Population Pharmacokinetics/Pharmacodynamics of Dabrafenib Plus Trametinib in Patients with BRAF-Mutated Metastatic Melanoma

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Results
2.1. Pharmacokinetic Data
2.2. Pharmacokinetic Data
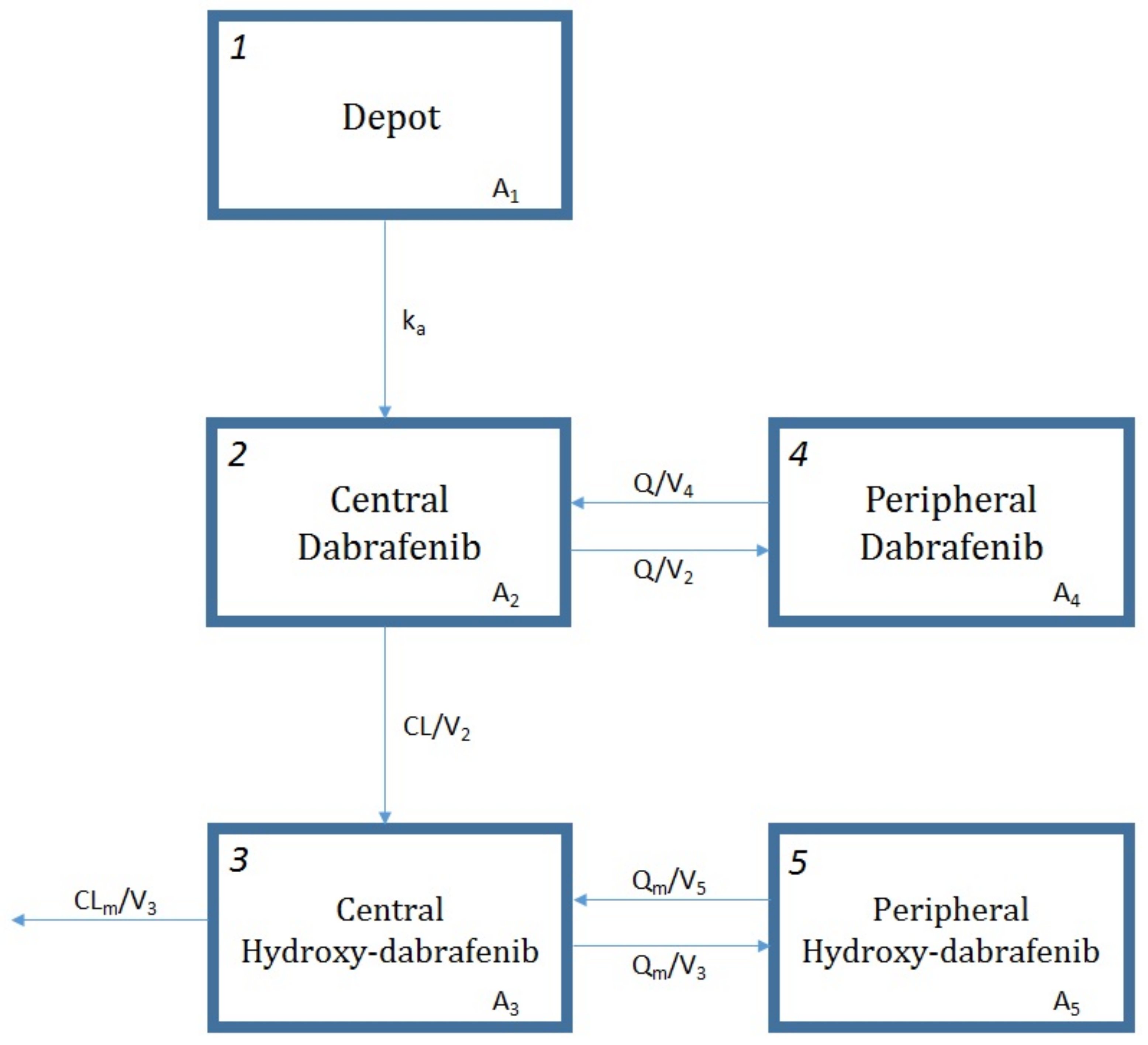
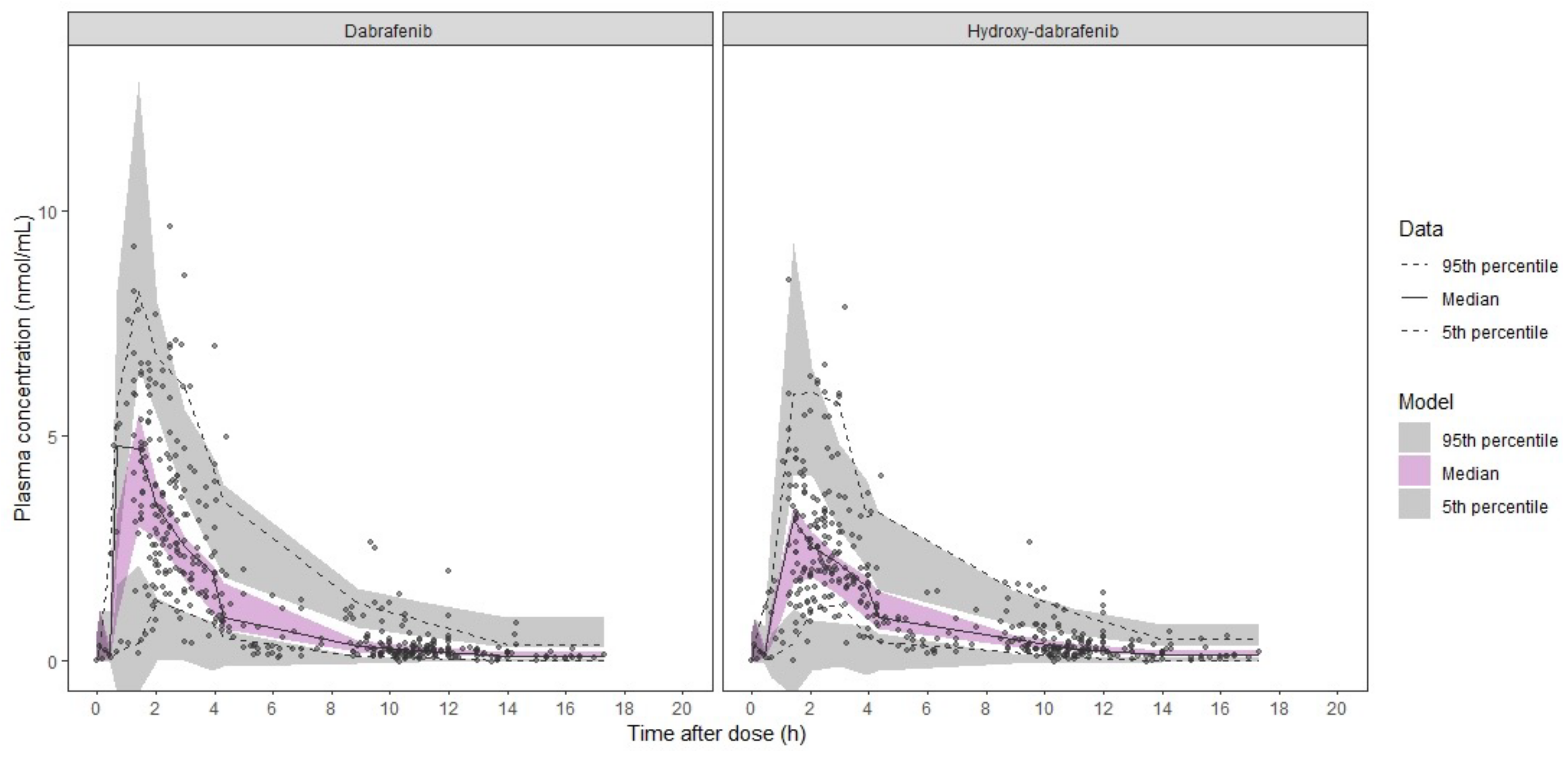
2.2.1. Dabrafenib/Hydroxy-dabrafenib Model
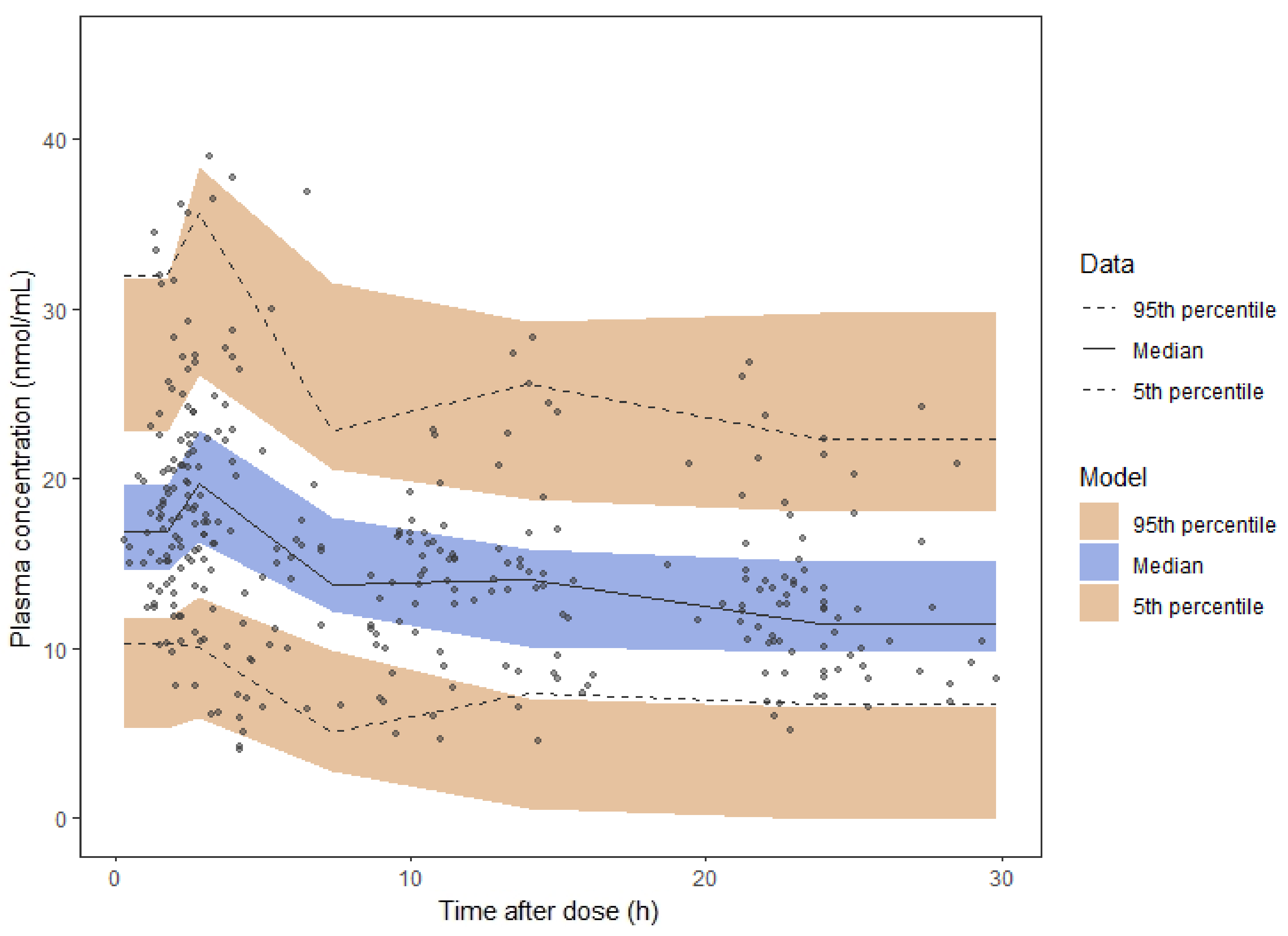
2.2.2. Trametinib Model
2.3. Exposure-Toxicity Relationship
2.4. Exposure-Survival Relationship
3. Discussion
4. Materials and Methods
4.1. Ethics
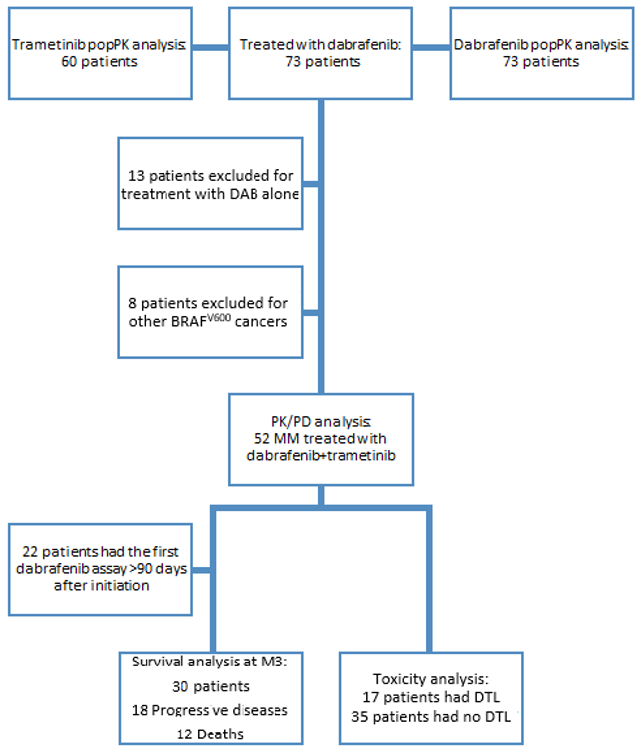
4.2. Study Population
4.3. Analytical Method
4.4. Population Pharmacokinetic Analysis
4.4.1. Structural and Statistical Model
4.4.2. Covariate Analysis
4.4.3. Parameter Estimation and Model Selection
4.4.4. Model Validation and Assessment
4.5. Pharmacokinetic/Pharmacodynamic Analysis
4.6. Statistical Analysis for Survival and Toxicity
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Roskoski, R., Jr. Targeting oncogenic Raf protein-serine/threonine kinases in human cancers. Pharmacol. Res. 2018, 135, 239–258. [Google Scholar] [CrossRef]
- Zaman, A.; Wu, W.; Bivona, T.G. Targeting Oncogenic BRAF: Past, Present, and Future. Cancers (Basel) 2019, 16, 11. [Google Scholar] [CrossRef] [Green Version]
- Puszkiel, A.; Noé, G.; Bellesoeur, A.; Kramkimel, N.; Paludetto, M.N.; Thomas-Schoemann, A.; Vidal, M.; Goldwasser, F.; Chatelut, E.; Blanchet, B. Clinical Pharmacokinetics and Pharmacodynamics of Dabrafenib. Clin. Pharmacokinet. 2019, 58, 451–467. [Google Scholar] [CrossRef]
- Robert, C.; Grob, J.J.; Stroyakovskiy, D.; Karaszewska, B.; Hauschild, A.; Levchenko, E.; Chiarion Sileni, V.; Schachter, J.; Garbe, C.; Bondarenko, I.; et al. Five-Year Outcomes with Dabrafenib plus Trametinib in Metastatic Melanoma. N. Engl. J. Med. 2019, 381, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Rousset, M.; Dutriaux, C.; Bosco-Lévy, P.; Prey, S.; Pham-Ledard, A.; Dousset, L.; Gérard, E.; Bouchet, S.; Canal-Raffin, M.; Titier, K.; et al. Trough dabrafenib plasma concentrations can predict occurrence of adverse events requiring dose reduction in metastatic melanoma. Clin. Chim. Acta 2017, 472, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Knispel, S.; Zimmer, L.; Kanaki, T.; Ugurel, S.; Schadendorf, D.; Livingstone, E. The safety and efficacy of dabrafenib and trametinib for the treatment of melanoma. Expert Opin. Drug Saf. 2018, 17, 73–87. [Google Scholar] [CrossRef]
