Are Leading Risk Factors for Cancer and Mental Disorders Multimorbidity Shared by These Two Individual Conditions in Community-Dwelling Middle-Aged Adults?

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Participant Characteristics
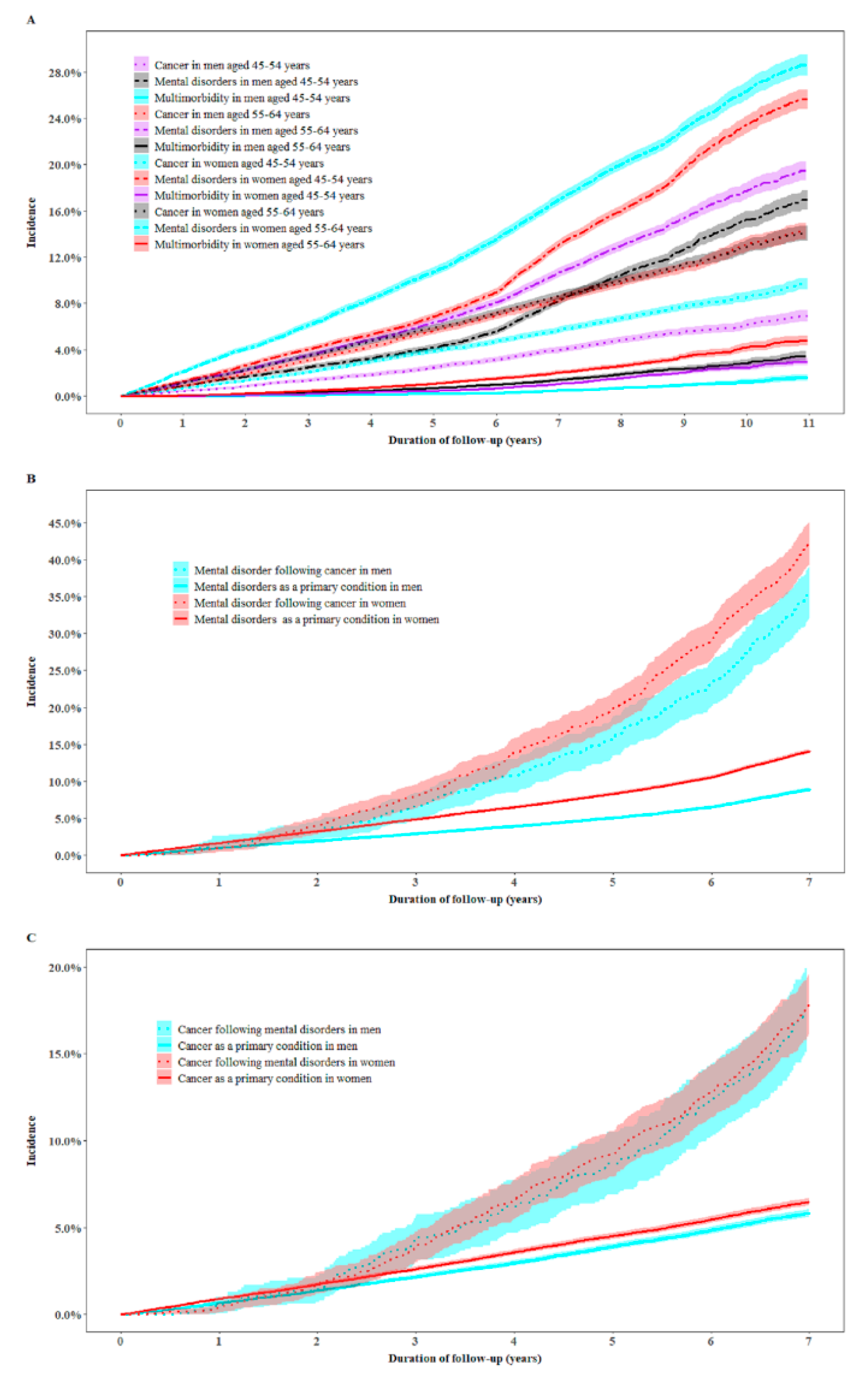
2.2. Incidence of Cancer, Mental Disorders, and Multimorbidity
2.3. Leading Predictors for Multimorbidity
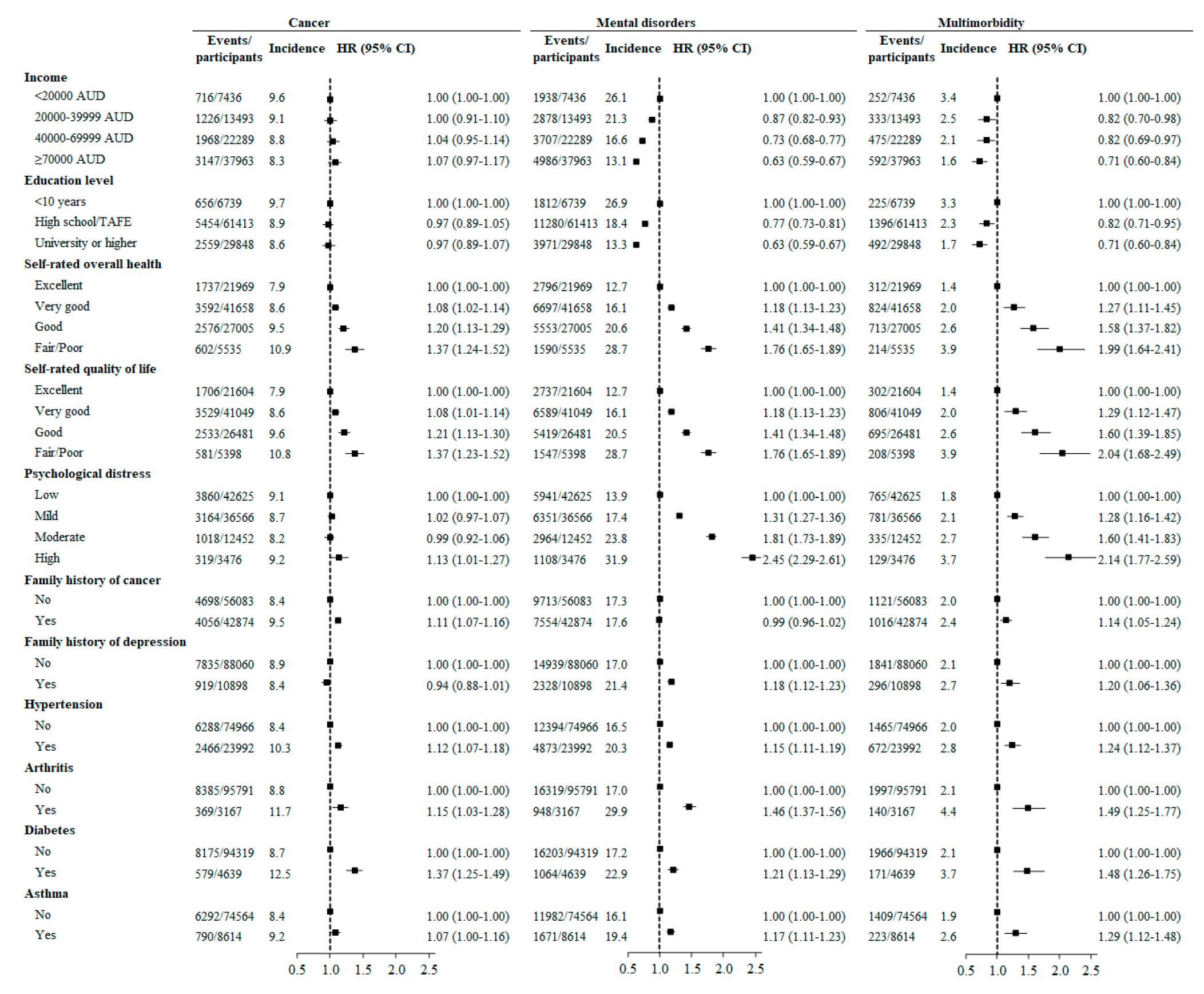
2.4. Hazard Ratios for Cancer, Mental Disorders, and Multimorbidity Associated with Potential Predictors
2.5. Sensitivity Analysis
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Independent Variables
4.3. Outcome Variables
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Global Burden of Disease Cancer Collaboration. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2016: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2018, 4, 1553–1568. [CrossRef]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Fitzsimmons, G.J.; Sadkowsky, K.R. The Australian Institute of Health and Welfare. Commun. Dis. Intell. Q. Rep. 2002, 26. [Google Scholar]
- Steel, Z.; Marnane, C.; Iranpour, C.; Chey, T.; Jackson, J.W.; Patel, V.; Silove, D. The global prevalence of common mental disorders: A systematic review and meta-analysis 1980–2013. Int. J. Epidemiol. 2014, 43, 476–493. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.R.; McGee, R.E.; Druss, B.G. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiatry 2015, 72, 334–341. [Google Scholar] [CrossRef]
- Vigo, D.; Thornicroft, G.; Atun, R. Estimating the true global burden of mental illness. Lancet Psychiatry 2016, 3, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Ng, H.S.; Roder, D.; Koczwara, B.; Vitry, A. Comorbidity, physical and mental health among cancer patients and survivors: An Australian population-based study. Asia-Pacific J. Clin. Oncol. 2017, 14, e181–e192. [Google Scholar] [CrossRef]
- Satin, J.R.; Linden, W.; Phillips, M.J. Depression as a predictor of disease progression and mortality in cancer patients. Cancer 2009, 115, 5349–5361. [Google Scholar] [CrossRef]
- Hawkins, N.A.; Soman, A.; Lunsford, N.B.; Leadbetter, S.; Rodriguez, J.L. Use of Medications for Treating Anxiety and Depression in Cancer Survivors in the United States. J. Clin. Oncol. 2017, 35, 78–85. [Google Scholar] [CrossRef]
- Kisely, S.; Crowe, E.; Lawrence, D. Cancer-Related Mortality in People With Mental Illness. JAMA Psychiatry 2013, 70, 209. [Google Scholar] [CrossRef] [Green Version]
- Pinquart, M.; Duberstein, P. Depression and cancer mortality: A meta-analysis. Psychol. Med. 2010, 40, 1797–1810. [Google Scholar] [CrossRef] [PubMed]
