The Role of Neoadjuvant Chemotherapy in Repeat Local Treatment of Recurrent Colorectal Liver Metastases: A Systematic Review and Meta-Analysis

 , , , , ,
, , , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategies
2.2. Study Selection
2.3. Data Extraction
2.4. Data Analysis
2.5. Guidelines
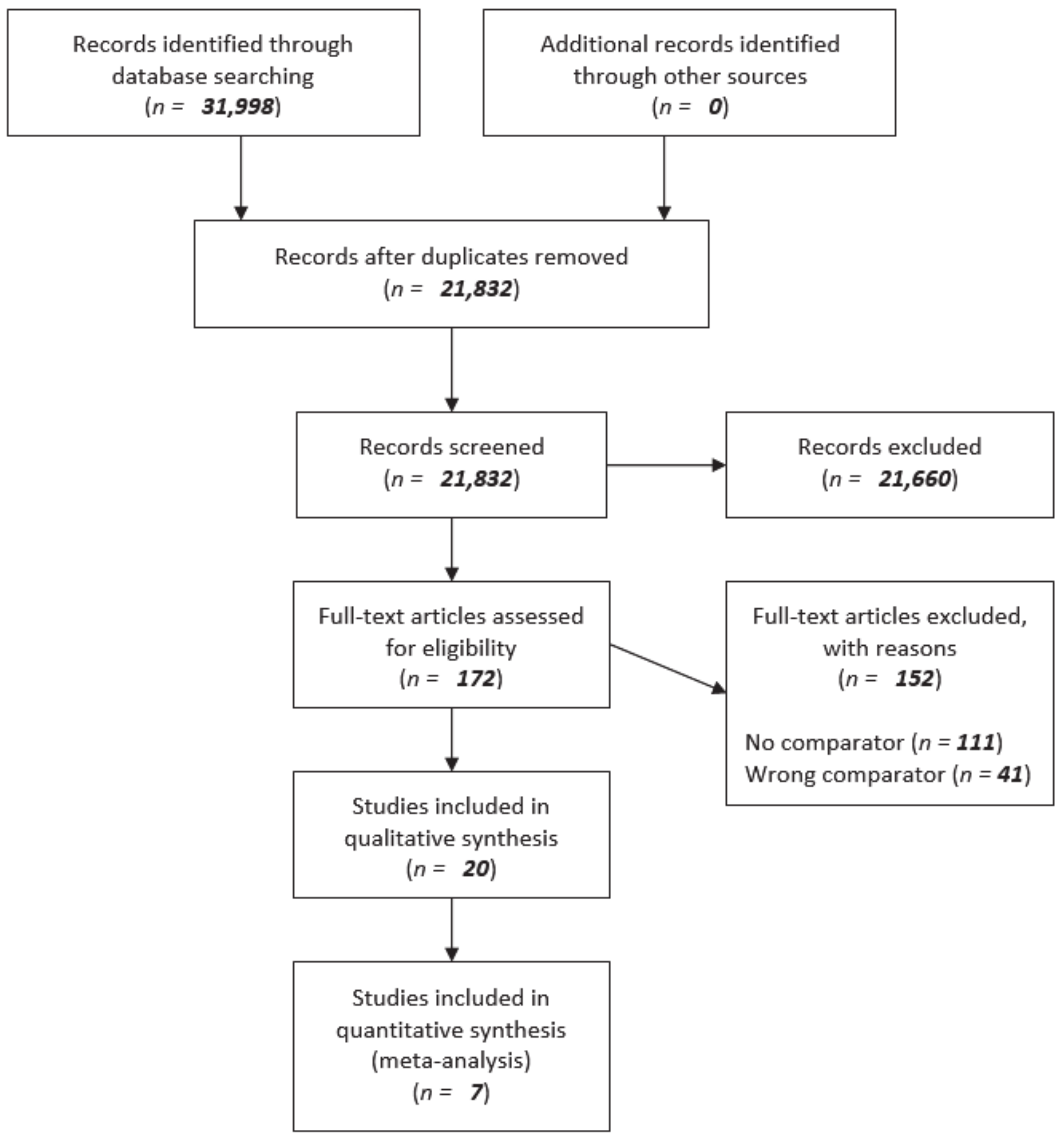
3. Results
3.1. Study Characteristics
3.2. Treatment Characteristics
3.3. Level of Evidence
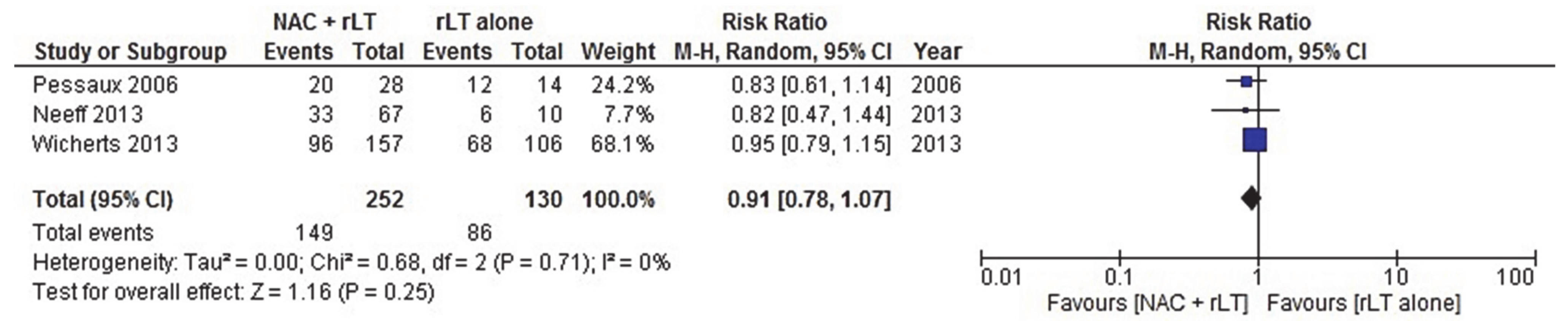
3.4. Overall Survival (Critical Endpoint) and Disease-Free Survival (Important Endpoint)
3.5. Complications, Quality of Life, and Cost-Effectiveness (Important Endpoints)
3.6. Guidelines
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 5-FU | 5-FluoroUracil |
| AGREE | Appraisal of Guidelines for Research and Evaluation |
| CEA | CarcinoEmbryonic Antigen |
| COLLISION | COLorectal LIver metastases: Surgery vs. thermal ablation |
| CI | Confidence Interval |
| CRC | Colorectal Liver Cancer |
| CRLM | Colorectal Liver Metastasis |
| CRS | Clinical Risk Score |
| DFS | Disease-Free Survival |
| EORTC | European Organization for Research and Treatment of Cancer |
| FOLFIRI | FOLinic acid, 5-Fluorouracil and IRInotecan |
| FOLFOX | FOLinic acid, 5-Fluorouracil and Oxaliplatin |
| FUFOL | 5-FluoroUracil and FOLinic acid |
| HR | Hazard Ratio |
| IKNL | The Dutch Comprehensive Cancer Centre; Integraal Kankercentrum Nederland |
| JCOG | Japan Clinical Oncology Group |
| JSCCR | Japanese Society for Cancer of the Colon and Rectum |
| MSI | MicroSatellite Instability |
| MWA | Microwave Ablation |
| NAC | NeoAdjuvant Chemotherapy |
| NICE | UK National Institute for Health and Care Excellence |
| OS | Overall Survival |
| PFS | Progression-Free Survival |
| PICO | Patients, Interventions, Comparisons, Outcomes |
| PST | Potential Salvage Therapy |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| QoL | Quality of Life |
| RCT | Randomized Controlled Trial |
| RFA | RadioFrequency Ablation |
| rLT | Repeat Local Treatment |
| RR | Risk Ratio |
| SD | Standard Deviation |
Appendix A. Search Strategies
| Search | Query | Results |
| #6 | #5 NOT “Case Reports” [Publication Type] | 8683 |
| #5 | #4 NOT (“Animals”[Mesh] NOT “Humans”[Mesh]) | 10,450 |
| #4 | #1 AND (#2 OR #3) | 10,856 |
| #3 | “Neoadjuvant Therapy”[Mesh] OR “neoadjuvan*”[tiab] OR “conversion*”[tiab] OR “inducti*”[tiab] OR “chemotherap*”[tiab] | 1,162,750 |
| #2 | “repeat*”[tiab] OR “repetition*”[tiab] OR “renew*”[tiab] OR “third”[tiab] OR “second”[tiab] OR “fourth”[tiab] OR “fifth”[tiab] OR “addition*”[tiab] OR “reresection*”[tiab] OR “rehepatectom*”[tiab] OR “re resection*”[tiab] OR “re hepatectom*”[tiab] | 4,439,761 |
| #1 | (“Intestine, Large”[Mesh:NoExp] OR “Colon”[Mesh] OR “Rectum”[Mesh] OR “Colorectal Neoplasms”[Mesh] OR “colon*”[tiab] OR “colorect*”[tiab] OR “rectal*”[tiab] OR “rectum”[tiab]) AND (“Liver Neoplasms”[Mesh] OR “Liver”[Mesh] OR “Hepatectomy”[Mesh] OR “liver*”[tiab] OR “hepatot*”[tiab] OR “hepate*”[tiab] OR “hepati*”[tiab]) AND (“Neoplasm Metastasis”[Mesh] OR “metasta*”[tiab] OR “seeding*”[tiab]) | 23,360 |
| No. | Query | Results |
| #6 | #5 NOT (‘case report’/exp OR ‘conference abstract’/it) | 11,270 |
| #5 | #4 NOT ([animals]/lim NOT [humans]/lim) | 20,018 |
| #4 | #1 AND (#2 OR #3) | 20,950 |
| #3 | ‘neoadjuvant chemotherapy’/exp OR neoadjuvan*:ti,ab,kw OR conversion*:ti,ab,kw OR inducti*:ti,ab,kw OR chemotherap*:ti,ab,kw | 1,602,822 |
