
Outcome of Stage IV Completely Necrotic Wilms Tumour and Local Stage III Treated According to the SIOP 2001 Protocol

 ,
,  , , , , , , , ,
, , , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Treatment Protocol
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
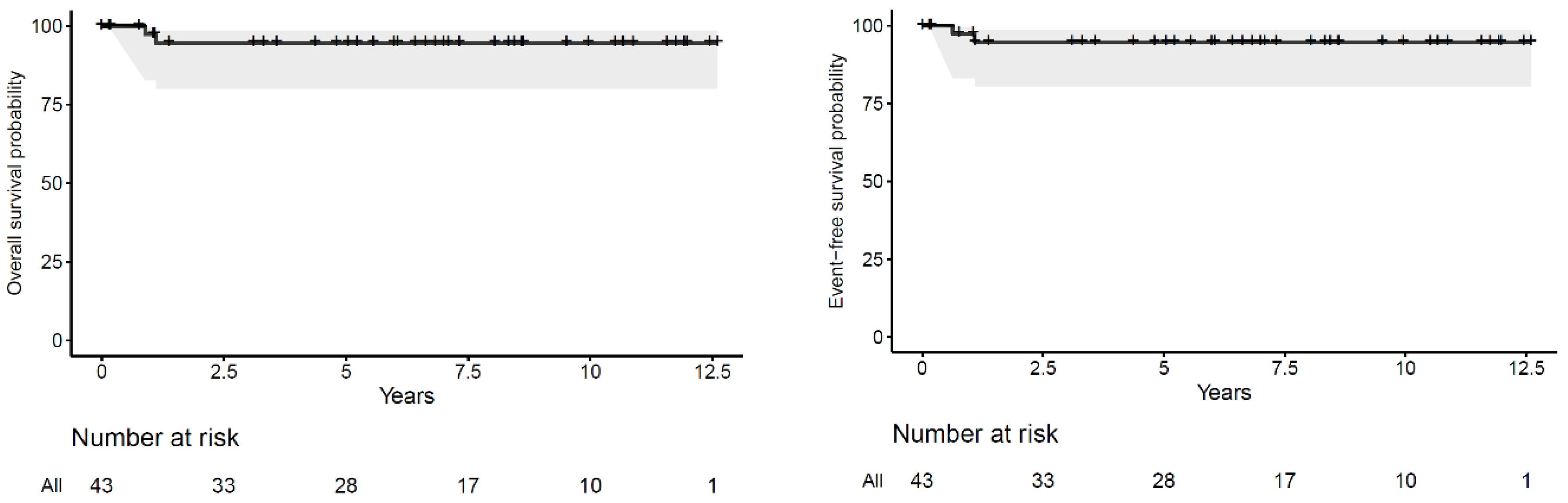
3.2. Disease Control and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Den Heuvel-eibrink, M.M.; Hol, J.A.; Pritchard-Jones, K.; Van Tinteren, H.; Furtwängler, R.; Verschuur, A.C.; Vujanic, G.M.; Leuschner, I.; Brok, J.; Rübe, C.; et al. Position paper: Rationale for the treatment of Wilms tumour in the UMBRELLA SIOP-RTSG 2016 protocol. International Society of Paediatric Oncology—Renal Tumour Study Group (SIOP–RTSG). Nat. Rev. Urol. 2017, 14, 743–752. [Google Scholar] [CrossRef] [Green Version]
- Iaboni, D.S.M.; Chi, Y.-Y.; Kim, Y.; Dome, J.S.; Fernandez, C.V. Outcome of Wilms tumor patients with bone metastasis enrolled on National Wilms Tumor Studies 1–5: A report from the Children’s Oncology Group. Pediatr. Blood Cancer 2019, 66, e27430. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.; Fernandez-Pineda, I.; Cabello, R.; Ramírez-Villar, G.L.; Márquez-Vega, C.; Nustede, R.; Linderkamp, C.; Schmid, I.; Neth, O.; Graf, N.; et al. The Relationship between the site of metastases and outcome in children with stage IV Wilms Tumor: Data from 3 European Pediatric Cancer Institutions. J. Pediatr. Hematol. Oncol. 2013, 35, 518–524. [Google Scholar] [CrossRef] [Green Version]
- Verschuur, A.; Tinteren, H.V.; Graf, N.; Bergeron, C.; Sandstedt, B.; de Kraker, J. Treatment of Pulmonary Metastasis in Children With Stage IV Nephroblastoma With Risk-Based Use of Pulmonary Radiotherapy. J. Clin. Oncol. 2012, 30, 980–988. [Google Scholar] [CrossRef]
- Ehrlich, P.F.; Ferrer, F.A.; Ritchey, M.L.; Anderson, J.R.; Green, D.M.; Grundy, P.E.; Dome, J.S.; Kalapurakal, J.A.; Perlman, E.J.; Shamberger, R.C. Hepatic metastasis at diagnosis in patients with Wilms tumor is not an independent adverse prognostic factor for stage IV Wilms tumor. A report from the Childrens Oncology Group/National Wilms Tumor Study Group. Ann. Surg. 2009, 250, 642–648. [Google Scholar] [CrossRef] [Green Version]
- Dix, D.B.; Seibel, N.L.; Chi, Y.Y.; Khanna, G.; Gratias, E.; Anderson, J.R.; Mullen, E.A.; Geller, J.I.; Kalapurakal, J.A.; Paulino, A.C.; et al. Treatment of Stage IV Favorable Histology Wilms Tumor with Lung Metastases: A Report From the Children’s Oncology Group AREN0533 Study. J. Clin. Oncol. 2018, 36, 1564–1570. [Google Scholar] [CrossRef] [PubMed]
