Pre-Existing Cardiovascular Conditions as Clinical Predictors of Myocarditis Reporting with Immune Checkpoint Inhibitors: A VigiBase Study


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
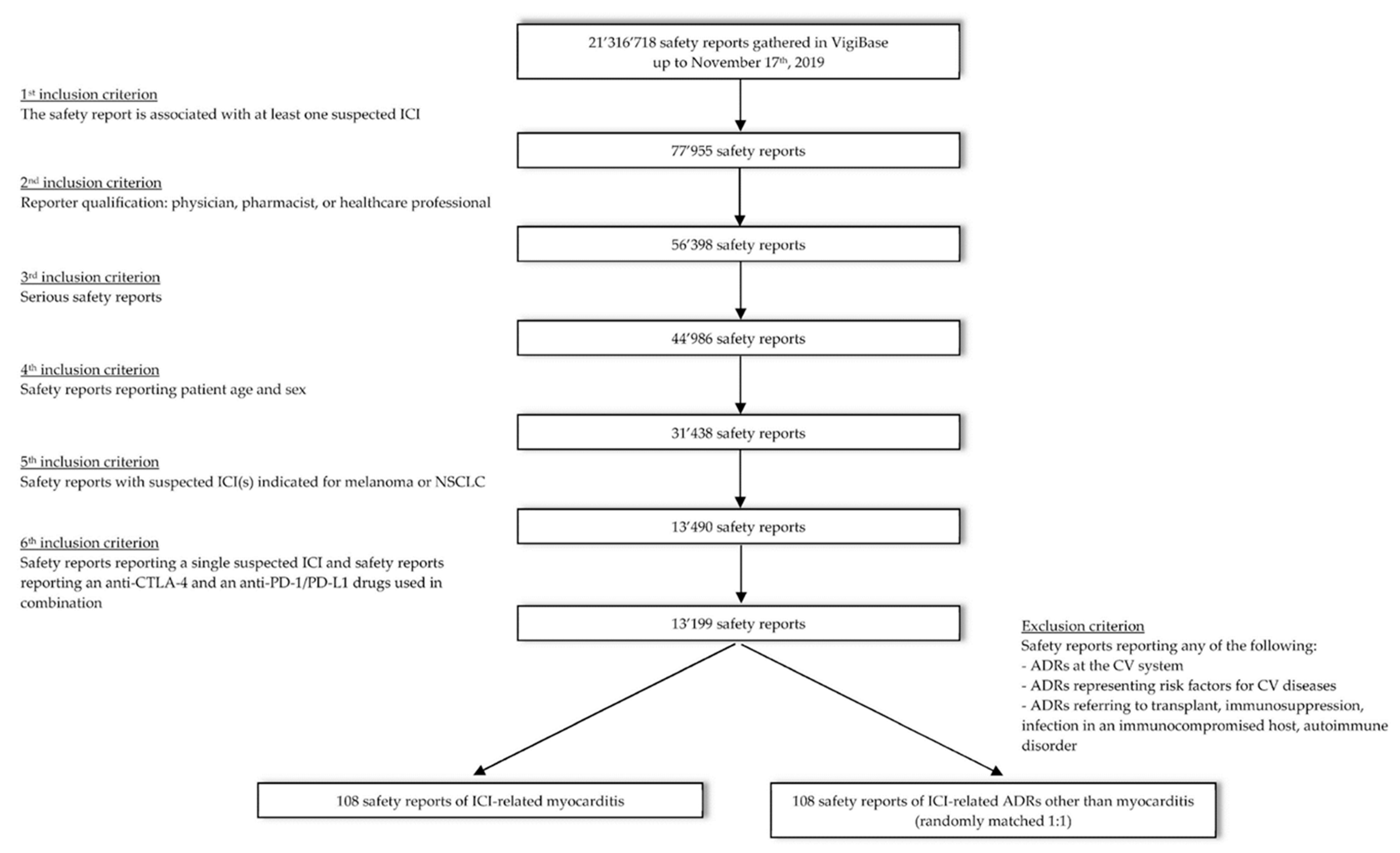
2.2. Data Retrieval and Selection
2.3. Study Design
2.4. Statistical Analysis
3. Results
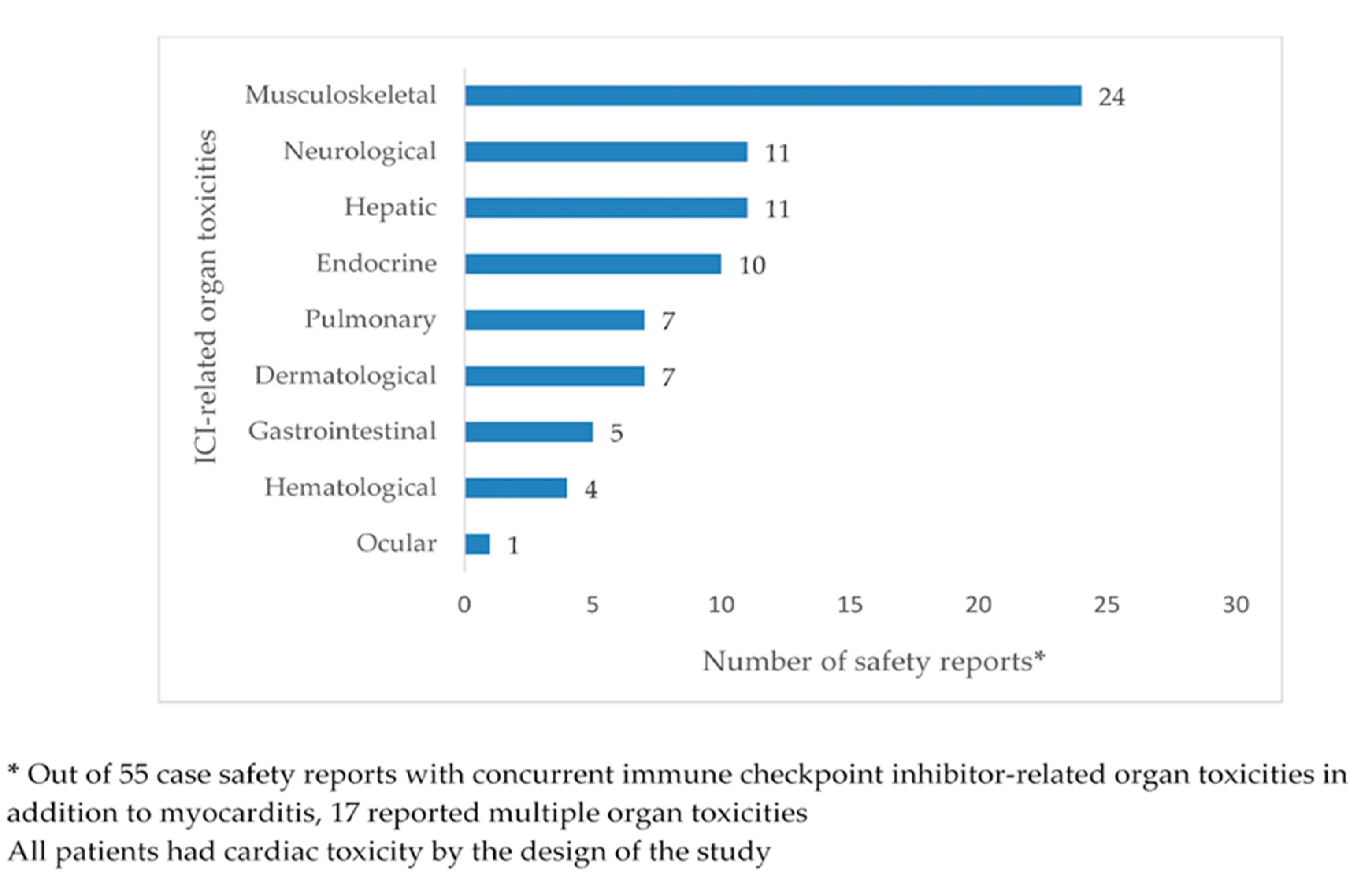
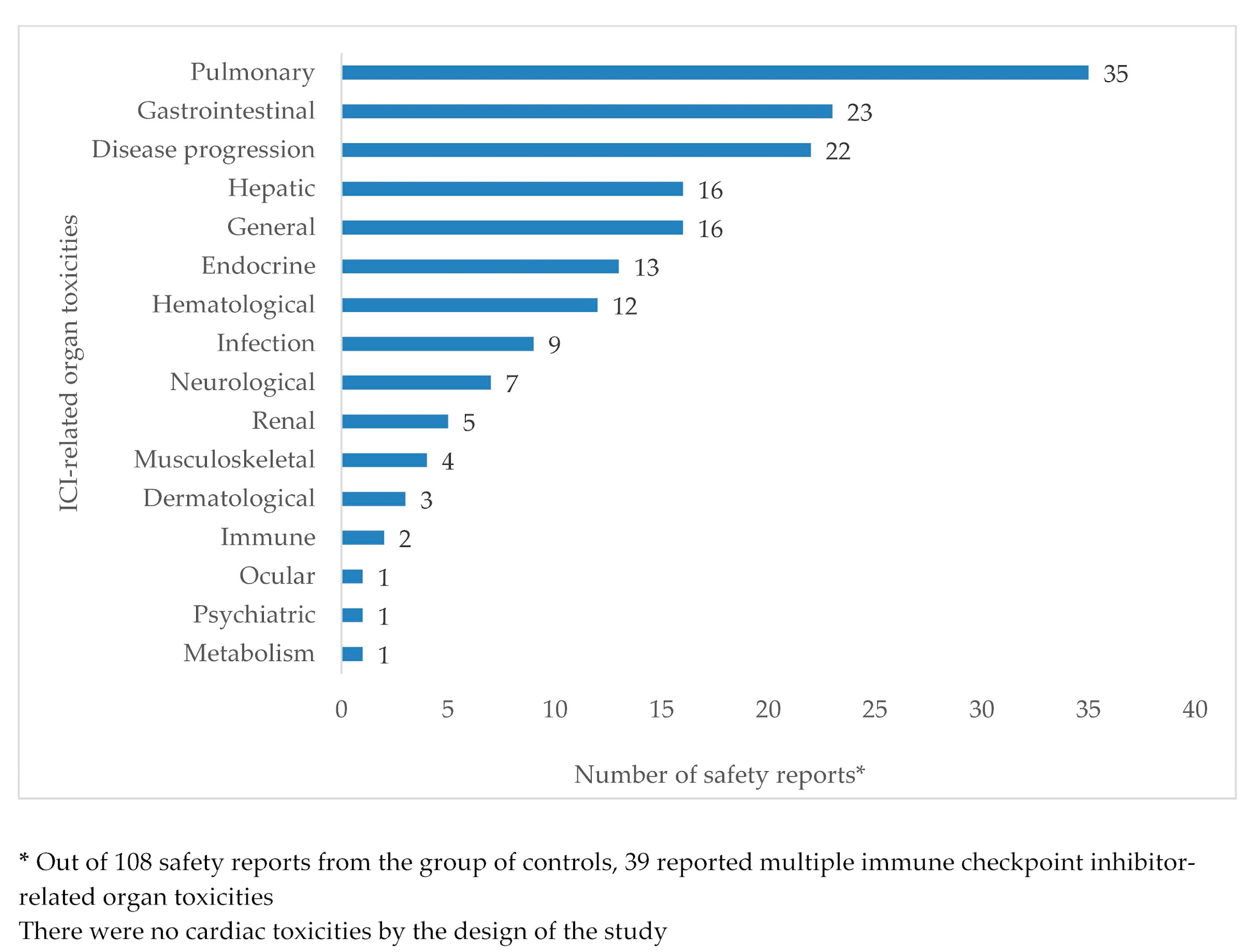
3.1. Safety Report Demographic and Clinical Characteristics
3.2. Statistical Analysis of Association
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Johnson, D.B.; Balko, J.M.; Compton, M.L.; Chalkias, S.; Gorham, J.; Xu, Y.; Hicks, M.; Puzanov, I.; Alexander, M.R.; Bloomer, T.L.; et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N. Engl. J. Med. 2016, 375, 1749–1755. [Google Scholar] [CrossRef] [PubMed]
- Salem, J.-E.; Manouchehri, A.; Moey, M.; Lebrun-Vignes, B.; Bastarache, L.; Pariente, A.; Gobert, A.; Spano, J.-P.; Balko, J.M.; Bonaca, M.P.; et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: An observational, retrospective, pharmacovigilance study. Lancet Oncol. 2018, 19, 1579–1589. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, R.; Nautiyal, A.; Singh, S. Diagnosis of immune checkpoint inhibitor-associated myocarditis: A systematic review. Int. J. Cardiol. 