
Prognostic Value of Carcinoembryonic Antigen (CEA) and Carbohydrate Antigen 19-9 (CA 19-9) in Gallbladder Cancer; 65 IU/mL of CA 19-9 Is the New Cut-Off Value for Prognosis

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
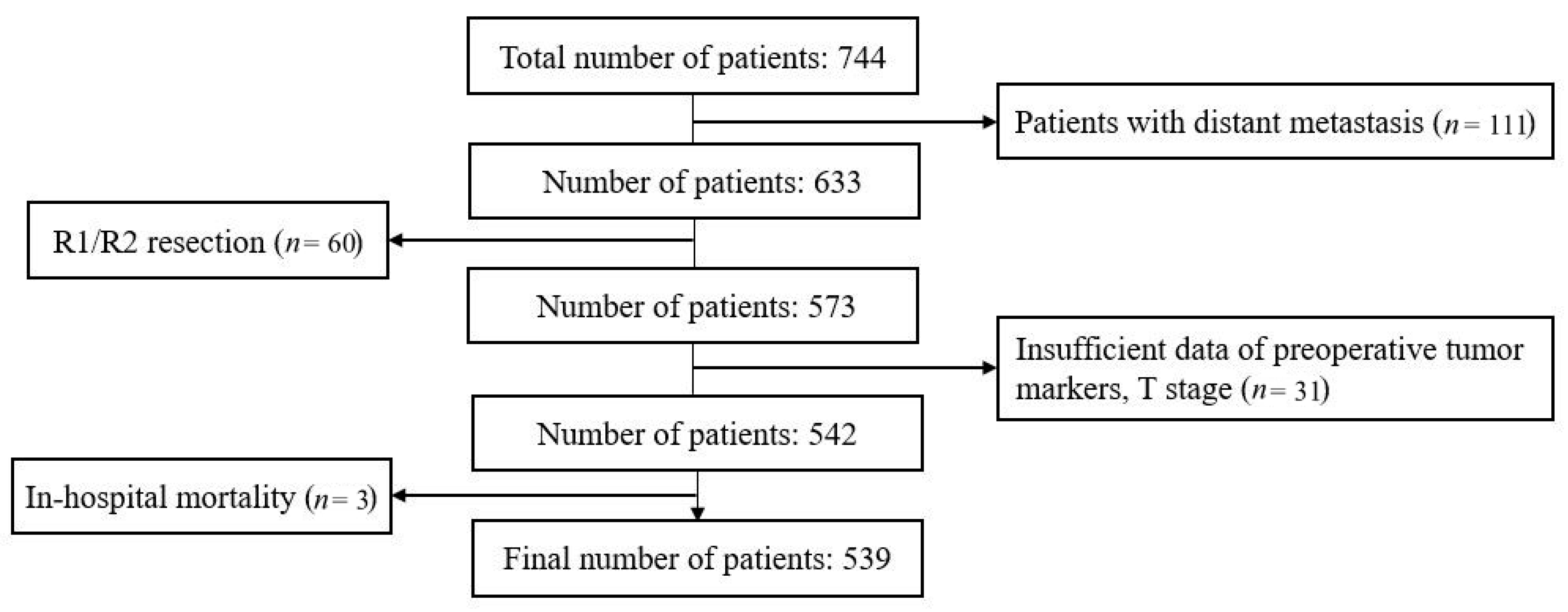
2.1. Patients and Data Collection
2.2. Statistical Analysis
3. Results
3.1. Demographics
3.2. Tumor Marker Distribution
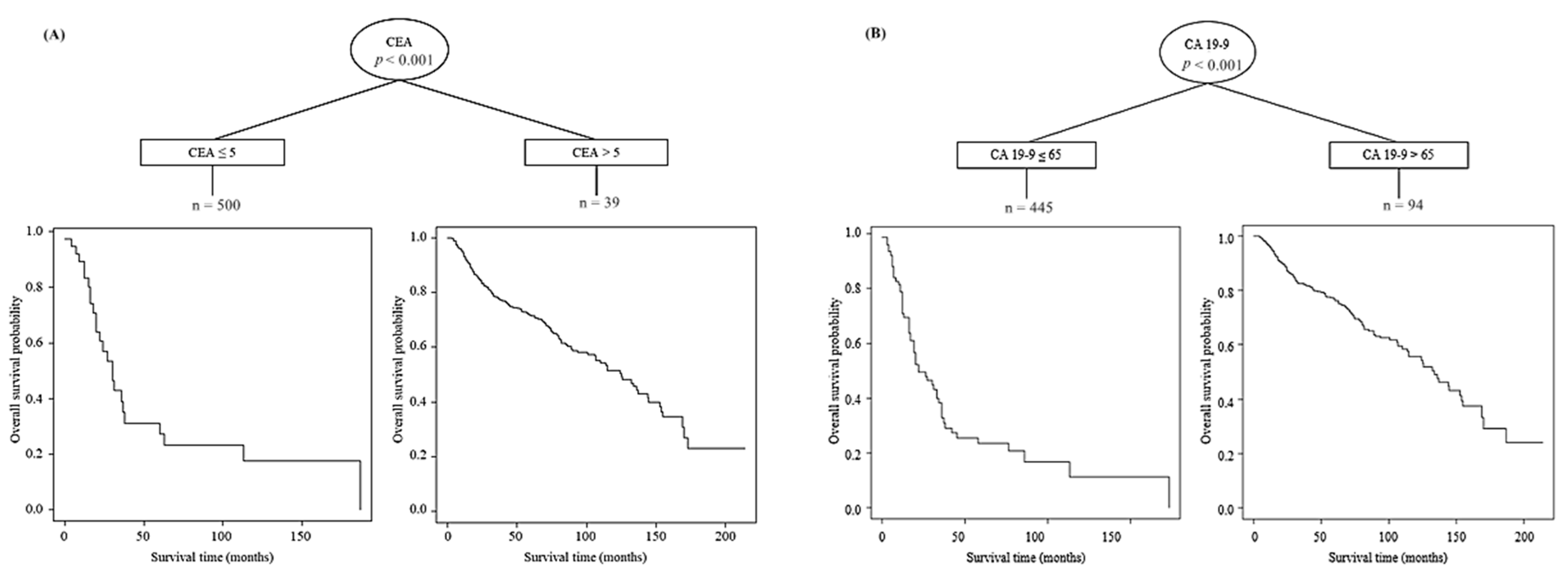
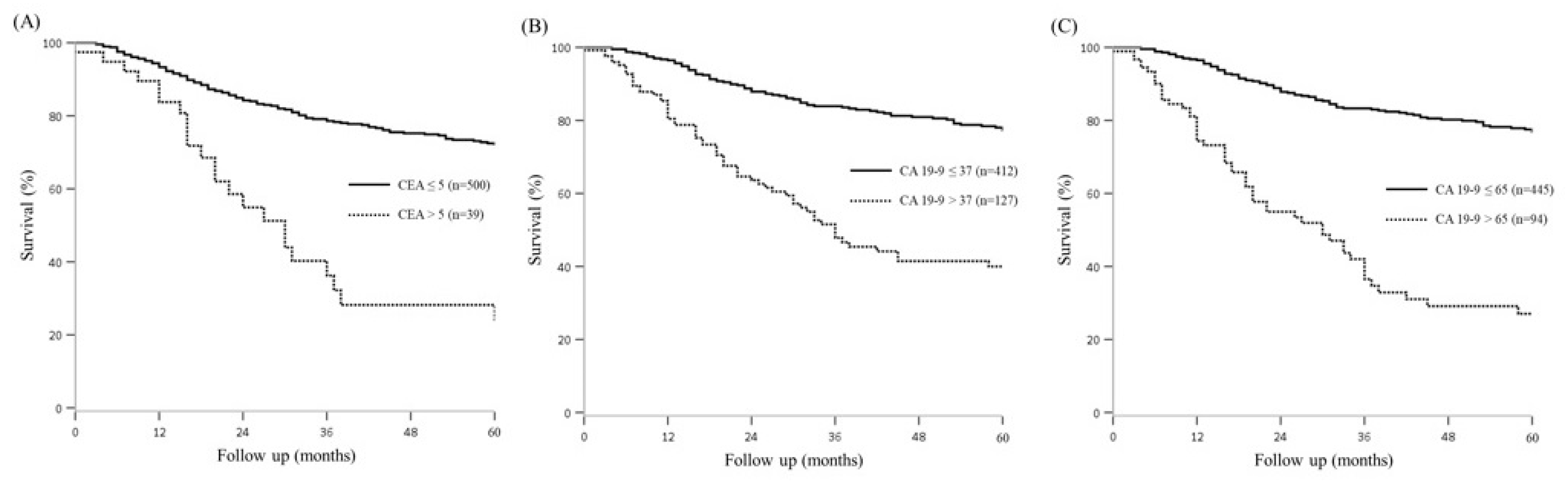
3.3. Survival According to the Tumor Marker and Optimal Cut Off Value
3.4. Prognostic Factors for Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mohamed, A.; Donald, W. Tumor markers in Cancer Diagnosis and Prognosis. CA Cancer J. Clin. 1988, 38, 104–126. [Google Scholar]
- Sachan, A.; Saluja, S.S. Raised CA19–9 and CEA have prognostic relevance in gallbladder carcinoma. BMC Cancer 2020, 20, 826. [Google Scholar] [CrossRef] [PubMed]
- Moon, D.K.; Kim, H.B. Preoperative carbohydrate antigen 19-9 and standard uptake value of positron emission tomography-computed tomography as prognostic markers in patients with pancreatic ductal adenocarcinoma. J Hepato Biliary Pancreat. Sci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Misra, S.; Chaturvedi, A. Carcinoma of the gallbladder. Lancet Oncol. 2003, 3, 167–176. [Google Scholar] [CrossRef]
- Hundal, R.; Shaffer, E.A. Gallbladder cancer: Epidemiology and outcome. Clin. Epidemiol. 2014, 6, 99–109. [Google Scholar] [PubMed]
- Stro, B.L.; Maislin, G. Serum CEA and CA 19-91 Potential Future Diagnostic or Screening Tests for Gallbladder Cancer? Int. J. Cancer. 1990, 45, 821–824. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Feng, F. Combined detection tumor markers for diagnosis and prognosis of gallbladder cancer. World J. Gastroenterol. 2014, 20, 4085–4092. