Prognostic Role of Non-Identification of Sentinel Lymph Node in Cutaneous Melanoma Patients: An Observational Retrospective Study

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
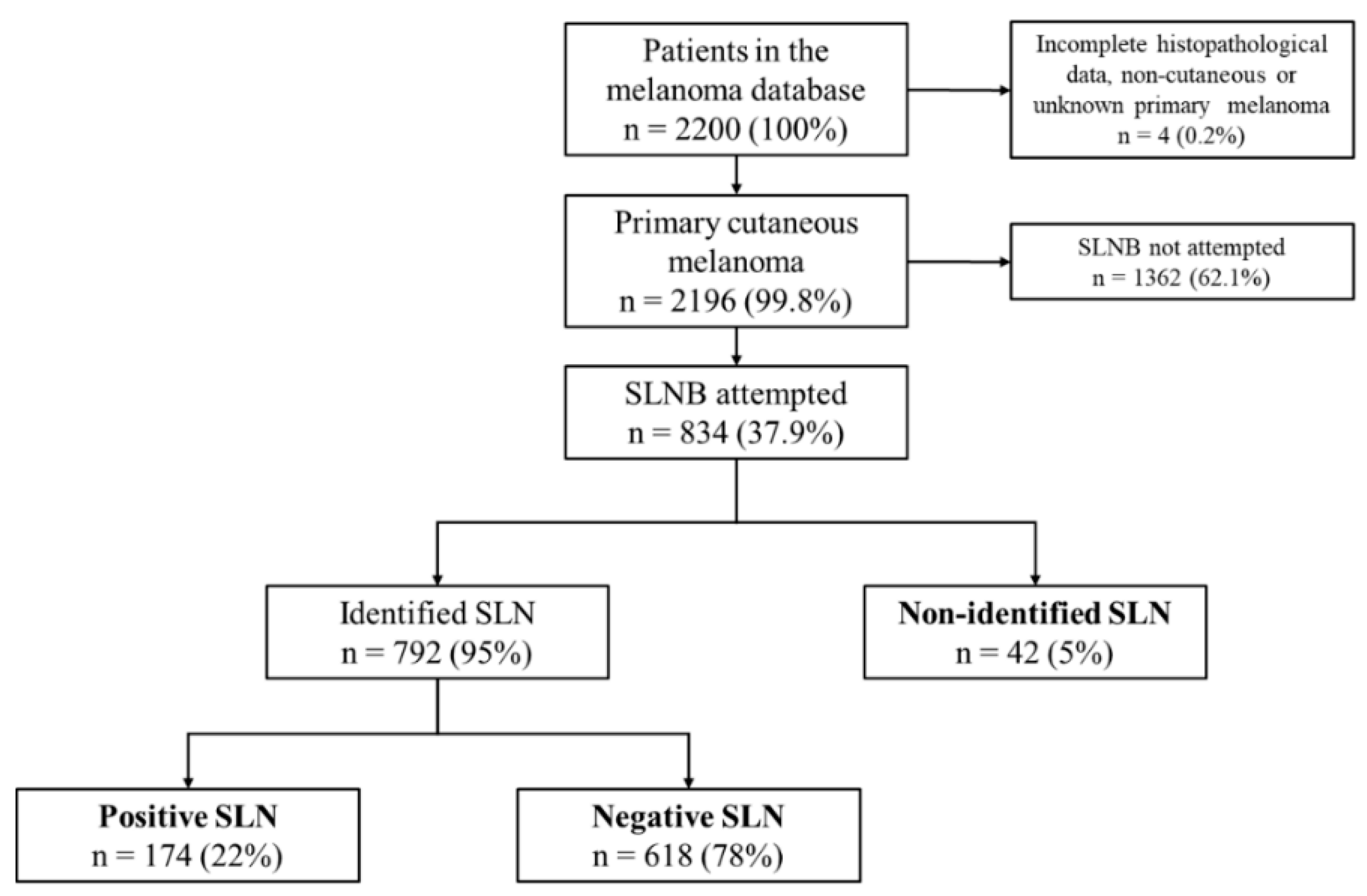
2.1. Patient Characteristics
2.2. SLN Identification
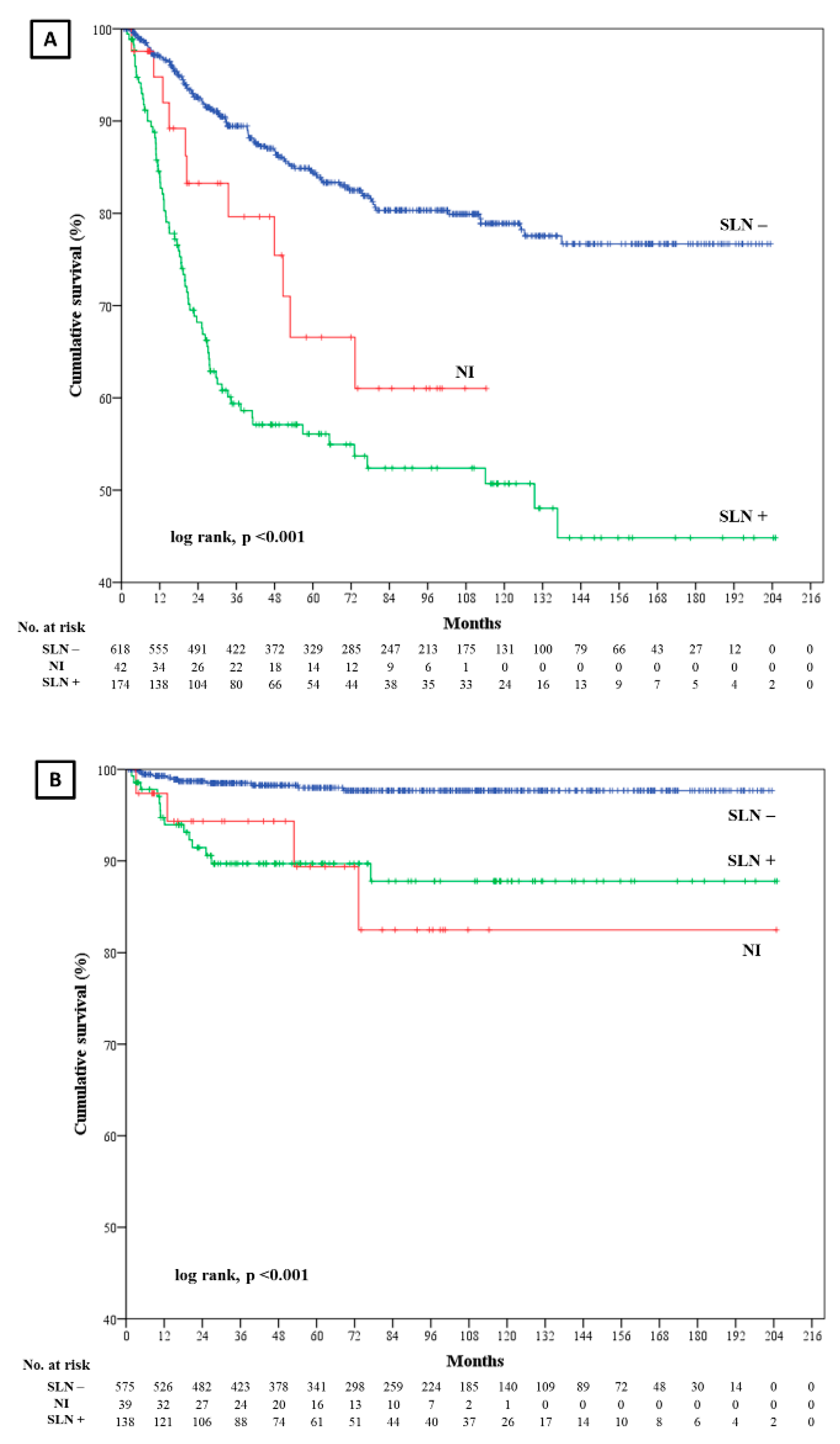
2.3. Disease Free Survival (DFS)
