
Maternal and Neonatal Outcome after the Use of G-CSF for Cancer Treatment during Pregnancy

 , , , , , ,
, , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
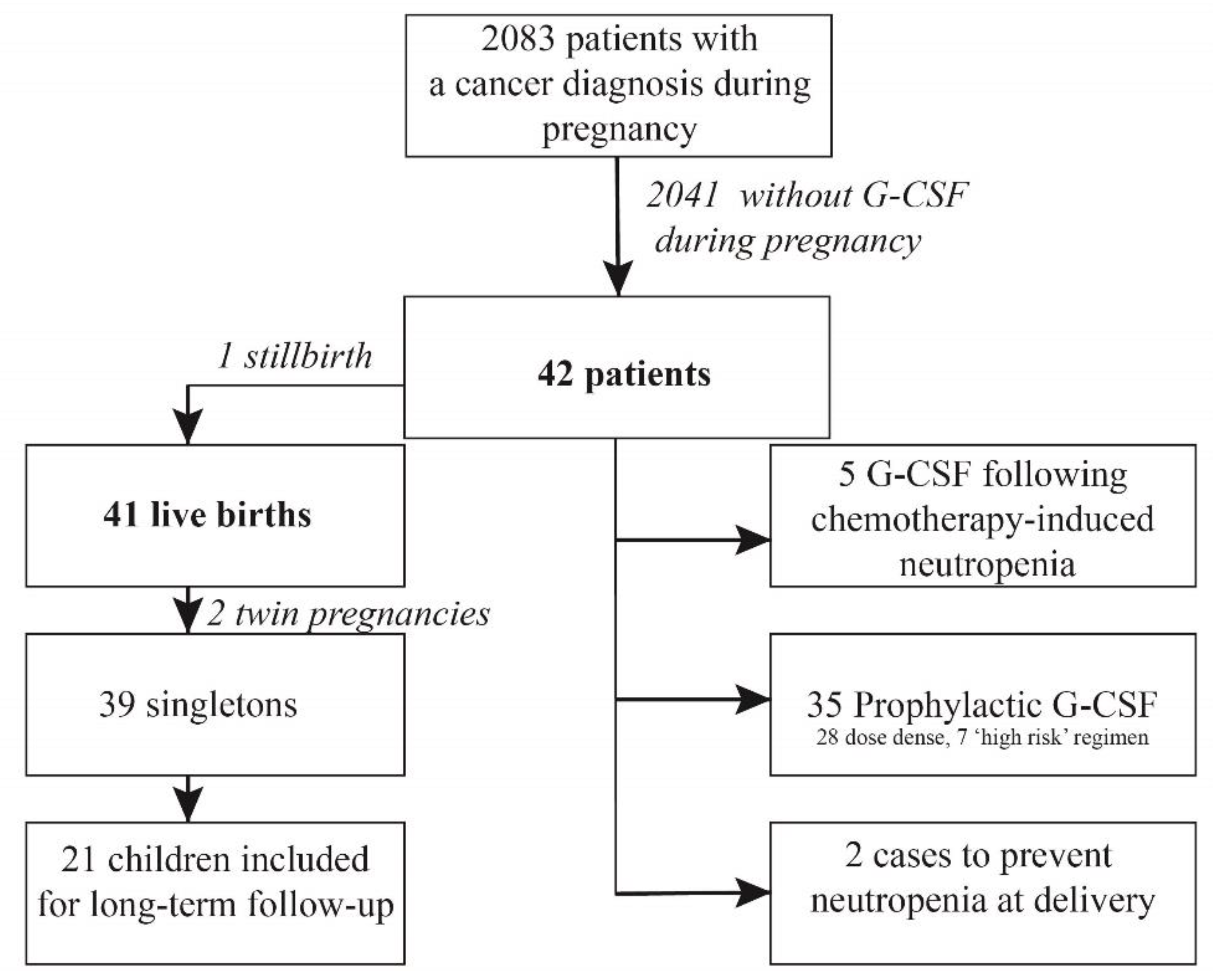
3.1. Treatment
- -
- Long-acting G-CSF was mostly given as part of a dose dense schedule (n = 28; 67%).
