
Low MicroRNA-19b Expression Shows a Promising Clinical Impact in Locally Advanced Rectal Cancer

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Experimental Section
2.1. Patients Tissue Samples
2.2. Evaluation of Pathological Response
2.3. RNA Isolation
2.4. Quantification of miRNA Expression Levels
2.5. Statistical Analysis
3. Results
3.1. Low miR-19b Expression Is a Common Alteration in LARC Patients that Associates with Molecular and Clinical PARAMETERS
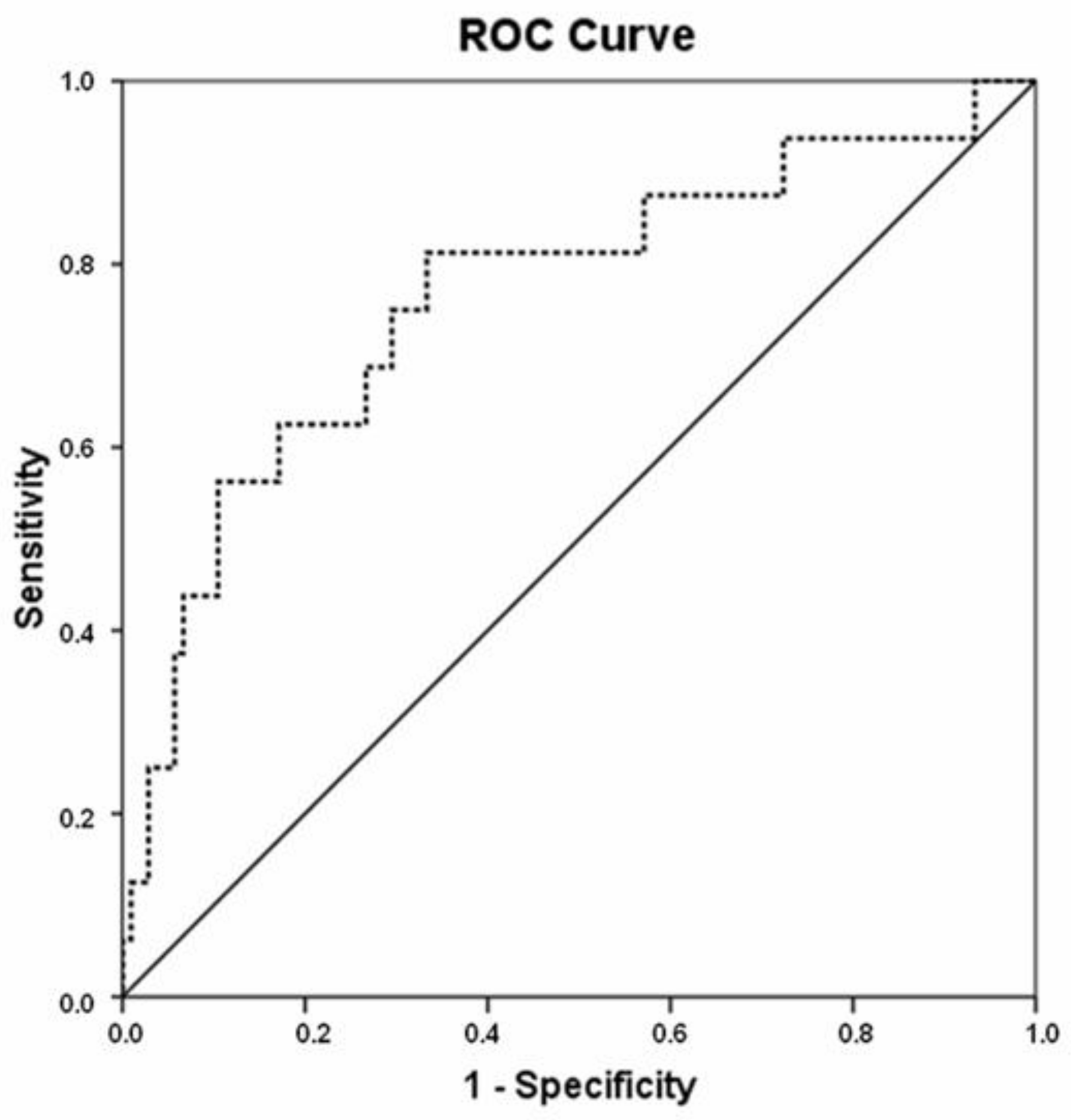
3.2. MiR-19b Is a Predictor of Pathological Response to Neoadjuvant CRT in Locally Advanced Rectal Cancer
3.3. MiR-19b Expression Determines Outcome in Locally Advanced Rectal Cancer Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spanish Society of Medical Oncology. Cancer Data in Spain. Available online: https://seom.org/dmcancer/wp-content/uploads/2019/Informe-SEOM-cifras-cancer-2019.pdf (accessed on 8 January 2021).