- Puszkiel, A.; White-Koning, M.; Dupin, N.; Kramkimel, N.; Thomas-Schoemann, A.; Noé, G.; Chapuis, N.; Vidal, M.; Goldwasser, F.; Chatelut, E.; et al. Plasma vemurafenib exposure and pre-treatment hepatocyte growth factor level are two factors contributing to the early peripheral lymphocytes depletion in BRAF-mutated melanoma patients. Pharmacol. Res. 2016, 113, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Funck-Brentano, E.; Alvarez, J.C.; Longvert, C.; Abe, E.; Beauchet, A.; Funck-Brentano, C.; Saiag, P. Plasma vemurafenib concentrations in advanced BRAFV600mut melanoma patients: Impact on tumour response and tolerance. Ann. Oncol. 2015, 6, 1470–1475. [Google Scholar] [CrossRef] [PubMed]
- Kichenadasse, G.; Hughes, J.H.; Miners, J.O.; Mangoni, A.A.; Rowland, A.; Hopkins, A.M.; Sorich, M.J. Relationship between vemurafenib plasma concentrations and survival outcomes in patients with advanced melanoma. Cancer Chemother. Pharmacol. 2020, 85, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Kramkimel, N.; Thomas-Schoemann, A.; Sakji, L.; Golmard, J.; Noe, G.; Regnier-Rosencher, E.; Chapuis, N.; Maubec, E.; Vidal, M.; Avril, M.; et al. Vemurafenib pharmacokinetics and its correlation with efficacy and safety in outpatients with advanced BRAF-mutated melanoma. Target. Oncol. 2016, 11, 59–69. [Google Scholar] [CrossRef]
- Menzies, A.M.; Ashworth, M.T.; Swann, S.; Kefford, R.F.; Flaherty, K.; Weber, J.; Infante, J.R.; Kim, K.B.; Gonzalez, R.; Hamid, O.; et al. Characteristics of pyrexia in BRAFV600E/K metastatic melanoma patients treated with combined dabrafenib and trametinib in a phase I/II clinical trial. Ann. Oncol. 2015, 26, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Duong, J.K.; Gonzalez, M.; Long, G.V.; Menzies, A.M.; Rizos, H.; Lim, S.Y.; Lee, J.; Boddy, A.V. Pharmacokinetic and cytokine profiles of melanoma patients with dabrafenib and trametinib-induced pyrexia. Cancer Chemother. Pharmacol. 2019, 83, 693–704. [Google Scholar] [CrossRef]
- Falchook, G.S.; Long, G.V.; Kurzrock, R.; Kim, K.B.; Arkenau, H.T.; Brown, M.P.; Hamid, O.; Infante, J.R.; Millward, M.; Pavlick, A.; et al. Dose selection, pharmacokinetics, and pharmacodynamics of BRAF inhibitor dabrafenib (GSK2118436). Clin. Cancer Res. 2014, 20, 4449–4458. [Google Scholar] [CrossRef] [Green Version]
- Ouellet, D.; Kassir, N.; Chiu, J.; Mouksassi, M.S.; Leonowens, C.; Cox, D.; DeMarini, D.J.; Gardner, O.; Crist, W.; Patel, K. Population pharmacokinetics and exposure-response of trametinib, a MEK inhibitor, in patients with BRAF V600 mutation-positive melanoma. Cancer Chemother. Pharmacol. 2016, 77, 807–817. [Google Scholar] [CrossRef]
