if clipped) is not identified, an Axillary lymph node dissection (ALND) is recommended | Not provided |
| Finland [14] | ALND | Not provided |
| Germany (S3 guideline) [15] | ALND | 2b, B |
| Germany (AGO Breast Committee) [11] | Targeted axillary dissection (TAD): + (i.e., this investigation or therapeutic intervention is of limited benefit for patients and can be performed) ALND: + (i.e., this investigation or therapeutic intervention is of limited benefit for patients and can be performed) SLNB only: +/− (i.e., this investigation or therapeutic intervention has not shown benefit for patients and may be performed only in individual cases. According to current knowledge a general recommendation cannot be given) | 2b, B |
| Hungary [16] | SLNB, preferably with double tracer technique (isotope + dye), and with at least 3 SLNs removed; in case of limited axillary tumor load and a realistic chance of cN1 → ycN0 conversion, clipping the metastatic node before neoadjuvant chemotherapy (NACT) is recommended | Not provided |
| India [17] | No specific recommendation for cN+ ycN0 patients | Not provided |
| Poland [18] | SLNB can be an option with some limitations:
| Power of recommendation in square brackets (score −2, −1, 0, 1+, 2+) |
| Romania | Last approved national guideline (2009) [19]: ALND is recommended, SLNB is not recommended after NACT New version proposed by the Romanian Society of Obstetrics and Gynecology (2019; not approved by the Ministry of Health) [20]: Suspicious lymph nodes must be biopsied, and clipped if possible; if SLNB after NACT is attempted, dual tracer is recommended | Not provided |
| Sweden [21] | ALND | Grade +++ Recommendation: B |
| Society Guidelines | ||
| Denmark (Danish Breast Cancer Cooperative Group) [22] | TAD including double tracer technique (radioactive tracer plus dye) Target lymph node(s) to be marked with radioactive iodine seeds or coils | Not provided |
| Italy (Assoziacione Italiana de Oncologica Medica = AIOM) [23] | SLNB; ALND omission may be considered in the case one or more negative sentinel lymph nodes, identified with double tracer and only in patients who were cN1/2 at time of diagnosis | Quality of evidence: Low Strength of Recommendation: Weak |
| Portugal (Portuguese Society of Senology) [24] | cN1 patients should be clipped and ycN0 patients should be managed by TAD, with omission of ALND in ypN0 if the following criteria are fulfilled: (1) SLNB performed using dual traced, (2) clipped node removed, and (3) more than 2 removed nodes | Not provided |
| Russia (Association of Oncologists of Russia) [25] | It is recommended to mark the tumor before starting neoadjuvant therapy to enable visualization during subsequent surgical treatment. If it is impossible to perform SLNB or if a metastatic focus in the SLN is detected, it is recommended to perform ALND. | III, B I, A |
| Spain (Spanish Society of Medical Oncology) [26] | ALND is recommended. In selected cN+ cases, in which positive axillary node has been marked prior to NACT, the identification and recovery of >2 negative SLNs (including the marked node) with a double tracer technique (Tc99 and methylene blue) may avoid ALND. | I, A II, C |
| Study | Number of Patients | Preoperative Axillary Assessment | Detection Rate of the Sentinel Node | False Negative Rate |
|---|---|---|---|---|
| SENTINA [4] | 592 | Clinical examination, ultrasound | 80.1% | 14.2% |
| SN FNAC [27] | 153 | Clinical examination, ultrasound | 87.6% | 8.4% 1 |
| ACOSOG Z1071 [5] | 649 | Surgical approach independent of clinical response | 92.9% | 12.6% 2 |
| GANEA 2 [1] | 307 | Surgical approach independent of clinical response | 79.8% | 11.9% |
| Meta-analysis [6] | 3398 | - | 91% | 13% |
| Marking | Localization | Advantages | Disadvantages |
|---|---|---|---|
| Clip |
|
|
|
| Radioactive seed | Intraoperative localization using gamma probe |
|
|
| Carbon suspension | Intraoperative visualization |
