
Delayed Surgery after Neoadjuvant Treatment for Rectal Cancer Does Not Lead to Impaired Quality of Life, Worry for Cancer, or Regret

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials & Methods
2.1. Study Design
2.2. Patient Selection
2.3. Questionnaires
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics & Non-Responder Analysis
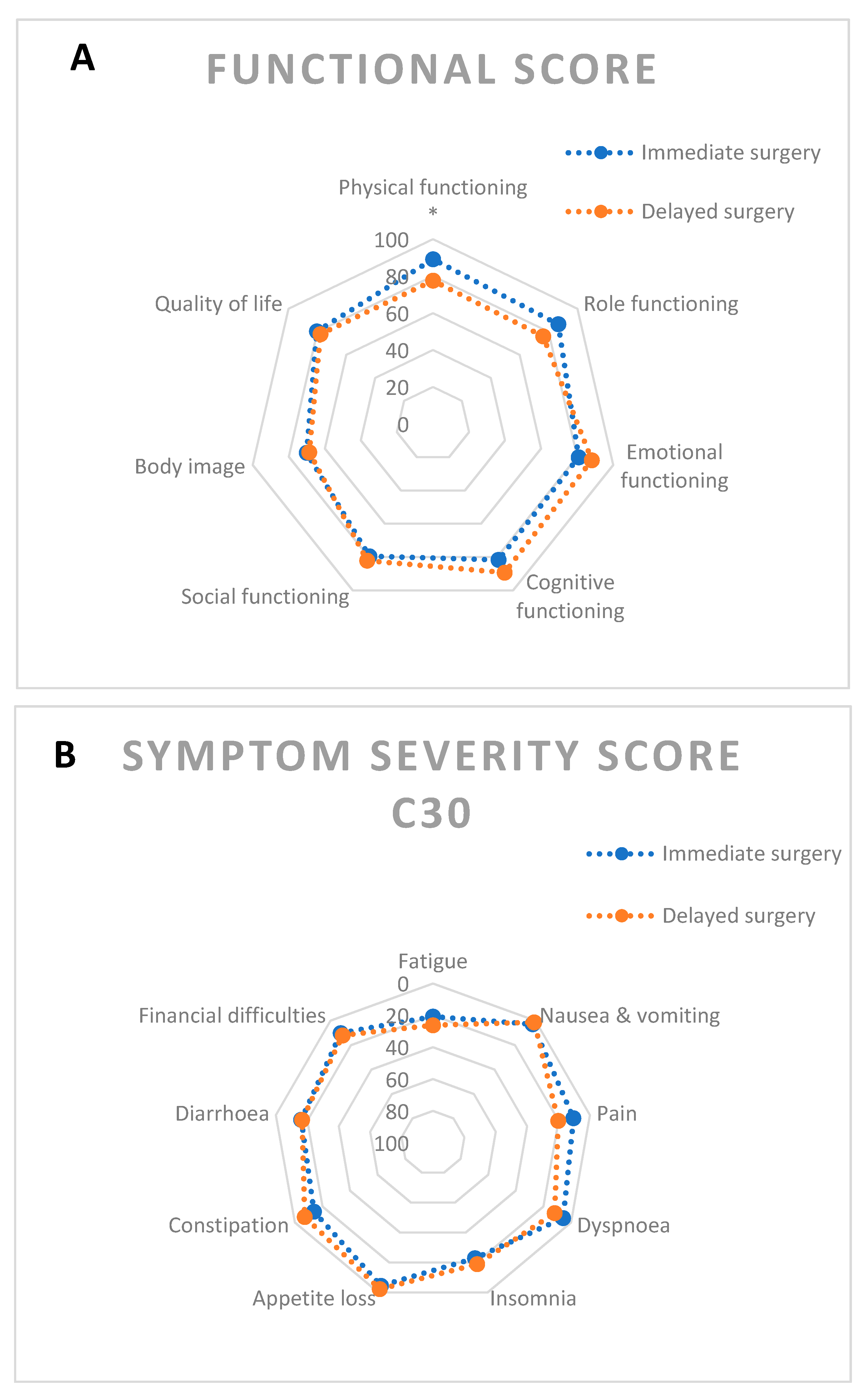
3.2. QLQC30 & CR29
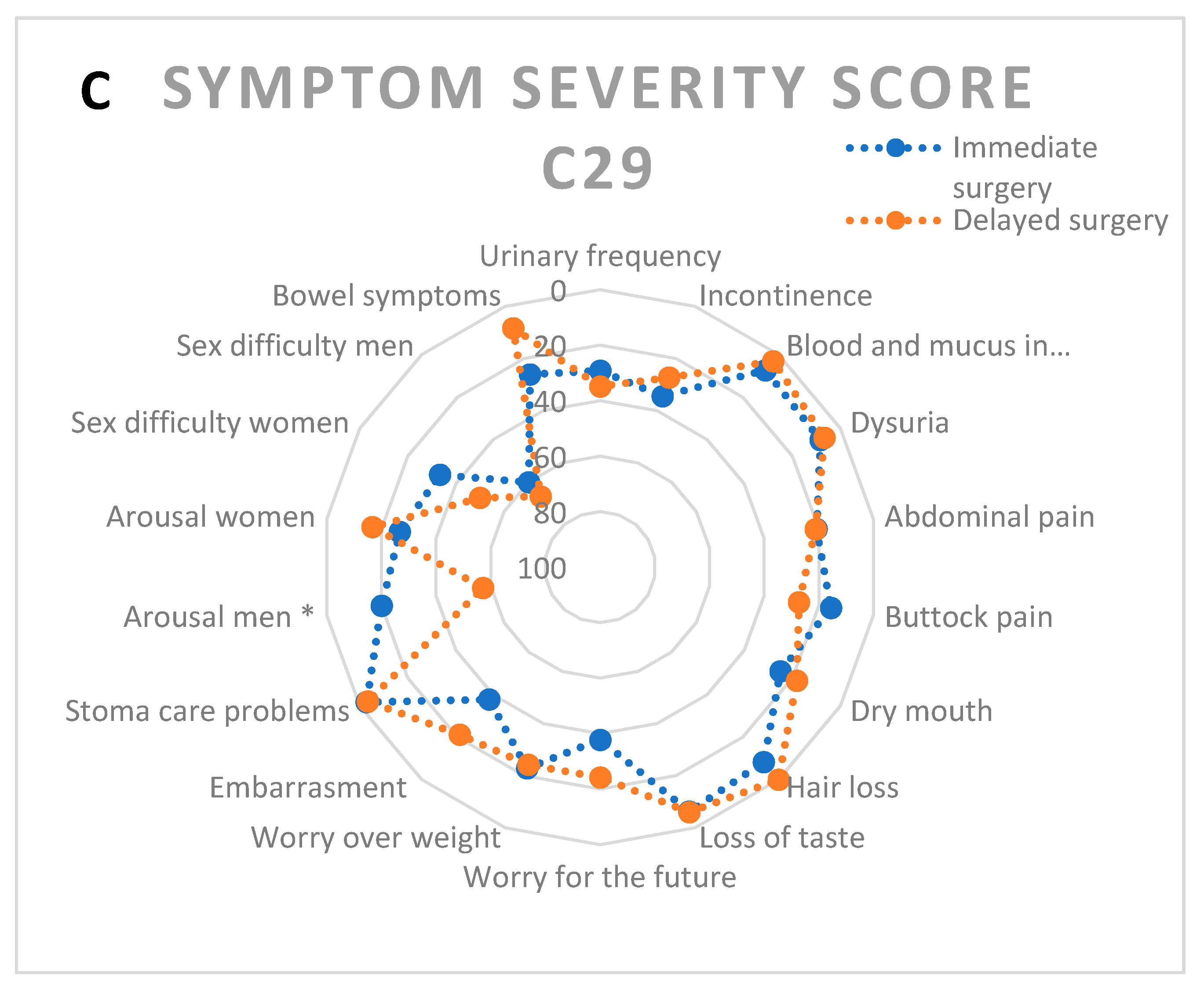
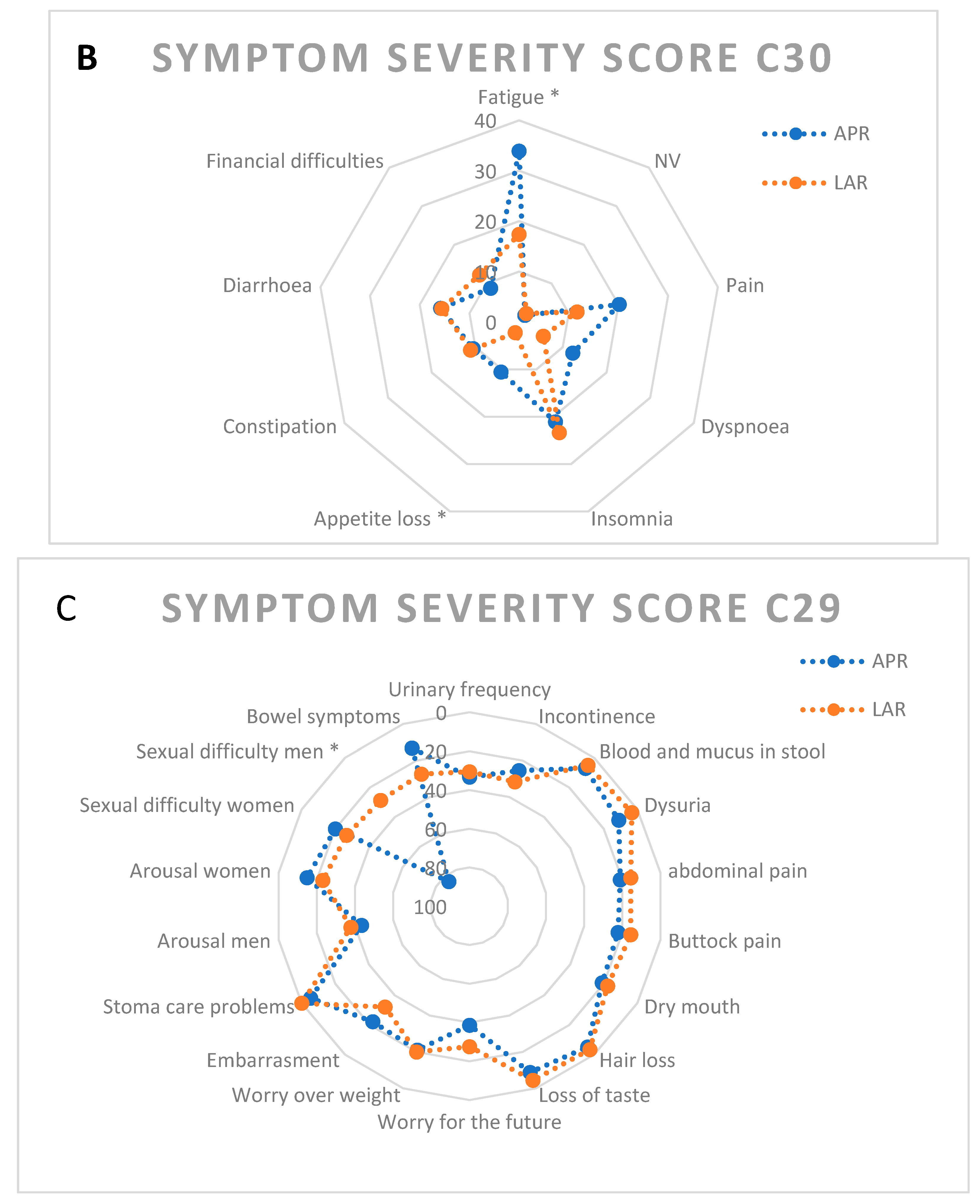
3.3. Known Groups Comparison: APR vs. LAR
3.4. Cancer Worry Scale
3.5. Decision Regret Scale
3.6. Factor Analysis and Reliability
4. Discussion
5. Conclusion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van der Valk, M.J.M.; Hilling, D.E.; Bastiaannet, E.; Meershoek-Klein Kranenbarg, E.; Beets, G.L.; Figueiredo, N.L.; Habr-Gama, A.; Perez, R.O.; Renehan, A.G.; van de Velde, C.J.H.; et al. Long-Term Outcomes of Clinical Complete Responders after Neoadjuvant Treatment for Rectal Cancer in the International Watch & Wait Database (IWWD): An International Multicentre Registry Study. Lancet 2018, 391, 2537–2545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dattani, M.; Heald, R.J.; Goussous, G.; Broadhurst, J.; São Julião, G.P.; Habr-Gama, A.; Oliva Perez, R.; Moran, B.J. Oncological and Survival Outcomes in Watch and Wait Patients with a Clinical Complete Response after Neoadjuvant Chemoradiotherapy for Rectal Cancer a Systematic Review and Pooled Analysis. Ann. Surg. 2018, 268, 955–967. [Google Scholar] [CrossRef] [PubMed]
- Perez, R.O.; Habr-Gama, A.; Pereira, G.V.; Lynn, P.B.; Alves, P.A.; Proscurshim, I.; Rawet, V.; Gama-Rodrigues, J. Role of Biopsies in Patients with Residual Rectal Cancer Following Neoadjuvant Chemoradiation after Downsizing: Can They Rule out Persisting Cancer? Colorectal Dis. 2012, 14, 714–720. [Google Scholar] [CrossRef]
