Cytoreductive Surgery for Heavily Pre-Treated, Platinum-Resistant Epithelial Ovarian Carcinoma: A Two-Center Retrospective Experience

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Institutional Review Board (IRB) Approval
2.2. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- SEER. Surveillance, Epidemiology and End Results Program. Available online: https://seer.cancer.gov/statfacts/html/ovary.html (accessed on 1 June 2020).
- Brand, A.H.; DiSilvestro, P.A.; Sehouli, J.; Berek, J.S. Cytoreductive surgery for ovarian cancer: Quality assessment. Ann. Oncol. 2017, 28, viii25–viii29. [Google Scholar] [CrossRef] [PubMed]
- Polterauer, S.; Vergote, I.; Concin, N.; Braicu, I.; Chekerov, R.; Mahner, S.; Woelber, L.; Cadron, I.; Van Gorp, T.; Zeillinger, R.; et al. Prognostic value of residual tumor size in patients with epithelial ovarian cancer FIGO stages IIA-IV: Analysis of the OVCAD data. Int. J. Gynecol. Cancer 2012, 22, 380–385. [Google Scholar] [CrossRef] [PubMed]
- Sehouli, J.; Senyuva, F.; Fotopoulou, C.; Neumann, U.; Denkert, C.; Werner, L.; Gülten, O.O. Intra-abdominal tumor dissemination pattern and surgical outcome in 214 patients with primary ovarian cancer. J. Surg. Oncol. 2009, 99, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Colombo, N.; Sessa, C.; du Bois, A.; Ledermann, J.; McCluggage, W.G.; McNeish, I.; Morice, P.; Pignata, S.; Ray-Coquard, I.; Vergote, I.; et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: Pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Ann. Oncol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Bois, A.D.; Vergote, I.; Ferron, G.; Reuss, A.; Meier, W.; Greggi, S.; Jensen, P.T.; Selle, F.; Guyon, F.; Pomel, C.; et al. Randomized controlled phase III study evaluating the impact of secondary cytoreductive surgery in recurrent ovarian cancer: AGO DESKTOP III/ENGOT ov20. J. Clin. Oncol. 2017, 35. [Google Scholar] [CrossRef]