- -
- Five patients (12%) developed grade 3–4 neutropenia (including one patient with neutropenic fever) after one to three cycles of 3-weekly chemotherapy (without G-CSF). Two of them received filgastrim during the acute episode of neutropenia and all five patients had long-acting G-CSF with the subsequent chemotherapy (without treatment delay) administrations in prevention of febrile neutropenia or dose delays.
- -
- Seven women (7%) received long-acting G-CSF following ‘high risk’ polychemotherapy for Non Hodgkin lymphoma (n = 4), Ewing sarcoma (n = 1) or ALL (n = 1).
- -
- Long-acting G-CSF (pegfilgastrim) was given prophylactically after the last chemotherapy before delivery in two women (5%).
3.2. Maternal Blood Results
3.3. Obstetric Outcome
3.4. Neonatal Outcome
3.5. Pediatric Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Smith, L.H.; Danielsen, B.; Allen, M.E.; Cress, R. Cancer associated with obstetric delivery: Results of linkage with the California cancer registry. Am. J. Obstet. Gynecol. 2003, 189, 1128–1135. [Google Scholar] [CrossRef]
- Amant, F.; Verheecke, M.; Wlodarska, I.; Dehaspe, L.; Brady, P.; Brison, N.; Van Den Bogaert, K.; Dierickx, D.; Vandecaveye, V.; Tousseyn, T.; et al. Presymptomatic Identification of Cancers in Pregnant Women During Noninvasive Prenatal Testing. JAMA Oncol. 2015, 1, 814–819. [Google Scholar] [CrossRef] [Green Version]
- Cottreau, C.M.; Dashevsky, I.; Andrade, S.E.; Li, D.K.; Nekhlyudov, L.; Raebel, M.A.; Ritzwoller, D.P.; Partridge, A.H.; Pawloski, P.A.; Toh, S. Pregnancy-Associated Cancer: A U.S. Population-Based Study. J. Women’s Health 2019, 28, 250–257. [Google Scholar] [CrossRef]
- de Haan, J.; Verheecke, M.; Van Calsteren, K.; Van Calster, B.; Shmakov, R.G.; Mhallem Gziri, M.; Halaska, M.J.; Fruscio, R.; Lok, C.A.R.; Boere, I.A.; et al. Oncological management and obstetric and neonatal outcomes for women diagnosed with cancer during pregnancy: A 20-year international cohort study of 1170 patients. Lancet Oncol. 2018, 19, 337–346. [Google Scholar] [CrossRef]
- Loibl, S.; Schmidt, A.; Gentilini, O.; Kaufman, B.; Kuhl, C.; Denkert, C.; von Minckwitz, G.; Parokonnaya, A.; Stensheim, H.; Thomssen, C.; et al. Breast Cancer Diagnosed During Pregnancy: Adapting Recent Advances in Breast Cancer Care for Pregnant Patients. JAMA Oncol. 2015, 1, 1145–1153. [Google Scholar] [CrossRef]
- Gregor, H.; Egarter, C.; Levin, D.; Sternberger, B.; Heinze, G.; Leitich, H.; Reisenberger, K. The Passage of Granulocyte-Macrophage Colony-Stimulating Factor Across the Human Placenta Perfused In Vitro. J. Soc. Gynecol. Investig. 1999, 6, 307–310. [Google Scholar] [CrossRef]
- Calhoun, D.A.; Rosa, C.; Christensen, R.D. Transplacental passage of recombinant human granulocyte colony-stimulating factor in women with an imminent preterm delivery. Am. J. Obstet. Gynecol. 1996, 174, 1306–1311. [Google Scholar] [CrossRef]
- Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available online: https://ctep.cancer.gov/ (accessed on 10 December 2020).