- Blazic, I.M.; Campbell, N.M.; Gollub, M.J. MRI for Evaluation of Treatment Response in Rectal Cancer. Br. J. Radiol. 2016, 89, 20150964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, F.M.; Wiland, H.; Mace, A.; Pai, R.K.; Kalady, M.F. Clinical Criteria Underestimate Complete Pathological Response in Rectal Cancer Treated with Neoadjuvant Chemoradiotherapy. Dis. Colon Rectum 2014, 57, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Beets-Tan, R.G.H.; Beets, G.L. MRI for Assessing and Predicting Response to Neoadjuvant Treatment in Rectal Cancer. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 480–488. [Google Scholar] [CrossRef]
- Hupkens, B.J.P.; Maas, M.; Martens, M.H.; van der Sande, M.E.; Lambregts, D.M.J.; Breukink, S.O.; Melenhorst, J.; Houwers, J.B.; Hoff, C.; Sosef, M.N.; et al. Organ Preservation in Rectal Cancer After Chemoradiation: Should We Extend the Observation Period in Patients with a Clinical Near-Complete Response? Ann. Surg. Oncol. 2018, 25, 197–203. [Google Scholar] [CrossRef]
- Habr-Gama, A.; São Julião, G.P.; Fernandez, L.M.; Vailati, B.B.; Andrade, A.; Araújo, S.E.A.; Gama-Rodrigues, J.; Perez, R.O. Achieving a Complete Clinical Response after Neoadjuvant Chemoradiation That Does Not Require Surgical Resection: It May Take Longer Than You Think! Dis. Colon Rectum 2019, 62, 802–808. [Google Scholar] [CrossRef] [PubMed]
- Kong, J.C.; Guerra, G.R.; Warrier, S.K.; Ramsay, R.G.; Heriot, A.G. Outcome and Salvage Surgery Following “Watch and Wait” for Rectal Cancer after Neoadjuvant Therapy. Dis. Colon Rectum 2017, 60, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, L.M.; Figueiredo, N.L.; Habr-Gama, A.; São Julião, G.P.; Vieira, P.; Vailati, B.B.; Nasir, I.; Parés, O.; Santiago, I.; Castillo-Martin, M.; et al. Salvage Surgery with Organ Preservation for Patients with Local Regrowth after Watch and Wait: Is It Still Possible? Dis. Colon Rectum 2020, 63, 1053–1062. [Google Scholar] [CrossRef]