|
|
| Magnetic seed | Intraoperative localization using magnetic probe |
|
|
| Radar reflector localization (RRL) | Intraoperative localization using radar locator |
|
|
| Radiofrequency identification devices (RFID tags) | Intraoperative localization using radiofrequency localizer |
|
|
| Marking Technique before NACT | Trial | Number of Patients | Localization Technique | Preoperative or Intraoperative Detection Rate of the Marker | Successful TLN Removal | FNR 1 |
|---|---|---|---|---|---|---|
| Clip | SENTA [28,29] | 473 | Preoperative wire localization in most patients | Ultrasound: 89% | 78% | TAD: 4.3% TLNB: 7.2% |
| Caudle 2016 [8] | 208 | Preoperative radioactive seed placement into the clipped area → intraoperative detection using gamma probe | NR | 98% 2 | Clipped node removal: 4.2% 3 Clipped node removal + SLNB: 2.0% SLNB alone: 10.1% | |
| ACOSOG Z1071 [5,7] | 203 | None | NR | 83% 4 | SLNB: 6.8% if TLN was SLN 19% if TLN was not SLN 5 | |
| Plecha 2015 [30] (in 98% HydroMARK clip) | 91 | Wire localization in 74% of patients | NR | 97% in patients with and 83% in patients without wire localization | NR | |
| Laws 2020 [31] | 57 | Preoperative placement of a magnetic seed, a RRL clip or a RFID tag into the clipped area | 98% | 89% | NR | |
| Ngyuen 2017 [32] | 56 | Preoperative radioactive seed placement → intraoperative detection using gamma probe | Ultrasound: 72% | 91% | NR | |
| Simons 2021 [33] | 50 | Preoperative magnetic seed placement → intraoperative detection using magnetic probe | Ultrasound: 100% | 98% | NR | |
| ILINA trial [34] (HydroMARK clip) | 46 | Intraoperative ultrasound | Ultrasound: 96% | NR | TAD: 4.1% 3 | |
| Sun 2020 [35] | 38 | Preoperative RRL clip placement → intraoperative detection using radar probe | 100% | 100% | NR | |
| Hartmann 2018 [36] (HydroMARK clip) | 30 | Wire localization in 80% of patients (67% US, 13% mammography) | Ultrasound: 83% | 70% in the entire cohort, 83% in patients with wire localization | 0% | |
| Diego 2016 [37] | 30 | Preoperative radioactive seed placement into the clipped area → intraoperative detection using gamma probe | Ultrasound: 93% | 93% | NR | |
| Mariscal Martinez 2021 [38] (HydroMARK 93%, Tumark 3%, UltraCor-Twirl 3%) | 29 | Preoperative magnetic seed placement → intraoperative detection using magnetic probe | 100% | 100% | SLNB alone: 21.4% TAD: 5.9% | |
| Kim 2019 [39] (UltraClip) | 28 | US-guided injection of ink and skin marking | Ultrasound: 79% clearly visible, 21% equivocally visible | 96% | NR | |
| Balasubramanian 2020 [40] (HydroMARK clip) | 25 | Wire localization | NR | 92% | NR | |
| Lim 2020 [41,42] | 14 | Preoperative US-guided skin marking | NR | 84% (UltraCor Twirl: 100% HydroMARK: 78% UltraClip DualTrigger: 50% UltraClip: 0%) | TLNB: 0% if ≥2 marked nodes were removed 7.1% if only first TLN was removed | |
| Radioactive seed | RISAS [43] | 227 | Gamma probe (intraoperative) | NR | 98% | TAD: 3.5% |
| Donker 2015 [44] | 100 | Gamma probe (intraoperative) | 100% (gamma probe) | 97% | TLNB: 7% 3 | |
| Magnetic seed | Thill 2020 [45] | 5 | Magnetic probe (intraoperative) | 100% | 100% | NR |
| Radar reflector localization-clip | Sun 2020 [35] | 7 | Intraoperative radar localization | 100% | 100% | NR |
| RFID tag | Malter 2020 [46] | 10 | Radiofrequency probe (intraoperative) | 100% | 100% | NR |
| Carbon suspension | Hartmann 2020 [47] | 118 | Intraoperative visualization | 94% | 94% | TAD: 9.1% |
| Natsiopoulos 2019 [48] | 75 | Intraoperative visualization | 100% | 100% | NR | |
| Allweis [49] | 63 | Intraoperative visualization | 95% | 95% | NR | |
| Khallaf 2020 [50] | 20 | Intraoperative visualization | 95% | 95% | TAD: 8.3% SLNB alone: 15.3% | |
| Gatek 2020 [51] | 20 | Intraoperative visualization | 100% | 100% | NR | |
| Choy 2014 [52] | 12 | Intraoperative visualization | 100% | 100% | NR |
| Only One Node Is Marked | All Suspicious Nodes Are Marked | |