- Kim, K.B.; Kefford, R.; Pavlick, A.C.; Infante, J.R.; Ribas, A.; Sosman, J.A.; Fecher, L.A.; Millward, M.; McArthur, G.A.; Hwu, P.; et al. Phase II study of the MEK1/MEK2 inhibitor Trametinib in patients with metastatic BRAF-mutant cutaneous melanoma previously treated with or without a BRAF inhibitor. J. Clin. Oncol. 2013, 31, 482–489. [Google Scholar] [CrossRef] [Green Version]
- Flaherty, K.T.; Robert, C.; Hersey, P.; Nathan, P.; Garbe, C.; Milhem, M.; Demidov, L.V.; Hassel, J.C.; Rutkowski, P.; Mohr, P.; et al. METRIC Study Group. Improved survival with MEK inhibition in BRAF-mutated melanoma. N. Engl. J. Med. 2012, 367, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.Y.; Upadhyay, P.J.; Fahmy, A.; Liu, X.; Duong, J.K.; Boddy, A.V. Clinical Pharmacokinetic and Pharmacodynamic Considerations in the (Modern) Treatment of Melanoma. Clin. Pharmacokinet. 2019, 58, 1029–1043. [Google Scholar] [CrossRef]
- Ouellet, D.; Gibiansky, E.; Leonowens, C.; O’Hagan, A.; Haney, P.; Switzky, J.; Goodman, V.L. Population pharmacokinetics of dabrafenib, a BRAF inhibitor: Effect of dose, time, covariates, and relationship with its metabolites. J. Clin. Pharmacol. 2014, 54, 696–706. [Google Scholar] [CrossRef]
- Sharma, M.; Holmes, H.M.; Mehta, H.B.; Chen, H.; Aparasu, R.R.; Shih, Y.T.; Giordano, S.H.; Johnson, M.L. The Concomitant Use of Tyrosine Kinase Inhibitors and Proton Pump Inhibitors: Prevalence, Predictors, and Impact on Survival and Discontinuation of Therapy in Older Adults with Cancer. Cancer 2019, 125, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, R.W.F.; Jansman, F.G.A.; Hunfeld, N.G.; Peric, R.; Reyners, A.K.L.; Imholz, A.L.T.; Brouwers, J.R.B.J.; Aerts, J.G.; Van Gelder, T.; Mathijssen, R.H.J. Tyrosine Kinase Inhibitors and Proton Pump Inhibitors: An Evaluation of Treatment Options. Clin. Pharmacokinet. 2017, 56, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Chu, M.P.; Ghosh, S.; Chambers, C.R.; Basappa, N.; Butts, C.A.; Chu, Q.; Fenton, D.; Joy, A.A.; Sangha, R.; Smylie, M.; et al. Gastric Acid suppression is associated with decreased erlotinib efficacy in non-small-cell lung cancer. Clin. Lung Cancer 2015, 16, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Mir, O.; Touati, N.; Lia, M.; Litière, S.; Le Cesne, A.; Sleijfer, S.; Blay, J.Y.; Leahy, M.; Young, R.; Mathijssen, R.H.J.; et al. Impact of Concomitant Administration of Gastric Acid-Suppressive Agents and Pazopanib on Outcomes in Soft-Tissue Sarcoma Patients Treated within the EORTC 62043/62072 Trials. Clin. Cancer Res. 2019, 25, 1479–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. Committee for Medicinal Products for Human Use (CHMP) Assessment Report: Tafinlar (dabrafenib). 