- Habr-Gama, A.; Perez, R.O. Non-Operative Management of Rectal Cancer after Neoadjuvant Chemoradiation. Br. J. Surg. 2009, 96, 125–127. [Google Scholar] [CrossRef]
- Pascual-Russo, A.; Milito, D.; Facio, L.; Furia, M.; Forestier, V.; Iseas, S.; Méndez, G.; Coraglio, M.; Lumi, C.M.; Masciangioli, G.; et al. Better Quality of Life and Reduced Fecal Incontinence in Rectal Cancer Patients with the Watch-and-Wait Follow-up Strategy. Rev. Gastroenterol. Mex. 2020. [Google Scholar] [CrossRef]
- Hupkens, B.J.P.; Martens, M.H.; Stoot, J.H.; Berbee, M.; Melenhorst, J.; Beets-Tan, R.G.; Beets, G.L.; Breukink, S.O. Quality of Life in Rectal Cancer Patients after Chemoradiation: Watch-and-Wait Policy versus Standard Resection—A Matched-Controlled Study. Dis. Colon Rectum 2017, 60, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Vivar, C.G.; Canga, N.; Canga, A.D.; Arantzamendi, M. The Psychosocial Impact of Recurrence on Cancer Survivors and Family Members: A Narrative Review. J. Adv. Nurs. 2009, 65, 724–736. [Google Scholar] [CrossRef]
- Taylor, C.; Richardson, A.; Cowley, S. Surviving Cancer Treatment: An Investigation of the Experience of Fear about, and Monitoring for, Recurrence in Patients Following Treatment for Colorectal Cancer. Eur. J. Oncol. Nurs. 2011, 15, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Stiggelbout, A.M.; Kunneman, M.; Baas-Thijssen, M.C.M.; Neijenhuis, P.A.; Loor, A.K.; Jägers, S.; Vree, R.; Marijnen, C.A.M.; Pieterse, A.H. The EORTC QLQ-CR29 Quality of Life Questionnaire for Colorectal Cancer: Validation of the Dutch Version. Qual. Life Res. 2016, 25, 1853–1858. [Google Scholar] [CrossRef] [Green Version]