| #2 | ‘repeat procedure’/exp OR repeat*:ti,ab,kw OR repetition*:ti,ab,kw OR renew*:ti,ab,kw OR third:ti,ab,kw OR second:ti,ab,kw OR fourth:ti,ab,kw OR fifth:ti,ab,kw OR addition*:ti,ab,kw OR reresection*:ti,ab,kw OR rehepatectom*:ti,ab,kw OR ‘re resection*’:ti,ab,kw OR ‘re hepatectom*’:ti,ab,kw | 5,719,489 |
| #1 | (‘large intestine’/de OR ‘colon’/exp OR ‘large intestine epithelium’/exp OR ‘large intestine mucosa’/exp OR ‘large intestine muscle’/exp OR ‘large intestine wall’/exp OR ‘rectum’/exp OR ‘large intestine tumor’/de OR ‘colon tumor’/exp OR ‘large intestine cancer’/de OR ‘colon cancer’/exp OR ‘rectum cancer’/exp OR ‘rectum tumor’/exp OR colon*:ti,ab,kw OR colorect*:ti,ab,kw OR rectal*:ti,ab,kw OR rectum:ti,ab,kw) AND (‘liver tumor’/exp OR ‘liver’/exp OR ‘liver resection’/exp OR liver*:ti,ab,kw OR hepatot*:ti,ab,kw OR hepate*:ti,ab,kw OR hepati*:ti,ab,kw) AND (‘metastasis’/exp OR ‘seeding’/exp OR metasta*:ti,ab,kw OR seeding*:ti,ab,kw) | 43,885 |
| Set | Query | Results |
| #3 | #2 AND #1 | 12,045 |
| #2 | TOPIC: (“repeat*” OR “repetition*” OR “renew*” OR “third” OR “second” OR “fourth” OR “fifth” OR “addition*” OR “reresection*” OR “rehepatectom*” OR “re resection*” OR “re hepatectom*” OR “neoadjuvan*” OR “conversion*” OR “inducti*” OR “chemotherap*”) | 8,375,170 |
| #1 | TOPIC: ((“colon*” OR “colorect*” OR “rectal*” OR “rectum”) AND (“liver*” OR “hepatot*” OR “hepate*” OR “hepati*”) AND (“metasta*” OR “seeding*”)) | 24,915 |
Appendix B. AGREE-II Instrument

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | Domain Score | |
|---|---|---|---|---|---|---|---|---|---|
| IKNL 2019 | 4 | 4 | 5 | 6 | 6 | 6 | 5 | 5 | 73.2 |
| JSCCR 2019 | 5 | 3 | 5 | 6 | 5 | 6 | 3 | 2 | 62.5 |
| NICE 2009 | 7 | 7 | 7 | 6 | 7 | 7 | 6 | 5 | 92.9 |
References
- WHO. Estimated Age-Standardized Incidence Rates (World) in 2018, All Cancers, Both Sexes, All Ages. Available online: http://gco.iarc.fr/today/online-analysis-map (accessed on 29 October 2020).
- Manfredi, S.; Lepage, C.; Hatem, C.; Coatmeur, O.; Faivre, J.; Bouvier, A.M. Epidemiology and management of liver metastases from colorectal cancer. Ann. Surg. 2006, 244, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Scheele, J.; Stangl, R.; Altendorf-Hofmann, A. Hepatic metastases from colorectal carcinoma: impact of surgical resection on the natural history. Br. J. Surg. 1990, 77, 1241–1246. [Google Scholar] [CrossRef]
- Leporrier, J.; Maurel, J.; Chiche, L.; Bara, S.; Segol, P.; Launoy, G. A population-based study of the incidence, management and prognosis of hepatic metastases from colorectal cancer. Br. J. Surg. 2006, 93, 465–474. [Google Scholar] [CrossRef]
- Engstrand, J.; Nilsson, H.; Stromberg, C.; Jonas, E.; Freedman, J. Colorectal cancer liver metastases - a population-based study on incidence, management and survival. BMC Cancer 2018, 18, 78. [Google Scholar] [CrossRef] [PubMed]
- Hackl, C.; Neumann, P.; Gerken, M.; Loss, M.; Klinkhammer-Schalke, M.; Schlitt, H.J. Treatment of colorectal liver metastases in Germany: A ten-year population-based analysis of 5772 cases of primary colorectal adenocarcinoma. BMC Cancer 2014, 14. [Google Scholar] [CrossRef] [Green Version]
- Guideline. Orde van Medische Specialisten en de Landelijke werkgroep Gastrointestinale tumoren van de Vereniging van Integrale Kanker Centra (VIKC): Diagnostiek en behandeling van colorectale levermetastasen. Available online: https://www.oncoline.nl/uploaded/docs/colorectale%20levermet/Levermetastasen.pdf (accessed on 29 October 2020).