- Feeney, G.; Sehgal, R.; Sheehan, M.; Hogan, A.; Regan, M.; Joyce, M.; Kerin, M. Neoadjuvant radiotherapy for rectal cancer management. World J. Gastroenterol. 2019, 25, 4850–4869. [Google Scholar] [CrossRef] [PubMed]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology. Available online: https://www.nccn.org/professionals/physician_gls (accessed on 8 January 2021).
- van Gijn, W.; Marijnen, C.A.; Nagtegaal, I.D.; Kranenbarg, E.M.-K.; Putter, H.; Wiggers, T.; Rutten, H.J.; Påhlman, L.; Glimelius, B.; van de Velde, C.J. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011, 12, 575–582. [Google Scholar] [CrossRef]
- Yeo, S.-G.; Kim, D.Y.; Kim, T.H.; Chang, H.J.; Oh, J.H.; Park, W.; Choi, D.H.; Nam, H.; Kim, J.; Cho, M.; et al. Pathologic Complete Response of Primary Tumor Following Preoperative Chemoradiotherapy for Locally Advanced Rectal Cancer: Long-term Outcomes and Prognostic Significance of Pathologic Nodal Status (KROG 09-01). Ann. Surg. 2010, 252, 998–1004. [Google Scholar] [CrossRef]
- Fokas, E.; Fietkau, R.; Hartmann, A.; Hohenberger, W.; Grützmann, R.; Ghadimi, M.; Liersch, T.; Ströbel, P.; Grabenbauer, G.; Graeven, U.; et al. Neoadjuvant rectal score as individual-level surrogate for disease-free survival in rectal cancer in the CAO/ARO/AIO-04 randomized phase III trial. Ann. Oncol. 2018, 29, 1521–1527. [Google Scholar] [CrossRef] [PubMed]
- Guillem, J.G.; Chessin, D.B.; Cohen, A.M.; Shia, J.; Mazumdar, M.; Enker, W.; Paty, P.B.; Weiser, M.R.; Klimstra, D.; Saltz, L.; et al. Long-term Oncologic Outcome Following Preoperative Combined Modality Therapy and Total Mesorectal Excision of Locally Advanced Rectal Cancer. Ann. Surg. 2005, 241, 829–838. [Google Scholar] [CrossRef]
- Benzoni, E.; Intersimone, D.; Terrosu, G.; Bresadola, V.; Cojutti, A.; Cerato, F.; Avellini, C. Prognostic value of tumour regression grading and depth of neoplastic infiltration within the perirectal fat after combined neoadjuvant chemo-radiotherapy and surgery for rectal cancer. J. Clin. Pathol. 2006, 59, 505–512. [Google Scholar] [CrossRef] [Green Version]
- Bottarelli, L.; de Angelis, G.L.; Azzoni, C.; Di Mario, F.; de Angelis, N.; Leandro, G.; Fornaroli, F.; Gaiani, F.; Negri, F. Potential predictive biomarkers in locally advanced rectal cancer treated with preoperative chemo-radiotherapy. Acta Biomed. 2018, 89, 102–106. [Google Scholar]
- Imedio, L.; Cristóbal, I.; Rubio, J.; Santos, A.; Rojo, F.; García-Foncillas, J. MicroRNAs in Rectal Cancer: Functional Significance and Promising Therapeutic Value. Cancers 2020, 12, 2040. [Google Scholar] [CrossRef]
- De Palma, F.D.E.; Luglio, G.; Tropeano, F.P.; Pagano, G.; D’Armiento, M.; Kroemer, G.; Maiuri, M.C.; De Palma, G.D. The Role of Micro-RNAs and Circulating Tumor Markers as Predictors of Response to Neoadjuvant Therapy in Locally Advanced Rectal Cancer. Int. J. Mol. Sci. 2020, 21, 7040. [Google Scholar] [CrossRef]
