Personalized Indicator Thrombocytosis Shows Connection to Staging and Indicates Shorter Survival in Colorectal Cancer Patients with or without Type 2 Diabetes


Abstract
:1. Introduction
2. Results
2.1. Measurements at the Time of Colorectal Cancer Diagnosis
2.2. Pre-Tumor Complete Blood Count Measurements
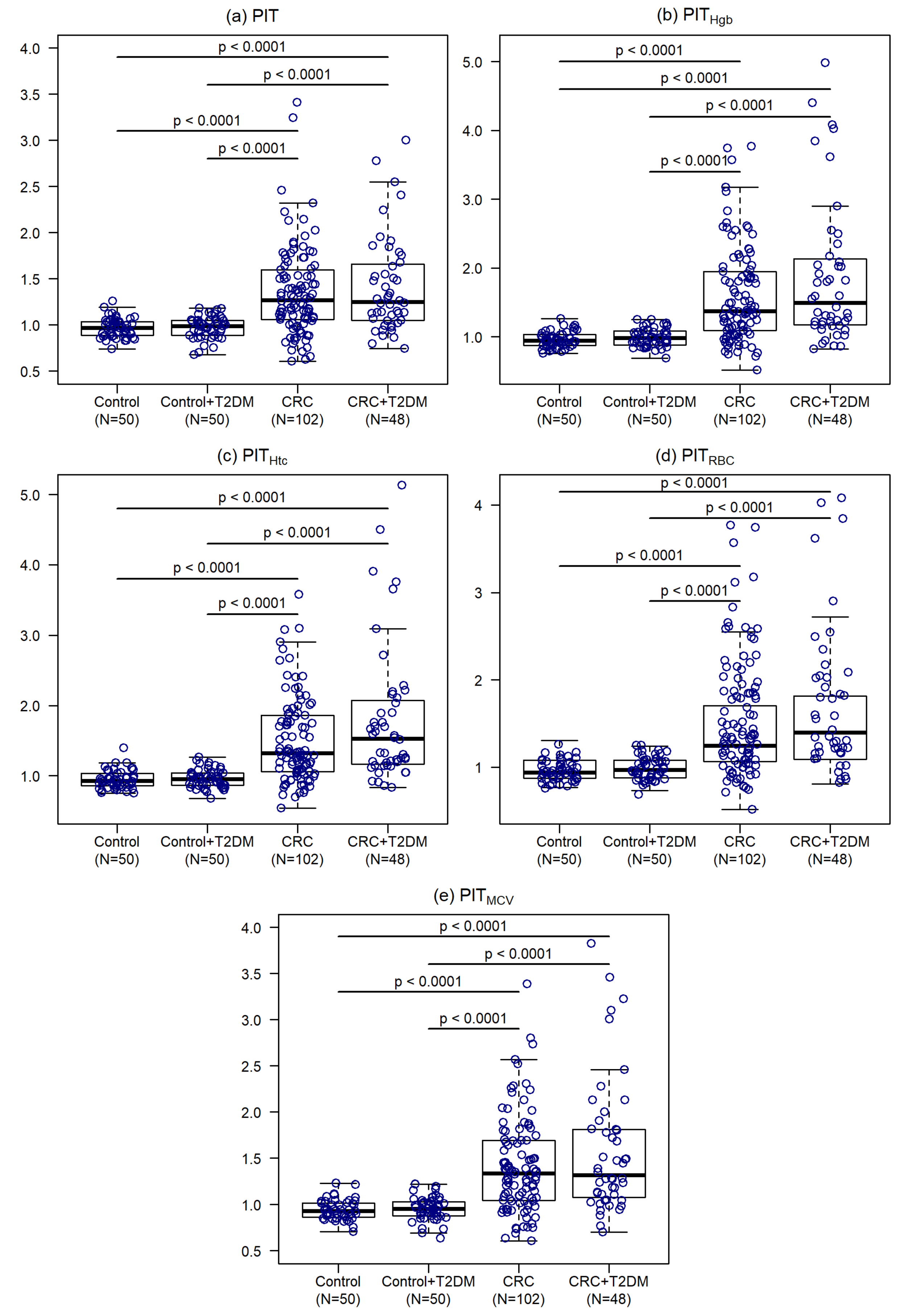
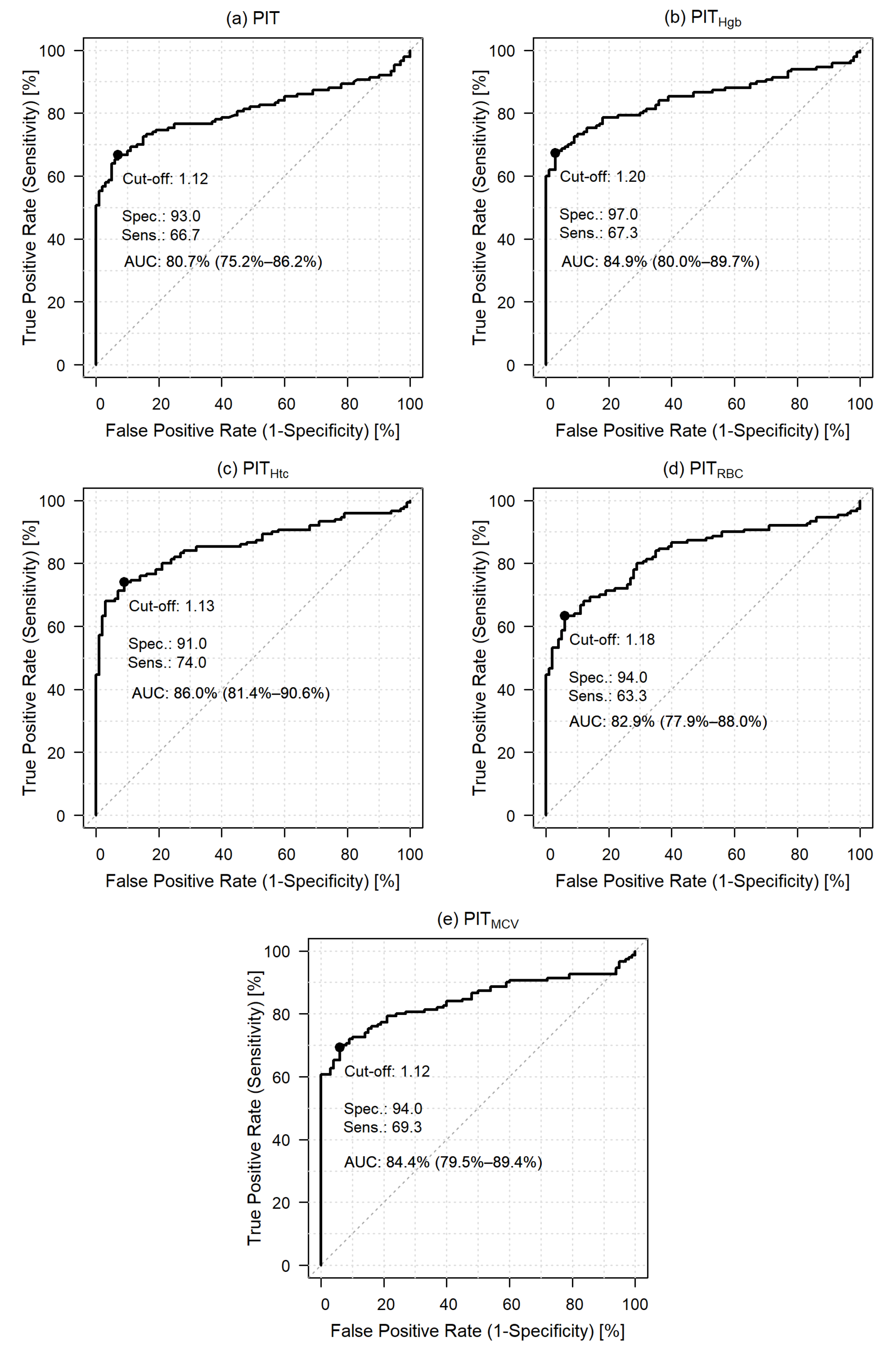
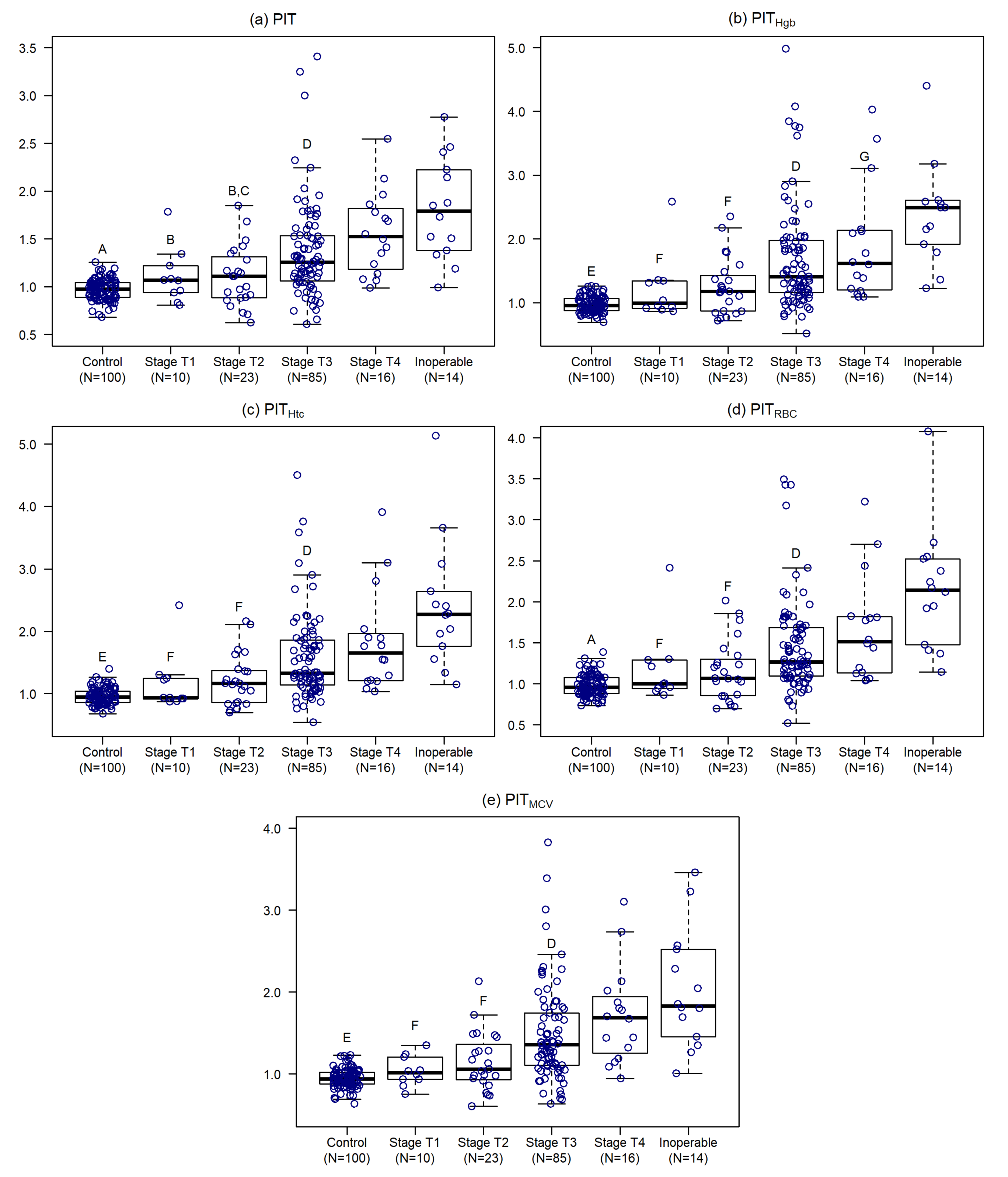
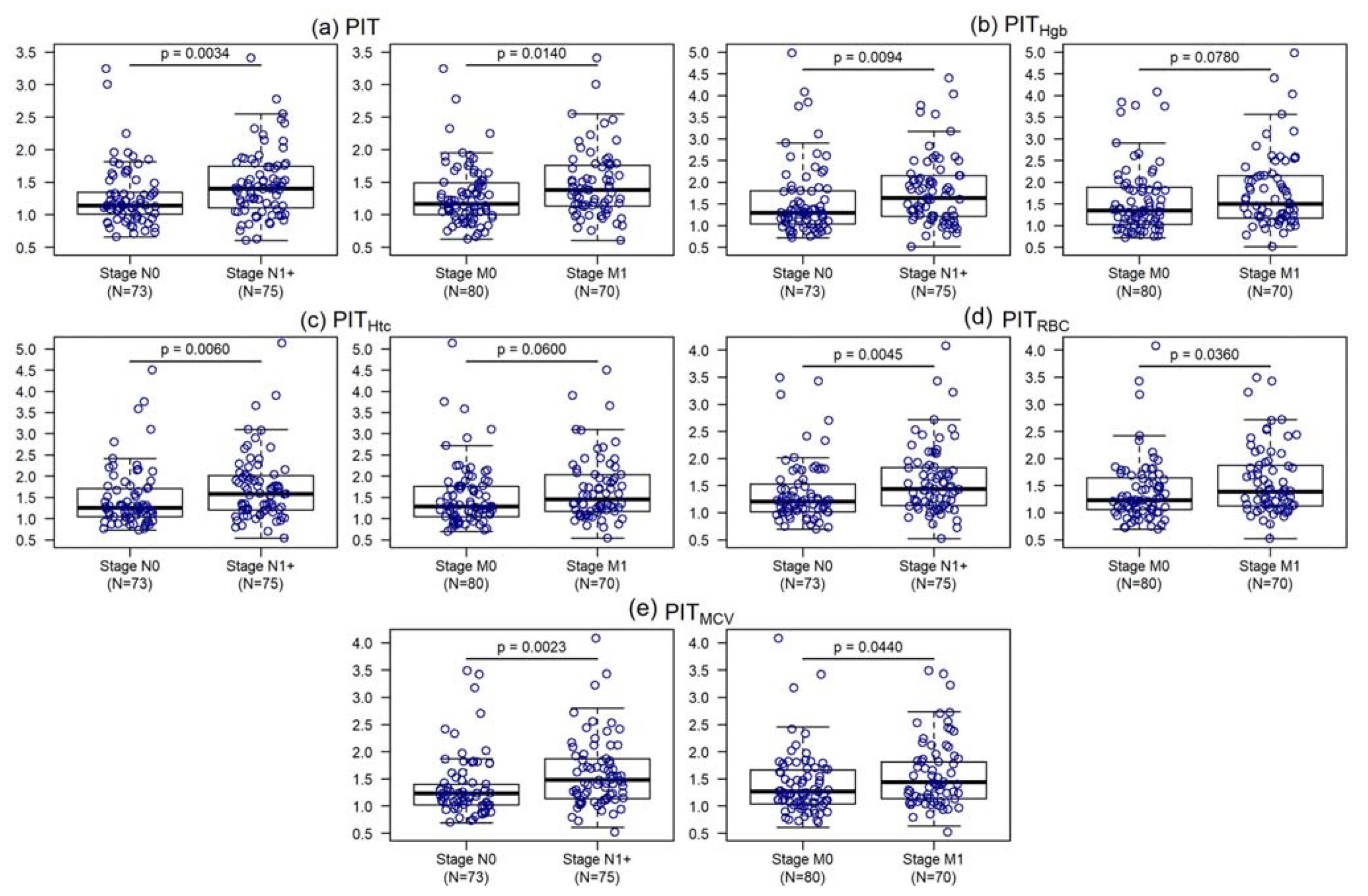
2.3. Personalized Indicator Thrombocytosis
2.3.1. Relationship of Personalized Indicator Thrombocytosis to other Grouping Variables
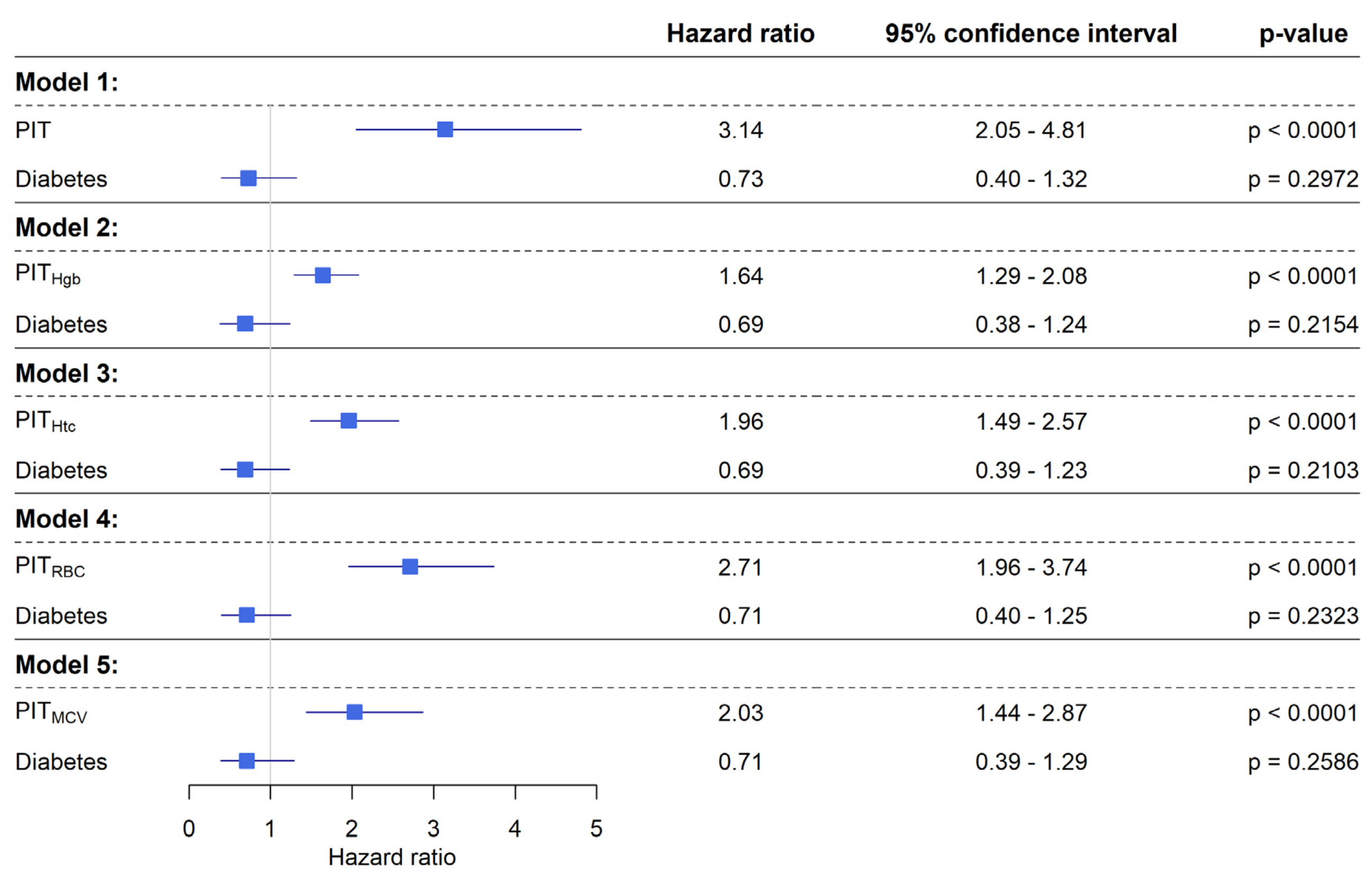
2.3.2. Survival Analysis of Personalized Indicator Thrombocytosis
3. Discussion
4. Materials and Methods
4.1. Patients and Study Design
4.2. Clinical and Laboratory Data Measurements
4.3. Personalized Indicator Thrombocytosis
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Haemmerle, M.; Stone, R.L.; Menter, D.G.; Afshar-Kharghan, V.; Sood, A.K. The Platelet Lifeline to Cancer: Challenges and Opportunities. Cancer Cell 2018, 33, 965–983. [Google Scholar] [CrossRef] [PubMed]
- Trousseau, A. Phlegmasia alba dolens. Lecutres Clin. Med. 1865, 5, 281–333. [Google Scholar]
- Camerer, E.; Qazi, A.A.; Duong, D.N.; Cornelissen, I.; Advincula, R.; Coughlin, S.R. Platelets, protease-activated receptors, and fibrinogen in hematogenous metastasis. Blood 2004, 104, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Labelle, M.; Begum, S.; Hynes, R.O. Direct signaling between platelets and cancer cells induces an epithelial-mesenchymal-like transition and promotes metastasis. Cancer Cell 2011, 20, 576–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieswandt, B.; Hafner, M.; Echtenacher, B.; Mannel, D.N. Lysis of tumor cells by natural killer cells in mice is impeded by platelets. Cancer Res. 1999, 59, 1295–1300. [Google Scholar]
- Palumbo, J.S.; Talmage, K.E.; Massari, J.V.; La Jeunesse, C.M.; Flick, M.J.; Kombrinck, K.W.; Jirouskova, M.; Degen, J.L. Platelets and fibrin(ogen) increase metastatic potential by impeding natural killer cell-mediated elimination of tumor cells. Blood 2005, 105, 178–185. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, D.; Strilic, B.; Sivaraj, K.K.; Wettschureck, N.; Offermanns, S. Platelet-Derived Nucleotides Promote Tumor-Cell Transendothelial Migration and Metastasis via P2Y(2) Receptor. Cancer Cell 2013, 24, 130–137. [Google Scholar] [CrossRef] [Green Version]