- Stangl, R.; Altendorf-Hofmann, A.; Charnley, R.M.; Scheele, J. Factors influencing the natural history of colorectal liver metastases. Lancet 1994, 343, 1405–1410. [Google Scholar] [CrossRef]
- Wagner, J.S.; Adson, M.A.; Van Heerden, J.A.; Adson, M.H.; Ilstrup, D.M. The natural history of hepatic metastases from colorectal cancer. A comparison with resective treatment. Ann. Surg. 1984, 199, 502–508. [Google Scholar] [CrossRef]
- Yang, Q.; Liao, F.; Huang, Y.; Jiang, C.; Liu, S.; He, W.; Kong, P.; Zhang, B.; Xia, L. Longterm effects of palliative local treatment of incurable metastatic lesions in colorectal cancer patients. Oncotarget 2016, 7, 21034–21045. [Google Scholar] [CrossRef] [Green Version]
- Bismuth, H.; Adam, R.; Levi, F.; Farabos, C.; Waechter, F.; Castaing, D.; Majno, P.; Engerran, L. Resection of nonresectable liver metastases from colorectal cancer after neoadjuvant chemotherapy. Ann. Surg. 1996, 224, 509–520, discussion 520–502. [Google Scholar] [CrossRef]
- Adam, R.; Delvart, V.; Pascal, G.; Valeanu, A.; Castaing, D.; Azoulay, D.; Giacchetti, S.; Paule, B.; Kunstlinger, F.; Ghemard, O.; et al. Rescue surgery for unresectable colorectal liver metastases downstaged by chemotherapy: A model to predict long-term survival. Ann. Surg. 2004, 240, 644–657. [Google Scholar] [CrossRef]
- Ismaili, N. Treatment of colorectal liver metastases. World J. Surg. Oncol. 2011, 9, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, R. Chemotherapy and surgery: New perspectives on the treatment of unresectable liver metastases. Ann. Oncol. 2003, 14, ii13–ii16. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Nordlinger, B.; Adam, R.; Köhne, C.H.; Pozzo, C.; Poston, G.; Ychou, M.; Rougier, P. Towards a pan-European consensus on the treatment of patients with colorectal liver metastases. Eur. J. Cancer 2006, 42, 2212–2221. [Google Scholar] [CrossRef] [PubMed]
- Gleisner, A.L.; Choti, M.A.; Assumpcao, L.; Nathan, H.; Schulick, R.D.; Pawlik, T.M. Colorectal liver metastases: recurrence and survival following hepatic resection, radiofrequency ablation, and combined resection-radiofrequency ablation. Arch. Surg. 2008, 143, 1204–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puijk, R.S.; Ruarus, A.H.; Vroomen, L.; van Tilborg, A.; Scheffer, H.J.; Nielsen, K.; de Jong, M.C.; de Vries, J.J.J.; Zonderhuis, B.M.; Eker, H.H.; et al. Colorectal liver metastases: surgery versus thermal ablation (COLLISION)—A phase III single-blind prospective randomized controlled trial. BMC Cancer 2018, 18, 821. [Google Scholar] [CrossRef] [PubMed]
- Scheele, J.; Stang, R.; Altendorf-Hofmann, A.; Paul, M. Resection of colorectal liver metastases. World J. Surg. 1995, 19, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Rees, M.; Tekkis, P.P.; Welsh, F.K.; O’Rourke, T.; John, T.G. Evaluation of long-term survival after hepatic resection for metastatic colorectal cancer: a multifactorial model of 929 patients. Ann. Surg. 2008, 247, 125–135. [Google Scholar] [CrossRef]
- Tomlinson, J.S.; Jarnagin, W.R.; DeMatteo, R.P.; Fong, Y.; Kornprat, P.; Gonen, M.; Kemeny, N.; Brennan, M.F.; Blumgart, L.H.; D’Angelica, M. Actual 10-year survival after resection of colorectal liver metastases defines cure. J. Clin. Oncol. 2007, 25, 4575–4580. [Google Scholar] [CrossRef]
- Kopetz, S.; Chang, G.J.; Overman, M.J.; Eng, C.; Sargent, D.J.; Larson, D.W.; Grothey, A.; Vauthey, J.N.; Nagorney, D.M.; McWilliams, R.R. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. J. Clin. Oncol. 2009, 27, 3677–3683. [Google Scholar] [CrossRef]
- Creasy, J.M.; Sadot, E.; Koerkamp, B.G.; Chou, J.F.; Gonen, M.; Kemeny, N.E.; Balachandran, V.P.; Kingham, T.P.; DeMatteo, R.P.; Allen, P.J.; et al. Actual 10-year survival after hepatic resection of colorectal liver metastases: what factors preclude cure? Surgery 2018, 163, 1238–1244. [Google Scholar] [CrossRef]
- Choti, M.A.; Sitzmann, J.V.; Tiburi, M.F.; Sumetchotimetha, W.; Rangsin, R.; Schulick, R.D.; Lillemoe, K.D.; Yeo, C.J.; Cameron, J.L. Trends in long-term survival following liver resection for hepatic colorectal metastases. Ann. Surg. 2002, 235, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Bale, R.; Widmann, G.; Schullian, P.; Haidu, M.; Pall, G.; Klaus, A.; Weiss, H.; Biebl, M.; Margreiter, R. Percutaneous stereotactic radiofrequency ablation of colorectal liver metastases. Eur Radiol. 2012, 22, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, E.K.; Vauthey, J.N.; Ellis, L.M.; Ellis, V.; Pollock, R.; Broglio, K.R.; Hess, K.; Curley, S.A. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Ann. Surg. 2004, 239, 818–825, discussion 825–817. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, S.M.; Mortensen, F.V.; Nielsen, D.T. Radiofrequency ablation of colorectal liver metastases: long-term survival. Acta Radiol. 2007, 48, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Gillams, A.R.; Lees, W.R. Five-year survival in 309 patients with colorectal liver metastases treated with radiofrequency ablation. Eur. Radiol. 2009, 19, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Meijerink, M.R.; Puijk, R.S.; van Tilborg, A.; Henningsen, K.H.; Fernandez, L.G.; Neyt, M.; Heymans, J.; Frankema, J.S.; de Jong, K.P.; Richel, D.J.; et al. Radiofrequency and Microwave Ablation Compared to Systemic Chemotherapy and to Partial Hepatectomy in the Treatment of Colorectal Liver Metastases: A Systematic Review and Meta-Analysis. Cardiovasc. Intervent. Radiol. 2018, 41, 1189–1204. [Google Scholar] [CrossRef] [Green Version]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2013, 14, 1208–1215. [Google Scholar] [CrossRef]