- Bois, A.D.; Sehouli, J.; Vergote, I.; Ferron, G.; Reuss, A.; Meier, W.; Greggi, S.; Jensen, P.T.; Selle, F.; Guyon, F.; et al. Randomized phase III study to evaluate the impact of secondary cytoreductive surgery in recurrent ovarian cancer: Final analysis of AGO DESKTOP III/ENGOT-ov20. JCO 2020, 38. [Google Scholar] [CrossRef]
- Coleman, R.L.; Brady, M.F.; Herzog, T.J.; Sabbatini, P.; Armstrong, D.K.; Walker, J.L.; Kim, B.G.; Fujiwara, K.; Tewari, K.S.; O’Malley, D.M.; et al. Bevacizumab and paclitaxel-carboplatin chemotherapy and secondary cytoreduction in recurrent, platinum-sensitive ovarian cancer (NRG Oncology/Gynecologic Oncology Group study GOG-0213): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2017, 18, 779–791. [Google Scholar] [CrossRef] [Green Version]
- Coleman, R.L.; Spirtos, N.M.; Enserro, D.; Herzog, T.J.; Sabbatini, P.; Armstrong, D.K.; Kim, J.W.; Park, S.Y.; Kim, B.G.; Nam, J.H.; et al. Secondary Surgical Cytoreduction for Recurrent Ovarian Cancer. N. Engl. J. Med. 2019, 381, 1929–1939. [Google Scholar] [CrossRef]
- Fotopoulou, C.; Savvatis, K.; Kosian, P.; Braicu, I.E.; Papanikolaou, G.; Pietzner, K.; Schmidt, S.C.; Sehouli, J. Quaternary cytoreductive surgery in ovarian cancer: Does surgical effort still matter? Br. J. Cancer 2013, 108, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Fotopoulou, C.; Richter, R.; Braicu, I.E.; Schmidt, S.C.; Neuhaus, P.; Lichtenegger, W.; Sehouli, J. Clinical outcome of tertiary surgical cytoreduction in patients with recurrent epithelial ovarian cancer. Ann. Surg. Oncol. 2011, 18, 49–57. [Google Scholar] [CrossRef]
- Fotopoulou, C.; Zang, R.; Gultekin, M.; Cibula, D.; Ayhan, A.; Liu, D.; Richter, R.; Braicu, I.; Mahner, S.; Harter, P.; et al. Value of tertiary cytoreductive surgery in epithelial ovarian cancer: An international multicenter evaluation. Ann. Surg. Oncol. 2013, 20, 1348–1354. [Google Scholar] [CrossRef] [PubMed]