2019, 296, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Veronese, G.; Ammirati, E. Differences in clinical presentation and outcome between immune checkpoint inhibitor-associated myocarditis and classical acute myocarditis: Same disease, distinct challenges to face. Int. J. Cardiol. 2019, 296, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Veronese, G.; Bottiroli, M.; Wang, D.W.; Cipriani, M.; Garascia, A.; Pedrotti, P.; Adler, E.D.; Frigerio, M. Update on acute myocarditis. Trends Cardiovasc. Med. 2020, 2020, 1050. [Google Scholar] [CrossRef]
- Vaddepally, R.K.; Kharel, P.; Pandey, R.; Garje, R.; Chandra, A.B. Review of Indications of FDA-Approved Immune Checkpoint Inhibitors per NCCN Guidelines with the Level of Evidence. Cancers 2020, 12, 738. [Google Scholar] [CrossRef] [Green Version]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in patients treated with immune checkpoint inhibitors. J. Am. Coll Cardiol. 2018, 871, 1755–1764. [Google Scholar]
- Zamami, Y.; Niimura, T.; Okada, N.; Koyama, T.; Fukushima, K.; Izawa-Ishizawa, Y.; Ishizawa, K. Factors Associated with Immune Checkpoint Inhibitor–Related Myocarditis. JAMA Oncol. 2019, 5, 1635–1637. [Google Scholar] [CrossRef]
- Guha, A.; Al-Kindi, S.; Jain, P.; Tashtish, N.; ElAmm, C.; Oliveira, G.H. Association between myocarditis and other immune-related adverse events secondary to immune checkpoint inhibitor use. Int. J. Cancer 2020, 147, 1753–1754. [Google Scholar] [CrossRef]