- Irtan, S.; Ehrlich, P.F.; Pritchard-Jones, K. Wilms tumor: “State-of-the-art” update. Semin. Pediatric Surg. 2016, 25, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Warmann, S.W.; Furtwängler, R.; Blumenstock, G.; Armeanu, S.; Nourkami, N.; Leuschner, I.; Schenk, J.P.; Graf, N.; Fuchs, J. Tumor Biology Influences the Prognosis of Nephroblastoma Patients With Primary Pulmonary Metastases: Results From SIOP 93-01/GPOH and SIOP 2001/GPOH. Ann. Surg. 2011, 254, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Dome, J.S.; Cotton, C.A.; Perlman, E.J.; Breslow, N.E.; Kalapurakal, J.A.; Ritchey, M.L.; Grundy, P.E.; Malogolowkin, M.; Beckwith, J.B.; Shamberger, R.C.; et al. Treatment op anaplastic histology Wilms’ Tumor: Results from the Fifth National Wilms’ Tumor Study. J. Clin. Oncol. 2006, 24, 2352–2358. [Google Scholar] [CrossRef]
- Weirich, A.; Leuschner, I.; Harms, D.; Vujanic, G.M.; Tröger, J.; Abel, U.; Graf, N.; Schmidt, D.; Ludwig, R.; Voûte, P.A. Clinical impact of histologic subtypes in localized non-anaplastic nephroblastoma treated according to the trial and study SIOP-9/GPOH. Ann. Oncol. 2001, 12, 311–319. [Google Scholar] [CrossRef]
- Boccon-Gibod, L.; Rey, A.; Sandstedt, B.; Delemarre, J.; Harms, D.; Vujanic, G.; De Kraker, J.; Weirich, A.; Tournade, M.-F. Complete necrosis induced by preoperative chemotherapy in Wilms tumor as an indicator of low risk: Report of the International Society of Paediatric Oncology (SIOP) Nephroblastoma Trial and Study. Med. Pediatr. Oncol. 2000, 34, 183–190. [Google Scholar] [CrossRef]
- Godzinski, J. The current status of treatment of Wilms’ tumor as per the SIOP trials. J. Indian Assoc. Pediatr. Surg. 2015, 20, 16–20. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013; ISBN 3-900051-07-01. [Google Scholar]
- Vujanić, G.M.; On Behalf of the International Society of Paediatric Oncology–Renal Tumour Study Group (SIOP–RTSG); Gessler, M.; Ooms, A.H.A.G.; Collini, P.; Coulomb-L’Hermine, A.; D’Hooghe, E.; De Krijger, R.R.; Perotti, D.; Pritchard-Jones, K.; et al. The UMBRELLA SIOP–RTSG 2016 Wilms tumour pathology and molecular biology protocol. Nat. Rev. Urol. 2018, 15, 693–701. [Google Scholar] [CrossRef] [Green Version]
- Vujanić, G.M.; Sandstedt, B.; Harms, D.; Kelsey, A.; Leuschner, I.; de Kraker, J.; SIOP Nephroblastoma Scientific Committee. Revised International Society of Paediatric Oncology working classification of renal tumors of childhood. Med. Pediatr. Oncol. 2002, 38, 79–82. [Google Scholar] [CrossRef]
- Pritchard-Jones, K.; Bergeron, C.; de Camargo, B.; van den Heuvel-Eibrink, M.M.; Acha, T.; Godzinski, J.; Oldenburger, F.; Boccon-Gibod, L.; Leuschner, I.; Vujanic, G.; et al. Omission of doxorubicin from the treatment of stage II–III, in-termediate-risk Wilms’ tumour (SIOP WT 2001): An open-label, non-inferiority, randomised controlled trial. Lancet 2015, 386, 1156–1164. [Google Scholar] [CrossRef] [Green Version]
- Dix, D.B.; Gratias, E.J.; Seibel, N.; Anderson, J.R.; Mullen, E.A.; Geller, J.I.; Khanna, G.; Kalapurakal, J.A.; Perlman, E.J.; Ehrlich, P.F.; et al. Omission of lung radiation in patients with stage IV favorable histology Wilms Tumor (FHWT) showing complete lung nodule response after chemotherapy: A report from Children’s Oncology Group study AREN. J. Clin. Oncol. 2015, 33, 10011. [Google Scholar] [CrossRef]