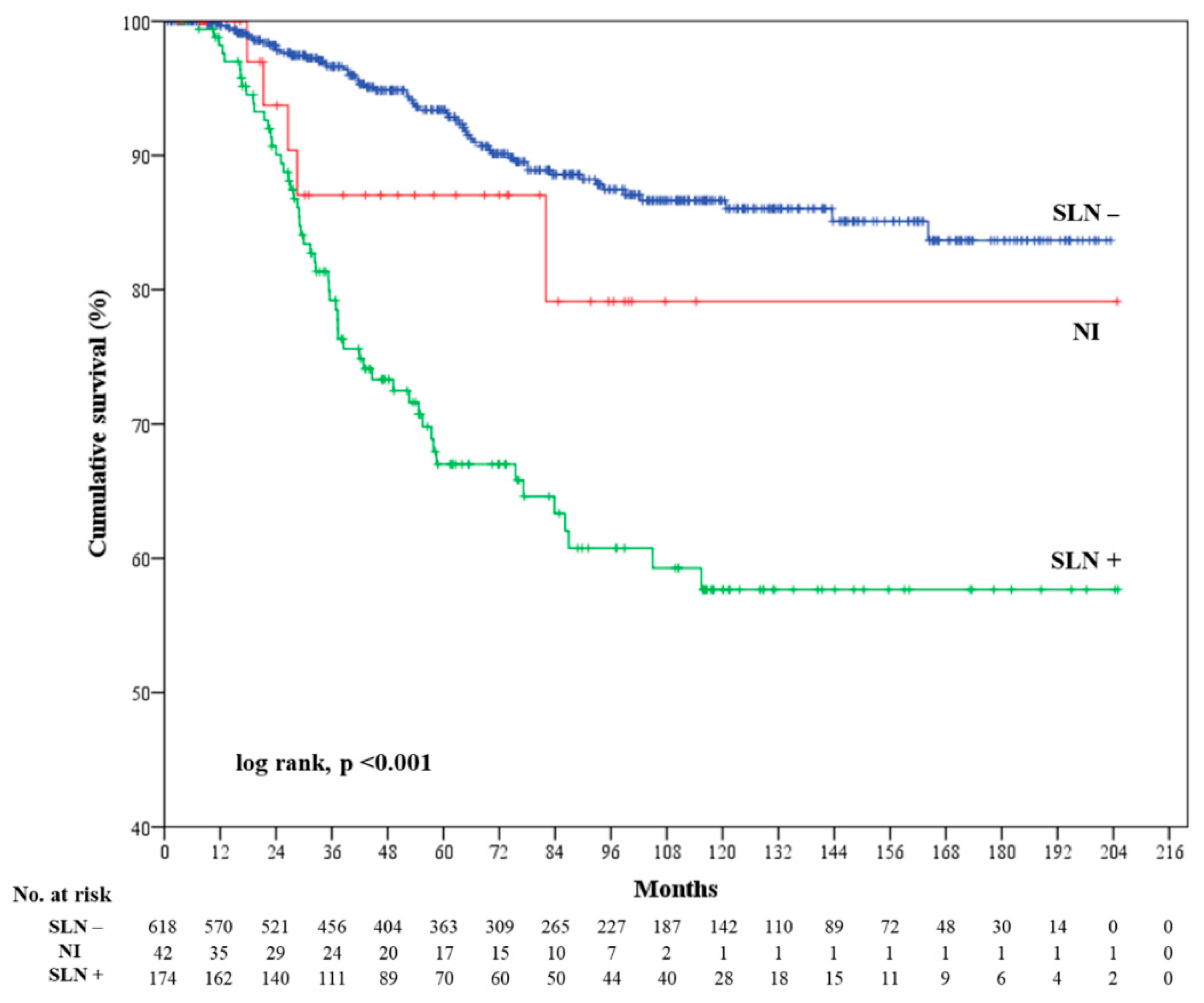
2.4. Melanoma Specific Survival (MSS)
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Lymphoscintigraphy Procedure
4.3. SLNB Procedure
4.4. Statistical Analysis
4.5. Ethics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Balch, C.M.; Gershenwald, J.E.; Soong, S.J.; Thompson, J.F.; Atkins, M.B.; Byrd, D.R.; Buzaid, A.C.; Cochran, A.J.; Coit, D.G.; Ding, S.; et al. Final version of 2009 AJCC melanoma staging and classification. J. Clin. Oncol. 2009, 27, 6199–6206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Comprehensive Cancer Network. Cutaneous Melanoma (Version 3.2020). Available online: https://www.nccn.org/professionals/physician_gls/pdf/cutaneous_melanoma.pdf (accessed on 2 June 2020).