- Oren, O.; Yang, E.H.; Molina, J.R.; Bailey, K.R.; Blumenthal, R.S.; Kopecky, S.L. Cardiovascular Health and Outcomes in Cancer Patients Receiving Immune Checkpoint Inhibitors. Am. J. Cardiol. 2020, 125, 1920–1926. [Google Scholar] [CrossRef]
- Shah, K.P.; Song, H.; Ye, F.; Moslehi, J.J.; Balko, J.M.; Salem, J.-E.; Johnson, D.B. Demographic Factors Associated with Toxicity in Patients Treated with Anti–Programmed Cell Death-1 Therapy. Cancer Immunol. Res. 2020, 8, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Lagerlund, O.; Strese, S.; Fladvad, M.; Lindquist, M. WHODrug: A Global, Validated and Updated Dictionary for Medicinal Information. Innov. Regul. Sci. 2020, 54, 1116–1122. [Google Scholar] [CrossRef] [Green Version]
- Lindquist, M. VigiBase, the WHO Global ICSR Database System: Basic Facts. Innov. Regul. Sci. 2008, 42, 409–419. [Google Scholar] [CrossRef]
- Chan, K.K.; Bass, A.R. Autoimmune complications of immunotherapy: Pathophysiology and management. BMJ 2020, 369, m736. [Google Scholar] [CrossRef] [Green Version]
- Armitage, P.; Berry, G.; Matthews, J.N.S. Statistical Methods in Medical Research, 4th ed.; Blackwell Science: Oxford, UK, 2002. [Google Scholar]
- Kendall, M.G. Rank Correlation Methods, 4th ed.; Griffin: London, UK, 1976. [Google Scholar]
- Rea, L.M.; Parker, R.A. Designing and Conducting Survey Research; Jossey-Boss: San Francisco, CA, USA, 1992. [Google Scholar]