- Tournade, M.F.; Com-Nougue, C.; De Kraker, J.; Ludwig, R.; Rey, A.; Burgers, J.M.B.; Sandstedt, B.; Godzinski, J.; Carli, M.; Potter, R.; et al. Optimal duration of preoperative therapy in unilateral and non-metastatic Wilms’ tumor in children older than 6 months: Results of the Ninth International Society of Pediatric Oncology Wilms’ Tumor Trial and Study. J. Clin. Oncol. 2001, 19, 488–500. [Google Scholar] [CrossRef] [PubMed]
- Dávila Fajardo, R.; Oldenburger, E.; Rübe, C.; López-Yurda, M.; Pritchard-Jones, K.; Bergeron, C.; Graf, N.; van Grotel, M.; van Tinteren, H.; Saunders, D.; et al. Evaluation of boost irradiation in patients with intermediate-risk stage III Wilms tumour with positive lymph nodes only: Results from the SIOP-WT-2001 registry. Pediatr. Blood Cancer 2018, 65, e27085. [Google Scholar] [CrossRef] [PubMed]
- Tournade, M.F.; Com-Nougué, C.; Voûte, P.A.; Lemerle, J.; De Kraker, J.; Delemarre, J.F.; Burgers, M.; Habrand, J.L.; Moorman, C.G.; Burger, D. Results of the Sixth International Society of Pediatric Oncology Wilms’ Tumor Trial and Study: A risk-adapted therapeutic approach in Wilms’ tumor. J. Clin. Oncol. 1993, 11, 1014–1023. [Google Scholar] [CrossRef]
- Lemerle, J.; Voute, P.A.; Tournade, M.F.; Rodary, C.; Delemarre, J.F.; Sarrazin, D.; Burgers, J.M.; Sandstedt, B.; Mildenberger, H.; Carli, M. Effectiveness of preoperative chemotherapy in Wilms’ tumor: Results of an International Society of Paediatric Oncology (SIOP) clinical trial. J. Clin. Oncol. 1983, 1, 604–609. [Google Scholar] [CrossRef]
- Wong, K.F.; Reulen, R.C.; Winter, D.L.; Guha, J.; Fidler, M.M.; Kelly, J.; Lancashire, E.R.; Pritchard-Jones, K.; Jenkinson, H.C.; Sugden, E.; et al. Risk of Adverse Health and Social Outcomes Up to 50 Years After Wilms Tumor: The British Childhood Cancer Survivor Study. J. Clin. Oncol. 2016, 34, 1772–1779. [Google Scholar] [CrossRef]
- Holmqvist, A.S.; Olsen, J.H.; Andersen, K.K.; Licht, S.D.F.; Hjorth, L.; Garwicz, S.; Moëll, C.; Anderson, H.; Wesenberg, F.; Tryggvadottir, L.; et al. Adult Life after Childhood Cancer in Scandinavia: Diabetes mellitus following treatment for cancer in childhood. Eur. J. Cancer 2014, 50, 1169–1175. [Google Scholar] [CrossRef] [PubMed]
- van Waas, M.; Neggers, S.J.; Raat, H.; van Rij, C.M.; Pieters, R.; van den Heuvel-Eibrink, M.M. Abdominal radiotherapy: A major determinant of metabolic syndrome in nephroblastoma and neuroblastoma survivors. PLoS ONE 2012, 7, e52237. [Google Scholar] [CrossRef] [Green Version]
- Termuhlen, A.M.; Tersak, J.M.; Liu, Q.; Yasui, Y.; Stovall, M.; Weathers, R.; Deutsch, M.; Sklar, C.A.; Oeffinger, K.C.; Armstrong, G.; et al. Twenty-five year follow-up of childhood Wilms tumor: A report from the Childhood Cancer Survivor Study. Pediatr. Blood Cancer 2011, 57, 1210–1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, A.J.; Winter, D.L.; Pritchard-Jones, K.; Stiller, C.A.; Frobisher, C.; Lancashire, E.R.; Reulen, R.C.; Hawkins, M.M. Second primary neoplasms in survivors of Wilms’ tumour-A population-based cohort study from the British Childhood Cancer Survivor Study. Int. J. Cancer 2008, 122, 2085–2093. [Google Scholar] [CrossRef]