- Zhang, B.; Pan, X.; Cobb, G.P.; Anderson, T.A. microRNAs as oncogenes and tumor suppressors. Dev. Biol. 2007, 302, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Xi, Y.; Formentini, A.; Chien, M.; Weir, D.B.; Russo, J.J.; Ju, J.; Kornmann, M.; Ju, J. Prognostic Values of microRNAs in Colorectal Cancer. Biomark. Insights 2006, 1, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Mosakhani, N.; Sarhadi, V.K.; Borze, I.; Karjalainen-Lindsberg, M.-L.; Sundström, J.; Ristamäki, R.; Osterlund, P.; Knuutila, S. MicroRNA profiling differentiates colorectal cancer according to KRAS status. Genes Chromosom Cancer 2012, 51, 1–9. [Google Scholar] [CrossRef]
- Wang, H.; Peng, R.; Wang, J.; Qin, Z.; Xue, L. Circulating microRNAs as potential cancer biomarkers: The advantage and disadvantage. Clin. Epigenetics 2018, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Machackova, T.; Prochazka, V.; Kala, Z.; Slaby, O. Translational Potential of MicroRNAs for Preoperative Staging and Prediction of Chemoradiotherapy Response in Rectal Cancer. Cancers 2019, 11, 1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caramés, C.; Cristóbal, I.; Moreno, V.; Del Puerto, L.; Moreno, I.; Rodriguez, M.; Marín, J.P.; Correa, A.V.; Hernández, R.; Zenzola, V.; et al. MicroRNA-21 predicts response to preoperative chemoradiotherapy in locally advanced rectal cancer. Int. J. Color. Dis. 2015, 30, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Caramés, C.; Cristobal, I.; Moreno, V.; Marín, J.P.; González-Alonso, P.; Torrejón, B.; Minguez, P.; Leon, A.; Martín, J.I.; Hernández, R.; et al. MicroRNA-31 Emerges as a Predictive Biomarker of Pathological Response and Outcome in Locally Advanced Rectal Cancer. Int. J. Mol. Sci. 2016, 17, 878. [Google Scholar] [CrossRef]
- Zhu, Y.; Peng, Q.; Lin, Y.; Zou, L.; Shen, P.; Chen, F.; Min, M.; Shen, L.; Chen, J.; Shen, B. Identification of biomarker microRNAs for predicting the response of colorectal cancer to neoadjuvant chemoradiotherapy based on microRNA regulatory network. Oncotarget 2016, 8, 2233–2248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristóbal, I.; Rubio, J.; Santos, A.; Torrejón, B.; Caramés, C.; Imedio, L.; Mariblanca, S.; Luque, M.; Sanz-Alvarez, M.; Zazo, S.; et al. MicroRNA-199b Downregulation Confers Resistance to 5-Fluorouracil Treatment and Predicts Poor Outcome and Response to Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer Patients. Cancers 2020, 12, 1655. [Google Scholar] [CrossRef]