- Gultekin, M.; Velipaşaoğlu, M.; Aksan, G.; Dursun, P.; Dogan, N.U.; Yuce, K.; Ayhan, A. A third evaluation of tertiary cytoreduction. J. Surg. Oncol. 2008, 98, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Hızlı, D.; Boran, N.; Yılmaz, S.; Turan, T.; Altınbaş, S.K.; Celik, B.; Köse, M.F. Best predictors of survival outcome after tertiary cytoreduction in patients with recurrent platinum-sensitive epithelial ovarian cancer. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 163, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Shih, K.K.; Chi, D.S.; Barakat, R.R.; Leitao, M.M. Beyond tertiary cytoreduction in patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer. Gynecol. Oncol. 2010, 116, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.; Gershenson, D.M.; Wharton, J.T. Secondary cytoreductive surgery in epithelial ovarian cancer: Nonresponders to first-line therapy. Gynecol. Oncol. 1989, 33, 1–5. [Google Scholar] [CrossRef]
- Petrillo, M.; Pedone Anchora, L.; Tortorella, L.; Fanfani, F.; Gallotta, V.; Pacciani, M.; Scambia, G.; Fagotti, A. Secondary cytoreductive surgery in patients with isolated platinum-resistant recurrent ovarian cancer: A retrospective analysis. Gynecol. Oncol. 2014, 134, 257–261. [Google Scholar] [CrossRef]
- Musella, A.; Marchetti, C.; Palaia, I.; Perniola, G.; Giorgini, M.; Lecce, F.; Vertechy, L.; Iadarola, R.; De Felice, F.; Monti, M.; et al. Secondary Cytoreduction in Platinum-Resistant Recurrent Ovarian Cancer: A Single-Institution Experience. Ann. Surg. Oncol. 2015, 22, 4211–4216. [Google Scholar] [CrossRef]
- Hatem, M.E.; Williams, S.; Huss, H.T.; Samuel, C.B.; Flynn, R.; del Priore, G.; Gupta, D.; Taha, M.; David, A.L.; Markman, M.; et al. Cytoreductive surgery (CRC) and heated intraperitoneal chemotherapy (HIPEC) in patients with platinum resistant epithelial ovarian cancer (PROC). J. Clin. Oncol. 2015, 33. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P.H. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat. Res. 1996, 82, 359–374. [Google Scholar]