- Danaei, G.; Hoorn, S.V.; Lopez, A.; Murray, C.J.; Ezzati, M. Causes of cancer in the world: Comparative risk assessment of nine behavioural and environmental risk factors. Lancet 2005, 366, 1784–1793. [Google Scholar] [CrossRef] [Green Version]
- Cole, M.G.; Dendukuri, N. Risk Factors for Depression Among Elderly Community Subjects: A Systematic Review and Meta-Analysis. Am. J. Psychiatry 2003, 160, 1147–1156. [Google Scholar] [CrossRef] [PubMed]
- Molendijk, M.; Molero, P.; Sánchez-Pedreño, F.O.; Van Der Does, W.; Martínez-González, M.A. Diet quality and depression risk: A systematic review and dose-response meta-analysis of prospective studies. J. Affect. Disord. 2018, 226, 346–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, K.; Hadgkiss, E.J.; Jelinek, G.; Weiland, T.; Pereira, N.G.; Marck, C.H.; Van Der Meer, D.M. Lifestyle factors, demographics and medications associated with depression risk in an international sample of people with multiple sclerosis. BMC Psychiatry 2014, 14, 327. [Google Scholar] [CrossRef]
- Dorak, M.T.; Karpuzoglu, E. Gender Differences in Cancer Susceptibility: An Inadequately Addressed Issue. Front. Genet. 2012, 3, 268. [Google Scholar] [CrossRef] [Green Version]
- Sandison, B. Australian Institute of Health and Welfare. Impact 2018, 2018, 80–81. [Google Scholar] [CrossRef]
- Pedersen, C.; Mors, O.; Bertelsen, A.; Waltoft, B.L.; Agerbo, E.; McGrath, J.J.; Mortensen, P.B.; Eaton, W.W. A Comprehensive Nationwide Study of the Incidence Rate and Lifetime Risk for Treated Mental Disorders. JAMA Psychiatry 2014, 71, 573–581. [Google Scholar] [CrossRef]
- Waraich, P.; Goldner, E.M.; Somers, J.M.; Hsu, L. Prevalence and Incidence Studies of Mood Disorders: A Systematic Review of the Literature. Can. J. Psychiatry 2004, 49, 124–138. [Google Scholar] [CrossRef] [Green Version]
- Jia, Y.; Li, F.; Liu, Y.; Zhao, J.; Leng, M.; Chen, L. Depression and cancer risk: A systematic review and meta-analysis. Public Heal. 2017, 149, 138–148. [Google Scholar] [CrossRef]
- Lu, D.; Andersson, T.M.-L.; Fall, K.; Hultman, C.M.; Czene, K.; Valdimarsdóttir, U.; Fang, F. Clinical Diagnosis of Mental Disorders Immediately Before and After Cancer Diagnosis. JAMA Oncol. 2016, 2, 1188. [Google Scholar] [CrossRef] [PubMed]
- Silver, J.K.; Baima, J. Cancer Prehabilitation. Am. J. Phys. Med. Rehabil. 2013, 92, 715–727. [Google Scholar] [CrossRef] [PubMed]