- Smith, T.J.; Bohlke, K.; Armitage, J.O. Recommendations for the Use of White Blood Cell Growth Factors: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Oncol. Pract. 2015, 11, 511–513. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group. Increasing the dose intensity of chemotherapy by more frequent administration or sequential scheduling: A patient-level meta-analysis of 37,298 women with early breast cancer in 26 randomised trials. Lancet 2019, 393, 1440–1452. [Google Scholar]
- Cardonick, E.; Gilmandyar, D.; Somer, R.A. Maternal and Neonatal Outcomes of Dose-Dense Chemotherapy for Breast Cancer in Pregnancy. Obstet. Gynecol. 2012, 120, 1267–1272. [Google Scholar] [CrossRef] [PubMed]
- Cardonick, E.; Irfan, F.; Torres, N. The Use of Neupogen (Filgrastim) or Neulasta (Pegfilgrastim) during Pregnancy When Chemotherapy Is Indicated for Maternal Cancer Treatment. J. Cancer Ther. 2012, 3, 157–161. [Google Scholar] [CrossRef] [Green Version]
- Schmutz, N.; Henry, E.; Jopling, J.; Christensen, R.D. Expected ranges for blood neutrophil concentrations of neonates: The Manroe and Mouzinho charts revisited. J. Perinatol. 2008, 28, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, A. Neutropenia in the newborn. Curr. Opin. Hematol. 2014, 21, 43–49. [Google Scholar] [CrossRef] [Green Version]
- La Nasa, M.; Gaughan, J.; Cardonick, E. Incidence of Neonatal Neutropenia and Leukopenia After In Utero Exposure to Chemotherapy for Maternal Cancer. Am. J. Clin. Oncol. 2019, 42, 351–354. [Google Scholar] [CrossRef]
- Sillers, L.; Van Slambrouck, C.; Lapping-Carr, G. Neonatal Thrombocytopenia: Etiology and Diagnosis. Pediatr. Ann. 2015, 44, e175–e180. [Google Scholar] [CrossRef] [PubMed]
- Widness, J.A. Pathophysiology of Anemia During the Neonatal Period, Including Anemia of Prematurity. NeoReviews 2008, 9, e520–e525. [Google Scholar] [CrossRef] [Green Version]
- Customised Centile Calculator GROW v8.0.4. Available online: https://www.gestation.net/ (accessed on 10 December 2020).
- Lyman, G.H.; Barron, R.L.; Natoli, J.L.; Miller, R.M. Systematic review of efficacy of dose-dense versus non-dose-dense chemotherapy in breast cancer, non-Hodgkin lymphoma, and non-small cell lung cancer. Crit. Rev. Oncol. Hematol. 2012, 81, 296–308. [Google Scholar] [CrossRef]
- van Hasselt, J.G.; van Calsteren, K.; Heyns, L.; Han, S.; Mhallem Gziri, M.; Schellens, J.H.; Beijnen, J.H.; Huitema, A.D.; Amant, F. Optimizing anticancer drug treatment in pregnant cancer patients: Pharmacokinetic analysis of gestation-induced changes for doxorubicin, epirubicin, docetaxel and paclitaxel. Ann. Oncol. 2014, 25, 2059–2065. [Google Scholar] [CrossRef]
- Smith, T.J.; Khatcheressian, J.; Lyman, G.H.; Ozer, H.; Armitage, J.O.; Balducci, L.; Bennett, C.L.; Cantor, S.B.; Crawford, J.; Cross, S.J.; et al. 2006 Update of Recommendations for the Use of White Blood Cell Growth Factors: An Evidence-Based Clinical Practice Guideline. J. Clin. Oncol. 2006, 24, 3187–3205. [Google Scholar] [CrossRef] [Green Version]
- Jabagi, M.J.; Vey, N.; Goncalves, A.; Le Tri, T.; Zureik, M.; Dray-Spira, R. Risk of secondary hematologic malignancies associated with breast cancer chemotherapy and G-CSF support: A nationwide population-based cohort. Int. J. Cancer 2020, 148, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, P.S.; Zeidler, C.; Bolyard, A.A.; Alter, B.P.; Bonilla, M.A.; Boxer, L.A.; Dror, Y.; Kinsey, S.; Link, D.C.; Newburger, P.E.; et al. Stable long-term risk of leukaemia in patients with severe congenital neutropenia maintained on G-CSF therapy. Br. J. Haematol. 2010, 150, 196–199. [Google Scholar] [CrossRef] [Green Version]
- Leblanc, R.; Roy, J.; Demers, C.; Vu, L.; Cantin, G. A prospective study of G-CSF effects on hemostasis in allogeneic blood stem cell donors. Bone Marrow Transplant. 1999, 23, 991–996. [Google Scholar] [CrossRef] [Green Version]