- Nieuwenhuizen, S.; Puijk, R.S.; van den Bemd, B.; Aldrighetti, L.; Arntz, M.; van den Boezem, P.B.; Bruynzeel, A.M.E.; Burgmans, M.C.; de Cobelli, F.; Coolsen, M.M.E.; et al. Resectability and Ablatability Criteria for the Treatment of Liver Only Colorectal Metastases: Multidisciplinary Consensus Document from the COLLISION Trial Group. Cancers 2020, 12. [Google Scholar] [CrossRef]
- Kanemitsu, Y.; Shimizu, Y.; Mizusawa, J.; Inaba, Y.; Hamaguchi, T.; Shida, D.; Ohue, M.; Komori, K.; Shiomi, A.; Shiozawa, M. A randomized phase II/III trial comparing hepatectomy followed by mFOLFOX6 with hepatectomy alone for liver metastasis from colorectal cancer: JCOG0603 study. J. Clin. Oncol. 2020, 38 (15_suppl), 4005. [Google Scholar] [CrossRef]
- Saiura, A.; Yamamoto, J.; Hasegawa, K.; Koga, R.; Sakamoto, Y.; Hata, S.; Makuuchi, M.; Kokudo, N. Liver resection for multiple colorectal liver metastases with surgery up-front approach: bi-institutional analysis of 736 consecutive cases. World J. Surg. 2012, 36, 2171–2178. [Google Scholar] [CrossRef]
- Vigano, L.; Ferrero, A.; Lo Tesoriere, R.; Capussotti, L. Liver surgery for colorectal metastases: results after 10 years of follow-up. Long-term survivors, late recurrences, and prognostic role of morbidity. Ann. Surg. Oncol. 2008, 15, 2458–2464. [Google Scholar] [CrossRef]
- Viganò, L.; Pedicini, V.; Comito, T.; Carnaghi, C.; Costa, G.; Poretti, D.; Franzese, C.; Personeni, N.; Del Fabbro, D.; Rimassa, L.; et al. Aggressive and Multidisciplinary Local Approach to Iterative Recurrences of Colorectal Liver Metastases. World J. Surg. 2018, 42, 2651–2659. [Google Scholar] [CrossRef]
- Petrowsky, H.; Gonen, M.; Jarnagin, W.; Lorenz, M.; DeMatteo, R.; Heinrich, S.; Encke, A.; Blumgart, L.; Fong, Y. Second liver resections are safe and effective treatment for recurrent hepatic metastases from colorectal cancer: A bi-institutional analysis. Ann. Surg. 2002, 235, 863–871. [Google Scholar] [CrossRef]
- Adam, R.; Bismuth, H.; Castaing, D.; Waechter, F.; Navarro, F.; Abascal, A.; Majno, P.; Engerran, L. Repeat hepatectomy for colorectal liver metastases. Ann. Surg. 1997, 225, 51–60, discussion 60–52. [Google Scholar] [CrossRef] [PubMed]
- Takamoto, T.; Hashimoto, T.; Miyata, A.; Shimada, K.; Maruyama, Y.; Makuuchi, M. Repeat Hepatectomy After Major Hepatectomy for Colorectal Liver Metastases. J. Gastrointest. Surg. 2020, 24, 380–387. [Google Scholar] [CrossRef]
- Imai, K.; Allard, M.A.; Benitez, C.C.; Vibert, E.; Sa Cunha, A.; Cherqui, D.; Castaing, D.; Bismuth, H.; Baba, H.; Adam, R. Early recurrence after hepatectomy for colorectal liver metastases: What optimal definition and what predictive factors? Oncologist 2016, 21, 887–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, D.; Xu, J.; Zhong, Y.; Wei, Y. Effect of Neoadjuvant Chemotherapy in Patients with Resectable Colorectal Liver Metastases. Ann. Oncol. 2013, 24, ix55. [Google Scholar] [CrossRef] [Green Version]
- Ayez, N.; van der Stok, E.P.; de Wilt, H.; Radema, S.A.; van Hillegersberg, R.; Roumen, R.M.; Vreugdenhil, G.; Tanis, P.J.; Punt, C.J.; Dejong, C.H.; et al. Neo-adjuvant chemotherapy followed by surgery versus surgery alone in high-risk patients with resectable colorectal liver metastases: The CHARISMA randomized multicenter clinical trial. BMC Cancer 2015, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayez, N.; Van Der Stok, E.P.; Grünhagen, D.J.; Rothbarth, J.; Van Meerten, E.; Eggermont, A.M.; Verhoef, C. The use of neo-adjuvant chemotherapy in patients with resectable colorectal liver metastases: Clinical risk score as possible discriminator. Eur. J. Surg. Oncol. 2015, 41, 859–867. [Google Scholar] [CrossRef]
- Kooby, D.A.; Fong, Y.; Suriawinata, A.; Gonen, M.; Allen, P.J.; Klimstra, D.S.; DeMatteo, R.P.; D’Angelica, M.; Blumgart, L.H.; Jarnagin, W.R. Impact of steatosis on perioperative outcome following hepatic resection. J. Gastrointest. Surg. 2003, 7, 1034–1044. [Google Scholar] [CrossRef]
- Vauthey, J.N.; Pawlik, T.M.; Ribero, D.; Wu, T.T.; Zorzi, D.; Hoff, P.M.; Xiong, H.Q.; Eng, C.; Lauwers, G.Y.; Mino-Kenudson, M.; et al. Chemotherapy regimen predicts steatohepatitis and an increase in 90-day mortality after surgery for hepatic colorectal metastases. J. Clin. Oncol. 2006, 24, 2065–2072. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adair, R.A.; Young, A.L.; Cockbain, A.J.; Malde, D.; Prasad, K.R.; Lodge, J.P.; Toogood, G.J. Repeat hepatic resection for colorectal liver metastases. Br. J. Surg 2012, 99, 1278–1283. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Pascal, G.; Azoulay, D.; Tanaka, K.; Castaing, D.; Bismuth, H. Liver resection for colorectal metastases: the third hepatectomy. Ann. Surg 2003, 238, 871–883, discussion 883–874. [Google Scholar] [CrossRef]
- Andreou, A.; Brouquet, A.; Abdalla, E.K.; Aloia, T.A.; Curley, S.A.; Vauthey, J.N. Repeat hepatectomy for recurrent colorectal liver metastases is associated with a high survival rate. HPB (Oxford) 2011, 13, 774–782. [Google Scholar] [CrossRef] [Green Version]
- Brachet, D.; Lermite, E.; Rouquette, A.; Lorimier, G.; Hamy, A.; Arnaud, J.P. Prognostic factors of survival in repeat liver resection for recurrent colorectal metastases: review of sixty-two cases treated at a single institution. Dis. Colon Rectum 2009, 52, 475–483. [Google Scholar] [CrossRef] [Green Version]
- Butte, J.M.; Gonen, M.; Allen, P.J.; Peter Kingham, T.; Sofocleous, C.T.; DeMatteo, R.P.; Fong, Y.; Kemeny, N.E.; Jarnagin, W.R.; D’Angelica, M.I. Recurrence After Partial Hepatectomy for Metastatic Colorectal Cancer: Potentially Curative Role of Salvage Repeat Resection. Ann. Surg Oncol. 2015, 22, 2761–2771. [Google Scholar] [CrossRef]
- Hallet, J.; Cunha, A.S.; Adam, R.; Goere, D.; Azoulay, D.; Mabrut, J.Y.; Muscari, F.; Laurent, C.; Navarro, F.; Pessaux, P. Outcomes of Rehepatectomy for Colorectal Liver Metastases: A Contemporary Multi-Institutional Analysis from the French Surgical Association Database. Ann. Surg. Oncol. 2016, 23, 894–903. [Google Scholar] [CrossRef]
