The Impact of Normalization Approaches to Automatically Detect Radiogenomic Phenotypes Characterizing Breast Cancer Receptors Status


Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
2.1.1. Clinical Data
2.1.2. Image Data
2.1.3. Radiomic Features
2.1.4. miRNA expression data
2.2. Statistical Methods
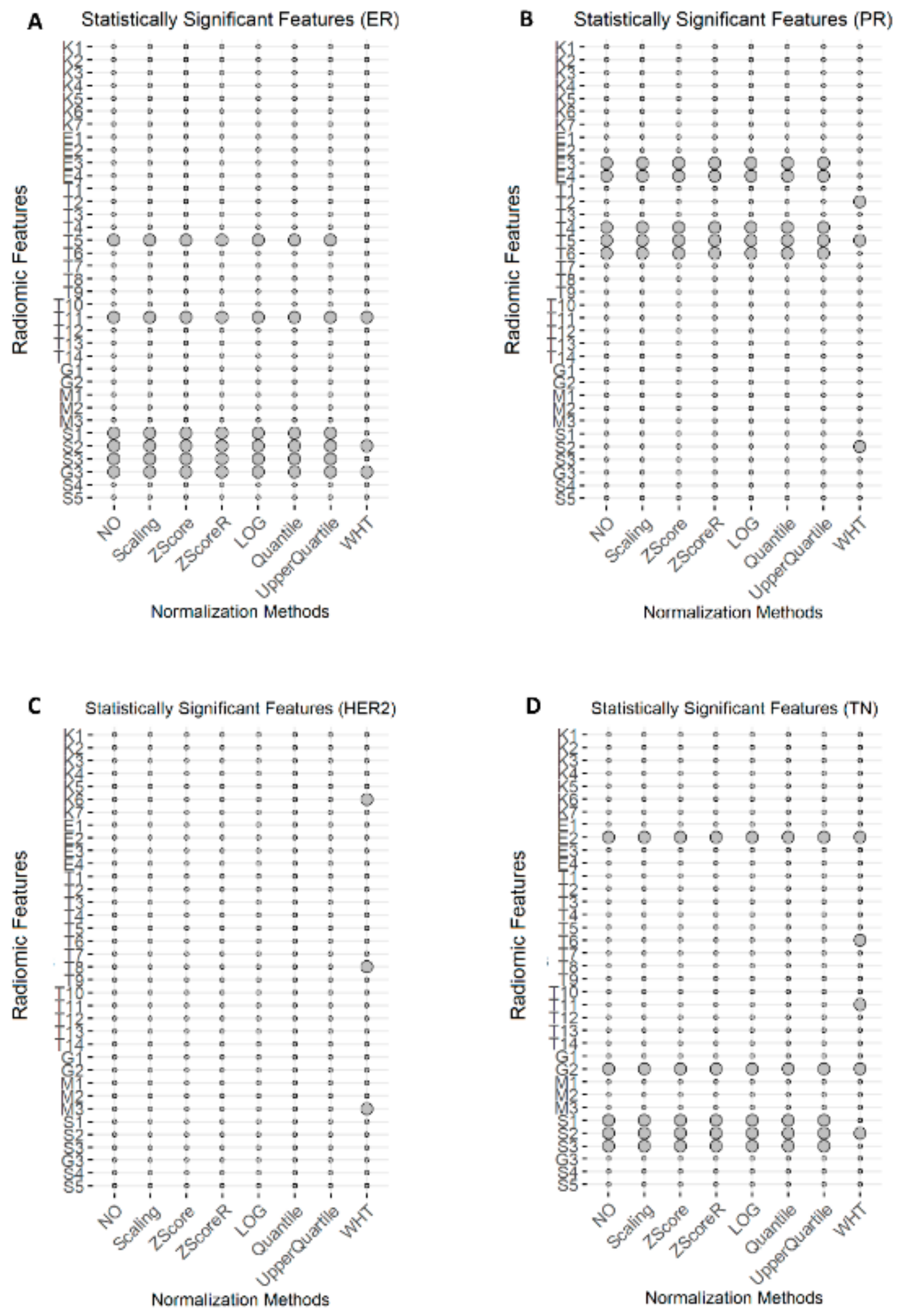
2.2.1. Radiomic Statistical Analysis
- Two arrows, ↓↓ (or ↑↑) were used to report a significant (p-value < 0.05) decrease (or increase) of radiomic feature median in negative receptor status (ER–, PR–, HER2 +, TN);
- One arrow was used for non-significant variations: ↓ (or ↑) indicated a non-significant (p-value > 0.05) decrease (or increase) of a radiomic feature median in negative receptor status (ER–, PR–, HER2+, TN).