- Erdemir, F.; Kilciler, M.; Bedir, S.; Ozgok, Y.; Coban, H.; Erten, K. Clinical significance of platelet count in patients with renal cell carcinoma. Urol. Int. 2007, 79, 111–116. [Google Scholar] [CrossRef]
- Heng, S.; Benjapibal, M. Preoperative thrombocytosis and poor prognostic factors in endometrial cancer. Asian Pac. J. Cancer Prev. 2014, 15, 10231–10236. [Google Scholar] [CrossRef] [Green Version]
- Monreal, M.; Fernandez-Llamazares, J.; Pinol, M.; Julian, J.F.; Broggi, M.; Escola, D.; Abad, A. Platelet count and survival in patients with colorectal cancer—A preliminary study. Thromb. Haemost. 1998, 79, 916–918. [Google Scholar] [CrossRef]
- Shimada, H.; Oohira, G.; Okazumi, S.; Matsubara, H.; Nabeya, Y.; Hayashi, H.; Takeda, A.; Gunji, Y.; Ochiai, T. Thrombocytosis associated with poor prognosis in patients with esophageal carcinoma. J. Am. Coll. Surg. 2004, 198, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Taucher, S.; Salat, A.; Gnant, M.; Kwasny, W.; Mlineritsch, B.; Menzel, R.C.; Schmid, M.; Smola, M.G.; Stierer, M.; Tausch, C.; et al. Impact of pretreatment thrombocytosis on survival in primary breast cancer. Thromb. Haemost. 2003, 89, 1098–1106. [Google Scholar] [PubMed]
- Bailey, S.E.; Ukoumunne, O.C.; Shephard, E.; Hamilton, W. How useful is thrombocytosis in predicting an underlying cancer in primary care? a systematic review. Fam. Pract. 2017, 34, 4–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, R.L.; Nick, A.M.; McNeish, I.A.; Balkwill, F.; Han, H.D.; Bottsford-Miller, J.; Rupairmoole, R.; Armaiz-Pena, G.N.; Pecot, C.V.; Coward, J.; et al. Paraneoplastic thrombocytosis in ovarian cancer. N. Engl. J. Med. 2012, 366, 610–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bleeker, J.S.; Hogan, W.J. Thrombocytosis: Diagnostic evaluation, thrombotic risk stratification, and risk-based management strategies. Thrombosis 2011, 2011, 536062. [Google Scholar] [CrossRef] [PubMed]
- Baranyai, Z.; Josa, V.; Toth, A.; Szilasi, Z.; Tihanyi, B.; Zarand, A.; Harsanyi, L.; Szallasi, Z. Paraneoplastic thrombocytosis in gastrointestinal cancer. Platelets 2016, 27, 269–275. [Google Scholar] [CrossRef] [Green Version]