- Gandini, S.; Botteri, E.; Iodice, S.; Boniol, M.; Lowenfels, A.B.; Maisonneuve, P.; Boyle, P. Tobacco smoking and cancer: A meta-analysis. Int. J. Cancer 2007, 122, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Liang, P.S.; Chen, T.-Y.; Giovannucci, E. Cigarette smoking and colorectal cancer incidence and mortality: Systematic review and meta-analysis. Int. J. Cancer 2009, 124, 2406–2415. [Google Scholar] [CrossRef]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. International Agency for Research on Cancer Handbook Working Group Body Fatness and Cancer—Viewpoint of the IARC Working Group. New Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.X.Z.; Mishra, S. Obesity-Linked Cancers: Current Knowledge, Challenges and Limitations in Mechanistic Studies and Rodent Models. Cancers 2018, 10, 523. [Google Scholar] [CrossRef] [Green Version]
- Wilson, L.; Antonsson, A.; Green, A.C.; Jordan, S.J.; Kendall, B.; Nagle, C.M.; Neale, R.; Olsen, C.M.; Webb, P.M.; Whiteman, D.C. How many cancer cases and deaths are potentially preventable? Estimates for Australia in 2013. Int. J. Cancer 2017, 142, 691–701. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, L.; Zhou, Q.; Imam, M.U.; Cai, J.; Wang, Y.; Qi, M.; Sun, P.; Ping, Z.; Fu, X. Body mass index had different effects on premenopausal and postmenopausal breast cancer risks: A dose-response meta-analysis with 3,318,796 subjects from 31 cohort studies. BMC Public Heal. 2017, 17, 936. [Google Scholar] [CrossRef]
- Boffetta, P.; Couto, E.; Wichmann, J.; Ferrari, P.; Trichopoulos, D.; Bueno-De-Mesquita, H.B.; Van Duijnhoven, F.J.B.; Büchner, F.L.; Key, T.J.; Boeing, H.; et al. Fruit and Vegetable Intake and Overall Cancer Risk in the European Prospective Investigation Into Cancer and Nutrition (EPIC). J. Natl. Cancer Inst. 2010, 102, 529–537. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.C.; Lee, I.-M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.; Arem, H.; De Gonzalez, A.B.; Hartge, P.; et al. Association of Leisure-Time Physical Activity With Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef]
- Zhao, H.; Yin, J.-Y.; Yang, W.-S.; Qin, Q.; Li, T.-T.; Shi, Y.; Deng, Q.; Wei, S.; Liu, L.; Wang, X.; et al. Sleep Duration and Cancer Risk: A Systematic Review and Meta-analysis of Prospective Studies. Asian Pac. J. Cancer Prev. 2013, 14, 7509–7515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, S.; Wang, R.; Zhao, Y.; Ma, X.; Wu, M.; Yan, X.; He, J. The relationship between self-rated health and objective health status: A population-based study. BMC Public Heal. 2013, 13, 320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molarius, A.; Janson, S. Self-rated health, chronic diseases, and symptoms among middle-aged and elderly men and women. J. Clin. Epidemiol. 2002, 55, 364–370. [Google Scholar] [CrossRef]