- Fan, Y.; Yin, S.; Hao, Y.; Yang, J.; Zhang, H.; Sun, C.; Ma, M.; Chang, Q.; Xi, J.J. miR-19b promotes tumor growth and metastasis via targeting TP53. Struct. 30s Ribosomal Decod. Complex. At. Ambient Temp. 2014, 20, 765–772. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.-L.; Yang, H.-J.; Liu, B.; Liu, T. Effects of MicroRNA-19b on the Proliferation, Apoptosis, and Migration of Wilms’ Tumor Cells Via the PTEN/PI3K/AKT Signaling Pathway. J. Cell. Biochem. 2017, 118, 3424–3434. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Su, Z.; Gu, W.; Shen, X.; Zhao, Q.; Shi, L.; Jin, C.; Wang, X.; Cong, H.; Ju, S. MiR-19b and miR-20a suppress apoptosis, promote proliferation and induce tumorigenicity of multiple myeloma cells by targeting PTEN. Cancer Biomark. 2019, 24, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Liang, X.; Yu, W.; Zhou, S.; Fang, M. Differential Expression of MicroRNA-19b Promotes Proliferation of Cancer Stem Cells by Regulating the TSC1/mTOR Signaling Pathway in Multiple Myeloma. Cell. Physiol. Biochem. 2018, 50, 1804–1814. [Google Scholar] [CrossRef]
- Baumgärtner, U.; Berger, F.; Gheinani, A.H.; Burgener, S.S.; Monastyrskaya, K.; Vassella, E. miR-19b enhances proliferation and apoptosis resistance via the EGFR signaling pathway by targeting PP2A and BIM in non-small cell lung cancer. Mol. Cancer 2018, 17, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, K.N.; Nielsen, B.S.; Lindebjerg, J.; Hansen, T.F.; Holst, R.; Sørensen, F.B. microRNA-17 Is the Most Up-Regulated Member of the miR-17-92 Cluster during Early Colon Cancer Evolution. PLoS ONE 2015, 10, e0140503. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, K.J.; Cobiac, L.; Le Leu, R.K.; Van Der Hoek, M.B.; Michael, M.Z. Histone deacetylase inhibition in colorectal cancer cells reveals competing roles for members of the oncogenic miR-17-92 cluster. Mol. Carcinog. 2012, 52, 459–474. [Google Scholar] [CrossRef]
- Jiang, T.; Ye, L.; Han, Z.; Liu, Y.; Yang, Y.; Peng, Z.; Fan, J. miR-19b-3p promotes colon cancer proliferation and oxaliplatin-based chemoresistance by targeting SMAD4: Validation by bioinformatics and experimental analyses. J. Exp. Clin. Cancer Res. 2017, 36, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wang, Z.; Han, X.; Jiang, L.; Ge, R.; Wang, X.; Li, J. Up-regulation of microRNA-19b is associated with metastasis and predicts poor prognosis in patients with colorectal cancer. Int. J. Clin. Exp. Pathol. 2018, 11, 3952–3960. [Google Scholar]
- Guo, Y.; Ye, Q.; Deng, P.; Cao, Y.; He, D.; Zhou, Z.; Wang, C.; Zaytseva, Y.Y.; Schwartz, C.E.; Lee, E.Y.; et al. Spermine synthase and MYC cooperate to maintain colorectal cancer cell survival by repressing Bim expression. Nat. Commun. 2020, 11, 1–16. [Google Scholar] [CrossRef]
- Gu, Y.Y.; Yu, J.; Zhang, J.F.; Wang, C. Suppressing the secretion of exosomal miR-19b by gw4869 could regulate oxaliplatin sensitivity in colorectal cancer. Neoplasma 2019, 66, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Kurokawa, K.; Tanahashi, T.; Iima, T.; Yamamoto, Y.; Akaike, Y.; Nishida, K.; Masuda, K.; Kuwano, Y.; Murakami, Y.; Fukushima, M.; et al. Role of miR-19b and its target mRNAs in 5-fluorouracil resistance in colon cancer cells. J. Gastroenterol. 2012, 47, 883–895. [Google Scholar] [CrossRef] [PubMed]