- Ishizuka, M.; Nagata, H.; Takagi, K.; Iwasaki, Y.; Kubota, K. Preoperative thrombocytosis is associated with survival after surgery for colorectal cancer. J. Surg. Oncol. 2012, 106, 887–891. [Google Scholar] [CrossRef]
- Josa, V.; Krzystanek, M.; Eklund, A.C.; Salamon, F.; Zarand, A.; Szallasi, Z.; Baranyai, Z. Relationship of postoperative thrombocytosis and survival of patients with colorectal cancer. Int. J. Surg. 2015, 18, 1–6. [Google Scholar] [CrossRef]
- Baranyai, Z.; Krzystanek, M.; Josa, V.; Dede, K.; Agoston, E.; Szasz, A.M.; Sinko, D.; Szarvas, V.; Salamon, F.; Eklund, A.C.; et al. The comparison of thrombocytosis and platelet-lymphocyte ratio as potential prognostic markers in colorectal cancer. Thromb. Haemost. 2014, 111, 483–490. [Google Scholar] [CrossRef]
- Jones, C.I. Platelet function and ageing. Mamm. Genome 2016, 27, 358–366. [Google Scholar] [CrossRef] [Green Version]
- Le Blanc, J.; Lordkipanidze, M. Platelet Function in Aging. Front. Cardiovasc. Med. 2019, 6, 109. [Google Scholar] [CrossRef] [PubMed]
- Bonaccio, M.; Di Castelnuovo, A.; Costanzo, S.; De Curtis, A.; Donati, M.B.; Cerletti, C.; de Gaetano, G.; Iacoviello, L.; Investigators, M.-S. Age-sex-specific ranges of platelet count and all-cause mortality: Prospective findings from the MOLI-SANI study. Blood 2016, 127, 1614–1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaninetti, C.; Biino, G.; Noris, P.; Melazzini, F.; Civaschi, E.; Balduini, C.L. Personalized reference intervals for platelet count reduce the number of subjects with unexplained thrombocytopenia. Haematologica 2015, 100, e338–e340. [Google Scholar] [CrossRef] [PubMed]
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.E.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017. [Google Scholar]
- American Diabetes Association. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [Green Version]
- Giovannucci, E.; Harlan, D.M.; Archer, M.C.; Bergenstal, R.M.; Gapstur, S.M.; Habel, L.A.; Pollak, M.; Regensteiner, J.G.; Yee, D. Diabetes and cancer: A consensus report. CA Cancer J. Clin. 2010, 60, 207–221. [Google Scholar] [CrossRef] [Green Version]