- Hashimoto, M.; Kobayashi, T.; Ishiyama, K.; Ide, K.; Ohira, M.; Tahara, H.; Kuroda, S.; Hamaoka, M.; Iwako, H.; Okimoto, M.; et al. Efficacy of repeat hepatectomy for recurrence following curative hepatectomy for colorectal liver metastases: A Retrospective Cohort Study of 128 patients. Int. J. Surg. 2016, 36, 96–103. [Google Scholar] [CrossRef]
- Heise, D.; Bayings, W.; Tuinhof, A.; Eickhoff, R.; Kroh, A.; Ulmer, F.; Dejong, C.H.C.; Neumann, U.; Binnebosel, M. Long-term outcome and quality of life after initial and repeat resection of colorectal liver metastasis: A retrospective analysis. Int. J. Surg. 2017, 48, 281–285. [Google Scholar] [CrossRef]
- Homayounfar, K.; Bleckmann, A.; Conradi, L.C.; Sprenger, T.; Lorf, T.; Niessner, M.; Sahlmann, C.O.; Meller, J.; Liersch, T.; Ghadimi, B.M. Metastatic recurrence after complete resection of colorectal liver metastases: Impact of surgery and chemotherapy on survival. Int. J. Colorectal Dis. 2013, 28, 1009–1017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, K.; Yamashita, Y.I.; Miyamoto, Y.; Nakagawa, S.; Okabe, H.; Hashimoto, D.; Chikamoto, A.; Baba, H. The predictors and oncological outcomes of repeat surgery for recurrence after hepatectomy for colorectal liver metastases. Int J. Clin. Oncol. 2018, 23, 908–916. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Benitez, C.C.; Allard, M.A.; Vibert, E.; Cunha, A.S.; Cherqui, D.; Castaing, D.; Bismuth, H.; Baba, H.; Adam, R. Impact of Surgical Treatment for Recurrence After 2-Stage Hepatectomy for Colorectal Liver Metastases, on Patient Outcome. Ann. Surg. 2019, 269, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Ishiguro, S.; Akasu, T.; Fujimoto, Y.; Yamamoto, J.; Sakamoto, Y.; Sano, T.; Shimada, K.; Kosuge, T.; Yamamoto, S.; Fujita, S.; et al. Second hepatectomy for recurrent colorectal liver metastasis: analysis of preoperative prognostic factors. Ann. Surg. Oncol. 2006, 13, 1579–1587. [Google Scholar] [CrossRef] [PubMed]
- Kishi, Y.; Nara, S.; Esaki, M.; Shimada, K. Feasibility of "Watch-and-Wait" Management before Repeat Hepatectomy for Colorectal Liver Metastases. Dig. Surg. 2019, 36, 233–240. [Google Scholar] [CrossRef]
- Matsuoka, H.; Morise, Z.; Tanaka, C.; Hayashi, T.; Ikeda, Y.; Maeda, K.; Masumori, K.; Koide, Y.; Katsuno, H.; Tanahashi, Y.; et al. Repeat hepatectomy with systemic chemotherapy might improve survival of recurrent liver metastasis from colorectal cancer-a retrospective observational study. World J. Surg. Oncol. 2019, 17, 33. [Google Scholar] [CrossRef]
- Neal, C.P.; Nana, G.R.; Jones, M.; Cairns, V.; Ngu, W.; Isherwood, J.; Dennison, A.R.; Garcea, G. Repeat hepatectomy is independently associated with favorable long-term outcome in patients with colorectal liver metastases. Cancer Med. 2017, 6, 331–338. [Google Scholar] [CrossRef] [Green Version]
- Neeff, H.P.; Drognitz, O.; Holzner, P.; Klock, A.; Bronsert, P.; Hopt, U.T.; Makowiec, F. Outcome after repeat resection of liver metastases from colorectal cancer. Int J. Colorectal Dis. 2013, 28, 1135–1141. [Google Scholar] [CrossRef]
- Pessaux, P.; Lermite, E.; Brehant, O.; Tuech, J.J.; Lorimier, G.; Arnaud, J.P. Repeat hepatectomy for recurrent colorectal liver metastases. J. Surg. Oncol. 2006, 93, 1–7. [Google Scholar] [CrossRef]
- Valdimarsson, V.T.; Hellberg, K.; Brismar, T.B.; Sparrelid, E.; Sturesson, C. Repeat procedures for recurrent colorectal liver metastases: analysis of long-term liver regeneration and outcome. Cancer Manag. Res. 2019, 11, 2617–2622. [Google Scholar] [CrossRef] [Green Version]
- Vigano, L.; Capussotti, L.; Lapointe, R.; Barroso, E.; Hubert, C.; Giuliante, F.; Ijzermans, J.N.; Mirza, D.F.; Elias, D.; Adam, R. Early recurrence after liver resection for colorectal metastases: risk factors, prognosis, and treatment. A LiverMetSurvey-based study of 6,025 patients. Ann. Surg. Oncol. 2014, 21, 1276–1286. [Google Scholar] [CrossRef] [PubMed]
- Wicherts, D.A.; de Haas, R.J.; Salloum, C.; Andreani, P.; Pascal, G.; Sotirov, D.; Adam, R.; Castaing, D.; Azoulay, D. Repeat hepatectomy for recurrent colorectal metastases. Br. J. Surg. 2013, 100, 808–818. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J.; Guyatt, G.; Oxman, A.D.; Alderson, P.; Dahm, P.; Falck-Ytter, Y.; Nasser, M.; Meerpohl, J.; Post, P.N.; Kunz, R.; et al. GRADE guidelines: 14. Going from evidence to recommendations: the significance and presentation of recommendations. J. Clin. Epidemiol. 2013, 66, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Kouri, B.E.; Abrams, R.A.; Al-Refaie, W.B.; Azad, N.; Farrell, J.; Gaba, R.C.; Gervais, D.A.; Gipson, M.G.; Kolbeck, K.J.; Marshalleck, F.E.; et al. ACR Appropriateness Criteria Radiologic Management of Hepatic Malignancy. Available online: https://acsearch.acr.org/docs/69379/Narrative/ (accessed on 29 October 2020).
- You, Y.N.; Hardiman, K.M.; Bafford, A.; Poylin, V.; Francone, T.D.; Davis, K.; Paquette, I.M.; Steele, S.R.; Feingold, D.L.; On Behalf of the Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons (A.S.C.R.S.). Clinical Practice Guidelines for the Management of Rectal Cancer. Available online: https://fascrs.org/ascrs/media/files/downloads/rectal-cancer-CPG-2020.pdf (accessed on 29 October 2020).
- Vogel, J.D.; Eskicioglu, C.; Weiser, M.R.; Feingold, D.L.; Steele, S.R.; The American Society of Colon and Rectal Surgeons. Clinical Practice Guidelines for the Treatment of Colon Cancer. Available online: https://fascrs.org/ascrs/media/files/downloads/Clinical%20Practice%20Guidelines/cpg_treatment_of_colon_cancer.pdf (accessed on 29 October 2020).