- Jain, P.; Bugarin, J.G.; Guha, A.; Jain, C.; Shen, T.; Stanevich, I.; Margevicius, S.P.; Fu, P.; Liu, F.; Nikore, V.; et al. Risk factors for myocarditis associated with immune checkpoint inhibitors using real-world clinical data. J. Clin. Oncol. 2020, 38, e15100. [Google Scholar] [CrossRef]
- Spigel, D.R.; McCleod, M.; Jotte, R.M.; Einhorn, L.; Horn, L.; Waterhouse, D.M.; Creelan, B.; Babu, S.; Leighl, N.B.; Chandler, J.C.; et al. Safety, efficacy, and patient-reported health-related quality of life and symptom burden with nivolumab in patients with advanced non-small cell lung cancer, including patients aged 70 years or older or with poor performance status (CheckMate 153). J. Thorac. Oncol. 2019, 14, 1628–1639. [Google Scholar]
- Van Holstein, Y.; Kapiteijn, E.; Bastiaannet, E.; Bos, F.V.D.; Portielje, J.; De Glas, N. Efficacy and Adverse Events of Immunotherapy with Checkpoint Inhibitors in Older Patients with Cancer. Drugs Aging 2019, 36, 927–938. [Google Scholar] [CrossRef] [Green Version]
- Duma, N.; Abdel-Ghani, A.; Yadav, S.; Hoversten, K.P.; Reed, C.T.; Sitek, A.N.; Enninga, E.A.L.; Paludo, J.; Aguilera, J.V.; Leventakos, K.; et al. Sex Differences in Tolerability to Anti-Programmed Cell Death Protein 1 Therapy in Patients with Metastatic Melanoma and Non-Small Cell Lung Cancer: Are We All Equal? Oncologist 2019, 24, e1148–e1155. [Google Scholar] [CrossRef] [Green Version]
