Statin Use Improves Overall Survival of Patients with Gastric Cancer after Surgery and Adjuvant Chemotherapy in Taiwan: A Nationwide Matched Cohort Study


Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Data Source
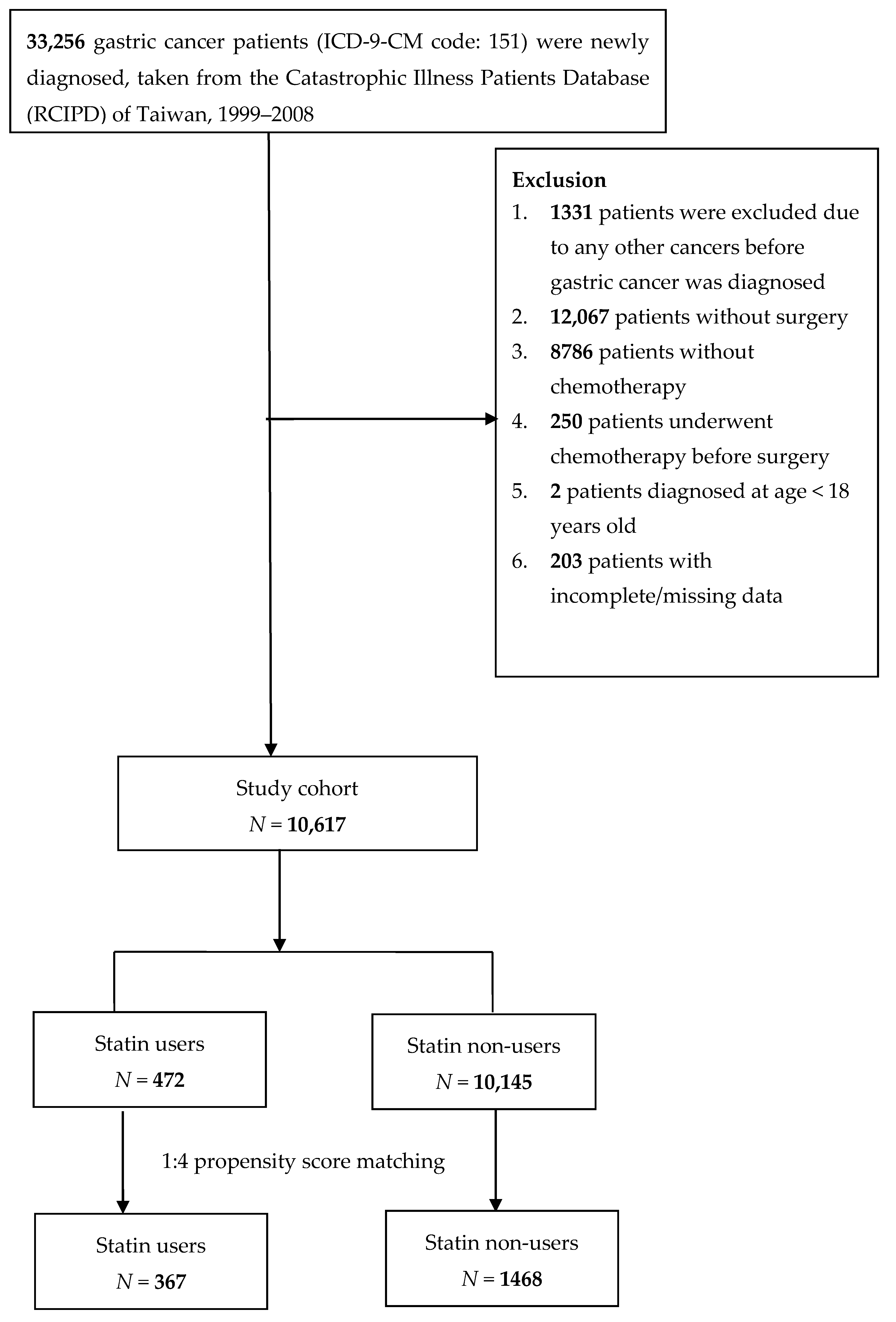
4.2. Study Population
4.3. Study Variables
4.4. Propensity Score Matching
4.5. Sensitivity Analyses
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| cDDDs | Cumulative defined daily doses |
| GC | gastric cancer |
| CI | confidence interval |
| H. pylori | Helicobacter pylori |
| HMG-CoA | 3-hydroxy-3-methylglutaryl-coenzyme A |
| OS | overall survival |
| NHIRD | National Health Insurance Research Database |
| RCIPD | Registry of Catastrophic Illness Patients Database |
| ICD-9-CM | International Classification of Diseases, Ninth Revision, Clinical Modification |
| ACE | angiotensin-converting enzyme |
| NSAID | non-steroidal anti-inflammatory drug |
| PS | propensity score |
| HR | hazard ratio |
| Cag A | cytotoxin-associated gene A |
| HDAC2 | histone deacetylase 2 |
References
- Irino, T.; Takeuchi, H.; Terashima, M.; Wakai, T.; Kitagawa, Y. Gastric Cancer in Asia: Unique Features and Management. Am. Soc. Clin. Oncol. Annu. Meet. 2017, 37, 279–291. [Google Scholar] [CrossRef]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2018. [Google Scholar]
- Correa, P. Gastric cancer: Two epidemics? Dig. Dis. Sci. 2011, 56, 1585–1586. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA: Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Promotion Administration. Ministry of Health and Welfare Cancer Registry Report. 2016. Available online: https://www.hpa.gov.tw/Pages/List.aspx?nodeid=119 (accessed on 25 December 2018).
- Waddell, T.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D. Gastric cancer: ESMO-ESSO-ESTRO clinical practice guidelines for diagnosis, treatment and follow-up. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2014, 40, 584–591. [Google Scholar] [CrossRef]
- Hung, K.F.; Hsu, C.P.; Chiang, J.H.; Lin, H.J.; Kuo, Y.T.; Sun, M.F.; Yen, H.R. Complementary Chinese herbal medicine therapy improves survival of patients with gastric cancer in Taiwan: A nationwide retrospective matched-cohort study. J. Ethnopharmacol. 2017, 199, 168–174. [Google Scholar] [CrossRef]