- Shlomai, G.; Neel, B.; LeRoith, D.; Gallagher, E.J. Type 2 Diabetes Mellitus and Cancer: The Role of Pharmacotherapy. J. Clin. Oncol. 2016, 34, 4261–4269. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Earle, C.C.; Bae, S.J.; Fischer, H.D.; Yun, L.; Austin, P.C.; Rochon, P.A.; Anderson, G.M.; Lipscombe, L. Incidence of Diabetes in Colorectal Cancer Survivors. J. Natl. Cancer Inst. 2016, 108, djv402. [Google Scholar] [CrossRef] [Green Version]
- Tsilidis, K.K.; Kasimis, J.C.; Lopez, D.S.; Ntzani, E.E.; Ioannidis, J.P. Type 2 diabetes and cancer: Umbrella review of meta-analyses of observational studies. BMJ 2015, 350, g7607. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez, N.; Prieto, I.; Del Puerto-Nevado, L.; Portal-Nunez, S.; Ardura, J.A.; Corton, M.; Fernandez-Fernandez, B.; Aguilera, O.; Gomez-Guerrero, C.; Mas, S.; et al. 2017 update on the relationship between diabetes and colorectal cancer: Epidemiology, potential molecular mechanisms and therapeutic implications. Oncotarget 2017, 8, 18456–18485. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Liu, J.; Gao, C.; Liu, F.; Zhao, H. Increased mortality for colorectal cancer patients with preexisting diabetes mellitus: An updated meta-analysis. Oncotarget 2017, 8, 62478–62488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreiro, J.L.; Gomez-Hospital, J.A.; Angiolillo, D.J. Platelet abnormalities in diabetes mellitus. Diabetes Vasc. Dis. Res. 2010, 7, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Kraakman, M.J.; Lee, M.K.; Al-Sharea, A.; Dragoljevic, D.; Barrett, T.J.; Montenont, E.; Basu, D.; Heywood, S.; Kammoun, H.L.; Flynn, M.; et al. Neutrophil-derived S100 calcium-binding proteins A8/A9 promote reticulated thrombocytosis and atherogenesis in diabetes. J. Clin. Invest. 2017, 127, 2133–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S103–S123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santilli, F.; Pignatelli, P.; Violi, F.; Davi, G. Aspirin for primary prevention in diabetes mellitus: From the calculation of cardiovascular risk and risk/benefit profile to personalised treatment. Thromb. Haemost. 2015, 114, 876–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Group, A.S.C.; Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; et al. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus. N Engl. J. Med. 2018, 379, 1529–1539. [Google Scholar] [CrossRef]