- De Rosa, N.; Lyman, G.H.; Silbermins, D.; Valsecchi, M.E.; Pruitt, S.K.; Tyler, D.M.; Lee, W.T. Sentinel node biopsy for head and neck melanoma: A systematic review. Otolaryngol. Head Neck Surg. 2011, 145, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Morton, D.L.; Cochran, A.J.; Thompson, J.F.; Elashoff, R.; Essner, R.; Glass, E.C.; Mozzillo, N.; Nieweg, O.E.; Roses, D.F.; Hoekstra, H.J.; et al. Sentinel node biopsy for early-stage melanoma: Accuracy and morbidity in MSLT-I, an international multicenter trial. Ann. Surg. 2005, 242, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Valsecchi, M.E.; Silbermins, D.; de Rosa, N.; Wong, S.L.; Lyman, G.H. Lymphatic mapping and sentinel lymph node biopsy in patients with melanoma: A meta-analysis. J. Clin. Oncol. 2011, 29, 1479–1487. [Google Scholar] [CrossRef]
- Vidal-Sicart, S.; Pons, F.; Puig, S.; Ortega, M.; Vilalta, A.; Martin, F.; Rull, R.; Palou, J.M.; Castel, T. Identification of the sentinel lymph node in patients with malignant melanoma: What are the reasons for mistakes? Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 362–366. [Google Scholar] [CrossRef]
- Zlotnik, O.; Bernstine, H.; Domachevsky, L.; Gutman, H. Failure to identify sentinel lymph nodes for malignant melanoma—Outcome after over 10 years median follow up. Eur. J. Surg. Oncol. 2019, 45, 231–234. [Google Scholar] [CrossRef]
- Pavri, S.N.; Gary, C.; Martinez, R.S.; Kim, S.; Han, D.; Ariyan, S.; Narayan, D. Nonvisualization of Sentinel Lymph Nodes by Lymphoscintigraphy in Primary Cutaneous Melanoma: Incidence, Risk Factors, and a Review of Management Options. Plast. Reconstr. Surg. 2018, 142, 527e–534e. [Google Scholar] [CrossRef] [PubMed]
- Schuitevoerder, D.; Grinlington, L.; Stevens, J.; Nance, R.; Fortino, J.; Vetto, J.T. Nonvisualized sentinel lymph nodes on lymphoscintigraphy in melanoma: Predictive factors and surgical outcomes. Nucl. Med. Commun. 2017, 38, 383–387. [Google Scholar] [CrossRef]
- Moro, R.; Gonzalez-Ramos, J.; Martinez-Garcia, S.; Requena, C.; Traves, V.; Manrique-Silva, E.; Nagore, E. Locoregional Lymph Node Recurrence of Trunk Melanoma in Non-sentinel Lymph Node Basins: An Observational Retrospective Study. Acta Derm Venereol. 2020, 100, adv00284. [Google Scholar] [CrossRef] [PubMed]
- Boada, A.; Tejera-Vaquerizo, A.; Ribero, S.; Puig, S.; Moreno-Ramirez, D.; Descalzo-Gallego, M.A.; Fierro, M.T.; Quaglino, P.; Carrera, C.; Malvehy, J.; et al. Sentinel lymph node biopsy versus observation in thick melanoma: A multicenter propensity score matching study. Int. J. Cancer 2018, 142, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Morera-Sendra, N.; Tejera-Vaquerizo, A.; Traves, V.; Requena, C.; Bolumar, I.; Pla, A.; Vazquez, C.; Soriano, V.; Nagore, E. Value of sentinel lymph node biopsy and adjuvant interferon treatment in thick (>4 mm) cutaneous melanoma: An observational study. Eur. J. Derm. 2016, 26, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Ribero, S.; Osella-Abate, S.; Sanlorenzo, M.; Balagna, E.; Senetta, R.; Fierro, M.T.; Macripo, G.; Macri, L.; Sapino, A.; Quaglino, P. Sentinel Lymph Node Biopsy in Thick-Melanoma Patients (N = 350): What is Its Prognostic Role? Ann. Surg. Oncol. 2015, 22, 1967–1973. [Google Scholar] [CrossRef]