- Perruccio, A.V.; Power, J.D.; Badley, E.M. The relative impact of 13 chronic conditions across three different outcomes. J. Epidemiol. Community Heal. 2007, 61, 1056–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riise, H.K.R.; Riise, T.; Natvig, G.K.; Daltveit, A.K. Poor self-rated health associated with an increased risk of subsequent development of lung cancer. Qual. Life Res. 2013, 23, 145–153. [Google Scholar] [CrossRef]
- Jylhä, M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef]
- Batty, G.D.; Russ, T.C.; Stamatakis, E.; Kivimaki, M. Psychological distress in relation to site specific cancer mortality: Pooling of unpublished data from 16 prospective cohort studies. BMJ 2017, 356. [Google Scholar] [CrossRef] [Green Version]
- Radišauskas, R.; Kuzmickienė, I.; Milinavičienė, E.; Everatt, R. Hypertension, serum lipids and cancer risk: A review of epidemiological evidence. Medicina 2016, 52, 89–98. [Google Scholar] [CrossRef]
- Tsilidis, K.K.; Kasimis, J.C.; Lopez, D.S.; Ntzani, E.E.; Ioannidis, J.P.A. Type 2 diabetes and cancer: Umbrella review of meta-analyses of observational studies. BMJ 2015, 350, g7607. [Google Scholar] [CrossRef] [Green Version]
- Simon, T.A.; Thompson, A.; Gandhi, K.K.; Hochberg, M.C.; Suissa, S. Incidence of malignancy in adult patients with rheumatoid arthritis: A meta-analysis. Arthritis Res. 2015, 17, 212. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Li, Y.; Chen, L.; Chen, P.; Hu, Y. Prevalence of Depression in Patients With Hypertension. Medicine 2015, 94, e1317. [Google Scholar] [CrossRef] [PubMed]
- Nouwen, A.; Winkley, K.; Twisk, J.; Lloyd, C.E.; Peyrot, M.; Ismail, K.; Pouwer, F. European Depression in Diabetes (EDID) Research Consortium Type 2 diabetes mellitus as a risk factor for the onset of depression: A systematic review and meta-analysis. Diabetologia 2010, 53, 2480–2486. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Aluko, Y.; Myint, P.K.; Smith, T. Prevalence of depressive symptoms and anxiety in osteoarthritis: A systematic review and meta-analysis. Age Ageing 2016, 45, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrell, L.; Hollingsworth, B.; Propper, C.; Shields, M.A. The socioeconomic gradient in physical inactivity: Evidence from one million adults in England. Soc. Sci. Med. 2014, 123, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Nohr, E.A.; Frydenberg, M.; Henriksen, T.B.; Olsen, J. Does Low Participation in Cohort Studies Induce Bias? Epidemiology 2006, 17, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Mealing, N.M.; Banks, E.; Jorm, L.; Steel, D.; Clements, M.S.; Rogers, K. Investigation of relative risk estimates from studies of the same population with contrasting response rates and designs. BMC Med Res. Methodol. 2010, 10, 26. [Google Scholar] [CrossRef] [Green Version]