- Steele, S.R.; Chang, G.J.; Hendren, S.; Weiser, M.; Irani, J.; Buie, W.D.; Rafferty, J.F.; Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. Practice Guideline for the Surveillance of Patients After Curative Treatment of Colon and Rectal Cancer. Available online: https://fascrs.org/ascrs/media/files/downloads/Clinical%20Practice%20Guidelines/practice_guideline_for_the_surveillance_of-1.pdf (accessed on 29 October 2020).
- Van Cutsem, E.; Cervantes, A.; Nordlinger, B.; Arnold, D. Metastatic Colorectal Cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Available online: https://www.annalsofoncology.org/article/S0923-7534(19)34091-8/pdf (accessed on 29 October 2020).
- Peeters, L.; Leroy, R.; Robays, J.; Veereman, G.; Bielen, D.; Ceelen, W.; Belgian Health Care Knowledge Center (K.C.E.). Colon Cancer: Diagnosis, Treatment and Follow-Up. Available online: https://www.kce.fgov.be/sites/default/files/atoms/files/KCE_218_Colon_cancer.pdf (accessed on 29 October 2020).
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. NCCN Guidelines Insights: Colon Cancer, Version 2. 2018. Available online: https://jnccn.org/view/journals/jnccn/16/4/article-p359.xml?ArticleBodyColorStyles=pdf-5590 (accessed on 29 October 2020).
- Scottish Intercollegiate Guidelines Network (S.I.G.N.) Diagnosis and Management of colorectal cancer. Available online: https://www.sign.ac.uk/media/1064/sign126.pdf (accessed on 29 October 2020).
- Gomez-Espana, M.A.; Gallego, J.; Gonzalez-Flores, E.; Maurel, J.; Paez, D.; Sastre, J.; Aparicio, J.; Benavides, M.; Feliu, J.; Vera, R. SEOM clinical guidelines for diagnosis and treatment of metastatic colorectal cancer (2018). Clin. Transl. Oncol. 2019, 21, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Phelip, J.M.; Tougeron, D.; Léonard, D.; Benhaim, L.; Desolneux, G.; Dupré, A.; Michel, P.; Penna, C.; Tournigand, C.; Louvet, C.; et al. Metastatic colorectal cancer (mCRC): French intergroup clinical practice guidelines for diagnosis, treatments and follow-up (SNFGE, FFCD, GERCOR, UNICANCER, SFCD, SFED, SFRO, SFR). Dig. Liver Dis. 2019, 51, 1357–1363. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (N.I.C.E.). Treatment for Metastatic Colorectal Cancer in the Liver Amenable to Treatment with Curative Intent: Colorectal Cancer (Update): Evidence Review D2a. Available online: https://www.nice.org.uk/guidance/ng151/evidence/d2a-treatment-for-metastatic-colorectal-cancer-in-the-liver-amenable-to-treatment-with-curative-intent-pdf-253058083672 (accessed on 29 October 2020).
- National Institute for Health and Care Excellence (N.I.C.E.). Radiofrequency Ablation for Colorectal Liver Metastases. Available online: https://www.nice.org.uk/guidance/IPG327 (accessed on 29 October 2020).
- National Institute for Health and Care Excellence (N.I.C.E.). Microwave ablation for treating liver metastases. Available online: https://www.nice.org.uk/guidance/IPG553 (accessed on 29 October 2020).
- Hashiguchi, Y.; Muro, K.; Saito, Y.; Ito, Y.; Ajioka, Y.; Hamaguchi, T.; Hasegawa, K.; Hotta, K.; Ishida, H.; Ishiguro, M.; et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int. J. Clin. Oncol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Integraal Kankercentrum Nederland (I.K.N.L.). Guideline Colorectaal Carcinoom. Available online: https://www.oncoline.nl/colorectaalcarcinoom (accessed on 29 October 2020).
- Brudvik, K.W.; Jones, R.P.; Giuliante, F.; Shindoh, J.; Passot, G.; Chung, M.H.; Song, J.; Li, L.; Dagenborg, V.J.; Fretland, A.A.; et al. RAS Mutation Clinical Risk Score to Predict Survival After Resection of Colorectal Liver Metastases. Ann. Surg. 2019, 269, 120–126. [Google Scholar] [CrossRef]
- Sofocleous, C.T.; Petre, E.N.; Gonen, M.; Brown, K.T.; Solomon, S.B.; Covey, A.M.; Alago, W.; Brody, L.A.; Thornton, R.H.; D’Angelica, M.; et al. CT-guided radiofrequency ablation as a salvage treatment of colorectal cancer hepatic metastases developing after hepatectomy. J. Vasc. Interv. Radiol. 2011, 22, 755–761. [Google Scholar] [CrossRef] [Green Version]
- Shady, W.; Petre, E.N.; Gonen, M.; Erinjeri, J.P.; Brown, K.T.; Covey, A.M.; Alago, W.; Durack, J.C.; Maybody, M.; Brody, L.A.; et al. Percutaneous radiofrequency ablation of colorectal cancer liver metastases: Factors affecting outcomes-a 10-year experience at a single center. Radiology 2016, 278, 601–611. [Google Scholar] [CrossRef] [Green Version]
- Nordlinger, B.; Van Cutsem, E.; Rougier, P.; Köhne, C.H.; Ychou, M.; Sobrero, A.; Adam, R.; Arvidsson, D.; Carrato, A.; Georgoulias, V.; et al. Does chemotherapy prior to liver resection increase the potential for cure in patients with metastatic colorectal cancer? A report from the European Colorectal Metastases Treatment Group. Eur. J. Cancer 2007, 43, 2037–2045. [Google Scholar] [CrossRef]
- de Gramont, A.; Figer, A.; Seymour, M.; Homerin, M.; Hmissi, A.; Cassidy, J.; Boni, C.; Cortes-Funes, H.; Cervantes, A.; Freyer, G.; et al. Leucovorin and fluorouracil with or without oxaliplatin as first-line treatment in advanced colorectal cancer. J. Clin. Oncol. 2000, 18, 2938–2947. [Google Scholar] [CrossRef] [PubMed]
- Fong, Y.; Fortner, J.; Sun, R.L.; Brennan, M.F.; Blumgart, L.H. Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: analysis of 1001 consecutive cases. Ann. Surg. 1999, 230, 309–318, discussion 318–321. [Google Scholar] [CrossRef] [PubMed]
- Pietrantonio, F.; Fuca, G.; Manca, P.; Pagani, F.; Raimondi, A.; Prisciandaro, M.; Randon, G.; Corti, F.; de Braud, F.; Cremolini, C.; et al. Validation of the Colon Life nomogram in patients with refractory metastatic colorectal cancer enrolled in the RECOURSE trial. Tumori 2020. [Google Scholar] [CrossRef] [PubMed]