- Kaptan, K.; Beyan, C.; Ifran, A. Granulocyte colony-stimulating factor and hypercoagulability. Int. J. Cardiol. 2008, 131, 129. [Google Scholar] [CrossRef] [PubMed]
- Boxer, L.A.; Bolyard, A.A.; Kelley, M.L.; Marrero, T.M.; Phan, L.; Bond, J.M.; Newburger, P.E.; Dale, D.C. Use of granulocyte colony-stimulating factor during pregnancy in women with chronic neutropenia. Obstet. Gynecol. 2015, 125, 197–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, R.; Modi, N.; Dore, C. G-CSF and GM-CSF for treating or preventing neonatal infections. Cochrane Database Syst. Rev. 2003, 2003, CD003066. [Google Scholar] [CrossRef]
- Cottle, T.E.; Fier, C.J.; Donadieu, J.; Kinsey, S.E. Risk and benefit of treatment of severe chronic neutropenia with granulocyte colony-stimulating factor. Semin. Hematol. 2002, 39, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Dale, D.C.; Cottle, T.E.; Fier, C.J.; Bolyard, A.A.; Bonilla, M.A.; Boxer, L.A.; Cham, B.; Freedman, M.H.; Kannourakis, G.; Kinsey, S.E.; et al. Severe chronic neutropenia: Treatment and follow-up of patients in the Severe Chronic Neutropenia International Registry. Am. J. Hematol. 2003, 72, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Zeidler, C.; Grote, U.A.; Nickel, A.; Brand, B.; Carlsson, G.; Cortesao, E.; Dufour, C.; Duhem, C.; Notheis, G.; Papadaki, H.A.; et al. Outcome and management of pregnancies in severe chronic neutropenia patients by the European Branch of the Severe Chronic Neutropenia International Registry. Haematologica 2014, 99, 1395–1402. [Google Scholar] [CrossRef] [Green Version]
- Kaufmann, S.J.; Sharif, K.; Sharma, V.; McVerry, B.A. Term delivery in a woman with severe congenital neutropenia, treated with growth colony stimulating factor. Hum. Reprod. 1998, 13, 498–499. [Google Scholar] [CrossRef] [Green Version]
- Ohba, T.; Yoshimura, T.; Araki, M.; Miyoshi, J.; Yonemura, Y.; Matsuura, K.; Okamura, H. Aplastic anemia in pregnancy: Treatment with cyclosporine and granulocyte-colony stimulating factor. Acta Obstet. Gynecol. Scand. 1999, 78, 458–461. [Google Scholar]
- Sangalli, M.R.; Peek, M.; McDonald, A. Prophylactic granulocyte colony-stimulating factor treatment for acquired chronic severe neutropenia in pregnancy. Aust. N. Z. J. Obstet. Gynaecol. 2001, 41, 470–471. [Google Scholar] [CrossRef]
- Fung, Y.L.; Pitcher, L.A.; Taylor, K.; Minchinton, R.M. Managing passively acquired autoimmune neonatal neutropenia: A case study. Transfus. Med. 2005, 15, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Sun, J.-L.; Zhang, Z.-L.; Pei, H.-H. Pregnancy complicated with agranulocytosis. Medicine 2016, 95, e5717. [Google Scholar] [CrossRef]
- Kikkawa, M.; Matsubara, S.; Takatoku, M.; Kuwata, T.; Ohkuchi, A.; Izumi, A.; Watanabe, T.; Suzuki, M. Granulocyte-colony stimulating factor for the treatment of ritodrine-induced neutropenia. J. Obstet. Gynaecol. Res. 2008, 34, 286–290. [Google Scholar] [CrossRef]
- Wang, C.Y.; Lai, Y.J.; Hwang, K.S.; Chen, C.H.; Yu, M.H.; Chen, H.T.; Su, H.Y. Successful treatment with granulocyte-colony stimulating factor for ritodrine-induced neutropenia in a twin pregnancy. Taiwan. J. Obstet. Gynecol. 2016, 55, 738–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pessach, I.; Shimoni, A.; Nagler, A. Granulocyte-colony stimulating factor for hematopoietic stem cell donation from healthy female donors during pregnancy and lactation: What do we know? Hum. Reprod. Update 2013, 19, 259–267. [Google Scholar] [CrossRef]
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef]
- Prevalences Rates of All Congenital Malformations by Year. Available online: https://eu-rd-platform.jrc.ec.europa.eu/ (accessed on 10 December 2020).