- 45 and Up Study Collaborators; Banks, E.; Redman, S.; Jorm, L.; Armstrong, B.; Bauman, A.; Beard, J.; Beral, V.; Byles, J.; Corbett, S.; et al. Cohort profile: The 45 and up study. Int. J. Epidemiol. 2007, 37, 941–947. [Google Scholar] [CrossRef] [Green Version]
- Obermeyer, Z.; Emanuel, E.J. Predicting the Future—Big Data, Machine Learning, and Clinical Medicine. New Engl. J. Med. 2016, 375, 1216–1219. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Men | Women | ||
|---|---|---|---|---|
| 45–54 Years | 55–64 Years | 45–54 Years | 55–64 Years | |
| Country of birth | – | – | – | – |
| Australia | 16,659 (75.7) | 16,407 (71.7) | 21,605 (76.1) | 19,042 (74.2) |
| Others | 5260 (23.9) | 6352 (27.7) | 6692 (23.6) | 6471 (25.2) |
| Missing | 93 (0.4) | 134 (0.6) | 108 (0.4) | 135 (0.5) |
| Household income | – | – | – | – |
| <20,000 AUD | 879 (4.0) | 1750 (7.6) | 1724 (6.1) | 3083 (12.0) |
| 20,000–39,999 AUD | 1853 (8.4) | 3363 (14.7) | 3712 (13.1) | 4565 (17.8) |
| 40,000–69,999 AUD | 4889 (22.2) | 5761 (25.2) | 6198 (21.8) | 5441 (21.2) |
| ≥70,000 AUD | 11,931 (54.2) | 8804 (38.5) | 11,428 (40.2) | 5800 (22.6) |
| Missing | 2460 (11.2) | 3215 (14.0) | 5343 (18.8) | 6759 (26.4) |
| Education level | – | – | – | – |
| <10 years | 1061 (4.8) | 1834 (8.0) | 1627 (5.7) | 2217 (8.6) |
| High school/TAFE | 13,157 (59.8) | 14,059 (61.4) | 17,304 (60.9) | 16,893 (65.9) |
| University or higher | 7608 (34.6) | 6724 (29.4) | 9247 (32.6) | 6269 (24.4) |
| Missing | 186 (0.8) | 276 (1.2) | 227 (0.8) | 269 (1.0) |
| Residential rurality 1 | – | – | – | – |
| Major cities | 12,308 (55.9) | 11,971 (52.3) | 15,008 (52.8) | 12,903 (50.3) |
| Inner regional | 6933 (31.5) | 7772 (33.9) | 9708 (34.2) | 9122 (35.6) |
| Outer regional | 2059 (9.4) | 2407 (10.5) | 2743 (9.7) | 2847 (11.1) |
| Remote | 249 (1.1) | 237 (1.0) | 363 (1.3) | 254 (1.0) |
| Missing | 463 (2.1) | 506 (2.2) | 583 (2.1) | 522 (2.0) |
| Relative socioeconomic disadvantage 2 | – | – | – | – |
| 1st quintile | 3392 (15.4) | 3832 (16.7) | 4529 (15.9) | 4585 (17.9) |
| 2nd quintile | 3957 (18.0) | 4434 (19.4) | 5429 (19.1) | 5132 (20.0) |
| 3rd quintile | 4088 (18.6) | 4176 (18.2) | 5490 (19.3) | 4781 (18.6) |
| 4th quintile | 4096 (18.6) | 4061 (17.7) | 5085 (17.9) | 4349 (17.0) |
| 5th quintile | 5877 (26.7) | 5703 (24.9) | 7091 (25.0) | 6081 (23.7) |