- Klein, S.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Khoja, L.; Day, D.; Chen, T.W.-W.; Siu, L.L.; Hansen, A.R. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: A systematic review. Ann. Oncol. 2017, 28, 2377–2385. [Google Scholar] [CrossRef]
- Gu, L.; Khadaroo, P.A.; Su, H.; Kong, L.; Chen, L.; Wang, X.; Li, X.; Zhu, H.; Zhong, X.; Pan, J.; et al. The safety and tolerability of combined immune checkpoint inhibitors (anti-PD-1/PD-L1 plus anti-CTLA-4): A systematic review and meta-analysis. BMC Cancer 2019, 19, 559. [Google Scholar]
- Moslehi, J.J.; Salem, J.-E.; Sosman, J.A.; Lebrun-Vignes, B.; Johnson, D.B. Increased reporting of fatal immune checkpoint inhibitor-associated myocarditis. Lancet 2018, 391, 933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: https://www.fda.gov/safety/medwatch-fda-safety-information-and-adverse-event-reporting-program (accessed on 2 October 2020).
- Conforti, F.; Pala, L.; Bagnardi, V.; De Pas, T.; Martinetti, M.; Viale, G.; Gelber, R.D.; Goldhirsch, A. Cancer immunotherapy efficacy and patients’ sex: A systematic review and meta-analysis. Lancet Oncol. 2018, 19, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.cancer.net/cancer-types/lung-cancer-non-small-cell/statistics (accessed on 2 October 2020).
- Available online: https://www.cancer.net/cancer-types/melanoma/statistics (accessed on 2 October 2020).