- Cardonick, E.; Iacobucci, A. Use of chemotherapy during human pregnancy. Lancet Oncol. 2004, 5, 283–291. [Google Scholar] [CrossRef]
- Eurocat. Malformation Coding Guides. Available online: http://www.eurocat-network.eu (accessed on 10 February 2021).
- Del Mastro, L.; De Placido, S.; Bruzzi, P.; De Laurentiis, M.; Boni, C.; Cavazzini, G.; Durando, A.; Turletti, A.; Nistico, C.; Valle, E.; et al. Fluorouracil and dose-dense chemotherapy in adjuvant treatment of patients with early-stage breast cancer: An open-label, 2 × 2 factorial, randomised phase 3 trial. Lancet 2015, 385, 1863–1872. [Google Scholar] [CrossRef]
- Lurie, S.; Rahamim, E.; Piper, I.; Golan, A.; Sadan, O. Total and differential leukocyte counts percentiles in normal pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 136, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Pavord, S.; Daru, J.; Prasannan, N.; Robinson, S.; Stanworth, S.; Girling, J.; on behalf of the BSH Committee. UK guidelines on the management of iron deficiency in pregnancy. Br. J. Haematol. 2020, 188, 819–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amant, F.; Vandenbroucke, T.; Verheecke, M.; Fumagalli, M.; Halaska, M.J.; Boere, I.; Han, S.; Gziri, M.M.; Peccatori, F.; Rob, L.; et al. Pediatric Outcome after Maternal Cancer Diagnosed during Pregnancy. N. Engl. J. Med. 2015, 373, 1824–1834. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, B.; Edmonds, C.J. School Age Neurological and Cognitive Outcomes of Fetal Growth Retardation or Small for Gestational Age Birth Weight. Front. Endocrinol. 2019, 10, 186. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Maternal Characteristics | Median | Range |
|---|---|---|
| Age at diagnosis (years) | 34 | 19–47 |
| BMI at booking (kg/m2) * | 25.9 | 18.3–36.9 |
| Number | % | |
| Ethnicity | ||
| Caucasian | 32 | 76.2 |
| Non-caucasian | 6 | 14.3 |
| Not reported | 4 | 9.5 |
| Type of malignancy | ||
| Breast cancer | 35 | 83.3 |
| Non Hodgkin lymphoma | 5 | 11.9 |
| Ewing sarcoma | 1 | 2.4 |
| Acute lymphocytic leukemia | 1 | 2.4 |
| Treatment modality | ||
| Chemotherapy | 28 | 66.7 |
| Chemotherapy + surgery | 14 | 33.3 |
| Chemotherapy | ||
| Anthracycline-based | 18 | 42.9 |
| Anthracycline-based with taxanes | 15 | 35.7 |
| Other ** | 9 | 21.4 |
| Median | Range | |
| Gestational age at first chemo (weeks) | 22 | 11–36 |
| Cycles of chemotherapy during pregnancy | 6 | 1–16 |
| Administrations of G-CSF | 4 | 1–16 |
| Number | % | |
| Indication G-CSF | ||
| Prophylactic in dose dense chemotherapy | 28 | 66.7 |
| Propyhlactic in polychemotherapy regimen | 7 | 16.7 |
| Prophylactic before delivery | 2 | 4.8 |
| Following chemotherapy-induced neutropenia | 5 | 11.9 |
| Type of G-CSF | ||
| Pegfilgrastim | 28 | 66.7 |
| Lipefilgrastim | 8 | 19.1 |
| Filgrastim | 3 | 7.1 |
| Not reported | 3 | 7.1 |
| Maternal Blood Results | Total n * | Grade 1–2 | Grade 3–4 | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Neutropenia | 5 | 21 | 2 | 8 | 3 * | 13 |
| Leukopenia * | 4 | 17 | 2 | 8 | 2 | 8 |
| Thrombocytopenia | 0 | 0 | 0 | 0 | 0 | 0 |
| Anemia | 16 | 67 | 14 | 58 | 2 | 8 |