- Bates, I. Reference Ranges and Normal Values. In Dacie and Lewis Practical Haematology, 12th ed.; Bain, B.J., Bates, I., Laffan, M.A., Eds.; Elsevier: London, UK, 2017; pp. 8–17. [Google Scholar] [CrossRef]
- Bain, B.J. Normal Ranges. In Blood Cells, 5th ed.; Bain, B.J., Ed.; Wiley-Blackwell: Oxford, UK, 2015; pp. 211–231. [Google Scholar] [CrossRef]
- Balduini, C.L.; Noris, P. Platelet count and aging. Haematologica 2014, 99, 953–955. [Google Scholar] [CrossRef] [Green Version]
- Biino, G.; Santimone, I.; Minelli, C.; Sorice, R.; Frongia, B.; Traglia, M.; Ulivi, S.; Di Castelnuovo, A.; Gogele, M.; Nutile, T.; et al. Age- and sex-related variations in platelet count in Italy: A proposal of reference ranges based on 40987 subjects’ data. PLoS ONE 2013, 8, e54289. [Google Scholar] [CrossRef] [Green Version]
- Yazbek, N.; Bapat, A.; Kleiman, N. Platelet abnormalities in diabetes mellitus. Coronary Artery Dis. 2003, 14, 365–371. [Google Scholar] [CrossRef]
- Plantureux, L.; Mege, D.; Crescence, L.; Dignat-George, F.; Dubois, C.; Panicot-Dubois, L. Impacts of Cancer on Platelet Production, Activation and Education and Mechanisms of Cancer-Associated Thrombosis. Cancers (Basel) 2018, 10, 441. [Google Scholar] [CrossRef] [Green Version]
- Voutsadakis, I.A. Thrombocytosis as a prognostic marker in gastrointestinal cancers. World J. Gastrointest. Oncol. 2014, 6, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.J.; Afshar-Kharghan, V.; Schafer, A.I. Paraneoplastic thrombocytosis: The secrets of tumor self-promotion. Blood 2014, 124, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-Y.; Zhang, X.; Qin, Y.-Y.; Qin, J.-Q.; Lin, F.-Q. Mean platelet volume/platelet count ratio in colorectal cancer: A retrospective clinical study. BMC Cancer 2019, 19, 314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, W.; Ge, X.X.; Wu, J.; Gong, F.R.; Wu, M.Y.; Xu, M.D.; Lian, L.; Wang, W.J.; Li, W.; Tao, M. Prognostic evaluation of resectable colorectal cancer using platelet-associated indicators. Oncol. Lett. 2019, 18, 571–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stojkovic Lalosevic, M.; Pavlovic Markovic, A.; Stankovic, S.; Stojkovic, M.; Dimitrijevic, I.; Radoman Vujacic, I.; Lalic, D.; Milovanovic, T.; Dumic, I.; Krivokapic, Z. Combined Diagnostic Efficacy of Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Mean Platelet Volume (MPV) as Biomarkers of Systemic Inflammation in the Diagnosis of Colorectal Cancer. Dis. Markers 2019, 2019, 6036979. [Google Scholar] [CrossRef] [PubMed]