- Fryar, C.D.; Chen, T.-C.; Li, X. Prevalence of uncontrolled risk factors for cardiovascular disease: United States, 1999–2010. NCHS Data Brief 2012, 103, 1–8. [Google Scholar] [PubMed]
- Indini, A.; Di Guardo, L.; Cimminiello, C.; Prisciandaro, M.; Randon, G.; De Braud, F.; Del Vecchio, M. Immune-related adverse events correlate with improved survival in patients undergoing anti-PD1 immunotherapy for metastatic melanoma. J. Cancer Res. Clin. Oncol. 2019, 145, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Roberto, G.; Piccinni, C.; D’Alessandro, R.; Poluzzi, E. Triptans and serious adverse vascular events: Data mining of the FDA Adverse Event Reporting System database. Cephalalgia 2013, 34, 5–13. [Google Scholar] [CrossRef]
- Sandberg, L.; Taavola, H.; Aoki, Y.; Chandler, R.; Norén, G.N. Risk Factor Considerations in Statistical Signal Detection: Using Subgroup Disproportionality to Uncover Risk Groups for Adverse Drug Reactions in VigiBase. Drug Saf. 2020, 43, 999–1009. [Google Scholar] [CrossRef]
- Hu, J.-R.; Florido, R.; Lipson, E.J.; Naidoo, J.; Ardehali, R.; Tocchetti, C.G.; Lyon, A.R.; Padera, R.F.; Johnson, D.B.; Moslehi, J. Cardiovascular toxicities associated with immune checkpoint inhibitors. Cardiovasc. Res. 2019, 115, 854–868. [Google Scholar] [CrossRef] [Green Version]
- Pearson, R.K.; Hauben, M.; Goldsmith, D.I.; Gould, A.L.; Madigan, D.; O’Hara, D.J.; Reisinger, S.J.; Hochberg, A.M. Influence of the MedDRA® hierarchy on pharmacovigilance data mining results. Int. J. Med. Inform. 2009, 78, e97–e103. [Google Scholar] [CrossRef]
- Raschi, E.; Mazzarella, A.; Antonazzo, I.C.; Bendinelli, N.; Forcesi, E.; Tuccori, M.; Moretti, U.; Poluzzi, E.; De Ponti, F. Toxicities with Immune Checkpoint Inhibitors: Emerging Priorities from Disproportionality Analysis of the FDA Adverse Event Reporting System. Target. Oncol. 2019, 14, 205–221. [Google Scholar] [CrossRef] [PubMed]
- Raschi, E.; Gatti, M.; Gelsomino, F.; Ardizzoni, A.; Poluzzi, E.; De Ponti, F. Lessons to be Learnt from Real-World Studies on Immune-Related Adverse Events with Checkpoint Inhibitors: A Clinical Perspective from Pharmacovigilance. Target. Oncol. 2020, 15, 449–466. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Cases (n = 108) | Controls (n = 108) |
|---|---|---|
| Patient sex * | ||
| Female | 41 (38.0) | 41 (38.0) |
| Male | 67 (62.0) | 67 (62.0) |
| Patient age * | ||
| <65 years | 42 (38.9) | 42 (38.9) |
| ≥65 years | 66 (61.1) | 66 (61.1) |
| Median (IQR), | 68 (60–74) | 68 (60–74) |
| Range (in years) | 7–83 | 7–83 |
| ICI regimen* | ||
| Anti-CTLA-4 monotherapy | 5 (4.6) | 5 (4.6) |
| ipilimumab | 5 | 5 |
| Anti-PD-1/PD-L1 monotherapy | 75 (69.4) | 75 (69.4) |
| nivolumab | 48 | 48 |
| pembrolizumab | 19 | 19 |
| atezolizumab | 7 | 7 |
| durvalumab | 1 | 1 |
| Combination of anti-CTLA-4 and anti-PD-1/PD-L1 | 28 (25.9) | 28 (25.9) |
| ipilimumab and nivolumab | 25 | 25 |
| ipilimumab and pembrolizumab | 3 | 3 |
| Cancer type * | ||
| Melanoma | 64 (59.3) | 64 (59.3) |
| Non-small cell lung cancer | 44 (40.7) | 44 (40.7) |
| Reporting year | ||
| 2013 | - | 1 (0.9) |
| 2014 | - | 1 (0.9) |
| 2015 | 1 (0.9) | 8 (7.4) |
| 2016 | 8 (7.4) | 18 (16.7) |
| 2017 | 26 (24.1) | 26 (24.1) |
| 2018 | 38 (35.2) | 25 (23.1) |