- Chakera, A.H.; Friis, E.; Hesse, U.; Al-Suliman, N.; Zerahn, B.; Hesse, B. Factors of importance for scintigraphic non-visualisation of sentinel nodes in breast cancer. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Cox, C.E.; Dupont, E.; Whitehead, G.F.; Ebert, M.D.; Nguyen, K.; Peltz, E.S.; Peckham, D.; Cantor, A.; Reintgen, D.S. Age and body mass index may increase the chance of failure in sentinel lymph node biopsy for women with breast cancer. Breast J. 2002, 8, 88–91. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Kruper, L.; Dieli-Conwright, C.M.; Mortimer, J.E. The Impact of Obesity on Breast Cancer Diagnosis and Treatment. Curr. Oncol. Rep. 2019, 21, 41. [Google Scholar] [CrossRef] [Green Version]
- Buckle, T.; KleinJan, G.H.; Engelen, T.; van den Berg, N.S.; DeRuiter, M.C.; van der Heide, U.; Valdes Olmos, R.A.; Webb, A.; van Buchem, M.A.; Balm, A.J.; et al. Diffusion-weighted-preparation (D-prep) MRI as a future extension of SPECT/CT based surgical planning for sentinel node procedures in the head and neck area? Oral Oncol. 2016, 60, 48–54. [Google Scholar] [CrossRef]
- Stoffels, I.; Boy, C.; Poppel, T.; Kuhn, J.; Klotgen, K.; Dissemond, J.; Schadendorf, D.; Klode, J. Association between sentinel lymph node excision with or without preoperative SPECT/CT and metastatic node detection and disease-free survival in melanoma. JAMA 2012, 308, 1007–1014. [Google Scholar] [CrossRef]
- Trinh, B.B.; Chapman, B.C.; Gleisner, A.; Kwak, J.J.; Morgan, R.; McCarter, M.D.; Gajdos, C.; Kounalakis, N. SPECT/CT Adds Distinct Lymph Node Basins and Influences Radiologic Findings and Surgical Approach for Sentinel Lymph Node Biopsy in Head and Neck Melanoma. Ann. Surg. Oncol. 2018, 25, 1716–1722. [Google Scholar] [CrossRef]
- Faries, M.B.; Thompson, J.F.; Cochran, A.J.; Andtbacka, R.H.; Mozzillo, N.; Zager, J.S.; Jahkola, T.; Bowles, T.L.; Testori, A.; Beitsch, P.D.; et al. Completion Dissection or Observation for Sentinel-Node Metastasis in Melanoma. N. Engl. J. Med. 2017, 376, 2211–2222. [Google Scholar] [CrossRef]
- Kyrgidis, A.; Tzellos, T.; Mocellin, S.; Apalla, Z.; Lallas, A.; Pilati, P.; Stratigos, A. Sentinel lymph node biopsy followed by lymph node dissection for localised primary cutaneous melanoma. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Macedo, F.I.; Fayne, R.A.; Azab, B.; Yakoub, D.; Moller, M.G. The Role of Completion Lymphadenectomy in Positive Regional Lymph Nodes in Melanoma: A Meta-analysis. J. Surg. Res. 2019, 236, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Long, X. Nonvisualization of Sentinel Lymph Nodes by Lymphoscintigraphy in Primary Cutaneous Melanoma: Incidence, Risk Factors, and a Review of Management Options. Plast. Reconstr. Surg. 2019, 144, 148e–149e. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B. Multiple Imputation for Nonresponse in Surveys; Wiley: New York, NY, USA, 1987. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Overall Population | Identified SLN | Non-Identified SLN | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | +SLN | −SLN | ||||||||||