- Herold, Z.; Ambrus, V.; Herold, M.; Herczeg, G.; Igaz, P.; Harsányi, L.; Somogyi, A. The occurrence and impact on survival of type 2 diabetes mellitus and thrombocytosis in colorectal cancer, before and after the surgical resection of the primary tumor. Orv. Hetil. 2018, 159, 756–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PDQ Adult Treatment Editorial Board. PDQ Colon Cancer Treatment. Bethesda, MD: National Cancer Institute. Available online: https://www.cancer.gov/types/colorectal/hp/colon-treatment-pdq (accessed on 17 December 2019).
- Recio-Boiles, A.; Waheed, A.; Cagir, B. Cancer, Colon. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Kannarkatt, J.; Joseph, J.; Kurniali, P.C.; Al-Janadi, A.; Hrinczenko, B. Adjuvant Chemotherapy for Stage II Colon Cancer: A Clinical Dilemma. J. Oncol. Pract. 2017, 13, 233–241. [Google Scholar] [CrossRef]
- Fotheringham, S.; Mozolowski, G.A.; Murray, E.M.A.; Kerr, D.J. Challenges and solutions in patient treatment strategies for stage II colon cancer. Gastroenterol. Rep. 2019, 7, 151–161. [Google Scholar] [CrossRef] [Green Version]
- Mamounas, E.; Wieand, S.; Wolmark, N.; Bear, H.D.; Atkins, J.N.; Song, K.; Jones, J.; Rockette, H. Comparative efficacy of adjuvant chemotherapy in patients with Dukes’ B versus Dukes’ C colon cancer: Results from four National Surgical Adjuvant Breast and Bowel Project adjuvant studies (C-01, C-02, C-03, and C-04). J. Clin. Oncol. 1999, 17, 1349–1355. [Google Scholar] [CrossRef]
- Quasar Collaborative, G.; Gray, R.; Barnwell, J.; McConkey, C.; Hills, R.K.; Williams, N.S.; Kerr, D.J. Adjuvant chemotherapy versus observation in patients with colorectal cancer: A randomised study. Lancet 2007, 370, 2020–2029. [Google Scholar] [CrossRef]
- Osterman, E.; Glimelius, B. Recurrence Risk After Up-to-Date Colon Cancer Staging, Surgery, and Pathology: Analysis of the Entire Swedish Population. Dis. Colon Rectum. 2018, 61, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Moy, B.; Jacobson, B.C. Surveillance after Colorectal Cancer Resection. Available online: https://www.uptodate.com/contents/surveillance-after-colorectal-cancer-resection (accessed on 18 December 2019).