- Zekri, A.-R.N.; Youssef, A.S.E.-D.; Lotfy, M.M.; Gabr, R.; Ahmed, O.S.; Nassar, A.; Hussein, N.; Omran, D.; Medhat, E.; Eid, S.; et al. Circulating Serum miRNAs as Diagnostic Markers for Colorectal Cancer. PLoS ONE 2016, 11, e0154130. [Google Scholar] [CrossRef] [PubMed]
- Marcuello, M.; Duran-Sanchon, S.; Moreno, L.; Lozano, J.J.; Bujanda, L.; Castells, A.; Gironella, M. Analysis of A 6-Mirna Signature in Serum from Colorectal Cancer Screening Participants as Non-Invasive Biomarkers for Advanced Adenoma and Colorectal Cancer Detection. Cancers 2019, 11, 1542. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Gil, S.; Sanchez-Martinez, R.; de Cedron, M.G.; Martin-Hernandez, R.; Vargas, T.; Molina, S.; Herranz, J.; Davalos, A.; Reglero, G.; de Molina, A.R. Targeting the lipid metabolic axis ACSL/SCD in colorectal cancer progression by therapeutic miRNAs: miR-19b-1 role. J. Lipid Res. 2018, 59, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Kahlert, C.; Klupp, F.; Brand, K.; Lasitschka, F.; Diederichs, S.; Kirchberg, J.; Rahbari, N.; Dutta, S.; Bork, U.; Fritzmann, J.; et al. Invasion front-specific expression and prognostic significance of microRNA in colorectal liver metastases. Cancer Sci. 2011, 102, 1799–1807. [Google Scholar] [CrossRef]
- Salvi, S.; Molinari, C.; Foca, F.; Teodorani, N.; Saragoni, L.; Puccetti, M.; Passardi, A.; Tamberi, S.; Avanzolini, A.; Lucci, E.; et al. miR-17-92a-1 cluster host gene (MIR17HG) evaluation and response to neoadjuvant chemoradiotherapy in rectal cancer. Oncotargets 2016, 9, 2735–2742. [Google Scholar] [CrossRef] [Green Version]
- Greenson, J.K.; Huang, S.-C.; Herron, C.; Moreno, V.; Bonner, J.D.; Tomsho, L.P.; Ben-Izhak, O.; Cohen, H.I.; Trougouboff, P.; Bejhar, J.; et al. Pathologic Predictors of Microsatellite Instability in Colorectal Cancer. Am. J. Surg. Pathol. 2009, 33, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real- time quantitative PCR and the 2(-Delta Delta C(T)). Method 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Sauerbrei, W.; Taube, S.E.; McShane, L.M.; Cavenagh, M.M.; Altman, D.G. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): An Abridged Explanation and Elaboration. J. Natl. Cancer Inst. 2018, 110, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Cristóbal, I.; Manso, R.; Rincón, R.; Caramés, C.; Senin, C.; Borrero, A.; Martínez-Useros, J.; Rodriguez, M.; Zazo, S.; Aguilera, O.; et al. PP2A Inhibition Is a Common Event in Colorectal Cancer and Its Restoration Using FTY720 Shows Promising Therapeutic Potential. Mol. Cancer 2014, 13, 