- Lampe, B.; Kroll, N.; Piso, P.; Forner, D.M.; Mallmann, P. Prognostic significance of Sugarbaker’s peritoneal cancer index for the operability of ovarian carcinoma. Int. J. Gynecol. Cancer 2015, 25, 135–144. [Google Scholar] [CrossRef]
- Chéreau, E.; Ballester, M.; Selle, F.; Cortez, A.; Daraï, E.; Rouzier, R. Comparison of peritoneal carcinomatosis scoring methods in predicting resectability and prognosis in advanced ovarian cancer. Am. J. Obstet. Gynecol. 2010, 202, 178.e1–178.e10. [Google Scholar] [CrossRef] [PubMed]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]
- Eisenkop, S.M.; Friedman, R.L.; Spirtos, N.M. The role of secondary cytoreductive surgery in the treatment of patients with recurrent epithelial ovarian carcinoma. Cancer 2000, 88, 144–153. [Google Scholar] [CrossRef]
- Gronlund, B.; Lundvall, L.; Christensen, I.J.; Knudsen, J.B.; Høgdall, C. Surgical cytoreduction in recurrent ovarian carcinoma in patients with complete response to paclitaxel-platinum. Eur. J. Surg. Oncol. 2005, 31, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Jänicke, F.; Hölscher, M.; Kuhn, W.; von Hugo, R.; Pache, L.; Siewert, J.R.; Graeff, H. Radical surgical procedure improves survival time in patients with recurrent ovarian cancer. Cancer 1992, 70, 2129–2136. [Google Scholar] [CrossRef]
- Sehouli, J.; Richter, R.; Braicu, E.I.; Bühling, K.J.; Bahra, M.; Neuhaus, P.; Lichtenegger, W.; Fotopoulou, C. Role of secondary cytoreductive surgery in ovarian cancer relapse: Who will benefit? A systematic analysis of 240 consecutive patients. J. Surg. Oncol. 2010, 102, 656–662. [Google Scholar] [CrossRef]