- Carli, M.; Frascella, E.; Tournade, M.F.; Kraker, J.D.; Rey, A.; Guzzinati, S.; Burgers, J.M.V.; Delemarre, J.F.; Masiero, L.; Simonato, L. Second malignant neoplasms in patients treated on SIOP Wilms tumour studies and trials 1, 2, 5, and 6. Med. Pediatr. Oncol. 1997, 29, 239–244. [Google Scholar] [CrossRef]
- Green, D.M.; Lange, J.M.; Qu, A.; Peterson, S.M.; Kalapurakal, J.A.; Stokes, D.C.; Grigoriev, Y.A.; Ba, J.R.T.; Norkool, P.; Friedman, D.L.; et al. Pulmonary disease after treatment for wilms tumor: A report from the national wilms tumor long-term follow-up study. Pediatr. Blood Cancer 2013, 60, 1721–1726. [Google Scholar] [CrossRef] [Green Version]
- Sasso, G.; Greco, N.; Murino, P.; Sasso, F.S. Late Toxicity in Wilms Tumor Patients Treated With Radiotherapy at 15 Years of Median Follow-up. J. Pediatr. Hematol. 2010, 32, e264–e267. [Google Scholar] [CrossRef]
- van Dijk, I.W.; Oldenburger, F.; Cardous-Ubbink, M.C.; Geenen, M.M.; Heinen, R.C.; de Kraker, J.; van Leeuwen, F.E.; van der Pal, H.J.; Caron, H.N.; Koning, C.C.; et al. Evaluation of late adverse events in long-term Wilms’ tumor survivors. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Paulino, A.C.; Wen, B.-C.; Brown, C.; Tannous, R.; Mayr, N.A.; Zhen, W.K.; Weidner, G.J.; Hussey, D.H. Late effects in children treated with radiation therapy for Wilms’ tumor. Int. J. Radiat. Oncol. 2000, 46, 1239–1246. [Google Scholar] [CrossRef]
- Shaw, N.J.; Eden, O.B.; Jenney, M.E.M.; Stevens, R.F.; Morris-Jones, P.H.; Craft, A.W.; Castillo, L. Pulmonary Function in Survivors of Wilms’ Tumor. Pediatr. Hematol. Oncol. 1991, 8, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Green, D.M.; Finklestein, J.Z.; Tefft, M.E.; Norkool, P. Diffuse interstitial pneumonia after pulmonary irradiation for metastatic Wilms’ tumor: A report from the National Wilms’ Tumor Study. Cancer 1989, 63, 450–453. [Google Scholar] [CrossRef]
- Green, D.M.; Grigoriev, Y.A.; Nan, B.; Takashima, J.R.; Norkool, P.A.; D’Angio, G.J.; Breslow, N.E. Congestive heart failure after treatment for Wilms’ tumor: A report from the National Wilms’ Tumor Study group. J. Clin. Oncol. 2001, 19, 1926–1934. [Google Scholar] [CrossRef]


{kind=link}
| RT | No RT | ||||
|---|---|---|---|---|---|
| N = 29 | N = 18 | ||||
| Flank/Abdomen | Flank/Abdomen/Lung | Total | |||
| N = 20 | N = 9 | N = 29 | |||
| Gender | Male | 9 | 2 | 11 | 10 |
| Female | 11 | 7 | 18 | 8 | |
| Tumour site | Right | 10 | 7 | 17 | 9 |
| Left | 10 | 2 | 12 | 9 | |
| Reason for local stage III | SM positive | 7 | 2 | 9 | 7 |
| LN positive | 6 | 4 | 10 | 9 | |
| SM and LN positive | 4 | 3 | 7 | 0 | |
| Tumour rupture | 1 | 0 | 1 | 1 | |
| Peritoneal implants | 1 | 0 | 1 | 0 | |
| SM positive and peritoneal implants | 1 | 0 | 1 | 0 | |