- Custers, J.A.E.; Kwakkenbos, L.; van de Wal, M.; Prins, J.B.; Thewes, B. Re-Validation and Screening Capacity of the 6-Item Version of the Cancer Worry Scale. Psycho-Oncology 2018, 27, 2609–2615. [Google Scholar] [CrossRef]
- Brehaut, J.C.; O’connor, A.M.; Wood, T.J.; Hack, T.F.; Siminoff, L.; Gordon, E.; Feldman-Stewart, D. ARTICLE Validation of a Decision Regret Scale. Med. Decis. Mak. 2003, 23, 281–292. [Google Scholar] [CrossRef]
- Neuman, H.B.; Schrag, D.; Cabral, C.; Weiser, M.R.; Paty, P.B.; Guillem, J.G.; Minsky, B.D.; Wong, W.D.; Temple, L.K. Can Differences in Bowel Function after Surgery for Rectal Cancer Be Identified by the European Organization for Research and Treatment of Cancer Quality of Life Instrument? Ann. Surg. Oncol. 2007, 14, 1727–1734. [Google Scholar] [CrossRef]
- De Winter, J.C.F.; Dodou, D.; Wieringa, P.A. Exploratory Factor Analysis with Small Sample Sizes. Multivar. Behav. Res. 2009, 44, 147–181. [Google Scholar] [CrossRef] [PubMed]
- Russell, M.M.; Ganz, P.A.; Lopa, S.; Yothers, G.; Ko, C.Y.; Arora, A.; Atkins, J.N.; Bahary, N.; Soori, G.S.; Robertson, J.M.; et al. Comparative Effectiveness of Sphincter-Sparing Surgery versus Abdominoperineal Resection in Rectal Cancer. Ann. Surg. 2015, 261, 144–148. [Google Scholar] [CrossRef] [Green Version]
- Näsvall, P.; Dahlstrand, U.; Löwenmark, T.; Rutegård, J.; Gunnarsson, U.; Strigård, K. Quality of Life in Patients with a Permanent Stoma after Rectal Cancer Surgery. Qual. Life Res. 2017, 26, 55–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nolte, S.; Liegl, G.; Petersen, M.A.; Aaronson, N.K.; Costantini, A.; Fayers, P.M.; Groenvold, M.; Holzner, B.; Johnson, C.D.; Kemmler, G.; et al. General Population Normative Data for the EORTC QLQ-C30 Health-Related Quality of Life Questionnaire Based on 15,386 Persons across 13 European Countries, Canada and the Unites States. Eur. J. Cancer 2019, 107, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Giandomenico, F.; Gavaruzzi, T.; Lotto, L.; del Bianco, P.; Barina, A.; Perin, A.; Pucciarelli, S. Quality of Life after Surgery for Rectal Cancer: A Systematic Review of Comparisons with the General Population. Expert Rev. Gastroenterol. Hepatol. 