- Burz, C.; Aziz, B.Y.; Balacescu, L.; Lelutiu, L.; Buiga, R.; Samasca, G.; Irimie, A.; Lisencu, C. Tumor markers used in monitoring the tumor recurrence in patients with colorectal cancer. Clujul. Med. 2016, 89, 378–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramphal, W.; Boeding, J.R.E.; van Iwaarden, M.; Schreinemakers, J.M.J.; Rutten, H.J.T.; Crolla, R.; Gobardhan, P.D. Serum carcinoembryonic antigen to predict recurrence in the follow-up of patients with colorectal cancer. Int. J. Biol. Markers 2019, 34, 60–68. [Google Scholar] [CrossRef]
- Issa, I.A.; Noureddine, M. Colorectal cancer screening: An updated review of the available options. World J. Gastroenterol. 2017, 23, 5086–5096. [Google Scholar] [CrossRef] [PubMed]
- Basu, P.; Ponti, A.; Anttila, A.; Ronco, G.; Senore, C.; Vale, D.B.; Segnan, N.; Tomatis, M.; Soerjomataram, I.; Primic Zakelj, M.; et al. Status of implementation and organization of cancer screening in The European Union Member States-Summary results from the second European screening report. Int. J. Cancer 2018, 142, 44–56. [Google Scholar] [CrossRef]
- Koo, S.; Neilson, L.J.; Von Wagner, C.; Rees, C.J. The NHS Bowel Cancer Screening Program: Current perspectives on strategies for improvement. Risk Manag. Healthc. Policy 2017, 10, 177–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirst, Y.; Stoffel, S.; Baio, G.; McGregor, L.; von Wagner, C. Uptake of the English Bowel (Colorectal) Cancer Screening Programme: An update 5 years after the full roll-out. Eur. J. Cancer 2018, 103, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Logan, R.F.; Patnick, J.; Nickerson, C.; Coleman, L.; Rutter, M.D.; von Wagner, C. Outcomes of the Bowel Cancer Screening Programme (BCSP) in England after the first 1 million tests. Gut 2012, 61, 1439–1446. [Google Scholar] [CrossRef]
- Hobbs, F.D. ABC of colorectal cancer: The role of primary care. BMJ 2000, 321, 1068–1070. [Google Scholar] [CrossRef]
- Bertels, L.; van der Heijden, S.; Hoogsteyns, M.; Dekker, E.; van Asselt, K.; van Weert, H.; Knottnerus, B. GPs’ perspectives on colorectal cancer screening and their potential influence on FIT-positive patients: An exploratory qualitative study from a Dutch context. BJGP Open 2019, 3, bjgpopen18X101631. [Google Scholar] [CrossRef]
- Dawson, G.; Crane, M.; Lyons, C.; Burnham, A.; Bowman, T.; Perez, D.; Travaglia, J. General practitioners’ perceptions of population based bowel screening and their influence on practice: A qualitative study. BMC Fam. Pract. 2017, 18, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, T.; Atkin, K.; Macleod, U. Cancer detection in primary care: Insights from general practitioners. Br. J. Cancer 2015, 112 (Suppl. S1), S41–S49. [Google Scholar] [CrossRef] [PubMed]
- Hogberg, C.; Samuelsson, E.; Lilja, M.; Fharm, E. Could it be colorectal cancer? General practitioners’ use of the faecal occult blood test and decision making—A qualitative study. BMC Fam. Pract. 2015, 16, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hippisley-Cox, J.; Coupland, C. Development and validation of risk prediction equations to estimate survival in patients with colorectal cancer: Cohort study. BMJ 2017, 357, j2497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajkumar, A.; Szallasi, A. Paraneoplastic thrombocytosis in breast cancer. Anticancer Res. 2013, 33, 4545–4546. [Google Scholar] [PubMed]
- Hisabe, T.; Hirai, F.; Matsui, T. Development and progression of colorectal cancer based on follow-up analysis. Dig. Endosc. 2014, 26 (Suppl. S2), 73–77. [Google Scholar] [CrossRef] [PubMed]
- Simon, K. Colorectal cancer development and advances in screening. Clin. Interv. Aging 2016, 11, 967–976. [Google Scholar] [CrossRef] [Green Version]
- Kundrapu, S.; Noguez, J. Laboratory Assessment of Anemia. Adv. Clin. Chem. 2018, 83, 197–225. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Hothorn, T.; Bretz, F.; Westfall, P. Simultaneous inference in general parametric models. Biom. J. 2008, 50, 346–363. [Google Scholar] [CrossRef] [Green Version]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Muller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- Pinheiro, J.; Bates, D.; DebRoy, S.; Sarkar, D.; R Core Team. {nlme}: Linear and Nonlinear Mixed Effects Models. version 3.1–142. 2019. Available online: https://cran.r-project.org/web/packages/nlme/index.html (accessed on 7 November 2019).
- Therneau, T.M. A Package for Survival Analysis in R. version 3.1-8. 2019. Available online: https://cran.r-project.org/web/packages/survival/index.html (accessed on 3 December 2019).