|---|---|---|
| Advantages |
|
|
| Disadvantages |
|
|
| At Time of Biopsy | After Pathological/Cytological Confirmation of Nodal Metastasis | |
|---|---|---|
| Advantages |
|
|
| Disadvantages |
|
|
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Study | Status | Study Design | Primary Endpoint(s) |
|---|---|---|---|
| ATNEC NCT04109079 | Not yet recruiting | Randomized trial cN+ → ypN0 patients Surgery: TAD Marking technique: clip or carbon suspension Arms: axillary treatment (ALND or ART) vs. no axillary treatment | DFS Patient-reported lymphedema |
| AXSANA NCT04373655 | Recruiting since June 2020 | Non-interventional cohort study cN+ patients | iDFS Axillary recurrence rate Quality of life and arm morbidity |
| GANEA 3 NCT03630913 | Recruiting since January 2019 | Single-arm trial cN+ patients (confirmed by biopsy) Surgery: TAD followed by ALND Marking technique: clip, marking of the most suspicious node only | False-negative rate of SLNB, TLNB, and TAD |
| MAGELLAN NCT03796559 | Recruiting | Single-arm trial cN+ patients (confirmed by biopsy) Surgery: TAD Marking technique: clip and magnetic seed | Retrieval rate of clipped node and magnetic seed |
| Pre-ATNEC NCT03640819 | Completed, results pending | Single-arm trial cN+ patients (confirmed by biopsy) Surgery: TLNB and—at surgeon’s discretion—SLNB or ALND Marking technique: carbon suspension | Identification rate of marked lymph node(s) |
| RISAS NCT02800317 | Completed, full publication pending [43,53] | Single-arm trial cN+ patients (confirmed by biopsy) Surgery: TAD followed by ALND Marking technique: Radioactive iodine seed | Identification rate, accuracy, and false negative rate |
| TATTOO DRKS00013169 | Completed, full results pending [47,66] | Single-arm trial cN+ patients (confirmed by biopsy) Surgery: TAD or TLNB + ALND Marking technique: carbon suspension | Detection rate of the TLN |
| TAXIS [67] NCT03513614 | Recruiting | Randomized phase III trial cN+ patients Surgery: tailored axillary surgery with or without ALND followed by radiotherapy | DFS |
| NCT03718455 | Terminated due to limited operating room availability | Single-arm trial cN+ patients (confirmed by biopsy) Marking technique: Magnetic seed | Detection rate of the TLN |
| NCT03411070 | Recruiting | Single-arm trial cN+ patients Surgery: Marking technique: radar reflector-localization clip | Rate of successful removal of the TLN |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banys-Paluchowski, M.; Gasparri, M.L.; de Boniface, J.; Gentilini, O.; Stickeler, E.; Hartmann, S.; Thill, M.; Rubio, I.T.; Di Micco, R.; Bonci, E.-A.; et al. Surgical Management of the Axilla in Clinically Node-Positive Breast Cancer Patients Converting to Clinical Node Negativity through Neoadjuvant Chemotherapy: Current Status, Knowledge Gaps, and Rationale for the EUBREAST-03 AXSANA Study. Cancers 2021, 13, 1565. https://doi.org/10.3390/cancers13071565
Banys-Paluchowski M, Gasparri ML, de Boniface J, Gentilini O, Stickeler E, Hartmann S, Thill M, Rubio IT, Di Micco R, Bonci E-A, et al. Surgical Management of the Axilla in Clinically Node-Positive Breast Cancer Patients Converting to Clinical Node Negativity through Neoadjuvant Chemotherapy: Current Status, Knowledge Gaps, and Rationale for the EUBREAST-03 AXSANA Study. Cancers. 2021; 13(7):1565. https://doi.org/10.3390/cancers13071565
Chicago/Turabian StyleBanys-Paluchowski, Maggie, Maria Luisa Gasparri, Jana de Boniface, Oreste Gentilini, Elmar Stickeler, Steffi Hartmann, Marc Thill, Isabel T. Rubio, Rosa Di Micco, Eduard-Alexandru Bonci, and et al. 2021. "Surgical Management of the Axilla in Clinically Node-Positive Breast Cancer Patients Converting to Clinical Node Negativity through Neoadjuvant Chemotherapy: Current Status, Knowledge Gaps, and Rationale for the EUBREAST-03 AXSANA Study" Cancers 13, no. 7: 1565. https://doi.org/10.3390/cancers13071565