2015, 9, 1227–1242. [Google Scholar] [CrossRef] [PubMed]
- Gosselink, M.P.; Busschbach, J.J.; Dijkhuis, C.M.; Stassen, L.P.; Hop, W.C.; Schouten, W.R. Quality of Life after Total Mesorectal Excision for Rectal Cancer. Colorectal Dis. 2006, 8, 15–22. [Google Scholar] [CrossRef]
- Salsman, J.M.; Segerstrom, S.C.; Brechting, E.H.; Carlson, C.R.; Andrykowski, M.A. Posttraumatic Growth and PTSD Symptomatology among Colorectal Cancer Survivors: A 3-Month Longitudinal Examination of Cognitive Processing. Psycho-Oncology 2009, 18, 30–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Custers, J.A.E.; Gielissen, M.F.M.; Janssen, S.H.V.; de Wilt, J.H.W.; Prins, J.B. Fear of Cancer Recurrence in Colorectal Cancer Survivors. Support. Care Cancer 2016, 24, 555–562. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Neuman, H.B.; Bennett, A.V.; Polskin, L.; Phang, P.T.; Wong, W.D.; Temple, L.K. Patient Expectations of Functional Outcomes after Rectal Cancer Surgery: A Qualitative Study. Dis. Colon Rectum 2014, 57, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Perwitasari, D.A.; Atthobari, J.; Dwiprahasto, I.; Hakimi, M.; Gelderblom, H.; Putter, H.; Nortier, J.W.R.; Guchelaar, H.J.; Kaptein, A.A. Translation and Validation of EORTC QLQ-C30 into Indonesian Version for Cancer Patients in Indonesia. Jpn. J. Clin. Oncol. 2011, 41, 519–529. [Google Scholar] [CrossRef] [Green Version]
- Engel, J.; Kerr, J.; Schlesinger-Raab, A.; Eckel, R.; Sauer, H.; Hölzel, D. Quality of Life in Rectal Cancer Patients. Ann. Surg. 2003, 238, 203–213. [Google Scholar] [CrossRef]