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Park, W. Optimal surgical treatment in patients with T1b gallbladder cancer: An international multicenter study. J. Hepatobiliary Pancreat. Sci. 2018, 25, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, T.; Abe, T.; Amano, H.; Hanada, K.; Hattori, M.; Kobayashi, T.; Nakahara, M.; Ohdan, H.; Noriyuki, T. Efficacy of the gallbladder cancer predictive risk score based on pathological findings: A propensity score-matched analysis. Ann. Surg. Oncol. 2018, 25, 1699–1708. [Google Scholar] [CrossRef] [PubMed]
- Wen, Z.; Si, A. Elevation of CA19-9 and CEA is associated with a poor prognosis in patients with resectable gallbladder carcinoma. HPB 2017, 19, 951–956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, T.; Yu, H.; Cai, X. Preoperative prediction of survival in resectable gallbadder cancer by a combined utilization of CA 19-9 and carcinoembryonic antigen. Chin. Med. J. 2014, 12, 127. [Google Scholar]
- Agrawal, S.; Lawrence, A. Does CA 19-9 Have Prognostic Relevance in Gallbladder Carcinoma (GBC)? J. Gastrointest. Cancer 2018, 49, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Liska, V.; Treska, V.; Skalicky, T.; Fichtl, J.; Bruha, J.; Vycital, O.; Topolcan, O.; Palek, R.; Rosendorf, J.; Polivka, J.; et al. Evaluation of tumor markers and their impact on prognosis in gallbladder, bile duct and cholangiocellular carcinomas—A pilot study. Anticancer Res. 2017, 37, 2003–2010. [Google Scholar] [PubMed] [Green Version]
- Xu, W.; Zhang, H. Prognostic significance of combined preoperative fibrinogen and CA199 in gallbladder cancer patients. World J. Gastroenterol. 2018, 24, 1451–1463. [Google Scholar] [CrossRef] [PubMed]