2013. Available online: https://www.ema.europa.eu/en/documents/product-information/tafinlar-epar-product-information_en.pdf (accessed on 20 February 2020).
- European Medicines Agency. Committee for Medicinal Products for Human Use (CHMP) Assessment Report: Mekinist (trametinib). 2014. Available online: https://www.ema.europa.eu/en/documents/product-information/mekinist-epar-product-information_en.pdf (accessed on 20 February 2020).
- Robert, C.; Karaszewska, B.; Schachter, J.; Rutkowski, P.; Mackiewicz, A.; Stroiakovski, D.; Lichinitser, M.; Dummer, R.; Grange, F.; Mortier, L.; et al. Improved overall survival in melanoma with combined dabrafenib and trametinib. N. Engl. J. Med. 2015, 372, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Dummer, R.; Brase, J.C.; Garrett, J.; Campbell, C.D.; Gasal, E.; Squires, M.; Gusenleitner, D.; Santinami, M.; Atkinson, V.; Mandalà, M.; et al. Adjuvant dabrafenib plus trametinib versus placebo in patients with resected, BRAFV600-mutant, stage III melanoma (COMBI-AD): Exploratory biomarker analyses from a randomised, phase 3 trial. Lancet Oncol. 2020, 21, 358–372. [Google Scholar] [CrossRef]
- Atkinson, V.; Sandhu, S.; Hospers, G.; Long, G.V.; Aglietta, M.; Ferrucci, P.F.; Tulyte, S.; Cappellini, G.C.A.; Soriano, V.; Ali, S.; et al. Dabrafenib plus trametinib is effective in the treatment of BRAF V600-mutated metastatic melanoma patients: Analysis of patients from the dabrafenib plus trametinib Named Patient Program (DESCRIBE II). Melanoma Res. 2019. [Google Scholar] [CrossRef]
- Hauschild, A.; Larkin, J.; Ribas, A.; Dréno, B.; Flaherty, K.T.; Ascierto, P.A.; Lewis, K.D.; McKenna, E.; Zhu, Q.; Mun, Y.; et al. Modeled Prognostic Subgroups for Survival and Treatment Outcomes in BRAF V600–Mutated Metastatic Melanoma: Pooled Analysis of 4 Randomized Clinical Trials. JAMA Oncol. 2018, 4, 1382–1388. [Google Scholar] [CrossRef] [Green Version]
- Manola, J.; Atkins, M.; Ibrahim, J.; Kirkwood, J. Prognostic factors in metastatic melanoma: A pooled analysis of Eastern Cooperative Oncology Group trials. J. Clin. Oncol. 2000, 18, 3782–3793. [Google Scholar] [CrossRef]