| 2019 | 35 (32.4) | 29 (26.9) |
| Country of origin | ||
| United States of America | 42 (38.9) | 26 (24.1) |
| Japan | 28 (25.9) | 41 (38.0) |
| European Union | 26 (24.1) | 27 (25.0) |
| Australia | 4 (3.7) | 1 (0.9) |
| United Kingdom | 3 (2.8) | 6 (5.6) |
| Switzerland | 2 (1.9) | - |
| Canada | 2 (1.9) | 6 (5.6) |
| Turkey | 1 (0.9) | - |
| Montenegro | - | 1 (0.9) |
| Type of reporter | ||
| Physician | 68 (63.0) | 74 (68.5) |
| Healthcare professional | 34 (31.5) | 30 (27.8) |
| Pharmacist | 6 (5.6) | 4 (3.7) |
| Seriousness criteria | ||
| Caused or prolonged hospitalization | 35 (32.4) | 53 (49.1) |
| Led to death | 37 (34.3) | 18 (16.7) |
| Was life-threatening | 22 (20.4) | 4 (3.7) |
| Disabled/incapacitated | - | 1 (0.9) |
| Determined other clinically relevant conditions | 14 (13.0) | 32 (29.6) |
| Co-suspected drugs (in addition to ICIs) | ||
| Not reported | 98 (90.7) | 98 (90.7) |
| Reported | 10 (9.3) | 10 (9.3) |
| Median number per safety report (IQR) | 1 (1–1.7) | 1 (1–2.7) |
| ATC L01 Antineoplastic agents | 6 (5.6) | 4 (3.7) |
| Concomitant drugs | ||
| Not reported | 59 (54.6) | 67 (62.0) |
| Reported | 49 (45.4) | 41 (38.0) |
| Median number per safety report (IQR) | 4 (2–8) | 5 (3–9) |
| ATC C1 Cardiovascular system | 30 (27.8) | 17 (15.7) |
| C01 Cardiac therapy | 6 (5.6) | 3 (2.8) |
| C02 Antihypertensives | 3 (2.8) | - |
| C03 Diuretics | 10 (9.3) | 4 (3.7) |
| C04 Peripheral vasodilators | 1 (0.9) | 1 (0.9) |
| C07 Beta blocking agents | 8 (7.4) | 7 (6.5) |
| C08 Calcium channel blockers | 8 (7.4) | 2 (1.9) |
| C09 Agents acting on the renin-angiotensin system | 12 (11.1) | 6 (5.6) |
| C10 Lipid modifying agents | 11 (10.2) | 12 (11.1) |
| ATC A10 Drugs used in diabetes | 5 (4.6) | 7 (6.5) |
| ATC A08 Antiobesity preparations | - | - |
| ATC C and A10 | 5 (4.6) | 6 (5.6) |
| (A). | ||||
| CASES | ||||
| With concomitant drugs of ATC C | Without concomitant drugs of ATC C | Totals | ||
| CONTROLS | With concomitant drugs of ATC C | 9 | 8 | 17 |
| Without concomitant drugs of ATC C | 21 | 70 | 91 | |
| Totals | 30 | 78 | 108 | |
| (B). | ||||
| CASES | ||||
| With concomitant drugs of ATC A10 | Without concomitant drugs of ATC A10 | Totals | ||
| CONTROLS | With concomitant drugs of ATC A10 | 1 | 6 | 7 |
| Without concomitant drugs of ATC A10 | 4 | 97 | 101 | |
| Totals | 5 | 103 | 108 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noseda, R.; Ruinelli, L.; van der Gaag, L.C.; Ceschi, A. Pre-Existing Cardiovascular Conditions as Clinical Predictors of Myocarditis Reporting with Immune Checkpoint Inhibitors: A VigiBase Study. Cancers 2020, 12, 3480. https://doi.org/10.3390/cancers12113480
Noseda R, Ruinelli L, van der Gaag LC, Ceschi A. Pre-Existing Cardiovascular Conditions as Clinical Predictors of Myocarditis Reporting with Immune Checkpoint Inhibitors: A VigiBase Study. Cancers. 2020; 12(11):3480. https://doi.org/10.3390/cancers12113480
Chicago/Turabian StyleNoseda, Roberta, Lorenzo Ruinelli, Linda C. van der Gaag, and Alessandro Ceschi. 2020. "Pre-Existing Cardiovascular Conditions as Clinical Predictors of Myocarditis Reporting with Immune Checkpoint Inhibitors: A VigiBase Study" Cancers 12, no. 11: 3480. https://doi.org/10.3390/cancers12113480