| Missing | 602 (2.7) | 687 (3.0) | 781 (2.7) | 720 (2.8) |
| Family history of cancer | – | – | – | – |
| No | 12,999 (59.1) | 13,069 (57.1) | 16,145 (56.8) | 13,870 (54.1) |
| Yes | 9013 (40.9) | 9824 (42.9) | 12,260 (43.2) | 11,777 (45.9) |
| Family history of depression | – | – | – | – |
| No | 19,818 (90.0) | 21,039 (91.9) | 24,476 (86.2) | 22,727 (88.6) |
| Yes | 2194 (10.0) | 1854 (8.1) | 3929 (13.8) | 2921 (11.4) |
| Body mass index 3 | – | – | – | – |
| 15–18.4 kg/m2 | 103 (0.5) | 108 (0.5) | 406 (1.4) | 323 (1.3) |
| 18.5–24.9 kg/m2 | 6110 (27.8) | 6187 (27.0) | 12,755 (44.9) | 10,035 (39.1) |
| 25–29.9 kg/m2 | 10,052 (45.7) | 10,539 (46.0) | 7881 (27.7) | 8041 (31.4) |
| ≥30 kg/m2 | 4735 (21.5) | 4932 (21.5) | 5546 (19.5) | 5559 (21.7) |
| Missing | 1012 (4.6) | 1127 (4.9) | 1817 (6.4) | 1690 (6.6) |
| Smoking | – | – | – | – |
| Never | 12,743 (57.9) | 11,940 (52.2) | 17,797 (62.7) | 17,356 (67.7) |
| Former | 7061 (32.1) | 9140 (39.9) | 8228 (29.0) | 6861 (26.8) |
| Current | 2204 (10.0) | 1807 (7.9) | 2374 (8.4) | 1425 (5.6) |
| Missing | 4 (0.0) | 6 (0.0) | 6 (0.0) | 6 (0.0) |
| Alcohol consumption | – | – | – | – |
| None | 4231 (19.2) | 4117 (18.0) | 9538 (33.6) | 9055 (35.3) |
| 1–4 sessions/week | 4450 (20.2) | 4225 (18.5) | 7293 (25.7) | 6076 (23.7) |
| 5–7 sessions/week | 3030 (13.8) | 3139 (13.7) | 4300 (15.1) | 4083 (15.9) |
| 7–14 sessions/week | 4537 (20.6) | 4978 (21.7) | 4959 (17.5) | 4428 (17.3) |
| ≥15 sessions/week | 5569 (25.3) | 6236 (27.2) | 2010 (7.1) | 1679 (6.5) |
| Missing | 195 (0.9) | 198 (0.9) | 305 (1.1) | 327 (1.3) |
| Physical activity | – | – | – | – |
| 0–4 sessions/week | 4160 (18.9) | 3934 (17.2) | 4808 (16.9) | 3681 (14.4) |
| 5–9 sessions/week | 6041 (27.4) | 6201 (27.1) | 8673 (30.5) | 7814 (30.5) |
| 10–14 sessions/week | 4690 (21.3) | 5115 (22.3) | 6976 (24.6) | 6588 (25.7) |
| ≥15 sessions/week | 6574 (29.9) | 6978 (30.5) | 7364 (25.9) | 6899 (26.9) |
| Missing | 547 (2.5) | 665 (2.9) | 584 (2.1) | 666 (2.6) |
| Sleep time | – | – | – | – |
| <7 h | 3753 (17.0) | 3457 (15.1) | 3871 (13.6) | 3634 (14.2) |
| 7–9 h | 17,419 (79.1) | 18,163 (79.3) | 23,256 (81.9) | 20,641 (80.5) |
| >9 h | 430 (2.0) | 843 (3.7) | 802 (2.8) | 853 (3.3) |
| Missing | 410 (1.9) | 430 (1.9) | 476 (1.7) | 520 (2.0) |
| Sitting time | – | – | – | – |
| <8 h | 13,526 (61.4) | 15,477 (67.6) | 19,628 (69.1) | 18,924 (73.8) |
| ≥8 h | 7611 (34.6) | 6308 (27.6) | 7327 (25.8) | 5077 (19.8) |
| Missing | 875 (4.0) | 1108 (4.8) | 1450 (5.1) | 1647 (6.4) |
| Chicken intake | – | – | – | – |
| None | 617 (2.8) | 892 (3.9) | 1021 (3.6) | 1017 (4.0) |