- Leitao, M.M.; Kardos, S.; Barakat, R.R.; Chi, D.S. Tertiary cytoreduction in patients with recurrent ovarian carcinoma. Gynecol. Oncol. 2004, 95, 181–188. [Google Scholar] [CrossRef]
- Scarabelli, C.; Gallo, A.; Carbone, A. Secondary cytoreductive surgery for patients with recurrent epithelial ovarian carcinoma. Gynecol. Oncol. 2001, 83, 504–512. [Google Scholar] [CrossRef]
- Harter, P.; du Bois, A.; Hahmann, M.; Hasenburg, A.; Burges, A.; Loibl, S.; Gropp, M.; Huober, J.; Fink, D.; Schröder, W.; et al. Surgery in recurrent ovarian cancer: The Arbeitsgemeinschaft Gynaekologische Onkologie (AGO) DESKTOP OVAR trial. Ann. Surg. Oncol. 2006, 13, 1702–1710. [Google Scholar] [CrossRef]
- Harter, P.; Sehouli, J.; Reuss, A.; Hasenburg, A.; Scambia, G.; Cibula, D.; Mahner, S.; Vergote, I.; Reinthaller, A.; Burges, A.; et al. Prospective validation study of a predictive score for operability of recurrent ovarian cancer: The Multicenter Intergroup Study DESKTOP II. A project of the AGO Kommission OVAR, AGO Study Group, NOGGO, AGO-Austria, and MITO. Int. J. Gynecol. Cancer 2011, 21, 289–295. [Google Scholar] [CrossRef]
- Bristow, R.E. Surgical standards in the management of ovarian cancer. Curr. Opin. Oncol. 2000, 12, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Gadducci, A.; Iacconi, P.; Cosio, S.; Fanucchi, A.; Cristofani, R.; Riccardo Genazzani, A. Complete salvage surgical cytoreduction improves further survival of patients with late recurrent ovarian cancer. Gynecol. Oncol. 2000, 79, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Pfisterer, J.; Harter, P.; Canzler, U.; Richter, B.; Jackisch, C.; Hahmann, M.; Hasenburg, A.; Burges, A.; Loibl, S.; Gropp, M.; et al. The role of surgery in recurrent ovarian cancer. Int. J. Gynecol. Cancer 2005, 15 (Suppl. 3), 195–198. [Google Scholar] [CrossRef]