938–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristóbal, I.; Rincón, R.; Manso, R.; Madoz-Gúrpide, J.; Caramés, C.; del Puerto-Nevado, L.; Rojo, F.; García-Foncillas, J. Hyperphosphorylation of PP2A in colorectal cancer and the potential therapeutic value showed by its forskolin-induced dephosphorylation and activation. Biochim. Biophys. Acta 2014, 1842, 1823–1829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCright, B.; Brothman, A.R.; Virshup, D.M. Assignment of human protein phosphatase 2A regulatory subunit genes b56alpha, b56beta, b56gamma, b56delta, and b56epsilon (PPP2R5A-PPP2R5E), highly expressed in muscle and brain, to chromosome regions 1q41, 11q12, 3p21, 6p21.1, and 7p11.2 --> p12. Genomics 1996, 36, 168–170. [Google Scholar] [CrossRef]
- Theendakara, V.; Bredesen, D.E.; Rao, R.V. Downregulation of protein phosphatase 2A by apolipoprotein E: Implications for Alzheimer’s disease. Mol. Cell Neurosci. 2017, 83, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Morita, K.; He, S.; Nowak, R.P.; Wang, J.; Zimmerman, M.W.; Fu, C.; Durbin, A.D.; Martel, M.W.; Prutsch, N.; Gray, N.S.; et al. Allosteric Activators of Protein Phosphatase 2A Display Broad Antitumor Activity Mediated by Dephosphorylation of MYBL2. Cell 2020, 181, 702–715.e20. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No. Cases | No. miR-19b Low (%) | No. miR-19b High (%) | p | |||
|---|---|---|---|---|---|---|
| MiR-19b | 121 | 47 (38.8) | 74 (61.2) | |||
| Gender | 121 | 47 | 74 | 0.605 | ||
| Male | 73 | 27 | (37) | 46 | (63) | |
| Female | 48 | 20 | (41.7) | 28 | (58.3) | |
| Age | 121 | 47 | 74 | 0.562 | ||
| <60 | 40 | 17 | (42.5) | 23 | (57.5) | |
| ≥60 | 81 | 30 | (37) | 51 | (63) | |
| ECOG 1 | 121 | 47 | 74 | 0.831 | ||
| 0 | 81 | 32 | (39.5) | 49 | (60.5) | |
| 1–2 | 40 | 15 | (37.5) | 25 | (62.5) | |
| Clinical stage pre-CRT 2 | 121 | 47 | 74 | 0.285 | ||
| II | 9 | 5 | (55.6) | 4 | (44.4) | |
| III | 112 | 42 | (37.5) | 70 | (62.5) | |
| Grade pre-CRT | 112 | 42 | 70 | 0.103 | ||
| Low | 40 | 19 | (47.5) | 21 | (52.5) | |
| Moderate-High | 72 | 23 | (31.9) | 49 | (68.1) | |
| ypT 3 | 121 | 47 | 74 | 0.003 | ||
| 0 | 16 | 13 | (81.3) | 3 | (18.7) | |
| 1 | 16 | 7 | (43.8) | 9 | (56.2) | |
| 2 | 38 | 12 | (31.6) | 26 | (68.4) | |
| 3 | 44 | 13 | (29.6) | 31 | (70.4) | |
| 4 | 4 | 0 | (0) | 4 | (100) | |
| x | 3 | 2 | (66.7) | 1 | (33.3) | |
| ypN 4 | 121 | 47 | 74 | 0.216 | ||
| N0 | 91 | 38 | (41.8) | 53 | (58.2) | |
| N1 | 26 | 9 | (34.6) | 17 | (65.4) | |
| N2 | 4 | 0 | (0) | 4 | (100) | |
| Pathological stage | 121 | 47 | 74 | 0.003 | ||
| yp0 | 16 | 13 | (81.3) | 3 | (18.7) | |
| ypI | 43 | 15 | (34.9) | 28 | (65.1) | |
| ypII | 32 | 10 | (31.3) | 22 | (68.7) | |
| ypIII | 30 | 9 | (30) | 21 | (70) | |
| Response to NCRT 1 | No. Cases | Responders 2 (%) | Non-Responders 3 (%) | p | ||