- De Wreede, L.C.; Fiocco, M.; Putter, H. mstate: An R Package for the Analysis of Competing Risks and Multi-State Models. J. Stat. Softw. 2011, 38, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Gordon, M.; Lumley, T. Forestplot: Advanced Forest Plot Using ‘grid’ Graphics. R Package Version 1.9. 2019. Available online: https://cran.r-project.org/web/packages/forestplot/index.html (accessed on 24 June 2019).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Cohort 1 (Control) (N = 50) | Cohort 2 (T2DM) (N = 50) | Cohort 3 (CRC) (N = 102) | Cohort 4 (CRC + T2DM) (N = 48) |
|---|---|---|---|---|
| Age [years] | 60.84 ± 12.29 A | 67.52 ± 9.48 | 68.13 ± 9.89 | 70.28 ± 7.33 |
| Duration of T2DM [years] | NA | 16.78 ± 8.63 | NA | 11.88 ± 7.52 1,B |
| White blood cell count [109/L] | 6.97 ± 1.91 | 7.73 ± 2.03 | 8.22 ± 3.21 | 9.19 ± 5.45 C |
| Red blood cell count [1012/L] | 4.80 ± 0.59 | 4.76 ± 1.59 | 4.50 ± 0.57 D | 4.28 ± 0.63 E |
| Platelet count [109/L] | 261.71 ± 64.11 | 248.78 ± 61.97 | 334.33 ± 132.21 E | 343.17 ± 124.39 E |
| Hemoglobin [g/L] | 144.20 ± 13.83 | 138.88 ± 10.76 | 123.68 ± 23.11 E | 113.40 ± 25.44 E,F |
| Hematocrit [L/L] | 0.43 ± 0.04 | 0.42 ± 0.03 | 0.38 ± 0.06 E | 0.35 ± 0.06 E,F |
| Mean corpuscular volume [fL] | 89.67 ± 5.18 | 88.43 ± 3.74 | 84.23 ± 7.09 E | 82.25 ± 8.08 E |
| Mean corpuscular hemoglobin [pg] | 30.18 ± 2.05 | 29.35 ± 1.58 | 27.43 ± 3.39 E | 26.43 ± 4.18 E |
| Mean corpuscular hemoglobin concentration [g/L] | 336.42 ± 9.24 | 325.78 ± 45.06 | 324.90 ± 19.54 | 319.75 ± 25.32 C |
| Red blood cell distribution width [%] | 13.24 ± 0.86 | 13.31 ± 0.90 2 | 14.82 ± 2.92 3,E | 15.60 ± 2.79 2,E |
| Mean survival time [months] | NA | NA | 31.15 ± 22.53 | 34.63 ± 25.60 |
| CRC related death | NA | NA | 41 (40.2%) | 16 (33.3%) |
| Sex (Female/Male) | 25/25 (50.0%/50.0%) | 25/25 (50.0%/50.0%) | 49/53 (48.0%/52.0%) | 16/32 (33.3%/66.7%) |
| Hypertension | 26 (52.0%) | 45 (90.0%) G | 76 (74.1%) H | 46 (90.0%) F,G |
| Previous major cardiovascular event | 7 (14.0%) | 14 (28.0%) | 22 (21.6%) | 21 (43.8%) C,F |
| Thyroid diseases | 4 (8.0%) | 9 (18.0%) | 16 (15.7%) | 8 (16.7%) |
| Previous cholelithiasis | 3 (6.0%) A | 16 (32.0%) | 29 (28.4%) | 19 (39.6%) |
| Previous appendicitis | 5 (10.0%) | 8 (16.0%) | 22 (21.6%) | 10 (20.8%) |
| Antiplatelet therapy | 12 (24.0%) | 42 (84.0%) I | 24 (23.5%) | 24 (50.0%) D,F |
| Chemotherapy | ||||
| NA | NA | 38 (37.3%) | 23 (47.9%) |
| NA | NA | 6 (5.9%) | 1 (2.1%) |
| NA | NA | 55 (53.9%) | 21 (43.8%) |
| NA | NA | 3 (2.9%) | 3 (6.3%) |
| Variables | Cohort 1 (Control) (N = 50) | Cohort 2 (T2DM) (N = 50) | Cohort 3 (CRC) (N = 102) | Cohort 4 (CRC + T2DM) (N = 48) |
|---|---|---|---|---|
| Age [years] | 50.86 ± 12.20 A | 60.06 ± 9.35 | 61.45 ± 9.73 | 62.94 ± 9.51 |
| Time between blood collections [months] | 119.79 ± 29.17 | 89.53 ± 32.86 | 81.59 ± 32.86 | 88.11 ± 71.28 |
| White blood cell count [109/L] | 7.30 ± 2.35 | 7.97 ± 2.21 | 7.73 ± 2.69 | 8.12 ± 2.70 |
| Red blood cell count [1012/L] | 4.80 ± 0.41 | 4.77 ± 0.42 | 4.69 ± 0.53 | 4.69 ± 0.46 |
| Platelet count [109/L] | 270.82 ± 61.45 | 255.76 ± 57.75 | 251.06 ± 58.84 | 250.25 ± 58.89 |
| Hemoglobin [g/L] | 142.56 ± 12.29 | 140.60 ± 11.00 | 140.93 ± 15.89 | 140.81 ± 16.45 |
| Hematocrit [L/L] | 0.42 ± 0.03 | 0.41 ± 0.03 | 0.42 ± 0.05 | 0.42 ± 0.04 |
| Mean corpuscular volume [fL] | 87.17 ± 4.30 | 86.51 ± 3.93 | 88.80 ± 6.36 | 89.54 ± 4.64 |
| Mean corpuscular hemoglobin [pg] | 29.77 ± 1.75 | 29.55 ± 1.56 | 30.13 ± 2.07 | 30.01 ± 2.23 |
| Mean corpuscular hemoglobin concentration [g/L] | 341.60 ± 12.49 | 341.58 ± 12.45 | 338.65 ± 13.84 | 335.19 ± 21.39 |
| Red blood cell distribution width [%] | 13.29 ± 0.81 1 | 13.47 ± 0.70 | 13.33 ± 1.02 2 | 13.67 ± 1.01 3 |
| Variables | Control Subjects (N = 100) | Colorectal Cancer Patients (N = 150) |
|---|---|---|
| Platelet | −0.41% (−0.52%)–(−0.33%) p = 0.0011 | 2.18% 1.80–2.59% p < 0.0001 |
| −0.10% (−0.52%)–(−0.32%) p = 0.0033 | 3.77% 2.99–4.58% p < 0.0001 | |
| −0.67% (−0.85%)–(−0.53%) p = 0.0033 | 3.42% 2.72–4.16% p < 0.0001 | |
| −0.40% (−0.51%)–(−0.32%) p = 0.0046 | 2.89% 2.26–3.58% p < 0.0001 | |
| −0.68% (−0.86%)–(−0.54%) p < 0.0001 | 2.70% 2.23–3.17% p < 0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herold, Z.; Herold, M.; Lohinszky, J.; Dank, M.; Somogyi, A. Personalized Indicator Thrombocytosis Shows Connection to Staging and Indicates Shorter Survival in Colorectal Cancer Patients with or without Type 2 Diabetes. Cancers 2020, 12, 556. https://doi.org/10.3390/cancers12030556
Herold Z, Herold M, Lohinszky J, Dank M, Somogyi A. Personalized Indicator Thrombocytosis Shows Connection to Staging and Indicates Shorter Survival in Colorectal Cancer Patients with or without Type 2 Diabetes. Cancers. 2020; 12(3):556. https://doi.org/10.3390/cancers12030556
Chicago/Turabian StyleHerold, Zoltan, Magdolna Herold, Julia Lohinszky, Magdolna Dank, and Aniko Somogyi. 2020. "Personalized Indicator Thrombocytosis Shows Connection to Staging and Indicates Shorter Survival in Colorectal Cancer Patients with or without Type 2 Diabetes" Cancers 12, no. 3: 556. https://doi.org/10.3390/cancers12030556