- Moradi, F.; Iagaru, A. The Role of Positron Emission Tomography in Pancreatic Cancer and Gallbladder Cancer. Semin. Nucl. Med. 2020, 50, 434–446. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.K.; Cho, M.S. Prognostic significance of muc4 expression in gallbladder carcinoma. World J. Surg. Oncol. 2012, 10, 224–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mojica, P.; Smith, D. Adjuvant Radiation Therapy for Gallbladder Carcinoma. J. Surg. Oncol. 2007, 96, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Kim, S.H. Adjuvant Chemoradiation Therapy in Gallbladder Cancer. J. Surg. Oncol. 2010, 102, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Gold, D.G.; Miller, R.C. Adjuvant Therapy for Gallbladder Carcinoma: The Mayo Clinic Experience. Int. J. Radiat. Oncol. 2009, 75, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Mantripragada, K.C.; Hamid, F. Adjuvant Therapy for Resected Gallbladder Cancer: Analysis of the National Cancer Data Base. JNCI J. Natl. Cancer Inst. 2017, 109, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables n = 539 | CA 19-9 ≤ 37 n = 412 | CA 19-9 > 37 n = 127 | p-Value | CA 19-9 ≤ 65 n = 445 | CA 19-9 > 65 n = 94 | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| Age (years) | 65.3 (10.4) | 65.5 (10.6) | 64.7 (10.0) | 0.072 | 65.4 (10.6) | 64.8 (9.6) | 0.121 | |
| Gender | Male | 255 (47.3) | 203 (49.3) | 52 (40.9) | <0.001 | 215 (48.3) | 40 (42.6) | 0.007 |
| Female | 284 (52.7) | 209 (50.7) | 75 (59.1) | 230 (51.7) | 54 (57.4) | |||
| Total bilirubin (mg/dL) | ≤1.3 | 362 (67.2) | 282 (68.4) | 80 (63.0) | 0.038 | 306 (68.8) | 56 (59.6) | 0.005 |
| >1.3 | 177 (32.8) | 130 (31.6) | 47 (37.0) | 139 (31.2) | 38 (40.4) | |||
| Operation type | Simple | 172 (31.9) | 142 (34.5) | 30 (23.6) | 0.599 | 152 (34.2) | 20 (21.3) | 0.265 |
| Extended | 305 (56.6) | 239 (58.0) | 66 (52.0) | 259 (58.2) | 46 (48.9) | |||
| Others | 62 (11.5) | 31 (7.5) | 31 (24.4) | 34 (7.6) | 28 (29.8) | |||