| 1 serving per week | 3313 (15.1) | 4637 (20.3) | 4041 (14.2) | 4626 (18.0) |
| 2 servings per week | 6372 (28.9) | 6836 (29.9) | 8165 (28.7) | 7641 (29.8) |
| 3 or more servings per week | 7508 (34.1) | 6373 (27.8) | 9670 (34.0) | 7572 (29.5) |
| Missing | 4202 (19.1) | 4155 (18.1) | 5508 (19.4) | 4792 (18.7) |
| Fish intake | – | – | – | – |
| None | 2037 (9.3) | 1510 (6.6) | 2698 (9.5) | 1713 (6.7) |
| 1 serving per week | 9887 (44.9) | 9917 (43.3) | 11,772 (41.4) | 9415 (36.7) |
| 2 servings per week | 5258 (23.9) | 6054 (26.4) | 7043 (24.8) | 7498 (29.2) |
| 3 or more servings per week | 3685 (16.7) | 4177 (18.2) | 5388 (19.0) | 5807 (22.6) |
| Missing | 1145 (5.2) | 1235 (5.4) | 1504 (5.3) | 1215 (4.7) |
| Red meat intake | – | – | – | – |
| 0 or 1 serving per week | 2324 (10.6) | 2250 (9.8) | 4007 (14.1) | 3269 (12.7) |
| 2 servings per week | 3850 (17.5) | 3689 (16.1) | 5371 (18.9) | 4341 (16.9) |
| 3 or 4 servings per week | 7370 (33.5) | 7884 (34.4) | 9967 (35.1) | 9319 (36.3) |
| 5 or more servings per week | 4351 (19.8) | 5169 (22.6) | 3568 (12.6) | 4028 (15.7) |
| Missing | 4117 (18.7) | 3901 (17.0) | 5492 (19.3) | 4691 (18.3) |
| Vegetable intake | – | – | – | – |
| 0 or 1 serving per day | 3534 (16.1) | 3601 (15.7) | 1833 (6.5) | 1264 (4.9) |
| 2 servings per day | 7635 (34.7) | 7113 (31.1) | 6528 (23.0) | 4884 (19.0) |
| 3 servings per day | 3554 (16.1) | 3562 (15.6) | 4994 (17.6) | 3853 (15.0) |
| 4 servings per day | 2666 (12.1) | 2905 (12.7) | 5105 (18.0) | 4729 (18.4) |
| 5 or more servings per day | 4159 (18.9) | 5154 (22.5) | 9251 (32.6) | 10,298 (40.2) |
| Missing | 464 (2.1) | 558 (2.4) | 694 (2.4) | 620 (2.4) |
| Fruit intake | – | – | – | – |
| None | 2344 (10.6) | 2029 (8.9) | 1701 (6.0) | 1045 (4.1) |
| 1 serving per day | 8256 (37.5) | 8400 (36.7) | 9126 (32.1) | 6735 (26.3) |
| 2 servings per day | 5912 (26.9) | 6356 (27.8) | 9920 (34.9) | 9491 (37.0) |
| 3 or more servings per day | 4318 (19.6) | 4748 (20.7) | 6426 (22.6) | 7321 (28.5) |
| Missing | 1182 (5.4) | 1360 (5.9) | 1232 (4.3) | 1056 (4.1) |
| Psychological distress 4 | – | – | – | – |
| Low | 8947 (40.6) | 11,232 (49.1) | 10,275 (36.2) | 12,171 (47.5) |
| Mild | 8596 (39.1) | 7907 (34.5) | 11,499 (40.5) | 8564 (33.4) |
| Moderate | 3189 (14.5) | 2227 (9.7) | 4426 (15.6) | 2610 (10.2) |
| High | 856 (3.9) | 605 (2.6) | 1327 (4.7) | 688 (2.7) |
| Missing | 424 (1.9) | 922 (4.0) | 878 (3.1) | 1615 (6.3) |
| Social interaction 5 | – | – | – | – |
| Low | 4531 (20.6) | 4107 (17.9) | 4623 (16.3) | 3075 (12.0) |
| Moderate | 12,845 (58.4) | 12,912 (56.4) | 17,348 (61.1) | 14,455 (56.4) |