- Pietrantonio, F.; Miceli, R.; Rimassa, L.; Lonardi, S.; Aprile, G.; Mennitto, A.; Marmorino, F.; Bozzarelli, S.; Antonuzzo, L.; Tamburini, E.; et al. Estimating 12-week death probability in patients with refractory metastatic colorectal cancer: The Colon Life nomogram. Ann. Oncol. 2017, 28, 555–561. [Google Scholar] [CrossRef] [PubMed]





| Author | Year | Years of Inclusion | Number of Patients with Repeat Local Treatment | Median Age in Years (Range) | Mean Age in Years ± SD |
|---|---|---|---|---|---|
| Adair [45] | 2012 | 1993–2010 | 195 | 63 (24–85) | NR |
| Adam [46] | 2003 | 1984–2000 | 139 (2nd) * 60 (3rd) * | NR (32–78) NR (33–86) | 56 ± 10 56 ± 10 |
| Andreou [47] | 2011 | 1993–2009 | 43 | 55 (32–74) | NR |
| Brachet [48] | 2009 | 1992–2007 | 62 (2nd) * 15 (3rd) * 2 (4th) * | NR NR NR | 62.2 ± 9.7 57.9 ± 10.8 54.5 ± 10.6 |
| Butte [49] | 2015 | 1994–2004 | 159 (PST) | 59 (31–81) | 58.1 ± 10.9 |
| Hallet [50] | 2016 | 2006–2013 | 447 | 61.4 (NR) | NR |
| Hashimoto [51] | 2016 | 2000–2012 | 17 | 60 (40–80) | NR |
| Heise [52] | 2017 | 2010–2016 | 38 | 59.1 (NR) | NR ± 12.1 |
| Homayounfar [53] | 2013 | 2001–2011 | 52 | 62.8 (NR) | NR |
| Imai [54] | 2018 | 2000–2016 | 54 | 64 (25–94) a | 63.1 ± 11.0 a |
| Imai [55] | 2019 | 1992–2012 | 29 | 57 (31–82) a | 55.8 ± 9.9 a |
| Ishiguro [56] | 2006 | 1985–2004 | 111 | NR | 59 ± NR |
| Kishi [57] | 2019 | 2000–2015 | 115 | 59 (28–86) | NR |
| Matsuoka [58] | 2019 | 1974–2016 | 59 | NR (25–95) a | 66 ± 11.2 a |
| Neal [59] | 2017 | 2001–2010 | 71 | 64 (26–85) a | 63.4 ± NR a |
| Neeff [60] | 2013 | 1999–2011 | 77 | NR | NR |
| Pessaux [61] | 2006 | 1992–2002 | 42 | NR (34–80) | 63.5 ± NR |
| Valdimarsson [62] | 2019 | 2005–2015 | 82 | 64 (NR) | NR |
| Viganò [63] | 2014 | 1998–2009 | 234 | NR | NR |
| Wicherts [64] | 2013 | 1990–2010 | 263 | NR | 57 ± 11 |
| Author | Chemotherapy + rLT, n (%) | Chemotherapeutic Agents (%) | rLT alone, n (%) | rLT Procedure (%) | Overall Mortality and Morbidity Rate (%) |
|---|---|---|---|---|---|
| Adair [45] | 52 (26.7%) | FUFOL (28.8%) FOLFOX (34.6%) FUFOL + irinotecan (9.6%) Capecitabine (3.8%) Oxaliplatin (23.1%) | 143 (73.3%) | Metastasectomy (70.8%) Segmentectomy (10.3%) Hemihepatectomy (12.2%) Trisectionectomy (4.6%) Caudate resection (2.1%) | 30-day mortality 1.5% 30-day morbidity 20% (4.6% relaparotomy) |
| Adam [46] | 2nd *: 127 (91%) 3rd *: 51 (85%) | FOLFOX (NR) | 2nd *: 12 (9%) 3rd *: 9 (15%) | 2nd *
| Mortality <2 months
|
| Andreou [47] | 19 (44%) | NR | 24 (56%) | Minor resections <3 segments (88%) Major liver resection ≥ 3 segments (12%) | 30-day mortality 0% 90-day mortality 0% Morbidity 12% (0% required intervention) |
| Brachet [48] | 2nd *: 38 (61.3%) 3rd *: 6 (40%) 4th *: 0 (0%) | 2nd *
| 2nd *: 24 (38.7%) 3rd *: 9 (60%) 4th *: 2 (100%) | 2nd *
| Mortality <30 days
<30 days (3.8% reoperation)
|
| Butte [49] | 47 (30%) | NR | 112 (70%) | Minor hepatectomy <hemi-liver (41%) Major hepatectomy: hemi-, central or extended (59%) | NR |
| Hallet [50] | 310 (69.4%) | NR | 137 (30.6%) | NR | Mortality <30 days 1.3% Morbidity <30 days 28.9% (8.1% re-intervention) |
| Hashimoto [51] | 4 (24%) | Oxaliplatin (NR) or irinotecan (NR) | 13 (76%) | Minor hepatectomy: wedge, segmental or sectional (88.2%) Major hepatectomy ≥ 3 segments (11.8%) | NR Morbidity 17.7% |
| Heise [52] | 36 (95%) | NR | 2 (5%) | Minor hepatectomy (76%) Major hepatectomy >hemi-liver (24%) | NR Morbidity 3% |
| Homayounfar [53] | 10 (19%) | 5FU (9%) 5FU + oxaliplatin (36%) 5FU + irinotecan (55%) Additional cetuximab (19%) Additional bevacizumab (34%) | 42 (81%) | Surgical exploration only (5.8%) Surgical exploration + RFA liver (7.7%) Non-anatomic liver resection (38%) Bisegmentectomy (3.8%) Bisegmentectomy + nonanatomic liver resection (1.9%) Hemihepatectomy (5.8%) Trisectorectomy (1.9%) Rectal resection (5.8%) Rectal extirpation + nonanatomic liver resection (1.9%) Others (26.9%) | Mortality 0% Morbidity 26% |
| Imai, 2018 [54] | 28 (51.9%) | Oxaliplatin-based (14.3%) Oxaliplatin-based + biologic agents (17.9%) Irinotecan-based (7.1%) Irinotecan-based + biologic agents (42.9%) Oxaliplatin and irinotecan-based + biologic agents (3.6%) Others (14.3%) | 26 (48.1%) | Hepatectomy (38.9%) Hepatectomy + RFA (5.6%) Hepatectomy + resection of peritoneal metastasis (1.9%) RFA for liver metastasis (14.8%) RFA for liver + lung metastasis (1.9%) Others (37.0%) | NR |
| Imai, 2019 [55] | 28 (73.7%) | NR | 10 (26.3%) | NR | NR |
| Ishiguro [56] | NR | NR | NR | Minor resection (89.2%) Hemihepatectomy (5.4%) Extended hemihepatectomy (4.5%) Central bisectionectomy (0.9%) | Mortality 0% Morbidity 14% |
| Kishi [57] | 6 (5.2%) | Oxaliplatin-based (NR) Irinotecan-based (NR) 5-FU with leucovorin (NR) Tegafur, Gimeracil, Oteracil Potassium (NR) | 109 (94.8%) | NR | Mortality 0.9% Morbidity 27% |
| Matsuoka [58] | 55 (93%) | NR | 4 (7%) | Sectionectomy (26%) Segmentectomy (10%) Partial resection (64%) | Mortality 5% Morbidity 39% |
| Neal [59] | 8 (11.3%) | NR | 63 (88.7%) | Anatomical resection (19.7%) Major hepatectomy ≥ 3 segments (16.9%) NR | Mortality <90 days Morbidity <90 days 21.1% |
| Neeff [60] | 67 (87%) | All 5-FU based | 10 (13%) | Atypical/wedge (39.1%) Segmental (23.9%) Hemihepatectomy (17.4%) Extended hemihepatectomy (17.4%) Central resection (2.2%) | Mortality 3.3% Morbidity 53.3% (12% operative revisions) |
| Pessaux [61] | 28 (66.7%) | NR | 14 (33.3%) | Anatomic hepatectomy (66.7%) Non-anatomic hepatectomy (33.3%) | Mortality <30 days 0% Morbidity <30 days 14.3% |
| Valdimarsson [62] | 37 (45%) | All oxaliplatin based | 45 (55%) | Major liver procedure ≥ 3 segments 19% Minor liver procedure 81% | NR Morbidity 18% |
| Viganò [63] | NR | Oxaliplatin-based (NR) Irinotecan-based (NR) Associated cetuximab (NR) Associated bevacizumab (NR) | NR | Anatomic resection (NR) Non-anatomic resection (NR) Associated intraoperative RFA | NR |