- Noé, G.; Bellesoeur, A.; Thomas-Schoemann, A.; Rangarajan, S.; Naji, F.; Puszkiel, A.; Huillard, O.; Saidu, N.; Golmard, L.; Alexandre, J.; et al. Clinical and kinomic analysis identifies peripheral blood mononuclear cells as a potential pharmacodynamic biomarker in metastatic renal cell carcinoma patients treated with sunitinib. Oncotarget 2016, 7, 67507–67520. [Google Scholar] [CrossRef] [Green Version]
- Miao, W.; Wang, Y. Quantitative Interrogation of the Human Kinome Perturbed by Two BRAF Inhibitors. J. Proteome Res. 2019, 18, 2624–2631. [Google Scholar] [CrossRef]
- Bowyer, S.; Lee, R.; Fusi, A.; Lorigan, P. Dabrafenib and its use in the treatment of metastatic melanoma. Melanoma Manag. 2015, 2, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.L.; Stuhlmiller, T.J.; Angus, S.P.; Zawistowski, J.S.; Graves, L.M. Molecular pathways: Adaptive kinome reprogramming in response to targeted inhibition of the BRAF-MEK-ERK pathway in cancer. Clin. Cancer Res. 2014, 20, 2516–2522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beal, S.; Sheiner, L.B.; Boeckmann, A.; Bauer, R.J. NONMEM User’s Guides (1989–2009); Icon Development Solutions: Dublin, Ireland, 2009. [Google Scholar]
- Lindbom, L.; Pihlgren, P.; Jonsson, E.N. PsN-Toolkit—A collection of computer intensive statistical methods for non-linear mixed effect modeling using NONMEM. Comput. Methods Programs Biomed. 2005, 79, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Bershas, D.A.; Ouellet, D.; Mamaril-Fishman, D.B.; Nebot, N.; Carson, S.W.; Blackman, S.C.; Morrison, R.A.; Adams, J.L.; Jurusik, K.E.; Knecht, D.M.; et al. Metabolism and disposition of oral dabrafenib in cancer patients: Proposed participation of aryl nitrogen in carbon-carbon bond cleavage via decarboxylation following enzymatic oxidation. Drug Metab. Dispos. 2013, 41, 2215–2224. [Google Scholar] [CrossRef] [PubMed]
- Janmahasatian, S.; Duffull, S.B.; Ash, S.; Ward, L.C.; Byrne, N.M.; Green, B. Quantification of Lean Bodyweight. Clin. Pharmacokinet. 2005, 44, 1051–1065. [Google Scholar] [CrossRef]
- Keizer, R. Package ‘vpc’-Create Visual Predictive Checks. 2018. Available online: https://cran.r-project.org/web/packages/vpc (accessed on 20 February 2020).
- Astrand, M. Package ‘nonmem2R’-Loading NONMEM Output Files with Functions for Visual Predictive Checks (VPC) and Goodness of Fit (GOF) Plots. 2019. Available online: https://cran.r-project.org/web/packages/nonmem2R (accessed on 20 February 2020).