| n | % | n | % | n | % | n | % | n | % | p * | p ** | |
| Age at diagnosis (m.v. = 0) | <0.001 | <0.001 | ||||||||||
| <64 years old | 549 | 65.8 | 532 | 67.2 | 108 | 62.1 | 424 | 68.6 | 17 | 40.5 | ||
| ≥64 years old | 285 | 34.2 | 260 | 32.8 | 66 | 37.9 | 194 | 31.4 | 25 | 59.5 | ||
| Gender (m.v. = 0) | 0.75 | 0.54 | ||||||||||
| Male | 439 | 52.6 | 418 | 52.8 | 98 | 56.3 | 320 | 51.8 | 21 | 50 | ||
| Female | 395 | 47.2 | 418 | 47.2 | 76 | 43.7 | 298 | 48.2 | 21 | 50 | ||
| BMI (m.v. = 240) | 0.007 | 0.025 | ||||||||||
| <30 | 476 | 80.1 | 457 | 81.2 | 89 | 80.2 | 368 | 81.4 | 19 | 61.3 | ||
| ≥30 | 118 | 19.9 | 106 | 18.8 | 22 | 19.8 | 84 | 18.6 | 12 | 38.7 | ||
| Anatomical loc. (m.v. = 0) | 0.80 | <0.001 | ||||||||||
| Head/neck | 127 | 15.2 | 103 | 13 | 15 | 8.6 | 88 | 14.2 | 24 | 57.1 | ||
| Upper extremities | 121 | 14.5 | 114 | 14.4 | 24 | 13.8 | 90 | 14.6 | 7 | 16.7 | ||
| Trunk | 337 | 40.4 | 330 | 41.7 | 79 | 45.4 | 251 | 40.6 | 7 | 16.7 | ||
| Lower extremities | 163 | 19.5 | 160 | 20.2 | 29 | 16.7 | 131 | 21.2 | 3 | 7.1 | ||
| Acral | 86 | 10.3 | 85 | 10.7 | 27 | 15.5 | 58 | 9.4 | 1 | 2.4 | ||
| Histological type (m.v. = 0) | <0.001 | <0.001 | ||||||||||
| Lentigo maligna melanoma | 32 | 3.8 | 24 | 3 | 0 | 0 | 24 | 3.9 | 8 | 19 | ||
| Superficial spreading | 474 | 56.8 | 452 | 57.1 | 80 | 46 | 372 | 60.2 | 22 | 52.4 | ||
| Nodular | 221 | 26.5 | 211 | 26.6 | 72 | 41.4 | 139 | 22.5 | 10 | 23.8 | ||
| Acral | 45 | 5.4 | 44 | 5.6 | 13 | 7.5 | 31 | 5 | 1 | 2.4 | ||
| Other/not specified | 62 | 7.4 | 61 | 7.7 | 9 | 5.2 | 52 | 8.4 | 1 | 2.4 | ||
| Breslow thickness (m.v. = 0) | 0.61 | <0.001 | ||||||||||
| ≤1.00 mm | 225 | 27.0 | 217 | 27.4 | 13 | 7.5 | 204 | 33 | 8 | 19.0 | ||
| 1.01–2.00 mm | 297 | 35.6 | 282 | 35.6 | 45 | 25.9 | 237 | 38.3 | 15 | 35.7 | ||
| 2.01–4.00 mm | 189 | 22.7 | 178 | 22.5 | 68 | 39.1 | 110 | 17.8 | 11 | 26.2 | ||
| >4.00 mm | 123 | 14.7 | 115 | 14.5 | 48 | 19 | 67 | 10.8 | 8 | 19.0 | ||
| Ulceration (m.v. = 23) | 0.92 | <0.001 | ||||||||||
| Present | 226 | 27.9 | 214 | 27.8 | 94 | 55.3 | 461 | 77 | 12 | 28.6 | ||
| Absent | 585 | 72.1 | 555 | 72.2 | 76 | 44.7 | 138 | 23 | 30 | 71.4 | ||
| Mitotic index (m.v. = 211) | 0.45 | <0.001 | ||||||||||
| ≤2 mit/mm2 | 350 | 56.2 | 331 | 56.5 | 43 | 32.8 | 288 | 63.3 | 19 | 51.4 | ||
| >2 mit/mm2 | 273 | 43.8 | 255 | 43.5 | 88 | 67.2 | 167 | 36.7 | 19 | 48.6 | ||
| Microscopic satellites (m.v. = 66) | 0.36 | 0.52 | ||||||||||
| Absent | 745 | 97 | 705 | 97.1 | 153 | 96.8 | 552 | 97.2 | 40 | 95.2 | ||
| Present | 23 | 3 | 21 | 2.9 | 5 | 3.2 | 16 | 2.8 | 2 | 4.8 | ||
| Vascular invasion (m.v. = 66) | 0.64 | 0.01 | ||||||||||
| Absent | 743 | 96.7 | 703 | 96.8 | 146 | 93 | 557 | 97.9 | 40 | 95.2 | ||