- Smith, T.; Stein, K.D.; Mehta, C.C.; Kaw, C.; Kepner, J.L.; Buskirk, T.; Stafford, J.; Baker, F. The Rationale, Design, and Implementation of the American Cancer Society’s Studies of Cancer Survivors. Cancer 2007, 109, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.J.; Fraze, T.K.; Hornik, R.C. Response Rates to a Mailed Survey of a Representative Sample of Cancer Patients Randomly Drawn from the Pennsylvania Cancer Registry: A Randomized Trial of Incentive and Length Effects. BMC Med. Res. Methodol. 2010, 10, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Immediate Surgery N = 33 | Delayed Surgery N = 18 | p | |||
|---|---|---|---|---|---|
| N (%) | Mean % | N (%) | Mean | ||
| Age | 63.9 | 61.2 | 0.33 | ||
| Sex | 0.57 | ||||
| M | 17 (51.5%) | 11 (61.1%) | |||
| F | 16 (48.5%) | 7 (38.9%) | |||
| ASAscore | 0.74 | ||||
| 1 | 11 (33.3%) | 7 (38.9%) | |||
| 2 | 20 (60.6%) | 9 (50.0%) | |||
| 3 | 2 (6.1%) | 2 (11.1%) | |||
| cT | 0.54 | ||||
| 3 | 30 (90.9%) | 17 (100%) | |||
| 4 | 3 (9.1%) | 0 (0%) | |||
| cN | 0.04 | ||||
| 0 | 1 (3.0%) | 4 (22.2%) | |||
| 1 | 9 (27.3%) | 6 (33.3%) | |||
| 2 | 23 (69.7%) | 8 (44.4%) | |||
| CRTx interrupted | 0.23 | ||||
| 0 | 30 (90.9%) | 14 (77.8%) | |||
| 1 | 3 (9.1%) | 4 (22.2%) | |||
| Endoscopic distance (cm) | 10 | 6 | 0.03 | ||
| Time to surgery (weeks) | 15 | 35 | <0.01 | ||
| Type of operation | 0.02 | ||||
| LAR | 24 (72.7%) | 7 (38.9%) | |||
| APR | 9 (27.30%) | 11 (61.1%) | |||
| Stoma-free survival | 0.02 | ||||
| no stoma | 21 (63.6%) | 5 (27.8%) | |||
| stoma in situ | 12 (36.4%) | 13 (72.2%) | |||
| Laparoscopy | 0.13 | ||||
| no | 8 (24.2%) | 1 (5.6%) | |||
| yes | 25 (75.8%) | 17 (94.4%) | |||
| Conversion | 0.53 | ||||
| no | 28 (84.8%) | 17 (94.4%) | |||
| yes | 4 (12.1%) | 1 (5.6%) | |||
| unknown | 1 (3.1%) | 0 (0%) | |||
| Readmission | 0.23 | ||||