- Benedetti Panici, P.; De Vivo, A.; Bellati, F.; Manci, N.; Perniola, G.; Basile, S.; Muzii, L.; Angioli, R. Secondary cytoreductive surgery in patients with platinum-sensitive recurrent ovarian cancer. Ann. Surg. Oncol. 2007, 14, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Aletti, G.D.; Dowdy, S.C.; Gostout, B.S.; Jones, M.B.; Stanhope, R.C.; Wilson, T.O.; Podratz, K.C.; Cliby, W.A. Quality improvement in the surgical approach to advanced ovarian cancer: The Mayo Clinic experience. J. Am. Coll. Surg. 2009, 208, 614–620. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Patients N = 50 (%) |
|---|---|
| Median age at first surgery (years, range) | 52.6 (31.9–75.1) |
| FIGO stage at primary diagnosis | |
| I | 2 (4%) |
| II | 3 (6%) |
| III A | 2 (4%) |
| III B | 3 (6%) |
| III C. | 31 (62%) |
| IV | 4 (8%) |
| Not available | 5 (10%) |
| Histology | |
| Serous | 45 (90%) |
| Endometrioid | 2 (4%) |
| Clear cell | 2 (4%) |
| Not available | 1 (2%) |
| Grading | |
| G1 | 1 (2%) |
| G2 | 4 (8%) |
| G3 | 40 (80%) |
| Not available | 5 (10%) |
| BRCA status | |
| BRCA 1 mut | 5 (10%) |
| BRCA 2 mut | 2 (4%) |
| VUS | 3 (6%) |
| Negative | 5 (10%) |
| Unknown | 35 (70%) |
| Type of surgery at diagnosis | |
| Upfront | 37 (74%) |
| IDS | 11 (22%) |
| No surgery (exploratory laparotomy) | 2 (4%) |
| Postoperative tumor residual at first surgery | |
| CC-0 | 16 (32%) |
| CC > 0 | 25 (50%) |
| Unknown | 9 (18%) |
| Median PFS at primary recurrence (months, range) | 7.5 (0–33) |
| Primary platinum-resistant | |
| Yes | 20 (40%) |
| No | 30 (60%) |
| Treatment at first recurrence | |
| Not surgery | 32 (64%) |
| Surgery | 18 (36%) |
| CT before surgery for platinum resistance | |
| Yes | 32 (64%) |
| No | 18 (36%) |
| Median PFI from last platinum regimen (months, range) (information available for 31 cases, missing in 19) | 3.0 (0–5.0) |
| Median number of previous CT lines before surgery for platinum resistance (N, range) (information available for 49 cases, missing in 1) | 3 (1–7) |