| Differentiation | WD | 187 (34.7) | 163 (39.6) | 24 (18.9) | 0.003 | 170 (38.2) | 17 (18.1) | 0.008 |
| MD | 196 (36.4) | 128 (31.1) | 68 (53.5) | 145 (32.6) | 51 (54.3) | |||
| PD | 51 (9.5) | 37 (9.0) | 14 (11.0) | 40 (9.0) | 11 (11.7) | |||
| N/A | 105 (19.5) | 84 (20.4) | 21 (16.5) | 90 (20.2) | 15 (16.0) | |||
| T stage | T1 | 143 (26.5) | 131 (31.8) | 12 (9.4) | 0.131 | 136 (30.6) | 7 (7.4) | 0.053 |
| T2 | 296 (54.9) | 232 (56.3) | 64 (50.4) | 254 (57.1) | 42 (44.7) | |||
| T3 | 94 (17.4) | 45 (10.9) | 49 (38.6) | 51 (11.5) | 43 (45.7) | |||
| T4 | 6 (1.1) | 4 (1.0) | 2 (1.6) | 4 (0.9) | 2 (2.1) | |||
| Node metastasis | Positive | 144 (26.7) | 80 (19.4) | 64 (50.3) | <0.001 | 91 (20.5) | 53 (56.4) | <0.001 |
| Negative | 395 (73.3) | 332 (80.6) | 63 (49.6) | 354 (79.6) | 41 (43.6) | |||
| Complication | Yes | 45 (8.3) | 21 (5.1) | 24 (18.9) | <0.001 | 25 (5.6) | 20 (21.3) | <0.001 |
| No | 494 (91.7) | 391 (94.9) | 103 (81.1) | 420 (94.4) | 74 (78.7) | |||
| Chemotherapy | Yes | 85 (15.8) | 55 (13.3) | 30 (23.6) | <0.001 | 60 (13.5) | 25 (26.6) | <0.001 |
| No | 454 (84.2) | 357 (86.7) | 97 (76.4) | 385 (86.5) | 69 (73.4) | |||
| Radiotherapy | Yes | 76 (14.1) | 45 (10.9) | 31 (24.4) | <0.001 | 50 (11.1) | 26 (27.7) | <0.001 |
| No | 467 (85.9) | 367 (89.1) | 96 (75.6) | 395 (88.8) | 68 (72.3) | |||
| Recurrence | Yes | 131 (24.5) | 76 (18.4) | 55 (43.3) | <0.001 | 83 (18.7) | 48 (51.1) | <0.001 |
| No | 408 (75.7) | 336 (81.6) | 72 (56.7) | 362 (81.3) | 46 (48.9) | |||
| Variable | Patients (n = 539) | 2-Year OS (%) | 5-Year OS (%) | p | Multivariate | ||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | |||||
| Sex male/female | 255/284 | 81.8/82.7 | 68.1/69.7 | 0.649 | |||
| Age (years) ≤ 60/>60 | 164/375 | 84.9/81.0 | 71.4/67.8 | <0.001 | 2.245 | 1.562–3.226 | <0.001 |