- Sheiner, L.B.; Beal, S.L. Some suggestions for measuring predictive performance. J. Pharmacokinet Biopharm. 1981, 9, 503–512. [Google Scholar] [CrossRef]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; Van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | DAB/OHD Model (n = 73) | TRA Model (n = 60) |
|---|---|---|
| Demographic Data | ||
| Sex, n (%) | ||
| Male/Female | 43 (59)/30 (41) | 33 (55)/27 (45) |
| Age (years) | 61.2 (20.0–90.0) | 60.0 (20.0–90.0) |
| Body weight (kg) | 73.0 (51.7–166.0) | 73.0 (53.0–166.0) |
| BMI (kg/m2) | 25.9 (17.4–44.6) | 25.9 (18.3–44.6) |
| FFM (kg) | 53.7 (34.2–94.4) | 52.7 (34.7–94.4) |
| BSA (m2) | 1.9 (1.0–3.0) | 3.1 (2.5–3.0) |
| Histological tumor type, n (%) | ||
| Melanoma | 65 (89) | 52 (87) |
| Other a | 8 (11) | 8 (13) |
| PPI intake, (n %) | ||
| Yes/No | 57 (78)/16 (22) | 52 (87)/8 (13) |
| Baseline Biological Data | ||
| AST (UI/L) | 30.0 (12.0–103.0) | 30.0 (12.0–103.0) |
| ALT (UI/L) | 28.0 (10.0–116) | 28.0 (13.0–116.0) |
| Total bilirubin (µmol/L) | 6.3 (1.4–47.0) | 6.3 (1.4–47.0) |
| Albumin (g/L) | 43.0 (23.0–49.0) | 43.0 (31.0–48.0) |
| CRP (mg/L) | 19.9 (1.0–248.0) | 17.2 (1.0–248.0) |
| Baseline Characteristics of MM Patients (n = 52) b | ||
| 8th AJCC stage | ||
| Stage IIIC, n (%) | 5 (10) | |
| Stage IV M1a, n (%) | 8 (15) | |
| Stage IV M1b, n (%) | 3 (6) | |
| Stage IV M1c, n (%) | 16 (31) | |
| Stage IV M1d, n (%) | 20 (38) | |
| ECOG PS, n (%) | ||
| 0 | 29 (56) | |
| 1 | 16 (31) | |
| 2 | 5 (9) | |
| 3 | 2 (4) | |
| Number of previous treatment lines, n (%) | ||
| 0 | 35 (67) | |
| 1 | 10 (19) | |
| ≥2 | 7 (14) | |
| Number of metastatic sites, n (%) | ||
| <3/≥3 | 25 (48)/27 (52) | |
| Cerebral metastases, n (%) | ||
| Yes/No | 31 (60)/21 (40) | |
| LDH, n (%) | 19.9 (1.0–248.0) | |
| <1.5 N | 39 (75) | |
| ≥1.5 N | 13 (25) | |
| Parameters | Base DAB/OHD Model | Final DAB/OHD Model | Bootstrap (n = 500 Samples) | |||
|---|---|---|---|---|---|---|
| Estimate | RSE (%) | Estimate | RSE (%) | Median | PI95% | |
| CL/F (L/h) | 17.7 | 6.4 | 19.3 | 7.5 | 19.2 | 16.0–22.4 |
| V2/F (L) | 39.5 | 13.1 | 39.1 | 13.7 | 38.3 | 26.9–52.1 |
| ka (1/h) | 1.8 fixed | 1.8 fixed | 1.8 fixed | |||
| Q/F (L/h) | 3.85 | 23.0 | 3.40 | 21.5 | 3.32 | 1.59–6.60 |
| V4/F (L) | 19.6 | 19.6 | 18.7 | 20.1 | 18.7 | 12.5–39.8 |
| CLm/F (L/h) | 22.8 | 5.8 | 23.2 | 5.9 | 22.9 | 19.8–25.9 |
| V3/F (L) | 5.23 | 26.2 | 5.11 | 30.5 | 4.99 | 0.385–9.03 |
| Qm/F (L/h) | 7.39 | 23.7 | 7.21 | 22.3 | 7.02 | 4.42–12.1 |
| V5/F (L) | 25.7 | 20.4 | 27.1 | 23.9 | 24.7 | 16.1–45.8 |
| Tlag (h) | 0.50 | 0.20 | 0.499 | 0.2 | 0.499 | 0.295–0.578 |
| θage/(CL/F) | - | - | −0.536 | 28.4 | −0.499 | −0.827−0.215 |