| NA | 0 | 0 | 0 | 1 | |
| Metastatic site | Lung only | 15 | 5 | 20 | 14 |
| Lung combined | 3 | 4 | 7 | 4 | |
| Liver/abdomen | 1 | 0 | 1 | 0 | |
| Other | 1 | 0 | 1 | 0 | |
| Postoperative chemotherapy regimen | AVD | 12 | 3 | 15 | 16 |
| AV-2 | 1 | 0 | 1 | 0 | |
| High-risk | 6 | 6 | 12 | 2 | |
| NA | 1 | 0 | 1 | 0 | |
| Metastatic status after preoperative chemotherapy and surgery | Metastases absent with chemotherapy alone | 9 | 1 | 10 | 10 |
| Completely excised | 3 | 2 | 5 | 2 | |
| Incompletely excised or multiple irresectable | 7 | 6 | 13 | 5 | |
| NA | 1 | 0 | 1 | 1 | |
| Recurrence status | Yes | 1 | 1 | 2 | 0 |
| No | 19 | 8 | 27 | 18 | |
| Collaborative group | GCBTTW | 0 | 0 | 0 | 1 |
| GPOH | 3 | 0 | 3 | 9 | |
| SFCE | 4 | 0 | 4 | 3 | |
| SIOP-NL | 9 | 2 | 11 | 4 | |
| CCLG | 4 | 7 | 11 | 1 | |
| Patient No | Age (Months) | Gender | Reason for Stage III | Metastasis CR at Week 6 | Metastasis CR at Week 10 (After CHT and Surgery) | Metastasis Surgically Removed | Postoperative CHT Schema | Abdominal RT Directed | RT Dose (Gy) Elective/Boost | RT Metastasis Directed | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 61 | F | SM and LN + | Yes | Yes | No | AVD | Yes | 14.4/10.8 | No | CR/Alive |
| 2 | 37 | F | SM + | No | No | No | AVD | Yes | 14.4 | No | CR/Alive |
| 3 | 26 | F | SM + | Yes | Yes | No | AV-2 | Yes | 14.4 | No | CR/Alive |
| 4 | 87 | M | SM and LN + | No | Yes | Yes | AVD | Yes | 16 | No | CR/Alive |
| 5 | 37 | M | SM and LN + | Yes | Yes | No | AVD | Yes | 14.4/10.8 | No | CR/Alive |
| 6 | 50 | F | LN + | No | No | No | High-risk | Yes | 14.4/10.8 | No | CR/Alive |
| 7 | 43 | M | SM + | No | No | No | High-risk | Yes | 14.4 | No | CR/Alive |
| 8 | 70 | F | LN + | Yes | Yes | No | AVD | Yes | 15 | No | CR/Alive |
| 9 | 77 | M | LN + | Yes | Yes | No | High-risk | Yes | 14.4/10.8 | Yes | CR/Alive |
| 10 | 28 | M | LN + | No | No | No | AVD | Yes | 14.4 | No | CR/Alive |
| 11 | 39 | M | Rupture | Yes | Yes | No | AVD | Yes | 14.4 | No | CR/Alive |
| 12 | 68 | M | Peritoneal implants | No | Yes | Yes | AVD | Yes | 21 | No | CR/Alive |
| 13 | 53 | M | SM + | Yes | Yes | No | AVD | Yes | 14.4 | No | CR/Alive |
| 14 | 28 | F | SM + | No | No | No | High-risk | Yes | 14.4 | No | CR/Alive |
| 15 | 36 | M | Peritoneal implants and SM + | No | No | Yes | High-risk | Yes | 19.5 | No | CR/Alive |
| 16 | 85 | M | SM + | No | Yes | Yes | High-risk | Yes | 20 | No | CR/Alive |
| 17 | 48 | F | LN + | No | No | No | High-risk | Yes | 14.4 | No | CR/Alive |
| 18 | 69 | F | LN + | No | No | No | AVD | Yes | 14.4 | Yes | CR/Alive |
| 19 | 44 | M | SM and LN + | No | Yes | Yes | High-risk | Yes | 15 | Yes | CR/Alive |
| 20 | 95 | F | SM and LN + | No | No | No | AVD | Yes | 14.4 | Yes | CR/Alive |
| 21 | 14 | F | LN + | No | No | No | High-risk | Yes | 15 | Yes | CR/Alive |
| 22 | 49 | F | SM and LN + | Yes | Yes | No | AVD | Yes | 14.4 | No | CR/Alive |
| 23 | 48 | F | LN + | No | No | No | High-risk | Yes | 14.4/7.5 | Yes | Relapse/Dead |