- Patel, T.N.; Roy, S.; Ravi, R. Gastric cancer and related epigenetic alterations. Ecancermedicalscience 2017, 11, 714. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Sagaert, X.; Topal, B.; Haustermans, K.; Prenen, H. Gastric cancer. Lancet 2016, 388, 2654–2664. [Google Scholar] [CrossRef]
- Coburn, N.; Cosby, R.; Klein, L.; Knight, G.; Malthaner, R.; Mamazza, J.; Mercer, C.D.; Ringash, J. Staging and surgical approaches in gastric cancer: A systematic review. Cancer Treat. Rev. 2018, 63, 104–115. [Google Scholar] [CrossRef]
- Association Japan Gasoline Corporation. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer 2017, 20, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Roukos, D.H.; Kappas, A.M. Perspectives in the treatment of gastric cancer. Nat. Clin. Pract. Oncol. 2005, 2, 98–107. [Google Scholar] [CrossRef]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Niksic, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Esteve, J.; et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Baigent, C.; Keech, A.; Kearney, P.M.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005, 366, 1267–1278. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.J.; Liao, W.C.; Lin, H.J.; Hsu, Y.M.; Lin, C.L.; Chen, Y.A.; Feng, C.L.; Chen, C.J.; Kao, M.C.; Lai, C.H.; et al. Statins Attenuate Helicobacter pylori CagA Translocation and Reduce Incidence of Gastric Cancer: In Vitro and Population-Based Case-Control Studies. PLoS ONE 2016, 11, e0146432. [Google Scholar] [CrossRef] [PubMed]
- Katoh, Y.; Katoh, M. Hedgehog signaling pathway and gastric cancer. Cancer Biol. Ther. 2005, 4, 1050–1054. [Google Scholar] [CrossRef] [Green Version]
- Manu, K.A.; Shanmugam, M.K.; Li, F.; Chen, L.; Siveen, K.S.; Ahn, K.S.; Kumar, A.P.; Sethi, G. Simvastatin sensitizes human gastric cancer xenograft in nude mice to capecitabine by suppressing nuclear factor-kappa B-regulated gene products. J. Mol. Med. 2014, 92, 267–276. [Google Scholar] [CrossRef] [Green Version]
- Chiu, H.F.; Ho, S.C.; Chang, C.C.; Wu, T.N.; Yang, C.Y. Statins are associated with a reduced risk of gastric cancer: A population-based case-control study. Am. J. Gastroenterol. 2011, 106, 2098–2103. [Google Scholar] [CrossRef]
- Spence, A.D.; Busby, J.; Hughes, C.M.; Johnston, B.T.; Coleman, H.G.; Cardwell, C.R. Statin use and survival in patients with gastric cancer in two independent population-based cohorts. Pharmacoepidemiol. Drug Saf. 2019, 28, 460–470. [Google Scholar] [CrossRef]