| High | 3278 (14.9) | 4184 (18.3) | 4588 (16.2) | 6218 (24.2) |
| Missing | 1358 (6.2) | 1690 (7.4) | 1846 (6.5) | 1900 (7.4) |
| Self-rated health status | – | – | – | – |
| Excellent | 4286 (19.5) | 4272 (18.7) | 7346 (25.9) | 6065 (23.6) |
| Very good | 8862 (40.3) | 9733 (42.5) | 11,786 (41.5) | 11,277 (44.0) |
| Good | 6857 (31.2) | 6791 (29.7) | 7059 (24.9) | 6298 (24.6) |
| Fair/Poor | 1512 (6.9) | 1481 (6.5) | 1364 (4.8) | 1178 (4.6) |
| Missing | 495 (2.2) | 616 (2.7) | 850 (3.0) | 830 (3.2) |
| Self-rated quality of life | – | – | – | – |
| Excellent | 4229 (19.2) | 4201 (18.4) | 7229 (25.4) | 5945 (23.2) |
| Very good | 8758 (39.8) | 9569 (41.8) | 11,652 (41.0) | 11,070 (43.2) |
| Good | 6755 (30.7) | 6625 (28.9) | 6952 (24.5) | 6149 (24.0) |
| Fair/Poor | 1486 (6.8) | 1440 (6.3) | 1338 (4.7) | 1134 (4.4) |
| Missing | 784 (3.6) | 1058 (4.6) | 1234 (4.3) | 1350 (5.3) |
| Hypertension | – | – | – | – |
| No | 17,307 (78.6) | 15,450 (67.5) | 23,902 (84.1) | 18,307 (71.4) |
| Yes | 4705 (21.4) | 7443 (32.5) | 4503 (15.9) | 7341 (28.6) |
| Dyslipidemia | – | – | – | – |
| No | 20,099 (91.3) | 19,821 (86.6) | 27,107 (95.4) | 22,556 (87.9) |
| Yes | 1913 (8.7) | 3072 (13.4) | 1298 (4.6) | 3092 (12.1) |
| Diabetes | – | – | – | – |
| No | 21,111 (95.9) | 21,189 (92.6) | 27,572 (97.1) | 24,447 (95.3) |
| Yes | 901 (4.1) | 1704 (7.4) | 833 (2.9) | 1201 (4.7) |
| Arthritis | – | – | – | – |
| No | 21,704 (98.6) | 22,278 (97.3) | 27,692 (97.5) | 24,117 (94.0) |
| Yes | 308 (1.4) | 615 (2.7) | 713 (2.5) | 1531 (6.0) |
| Asthma | – | – | – | – |
| No | 16,548 (75.2) | 17,870 (78.1) | 20,900 (73.6) | 19,246 (75.0) |
| Yes | 1779 (8.1) | 1680 (7.3) | 2745 (9.7) | 2410 (9.4) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shang, X.; Hodge, A.M.; Peng, W.; He, M.; Zhang, L. Are Leading Risk Factors for Cancer and Mental Disorders Multimorbidity Shared by These Two Individual Conditions in Community-Dwelling Middle-Aged Adults? Cancers 2020, 12, 1700. https://doi.org/10.3390/cancers12061700
Shang X, Hodge AM, Peng W, He M, Zhang L. Are Leading Risk Factors for Cancer and Mental Disorders Multimorbidity Shared by These Two Individual Conditions in Community-Dwelling Middle-Aged Adults? Cancers. 2020; 12(6):1700. https://doi.org/10.3390/cancers12061700
Chicago/Turabian StyleShang, Xianwen, Allison M. Hodge, Wei Peng, Mingguang He, and Lei Zhang. 2020. "Are Leading Risk Factors for Cancer and Mental Disorders Multimorbidity Shared by These Two Individual Conditions in Community-Dwelling Middle-Aged Adults?" Cancers 12, no. 6: 1700. https://doi.org/10.3390/cancers12061700