| 24 | 97 | F | SM + | No | No | No | AVD | Yes | 14.4/10.8 | Yes | CR/Alive |
| 25 | 41 | F | LN + | Yes | Yes | No | AVD | Yes | 14.4/10.8 | No | CR/Alive |
| 26 | 44 | F | SM + | No | NA | NA | NA | Yes | 21 | No | Relapse/Dead |
| 27 | 105 | F | SM + | No | Yes | Yes | High-risk | Yes | 15/6 | Yes | CR/Alive |
| 28 | 99 | F | LN + | Yes | Yes | No | AVD | Yes | 21 | No | CR/Alive |
| 29 | 97 | F | SM and LN + | No | No | No | High-risk | Yes | 14.4/10.8 | Yes | CR/Alive |
| 30 | 38 | F | LN + | Yes | Yes | No | AVD | No | - | No | CR/Alive |
| 31 | 48 | F | SM + | Yes | Yes | No | AVD | No | - | No | CR/Alive |
| 32 | 43 | F | SM + | No | NA | NA | AVD | No | - | No | CR/Alive |
| 33 | 75 | M | LN + | Yes | Yes | No | AVD | No | - | No | CR/Alive |
| 34 | 23 | M | SM + | Yes | Yes | No | AVD | No | - | No | CR/Alive |
| 35 | 49 | M | LN + | No | No | No | High-risk | No | - | No | CR/Alive |
| 36 | 87 | M | LN + | No | No | No | AVD | No | - | No | CR/Alive |
| 37 | 35 | M | LN + | No | No | No | High-risk | No | - | No | CR/Alive |
| 38 | 68 | F | SM + | No | No | No | AVD | No | - | No | CR/Alive |
| 39 | 67 | M | LN + | Yes | Yes | No | AVD | No | - | No | CR/Alive |
| 40 | 40 | M | LN + | Yes | Yes | No | AVD | No | - | No | CR/Alive |
| 41 | 144 | M | LN + | No | Yes | Yes | AVD | No | - | No | CR/Alive |
| 42 | 52 | F | LN + | No | No | No | AVD | No | - | No | CR/Alive |
| 43 | 75 | M | LN + | Yes | Yes | No | AVD | No | - | No | CR/Alive |
| 44 | 53 | F | SM + | No | Yes | No | AVD | No | - | No | CR/Alive |
| 45 | 72 | M | SM + | Yes | Yes | No | AVD | No | - | No | CR/Alive |
| 46 | 50 | F | Rupture | No | No | No | AVD | No | - | No | CR/Alive |
| 47 | 59 | F | SM + | No | Yes | No | AVD | No | - | No | CR/Alive |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dávila Fajardo, R.; Furtwängler, R.; van Grotel, M.; van Tinteren, H.; Pasqualini, C.; Pritchard-Jones, K.; Al-Saadi, R.; de Camargo, B.; Ramírez Villar, G.L.; Graf, N.; et al. Outcome of Stage IV Completely Necrotic Wilms Tumour and Local Stage III Treated According to the SIOP 2001 Protocol. Cancers 2021, 13, 976. https://doi.org/10.3390/cancers13050976
Dávila Fajardo R, Furtwängler R, van Grotel M, van Tinteren H, Pasqualini C, Pritchard-Jones K, Al-Saadi R, de Camargo B, Ramírez Villar GL, Graf N, et al. Outcome of Stage IV Completely Necrotic Wilms Tumour and Local Stage III Treated According to the SIOP 2001 Protocol. Cancers. 2021; 13(5):976. https://doi.org/10.3390/cancers13050976
Chicago/Turabian StyleDávila Fajardo, Raquel, Rhoikos Furtwängler, Martine van Grotel, Harm van Tinteren, Claudia Pasqualini, Kathy Pritchard-Jones, Reem Al-Saadi, Beatriz de Camargo, Gema L. Ramírez Villar, Norbert Graf, and et al. 2021. "Outcome of Stage IV Completely Necrotic Wilms Tumour and Local Stage III Treated According to the SIOP 2001 Protocol" Cancers 13, no. 5: 976. https://doi.org/10.3390/cancers13050976