- Nam, D.H.; Lee, H.; Park, J.C.; Shin, S.K.; Lee, S.K.; Hyung, W.J.; Lee, Y.C.; Kang, M.W.; Noh, S.H. Long-term statin therapy improves oncological outcome after radical gastrectomy for stage II and III gastric cancer. Anticancer Res. 2014, 34, 355–361. [Google Scholar]
- Demierre, M.F.; Higgins, P.D.; Gruber, S.B.; Hawk, E.; Lippman, S.M. Statins and cancer prevention. Nat. Rev. Cancer 2005, 5, 930–942. [Google Scholar] [CrossRef]
- Joo, M.K.; Park, J.J.; Chun, H.J. Additional Benefits of Routine Drugs on Gastrointestinal Cancer: Statins, Metformin, and Proton Pump Inhibitors. Dig. Dis. 2018, 36, 1–14. [Google Scholar] [CrossRef]
- Zhang, L.; Kang, W.; Lu, X.; Ma, S.; Dong, L.; Zou, B. Weighted gene co-expression network analysis and connectivity map identifies lovastatin as a treatment option of gastric cancer by inhibiting HDAC2. Gene 2019, 681, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.P.; Singh, S. Statins are associated with reduced risk of gastric cancer: A systematic review and meta-analysis. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2013, 24, 1721–1730. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.T.; Kang, J.H.; Lee, J.; Park, S.H.; Park, J.O.; Park, Y.S.; Lim, H.Y.; Hwang, I.G.; Lee, S.C.; Park, K.W.; et al. Simvastatin plus capecitabine-cisplatin versus placebo plus capecitabine-cisplatin in patients with previously untreated advanced gastric cancer: A double-blind randomised phase 3 study. Eur. J. Cancer 2014, 50, 2822–2830. [Google Scholar] [CrossRef] [PubMed]
- Bujanda, L.; Rodriguez-Gonzalez, A.; Sarasqueta, C.; Eizaguirre, E.; Hijona, E.; Marin, J.J.; Perugorria, M.J.; Banales, J.M.; Cosme, A. Effect of pravastatin on the survival of patients with advanced gastric cancer. Oncotarget 2016, 7, 4379–4384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friis, S.; Poulsen, A.H.; Johnsen, S.P.; McLaughlin, J.K.; Fryzek, J.P.; Dalton, S.O.; Sorensen, H.T.; Olsen, J.H. Cancer risk among statin users: A population-based cohort study. Int. J. cancer 2005, 114, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Insurance BoNH. The National Health Insurance Annual Statistical Report; Bureau of National Health Insurance: Taipei, Taiwan, 2010.