| Obstetric Outcomes | n | % |
|---|---|---|
| Live birth | 39 | 97.5 |
| Still Birth | 1 | 2.5 |
| Gestational age at delivery (n = 39 *) | ||
| ≥37 weeks (a term) | 20 | 51.3 |
| <37 weeks (pre term) | 19 | 48.7 |
| Onset of labor | ||
| Spontaneous | 13 | 32.05 |
| Induction of labor | 18 | 45.0 |
| Cesarean section | 9 | 22.5 |
| Emergency (fetal distress) | 2 | 22.2 |
| Elective (all for obstetrical reason **) | 7 | 77.8 |
| Reason induction of labor (n = 18) | ||
| Obstetrical reason *** | 1 | 5.6 |
| Therapy planning | 14 | 77.8 |
| Deterioration of maternal condition | 2 | 11.1 |
| Other | 1 | 5.6 |
| Mode of delivery | ||
| Vaginal delivery | 27 | 67.5 |
| Assisted vaginal delivery | 2 | 5.0 |
| Elective Cesarean section | 8 | 20.0 |
| Emergency cesarean section | 3 | 7.5 |
| Complications | ||
| Maternal infection (including 1 chorioamnionitis) | 4 (1 postpartum) | 10.0 |
| Gestational diabetes | 1 | 2.5 |
| Preeclampsia | 1 | 2.5 |
| Maternal neutropenia/leukopenia | 7 | 17.5 |
| PPROM or preterm contractions | 9 | 22.5 |
| Stillbirth | 1 | 2.5 |
| Postpartum hemorrhage | 2 | 5.0 |
| Neonatal Outcomes | Median | Range |
|---|---|---|
| Birth weight (grams) | 2855 | 850–3780 |
| n | % | |
| Customized birthweight percentile | ||
| <10 | 11 | 28.2 |
| 11–49 | 18 | 46.1 |
| 50–89 | 8 | 20.5 |
| >90 | 2 | 5.1 |
| APGAR at 5 min | ||
| 4 | 1 | 2.6 |
| 9 | 8 | 20.5 |
| 10 | 29 | 74.4 |
| Not reported | 1 | 2.6 |
| Congenital malformation | ||
| yes | 2 | 5.1 |
| no | 37 | 94.8 |
| Admission neonatal care unit | ||
| yes | 16 | 41.0 |
| no | 20 | 51.3 |
| Not reported | 3 | 7.7 |
| Reason admission neonatal care unit | ||
| Prematurity | 13 | 81.3 |
| Observation because of maternal chemotherapy | 1 | 6.3 |
| Other | 2 | 12.5 |
| Neonatal blood results | ||
| Leukopenia * | 0 | 0 |
| Neutropenia ** | 0 | 0 |
| Thrombocytopenia *** | 1 | 5.8 |
| Anemia **** | 2 | 10 |
| Neonatal complications | ||
| Hyperbilirubinemia | 2 | 5.2 |
| Neonatal sepsis | 3 | 7.7 |
| First degree cerebral bleeding related to prematurity | 1 | 2.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berends, C.; Maggen, C.; Lok, C.A.R.; van Gerwen, M.; Boere, I.A.; Wolters, V.E.R.A.; Van Calsteren, K.; Segers, H.; van den Heuvel-Eibrink, M.M.; Painter, R.C.; et al. Maternal and Neonatal Outcome after the Use of G-CSF for Cancer Treatment during Pregnancy. Cancers 2021, 13, 1214. https://doi.org/10.3390/cancers13061214
Berends C, Maggen C, Lok CAR, van Gerwen M, Boere IA, Wolters VERA, Van Calsteren K, Segers H, van den Heuvel-Eibrink MM, Painter RC, et al. Maternal and Neonatal Outcome after the Use of G-CSF for Cancer Treatment during Pregnancy. Cancers. 2021; 13(6):1214. https://doi.org/10.3390/cancers13061214
Chicago/Turabian StyleBerends, Claudia, Charlotte Maggen, Christianne A. R. Lok, Mathilde van Gerwen, Ingrid A. Boere, Vera E. R. A. Wolters, Kristel Van Calsteren, Heidi Segers, Marry M. van den Heuvel-Eibrink, Rebecca C. Painter, and et al. 2021. "Maternal and Neonatal Outcome after the Use of G-CSF for Cancer Treatment during Pregnancy" Cancers 13, no. 6: 1214. https://doi.org/10.3390/cancers13061214