| Median number of previous surgeries before surgery for platinum resistance (N, range) | 1 (1–4) |
| Variables | Patients N = 50 (%) |
|---|---|
| Median age at surgery for platinum resistance (years, range) | 56.5 (35.6–78.4) |
| Isolated relapse | |
| No | 48 (96%) |
| Yes | 2 (4%) |
| Relapse at platinum resistance a | |
| Peritoneum | 31 (62%) |
| Lymph node | 22 (44%) |
| Pelvis | 8 (16%) |
| Liver | 8 (16%) |
| Bowel | 7 (14%) |
| Omentum | 4 (8%) |
| Spleen | 3 (6%) |
| Sigma rectum | 3 (6%) |
| Diaphragm | 2 (4%) |
| Paraombelical lesion | 2 (5%) |
| Vagina | 1 (2%) |
| Intraoperative ascites at surgery for platinum resistance | |
| No | 27 (54%) |
| Yes | 17 (34%) |
| Unknown | 6 (12%) |
| PCI at surgery for platinum resistance | |
| <16 | 23 (46%) |
| ≥16 | 20 (40%) |
| Not available | 7 (14%) |
| Upper abdomen procedures during surgery for platinum resistance | |
| Yes | 21 (42%) |
| No | 28 (56%) |
| Unknown | 1 (2%) |
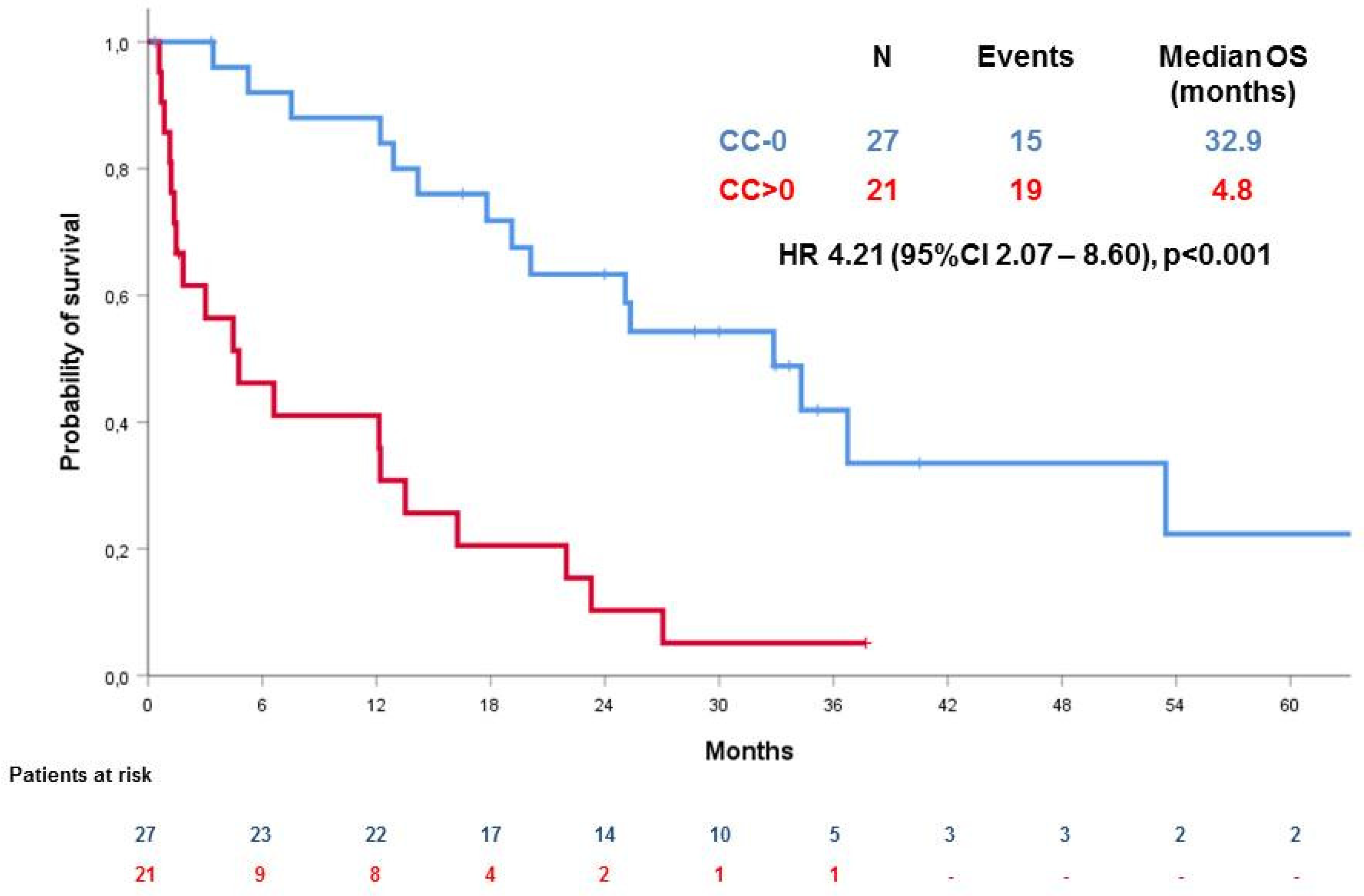
| Post-operative tumour residue at surgery for platinum resistance | |
| CC-0 | 27 (54%) |
| CC > 0 | 21 (42%) |
| Unknown | 2 (4%) |
| Median duration of surgery for platinum resistance (minutes, range) (information available for 39, missing in 11) | 170 (30–660) |
| Major morbidities of surgery for platinum resistance | |
| Pneumothorax | 5 (10%) |
| Acute respiratory failure | 2 (4%) |
| Lymphocele | 2 (4%) |
| Parenteral nutrition | 2 (4%) |
| Renal insufficiency and electrolytic imbalance | 2 (4%) |
| Infection/sepsis | 2 (4%) |
| Pleural effusion | 1 (2%) |
| Gastric laceration | 1 (2%) |
| Subocclusion | 1 (2%) |
| Pielostomy | 1 (2%) |
| 30-day mortality | 4 (8%) |
| Surgical procedures performed b | |
| Intestinal resection | 22 (44%) |
| Peritonectomy | 18 (36%) |
| Omentectomy | 16 (32%) |
| Pelvic LND | 12 (24%) |
| Paraortic LND | 12 (24%) |
| Splenectomy | 8 (16%) |
| Definitive stoma | 7 (14%) |
| Liver resection | 5 (10%) |