| θage/(CLm/F) | - | - | −0.589 | 33.6 | −0.543 | −0.879−0.168 |
| θsex/(CL/F) | - | - | 0.832 | 6.4 | 0.829 | 0.732–0.932 |
| IIVCL/F (%) | 21.9 | 17.2 | 16.0 | 21.9 | 14.4 | 5.83–20.9 |
| IIVV2/F (%) | 43.0 | 18.1 | 50.8 | 20.0 | 69.4 | 44.3–88.9 |
| IIVCLm/F (%) | 26.8 | 11.9 | 24.0 | 14.4 | 21.8 | 15.5–28.5 |
| IIVV3/F (%) | 84.0 | 47.5 | 47.5 | 51.5 | 82.0 | 15.9–278 |
| IOV (%) | 17.2 | 11.8 | 17.4 | 12.0 | 17.0 | 13.1–20.3 |
| RUV of DAB (%) | 49.2 | 6.4 | 48.7 | 6.6 | 48.2 | 41.8–54.6 |
| RUV of OHD (%) | 53.1 | 6.4 | 53.1 | 6.3 | 52.7 | 46.2–59.1 |
| RUVcorr (%) | 87.3 | 11.5 | 87.0 | 2.1 | 87.3 | 80.4–92.1 |
| Parameters | Final TRA Model | Bootstrap (n = 500 Samples) | ||
|---|---|---|---|---|
| Estimate | RSE (%) | Median | PI95% | |
| CL/F (L/h) | 5.83 | 4.6 | 5.82 | 5.35–6.35 |
| V2/F (L) | 61.9 | 26.8 | 65.1 | 22.3–125.4 |
| ka (1/h) | 0.913 | 38.2 | 1.04 | 0.390–3.10 |
| Q/F (L/h) | 64.9 | 23.4 | 62.6 | 33.6–116.8 |
| V3/F (L) | 417.0 | 42.2 | 448.2 | 193.9–2145.0 |
| Tlag (h) | 0.709 | 17.1 | 0.728 | 0.505–1.06 |
| IIVCL/F (%) | 29.6 | 16.3 | 28.6 | 18.9–38.0 |
| IIVQ (%) | 80.2 | 23.7 | 80.1 | 30.6–167.1 |
| RUV (ng/mL) | 4.14 | 6.2 | 4.10 | 3.69–4.61 |
| Parameters | DLT | No DLT | p Value |
|---|---|---|---|
| Dabrafenib/Hydroxy-dabrafenib | |||
| AUCDAB (ng∙h/mL) | 9624 (8121–11676) | 7485 (3399–17712) | 0.0065 |
| AUCOHD (ng∙h/mL) | 7509.5 (4918–10300) | 5812 (2459–10300) | 0.16 |
| AUCCOMPOSITE (ng∙h/mL) | 16855 (13491–21976) | 13605 (5877–28012) | 0.030 |
| Age * (years) | 54.5 (37–81) | 59 (20–90) | 0.66 |
| BMI * (kg/m2) | 25.9 (20.4–33.4) | 25.1 (19.6–40.9) | 0.87 |
| Sex | 0.094 | ||
| Male | 8 (67%) | 14 (35%) | |
| Female | 4 (33%) | 26 (65%) | |
| ECOG PS * | 0.51 | ||
| 0-1 | 8 (67%) | 21 (52%) | |
| ≥2 | 4 (33%) | 19 (48%) | |
| LDH | 0.47 | ||
| <1.5N | 10 (83%) | 27 (68%) | |
| ≥1.5N | 2 (17%) | 13 (32%) | |
| Trametinib | |||
| AUCTRA (ng∙h/mL) | 268 (144–448) | 268 (111–750) | 0.47 |
| Age * (years) | 55 (37–90) | 61 (20–89) | 0.61 |
| BMI * (kg/m2) | 25.9 (20.4–35.5) | 25.2 (19.6–40.9) | 0.68 |
| Sex | 0.37 | ||
| Male | 9 (53) | 13 (37) | |
| Female | 8 (47) | 22 (63) | |
| ECOG PS * | 1 | ||
| 0–1 | 10 (59) | 19 (54) | |
| ≥2 | 7 (41) | 16 (46) | |
| LDH | 0.33 | ||
| <1.5N | 9 (53) | 20 (57) | |
| ≥1.5N | 8 (47) | 15 (43) | |
| Univariate Model | Risk of Death | Risk of Progression | ||
|---|---|---|---|---|
| HR (CI95%) | p Value | HR (CI95%) | p Value | |
| Sex | 1.47 (0.46–4.67) | 0.51 | 1.04 (0.44–2.47) | 0.82 |