|---|---|---|---|---|---|---|
| MiR-19b Expression | 121 | 58 | 63 | <0.001 | ||
| Low | 47 | 24 | (72.3) | 13 | (27.7) | |
| High | 74 | 34 | (32.4) | 50 | (67.6) | |
| Recurrence | No. Cases | Yes (%) | No (%) | p | ||
|---|---|---|---|---|---|---|
| MiR-19b Expression | 121 | 26 | 95 | 0.001 | ||
| Low | 47 | 3 | (6.4) | 44 | (93.6) | |
| High | 74 | 23 | (31.1) | 51 | (68.9) | |
| Response 1 vs. Non-Response 2 | ||
|---|---|---|
| OR 3 (95% CI 4) | p | |
| Gender, Male vs. Female | 1.227 (0.558 to 2.98) | 0.611 |
| Age, < 60 vs. ≥60 | 0.778 (0.714 to 1.925) | 0.587 |
| Clinical stage pre-CRT 5, II vs. III | 1.210 (0.709 to 2.064) | 0.485 |
| Grade pre CRT, Low vs. Moderate/High | 1.021 (0.492 to 2.119) | 0.956 |
| ECOG 6, 0 vs. 1–2 | 1.174 (0.484 to 2.850) | 0.722 |
| miR-19b, High vs. Low | 0.166 (0.071 to 0.390) | <0.001 |
| Univariate OS 1 Analysis | Multivariate OS Cox Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| HR 3 | 95% CI 2 | p | HR | 95% CI | p | ||||
| Lower | Upper | Lower | Upper | ||||||
| Gender | 0.816 | - | |||||||
| Male | 1.000 | ||||||||
| Female | 0.888 | 0.326 to 2.418 | - | - | |||||
| Age | 0.225 | - | |||||||
| <60 | 1.000 | ||||||||
| ≥60 | 2.167 | 0.621 to 7.564 | - | - | |||||
| Pathological stage | 0.030 | 0.490 | |||||||
| 0-I | 1.000 | 1.000 | |||||||
| II-III | 3.484 | 1.131 to 10.732 | 1.635 | 0.405 to 6.607 | |||||
| ypT 4 | 0.139 | - | |||||||
| 0–2 | 1.000 | ||||||||
| 3–4 | 2.120 | 0.783 to 5.741 | - | - | |||||
| ypN 5 | 0.007 | 0.105 | |||||||
| N- | 1.000 | 1.000 | |||||||
| N+ | 3.747 | 1.443 to 9.729 | 2.658 | 0.814 to 8.677 | |||||
| ECOG 6 | 0.454 | - | |||||||
| 0 | 1.000 | ||||||||
| 1–2 | 1.450 | 0.548 to 3.836 | - | - | |||||
| MiR-19b | 0.018 | 0.024 | |||||||
| High | 1.000 | 1.000 | |||||||
| Low | 0.085 | 0.011 to 0.656 | 0.093 | 0.012 to 0.727 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rubio, J.; Cristóbal, I.; Santos, A.; Caramés, C.; Luque, M.; Sanz-Alvarez, M.; Zazo, S.; Madoz-Gúrpide, J.; Rojo, F.; García-Foncillas, J. Low MicroRNA-19b Expression Shows a Promising Clinical Impact in Locally Advanced Rectal Cancer. Cancers 2021, 13, 1456. https://doi.org/10.3390/cancers13061456
Rubio J, Cristóbal I, Santos A, Caramés C, Luque M, Sanz-Alvarez M, Zazo S, Madoz-Gúrpide J, Rojo F, García-Foncillas J. Low MicroRNA-19b Expression Shows a Promising Clinical Impact in Locally Advanced Rectal Cancer. Cancers. 2021; 13(6):1456. https://doi.org/10.3390/cancers13061456
Chicago/Turabian StyleRubio, Jaime, Ion Cristóbal, Andrea Santos, Cristina Caramés, Melani Luque, Marta Sanz-Alvarez, Sandra Zazo, Juan Madoz-Gúrpide, Federico Rojo, and Jesús García-Foncillas. 2021. "Low MicroRNA-19b Expression Shows a Promising Clinical Impact in Locally Advanced Rectal Cancer" Cancers 13, no. 6: 1456. https://doi.org/10.3390/cancers13061456