- World Health Organization. World Health Organization collaborating centre for drug Stat Methodology. Available online: https://www.whocc.no/atc_ddd_methodology/who_collaborating_centre/ (accessed on 11 June 2019).
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | Statin Users (N = 367) | Statin Non-Users (N = 1468) | p-Value * | ||
|---|---|---|---|---|---|
| No. | % | No. | % | ||
| Gender | 0.5543 | ||||
| Female | 159 | 43.3 | 611 | 41.6 | |
| Male | 208 | 56.7 | 857 | 58.4 | |
| Age at Surgery | 0.4388 | ||||
| 18–64 | 172 | 46.9 | 655 | 44.6 | |
| ≥65 | 195 | 53.1 | 813 | 55.4 | |
| Mean (SD) | 64.3 (10.5) | 64.1 (12.6) | 0.758 | ||
| Insured Salaries (NTD$/month) a | |||||
| 0+ | 70 | 19.1 | 277 | 18.9 | |
| 1–15,840 | 38 | 10.4 | 154 | 10.5 | |
| 15,841–25,000 | 185 | 50.4 | 733 | 49.9 | |
| >25,000 | 74 | 20.2 | 304 | 20.7 | |
| Urbanization Level | 0.5232 | ||||
| Very High | 106 | 28.9 | 395 | 26.9 | |
| High | 170 | 46.3 | 737 | 50.2 | |
| Moderate | 62 | 16.9 | 241 | 16.4 | |
| Low | 29 | 7.9 | 95 | 6.5 | |
| Comorbidities | |||||
| Hypertension | 214 | 58.3 | 878 | 59.8 | 0.6009 |
| Diabetes Mellitus | 122 | 33.2 | 467 | 31.8 | 0.5996 |
| Alcoholism | 8 | 2.2 | 23 | 1.6 | 0.4150 |
| Smoking-related disorder | 40 | 10.9 | 166 | 11.3 | 0.8244 |
| Chronic kidney disease | 13 | 3.5 | 64 | 4.4 | 0.4848 |
| Liver cirrhosis | 14 | 3.8 | 61 | 4.2 | 0.7682 |
| Chemotherapy Regimen | 0.9425 | ||||
| Group 1 (epirubicin-based) | 29 | 7.9 | 105 | 7.2 | |
| Group 2 (mitomycin-based) | 49 | 13.4 | 205 | 14.0 | |
| Group 3 (taxanes) | 2 | 0.5 | 10 | 0.7 | |
| Group 4 (others) b | 287 | 78.2 | 1148 | 78.2 | |
| Medication | |||||
| Triglyceride-Lowering Drugs | 0.0046 | ||||
| User | 19 | 5.2 | 35 | 2.4 | |
| Non-user | 348 | 94.8 | 1433 | 97.6 | |
| Non-Statin Lipid-Lowering Drugs | 0.4756 | ||||
| User | 8 | 2.2 | 24 | 1.6 | |
| Non-user | 359 | 97.8 | 1444 | 98.4 | |
| ACE Inhibitors | 0.9579 | ||||
| User | 98 | 26.7 | 390 | 26.6 | |
| Non-user | 269 | 73.3 | 1078 | 73.4 | |
| Aspirin | 0.3669 | ||||
| User | 123 | 33.5 | 529 | 36.0 | |
| Non-user | 244 | 66.5 | 939 | 64.0 | |
| NSAID | 0.7487 | ||||
| User | 291 | 79.3 | 1175 | 80.0 | |
| Non-user | 76 | 20.7 | 293 | 20.0 | |
| Death | 138 | 37.6 | 895 | 61.0 | |
| Variables | 28–167 cDDD | ≥168 cDDD | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |||
| Main Model * | 0.62 | 0.50 | 0.78 | <0.0001 | 0.34 | 0.26 | 0.45 | <0.0001 |
| Additional Covariates † | ||||||||