| no | 23 (76.7%) | 17 (94.4%) | |||
| yes | 7 (23.3%) | 1 (5.6%) | |||
| Distant relapse | 0.46 | ||||
| no | 26 (78.8%) | 16 (88.9%) | |||
| yes | 7 (21.2%) | 2 (11.1%) | |||
| Follow up (months) | 35 | 25 | 0.07 | ||
| Immediate surgery | Delayed surgery | |||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| CWS | 14.00 | 9.12 | 10.79 | 7.91 |
| Decision Regret Scale Score (n = 16) | ||
|---|---|---|
| Item No. | Question | Score (%) |
| 1 | It was the right decision | 12.5 |
| 2 | I regret the choice that was made | 10.7 |
| 3 | I would go for the same choice if I had to do it over again | 14.3 |
| 4 | The choice did me a lot of harm | 14.3 |
| 5 | The decision was a wise one | 16.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, V.M.; Meuzelaar, R.R.; Schoenaker, Y.; de Groot, J.-W.; de Boer, E.; Reerink, O.; de Vos tot Nederveen Cappel, W.; Beets, G.L.; van Westreenen, H.L. Delayed Surgery after Neoadjuvant Treatment for Rectal Cancer Does Not Lead to Impaired Quality of Life, Worry for Cancer, or Regret. Cancers 2021, 13, 742. https://doi.org/10.3390/cancers13040742
Meyer VM, Meuzelaar RR, Schoenaker Y, de Groot J-W, de Boer E, Reerink O, de Vos tot Nederveen Cappel W, Beets GL, van Westreenen HL. Delayed Surgery after Neoadjuvant Treatment for Rectal Cancer Does Not Lead to Impaired Quality of Life, Worry for Cancer, or Regret. Cancers. 2021; 13(4):742. https://doi.org/10.3390/cancers13040742
Chicago/Turabian StyleMeyer, Vincent Maurice, Richtje R Meuzelaar, Yvonne Schoenaker, Jan-Willem de Groot, Edwin de Boer, Onno Reerink, Wouter de Vos tot Nederveen Cappel, Geerard L Beets, and Henderik L van Westreenen. 2021. "Delayed Surgery after Neoadjuvant Treatment for Rectal Cancer Does Not Lead to Impaired Quality of Life, Worry for Cancer, or Regret" Cancers 13, no. 4: 742. https://doi.org/10.3390/cancers13040742