| Wicherts [64] | 157 (60.7%) | Last line regimen
| 106 (40.3%) | Major resection ≥3 segments (17.0%) Anatomical (27.9%) Non-anatomical (52.1%) Both anatomical and non-anatomical (20.0%) | 90-day mortality 2.4% Morbidity 34.4% |
| Author | Outcomes (NAC + rLT vs. rLT Alone) | Conclusions | Limitations |
|---|---|---|---|
| Adair [45] | Univariable analysis proportional hazards model OS: p= 0.250 DFS: not significant (p-value NR) | NAC before repeat resection did not reduce OS or affect DFS. NAC before local treatment could enhance resectability rates. | Long study duration |
| Adam [46] | Log-rank test survival one-year OS: 70% vs. 70% three-year OS: 45% vs. 53% p = 0.86 | No significant difference in survival for NAC in third hepatectomy. Higher risk of bleeding and more fragile liver caused by chemotherapy. | Limited population |
| Brachet [48] | Univariate Cox regression analysis survival HR = 1.034 (0.521–2.051) p = 0.923 | NAC is not a prognostic factor but might increase survival in repeat hepatectomy. NAC improves resectability of repeat resection. | Limited population Long study duration |
| Butte [49] | Effective salvage therapy 27.3% vs. 24.0% p = 0.7 | No significant difference in effectiveness of salvage therapy between NAC + resection and resection alone. | Selection bias |
| Heise [52] | Univariate analysis DFS p = 0.483 | No significant difference in disease-free survival for perioperative chemotherapy. | Limited population |
| Neal [59] | Univariate Cox regression survival analysis OS: HR (95% CI) = 0.951 (0.400–2.261) p = 0.910 Cancer-specific survival: HR (95% CI) = 1.033 (0.434–2.455) p = 0.942 | No significant association in OS between NAC + hepatectomy and hepatectomy alone. | Limited population Selection bias |
| Neeff [60] | Univariate analysis of survival log-rank test one-year OS: 96.9% vs. 100.0% three-year OS: 59.8% vs. 80.0% five-year OS: 50.4% vs. 40.0% p = 0.89 | Chemotherapy did not univariately affected long-term outcome in survival. | Small sample size |
| Pessaux [61] | Univariate analysis log-rank test two-tailed five-year OS: 27% vs. 11% p = 0.39 | Effective chemotherapy and repeat local treatment is suggested for improved prognosis. | Limited population |
| Valdimarsson [62] | Relative liver volumes after second procedure 100% vs. 91% p = 0.200 | Liver volume did not significantly differ between patients with and without chemotherapy | Selection bias |
| Viganò [63] | Univariate analysis log rank test five-year OS: 61.5% vs. 43.7% p = 0.021 Multivariate analysis Cox proportional hazard model HR (95% CI) = 0.529 (0.299–0.934) p = 0.028 | Higher survival rates for patients with preoperative chemotherapy before re-resection. Response to chemotherapy univariately improved survival, but multivariately the prognostic role was not confirmed. | Selection bias |
| Wicherts [64] | Univariable analysis five-year OS: 39% vs. 36% p = 0.572 | No significant Repeat local treatment is more challenging after preoperative chemotherapy due to liver damage. | Limited population |
| Author | Conclusions and Recommendations | Limitations |
|---|---|---|
| Andreou [47] | No negative effect of NAC on surgical results of repeat local treatment. | Selection bias |
| Hallet [50] | The liver is potentially more friable after chemotherapy before repeat local treatment. | Selection bias Information bias Misclassification bias |
| Hashimoto [51] | Suggestion of aggressive oncosurgical approach if recurrent CRLM is resectable. Chemotherapy and repeat local treatment are related to increased PFS. Evaluation of responsiveness of chemotherapy affected selection of repeat local treatment. | Limited sample size Long study duration Selection bias |
| Homayounfar [53] | Intensive chemotherapy protocols could qualify a larger group of patients for repeat local treatment. | Selection bias |
| Imai, 2018 [54] | Prognostic character of chemotherapy remains unclear. Aggressive oncosurgical approach might be associated with increased survival. | Selection bias |
| Imai, 2019 [55] | Beneficial outcome for patients with NAC and repeat local treatment. | Historical bias |
| Ishiguro [56] | Chemotherapy before local treatment could prolong survival for patients with risk factors (extended disease). | Selection bias |
| Kishi [57] | The OS of NAC + repeat resection and repeat resection alone was comparable. | Selection bias |
| Matsuoka [58] | Aggressive oncosurgical approach should be performed, considering repeat hepatectomy and systemic chemotherapy. It might improve survival in selected patients. | Selection bias |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dijkstra, M.; Nieuwenhuizen, S.; Puijk, R.S.; Geboers, B.; Timmer, F.E.F.; Schouten, E.A.C.; Scheffer, H.J.; de Vries, J.J.J.; Ket, J.C.F.; Versteeg, K.S.; et al. The Role of Neoadjuvant Chemotherapy in Repeat Local Treatment of Recurrent Colorectal Liver Metastases: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 378. https://doi.org/10.3390/cancers13030378
Dijkstra M, Nieuwenhuizen S, Puijk RS, Geboers B, Timmer FEF, Schouten EAC, Scheffer HJ, de Vries JJJ, Ket JCF, Versteeg KS, et al. The Role of Neoadjuvant Chemotherapy in Repeat Local Treatment of Recurrent Colorectal Liver Metastases: A Systematic Review and Meta-Analysis. Cancers. 2021; 13(3):378. https://doi.org/10.3390/cancers13030378
Chicago/Turabian StyleDijkstra, Madelon, Sanne Nieuwenhuizen, Robbert S. Puijk, Bart Geboers, Florentine E. F. Timmer, Evelien A. C. Schouten, Hester J. Scheffer, Jan J. J. de Vries, Johannes C. F. Ket, Kathelijn S. Versteeg, and et al. 2021. "The Role of Neoadjuvant Chemotherapy in Repeat Local Treatment of Recurrent Colorectal Liver Metastases: A Systematic Review and Meta-Analysis" Cancers 13, no. 3: 378. https://doi.org/10.3390/cancers13030378