| Main model + Diabetes mellitus | 0.64 | 0.51 | 0.80 | <0.0001 | 0.33 | 0.25 | 0.44 | <0.0001 |
| Main model + Hypertension | 0.62 | 0.50 | 0.78 | <0.0001 | 0.34 | 0.26 | 0.45 | <0.0001 |
| Main model + Alcoholism | 0.62 | 0.50 | 0.78 | <0.0001 | 0.34 | 0.26 | 0.45 | <0.0001 |
| Main model + Smoking-related disorder | 0.62 | 0.50 | 0.78 | <0.0001 | 0.34 | 0.26 | 0.45 | <0.0001 |
| Main model + Chronic renal failure | 0.62 | 0.50 | 0.78 | <0.0001 | 0.34 | 0.26 | 0.45 | <0.0001 |
| Main model + Liver cirrhosis | 0.62 | 0.50 | 0.77 | <0.0001 | 0.34 | 0.26 | 0.45 | <0.0001 |
| Main model + Chemotherapy regimen | 0.63 | 0.50 | 0.78 | <0.0001 | 0.33 | 0.25 | 0.44 | <0.0001 |
| Main model + Triglyceride-lowering drugs | 0.62 | 0.50 | 0.78 | <0.0001 | 0.35 | 0.26 | 0.46 | <0.0001 |
| Main model + Non-statin lipid-lowering drugs | 0.62 | 0.50 | 0.78 | <0.0001 | 0.34 | 0.26 | 0.45 | <0.0001 |
| Main model + ACE inhibitors | 0.61 | 0.49 | 0.76 | <0.0001 | 0.34 | 0.26 | 0.45 | <0.0001 |
| Main model + Aspirin | 0.60 | 0.48 | 0.75 | <0.0001 | 0.33 | 0.25 | 0.44 | <0.0001 |
| Main model + NSAID | 0.60 | 0.48 | 0.75 | <0.0001 | 0.32 | 0.24 | 0.43 | <0.0001 |
| Subgroup Effects | ||||||||
| Sex | ||||||||
| Male | 0.76 | 0.57 | 1.02 | 0.0674 | 0.41 | 0.30 | 0.57 | <0.0001 |
| Female | 0.49 | 0.35 | 0.70 | <0.0001 | 0.23 | 0.14 | 0.40 | <0.0001 |
| Age at Surgery | ||||||||
| 18–64 | 0.46 | 0.31 | 0.67 | <0.0001 | 0.24 | 0.14 | 0.41 | <0.0001 |
| ≥65 | 0.75 | 0.57 | 0.99 | 0.0402 | 0.40 | 0.29 | 0.55 | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, P.-R.; Tsai, Y.-Y.; Chen, K.-J.; Yang, Y.-H.; Shih, W.-T. Statin Use Improves Overall Survival of Patients with Gastric Cancer after Surgery and Adjuvant Chemotherapy in Taiwan: A Nationwide Matched Cohort Study. Cancers 2020, 12, 2055. https://doi.org/10.3390/cancers12082055
Yang P-R, Tsai Y-Y, Chen K-J, Yang Y-H, Shih W-T. Statin Use Improves Overall Survival of Patients with Gastric Cancer after Surgery and Adjuvant Chemotherapy in Taiwan: A Nationwide Matched Cohort Study. Cancers. 2020; 12(8):2055. https://doi.org/10.3390/cancers12082055
Chicago/Turabian StyleYang, Pei-Rung, Ying-Ying Tsai, Ko-Jung Chen, Yao-Hsu Yang, and Wei-Tai Shih. 2020. "Statin Use Improves Overall Survival of Patients with Gastric Cancer after Surgery and Adjuvant Chemotherapy in Taiwan: A Nationwide Matched Cohort Study" Cancers 12, no. 8: 2055. https://doi.org/10.3390/cancers12082055