| Total bilirubin (mg/dL) ≤ 1.3/> 1.3 | 362/177 | 85.5/76.1 | 72.5/62.6 | 0.710 | |||
| CEA (ng/mL) ≤ 5/>5 | 500/39 | 84.2/54.9 | 72.1/24.2 | 0.029 | 1.613 | 1.037–2.510 | 0.034 |
| CA19-9 (IU/mL) ≤ 65/>65 | 445/94 | 87.8/55.0 | 76.8/24.0 | <0.001 | 2.557 | 1.763–3.710 | <0.001 |
| Operation type Simple/Extended | 172/305 | 86.5/84.7 | 69.8/74.4 | 0.004 | 0.567 | 0.399–0.804 | 0.001 |
| T stage 1–2/T stage 3–4 | 439/100 | 87.5/57.8 | 75.8/38.0 | 0.015 | 1.752 | 1.162–2.641 | 0.007 |
| N negative/positive | 395/144 | 89.4/62.5 | 78.7/42.1 | <0.001 | 2.341 | 1.668–3.287 | <0.001 |
| Complication Y/N | 45/494 | 65.9/83.7 | 50.2/70.6 | 0.672 | |||
| Chemotherapy Y/N | 85/454 | 67.2/85.4 | 51.0/72.8 | 0.353 | |||
| Radiation therapy Y/N | 76/463 | 63.6/85.6 | 48.7/72.7 | 0.189 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Kim, H.; Han, Y.; Sohn, H.; Kang, J.S.; Kwon, W.; Jang, J.-Y. Prognostic Value of Carcinoembryonic Antigen (CEA) and Carbohydrate Antigen 19-9 (CA 19-9) in Gallbladder Cancer; 65 IU/mL of CA 19-9 Is the New Cut-Off Value for Prognosis. Cancers 2021, 13, 1089. https://doi.org/10.3390/cancers13051089
Kim M, Kim H, Han Y, Sohn H, Kang JS, Kwon W, Jang J-Y. Prognostic Value of Carcinoembryonic Antigen (CEA) and Carbohydrate Antigen 19-9 (CA 19-9) in Gallbladder Cancer; 65 IU/mL of CA 19-9 Is the New Cut-Off Value for Prognosis. Cancers. 2021; 13(5):1089. https://doi.org/10.3390/cancers13051089
Chicago/Turabian StyleKim, Myongjin, Hongbeom Kim, Youngmin Han, Heeju Sohn, Jae Seung Kang, Wooil Kwon, and Jin-Young Jang. 2021. "Prognostic Value of Carcinoembryonic Antigen (CEA) and Carbohydrate Antigen 19-9 (CA 19-9) in Gallbladder Cancer; 65 IU/mL of CA 19-9 Is the New Cut-Off Value for Prognosis" Cancers 13, no. 5: 1089. https://doi.org/10.3390/cancers13051089