| Age | 1.01 (0.97–1.05) | 0.64 | 0.99 (0.96–1.02) | 0.63 |
| BMI | 1.01 (0.86–1.18) | 0.89 | 0.99 (0.87–1.12) | 0.84 |
| ECOG PS ≥2 | 6.64 (1.31–33.78) | 0.022 | 1.98 (0.72–5.46) | 0.19 |
| Number of metastatic sites ≥3 | 3.20 (0.86–11.93) | 0.083 | 3.64 (1.27–10.39) | 0.016 |
| Cerebral metastases | 2.51 (0.79–7.96) | 0.12 | 4.05 (1.47–11.19) | 0.0070 |
| PPI | 3.51 (0.90–13.71) | 0.071 | 1.80 (0.51–6.38) | 0.57 |
| LDH | 0.55 (0.12–2.52) | 0.44 | 1.03 (0.36–2.90) | 0.96 |
| AUCM3 DAB | 1.02 (0.75–1.39) | 0.88 | 1.04 (0.82–1.32) | 0.75 |
| AUCM3 OHD | 1.64 (1.09–2.48) | 0.019 | 1.37 (1.02–1.83) | 0.037 |
| AUCM3 Composite | 1.15 (0.93–1.43) | 0.20 | 1.11 (0.94–1.30) | 0.21 |
| AUCM3 ratio OH/DAB | 4.11 (1.18–14.29) | 0.026 | 1.66 (0.62–4.46) | 0.31 |
| AUCM3 TRA | 1.37 (0.94–1.98) | 0.10 | 1.31 (0.93–1.83) | 0.12 |
| Multivariate models | HR (CI95%) | p value | HR (CI95%) | p value |
| Using AUCM3,OHD | ||||
| ECOG PS≥2 | 6.58 (1.29–33.56) | 0.023 | ||
| AUCM3,OHD | 1.61 (1.07–2.45) | 0.023 | ||
| Using AUCM3,OHD/DAB | ||||
| ECOG PS≥2 | 16.52 (2.51–108.86) | 0.0036 | ||
| AUCM3,OHD/DAB | 10.61 (2.34–48.15) | 0.0022 | ||
| Using AUCM3,OHD | ||||
| Number of metastasis site ≥3 | 3.25 (1.11–9.50) | 0.032 | ||
| AUCM3,OHD | 1.27 (0.97–1.68) | 0.088 | ||
| Using AUCM3,OHD | ||||
| Cerebral metastases | 1.23 (1.35–10.39) | 0.011 | ||
| AUCM3,OHD | 1.29 (0.99–1.68) | 0.064 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balakirouchenane, D.; Guégan, S.; Csajka, C.; Jouinot, A.; Heidelberger, V.; Puszkiel, A.; Zehou, O.; Khoudour, N.; Courlet, P.; Kramkimel, N.; et al. Population Pharmacokinetics/Pharmacodynamics of Dabrafenib Plus Trametinib in Patients with BRAF-Mutated Metastatic Melanoma. Cancers 2020, 12, 931. https://doi.org/10.3390/cancers12040931
Balakirouchenane D, Guégan S, Csajka C, Jouinot A, Heidelberger V, Puszkiel A, Zehou O, Khoudour N, Courlet P, Kramkimel N, et al. Population Pharmacokinetics/Pharmacodynamics of Dabrafenib Plus Trametinib in Patients with BRAF-Mutated Metastatic Melanoma. Cancers. 2020; 12(4):931. https://doi.org/10.3390/cancers12040931
Chicago/Turabian StyleBalakirouchenane, David, Sarah Guégan, Chantal Csajka, Anne Jouinot, Valentine Heidelberger, Alicja Puszkiel, Ouidad Zehou, Nihel Khoudour, Perrine Courlet, Nora Kramkimel, and et al. 2020. "Population Pharmacokinetics/Pharmacodynamics of Dabrafenib Plus Trametinib in Patients with BRAF-Mutated Metastatic Melanoma" Cancers 12, no. 4: 931. https://doi.org/10.3390/cancers12040931