| Present | 25 | 3.3 | 23 | 3.2 | 11 | 7 | 12 | 2.1 | 2 | 4.8 | ||
| Regression (m.v. = 66) | 0.37 | 0.02 | ||||||||||
| Absent | 641 | 86.6 | 604 | 86.4 | 139 | 93.3 | 465 | 84.5 | 37 | 90.2 | ||
| Present | 99 | 13.4 | 95 | 13.6 | 10 | 6.7 | 85 | 15.5 | 4 | 9.8 | ||
| Univariate | Multivariate with BMI * | Multivariate without BMI | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | CI 95% | p | OR | CI 95% | p | OR | CI 95% | p | |
| Age at diagnosis | |||||||||
| <64 years | Ref. | Ref. | - | Ref. | Ref. | - | Ref. | Ref. | - |
| ≥64 years | 3.0 | 1.6–5.7 | 0.001 | 2.9 | 1.3–6.6 | 0.009 | 2.2 | 1.1–4.2 | 0.021 |
| BMI | |||||||||
| <30 | Ref. | Ref. | - | Ref. | Ref. | - | - | - | - |
| ≥30 | 2.7 | 1.3–5.8 | 0.009 | 3.8 | 1.6–9.0 | 0.002 | - | - | - |
| Anatomical localization | |||||||||
| Head/neck | 12.2 | 5.8–25.6 | <0.001 | 17.5 | 7.1–43.1 | <0.001 | 12.2 | 5.8–25.6 | <0.001 |
| Upper extremities | 3.2 | 1.2–8.5 | 0.018 | 2.8 | 0.8–9.7 | 0.111 | 3.2 | 1.2–8.5 | 0.018 |
| Other location | Ref. | Ref. | - | Ref. | Ref. | - | Ref. | Ref. | - |
| Histological type | |||||||||
| LMM | 7.5 | 3.2–18.0 | <0.001 | - | - | - | - | - | - |
| Non-LMM | Ref. | - | - | - | - | - | - | - | |
| Nodal DFS | MSS | |||||
|---|---|---|---|---|---|---|
| HR | CI 95% | p | HR | CI 95% | p | |
| SLN | ||||||
| Negative | Ref. | Ref. | - | Ref. | Ref. | - |
| Positive | 3.2 | 1.4–7.5 | 0.006 | 2.9 | 1.9–4.3 | <0.001 |
| Non-identified | 5.1 | 1.6–16.2 | 0.006 | 1.2 | 0.5–3.1 | 0.665 |
| Breslow | ||||||
| <2 mm | Ref. | Ref. | - | Ref. | Ref. | - |
| ≥2 mm | 4.2 | 1.7–10.4 | 0.002 | 3.2 | 2.0–4.7 | <0.001 |
| Vascular invasion | ||||||
| Absent | Ref. | Ref. | - | - | - | - |
| Present | 3.7 | 1.2–11.2 | 0.022 | - | - | - |
| Age at diagnosis | ||||||
| <64 years | - | - | - | Ref. | Ref. | - |
| ≥64 years | - | - | - | 2.3 | 1.6–3.3 | <0.001 |
| Microscopic satellites | ||||||
| Absent | - | - | - | Ref. | Ref. | - |
| Present | - | - | - | 2.7 | 1.3–5.7 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moro, R.; Arjona-Aguilera, C.; Requena, C.; Pont-Sanjuan, V.; Traves, V.; Manrique-Silva, E.; Nagore, E. Prognostic Role of Non-Identification of Sentinel Lymph Node in Cutaneous Melanoma Patients: An Observational Retrospective Study. Cancers 2020, 12, 3151. https://doi.org/10.3390/cancers12113151
Moro R, Arjona-Aguilera C, Requena C, Pont-Sanjuan V, Traves V, Manrique-Silva E, Nagore E. Prognostic Role of Non-Identification of Sentinel Lymph Node in Cutaneous Melanoma Patients: An Observational Retrospective Study. Cancers. 2020; 12(11):3151. https://doi.org/10.3390/cancers12113151
Chicago/Turabian StyleMoro, Ruggero, Cintia Arjona-Aguilera, Celia Requena, Virginia Pont-Sanjuan, Victor Traves, Esperanza Manrique-Silva, and Eduardo Nagore. 2020. "Prognostic Role of Non-Identification of Sentinel Lymph Node in Cutaneous Melanoma Patients: An Observational Retrospective Study" Cancers 12, no. 11: 3151. https://doi.org/10.3390/cancers12113151