| Cholecystectomy | 5 (10%) |
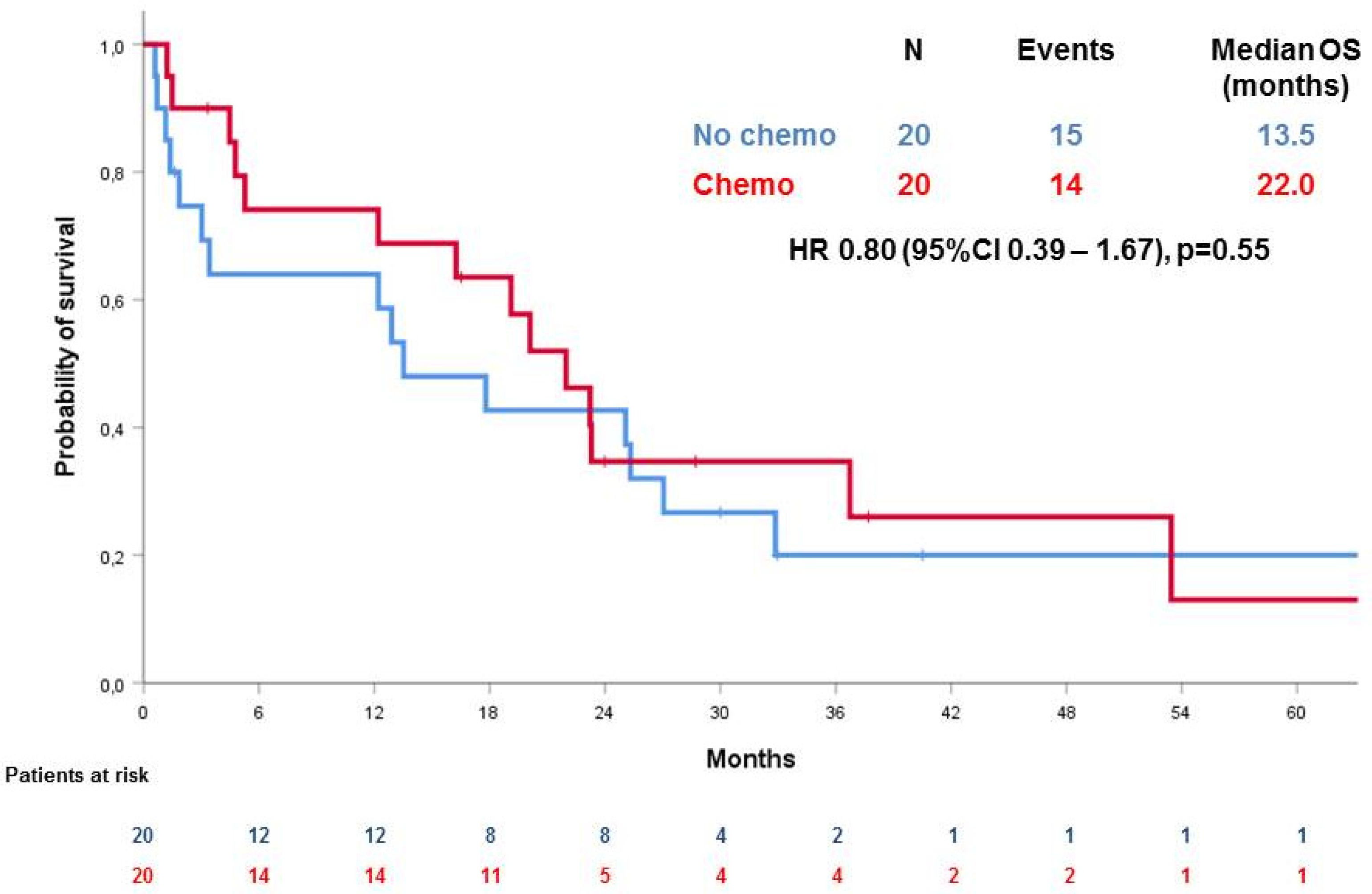
| Post-operative CT | |
| Yes | 20 (40%) |
| No | 20 (40%) |
| Unknown | 10 (20%) |
| Other treatments | |
| Yes | 14 (28%) |
| No | 26 (52%) |
| Unknown | 10 (20%) |
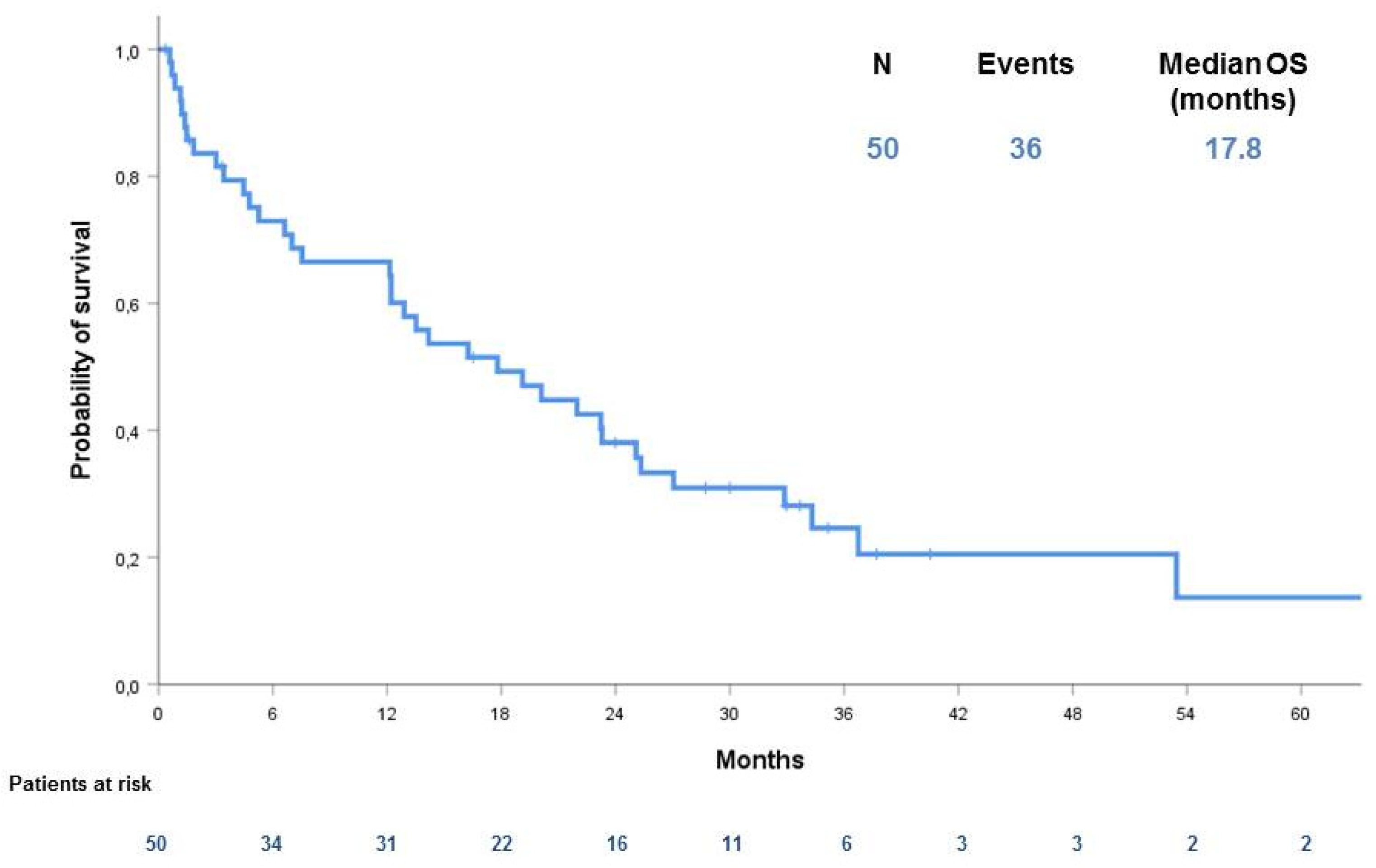
| OS (months) | |
| Median, 95% CI | 23.0 (14.1–31.8) |
| Heading Title | p Value | HR | 95% CI |
|---|---|---|---|
| CC > 0 vs. not | 0.016 | 11.1 | 1.6–78.5 |
| Post-operative CT vs. not | 0.9 | 0.9 | 0.2–5.0 |
| Intra-operative ascites vs. not | 0.65 | 0.65 | 0.1–4.0 |
| PCI > 16 vs. not | 0.8 | 1.3 | 0.2–9.3 |
| Upper abdomen procedures | 0.5 | 0.5 | 0.1–2.9 |
| Age > 65 years vs. not | 0.2 | 2.5 | 0.6–10.0 |
| G3 * | NA | NA | NA |
| FIGO stage ≥ IIIC | 0.2 | 0.2 | 0.02–1.9 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuninetti, V.; Di Napoli, M.; Ghisoni, E.; Maggiorotto, F.; Robella, M.; Scotto, G.; Giannone, G.; Turinetto, M.; Siatis, D.; Ponzone, R.; et al. Cytoreductive Surgery for Heavily Pre-Treated, Platinum-Resistant Epithelial Ovarian Carcinoma: A Two-Center Retrospective Experience. Cancers 2020, 12, 2239. https://doi.org/10.3390/cancers12082239
Tuninetti V, Di Napoli M, Ghisoni E, Maggiorotto F, Robella M, Scotto G, Giannone G, Turinetto M, Siatis D, Ponzone R, et al. Cytoreductive Surgery for Heavily Pre-Treated, Platinum-Resistant Epithelial Ovarian Carcinoma: A Two-Center Retrospective Experience. Cancers. 2020; 12(8):2239. https://doi.org/10.3390/cancers12082239
Chicago/Turabian StyleTuninetti, Valentina, Marilena Di Napoli, Eleonora Ghisoni, Furio Maggiorotto, Manuela Robella, Giulia Scotto, Gaia Giannone, Margherita Turinetto, Dimitris Siatis, Riccardo Ponzone, and et al. 2020. "Cytoreductive Surgery for Heavily Pre-Treated, Platinum-Resistant Epithelial Ovarian Carcinoma: A Two-Center Retrospective Experience" Cancers 12, no. 8: 2239. https://doi.org/10.3390/cancers12082239