2.2.2. Genomic Statistical Analysis
2.2.3. Radiogenomic Statistical Analysis
2.3. Machine Learning Classification
2.3.1. Feature Selection Methods
2.3.2. Training, Validation, and Testing
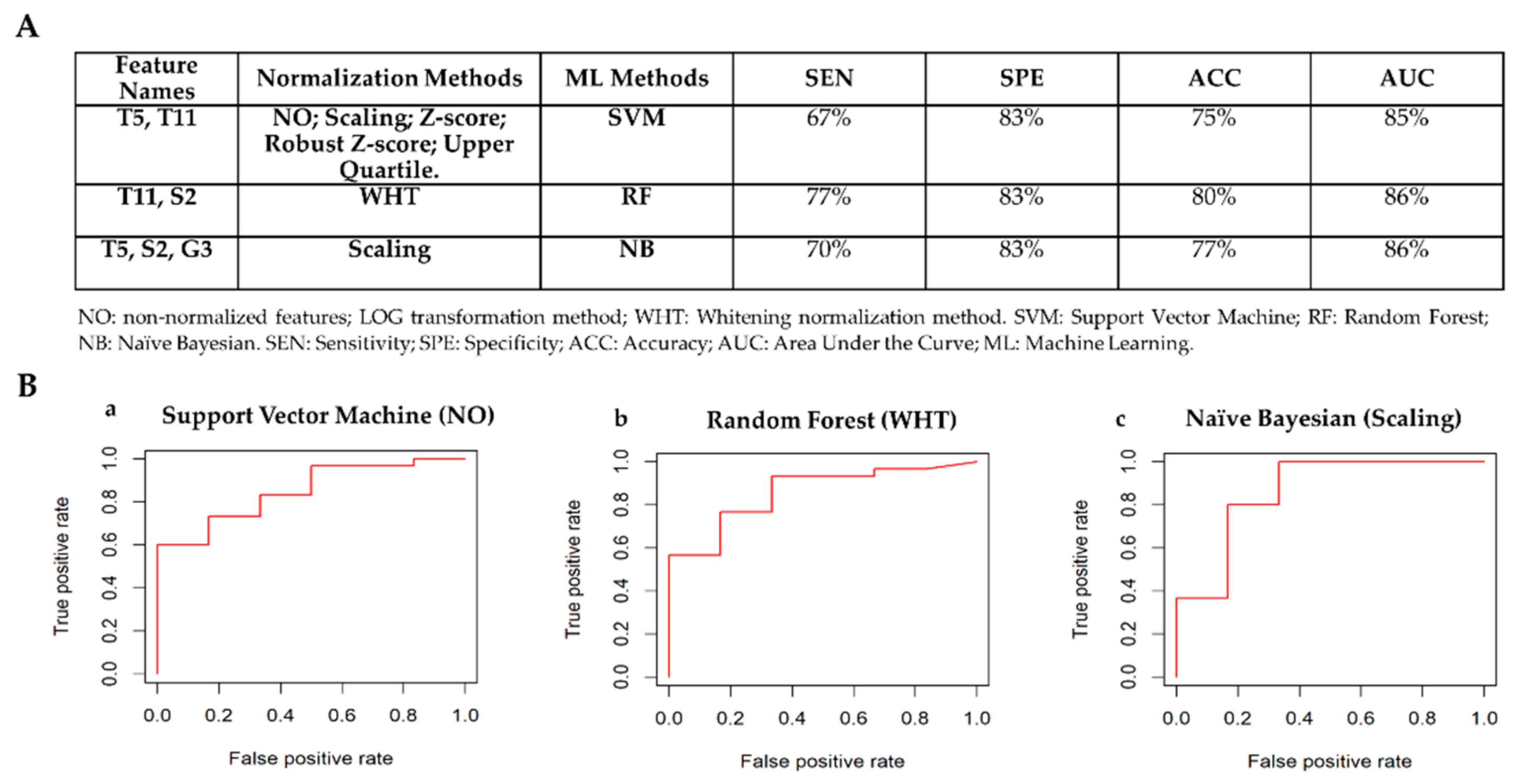
2.3.3. Best Model Selection
3. Results
3.1. Radiomics
3.1.1. Statistical Analysis per Receptor Status: ER+ vs ER–
3.1.2. Statistical Analysis per Receptor Status: PR+ vs PR–
3.1.3. Statistical Analysis per Receptor Status: HER2+ vs HER2–
3.1.4. Statistical Analysis per Receptor Status: TN vs Others
3.2. Genomics
3.3. Radiogenomics
3.3.1. Correlation Analysis per Receptor Status: ER+ vs ER–
3.3.2. Correlation Analysis per Receptor Status: PR+ vs PR–
3.3.3. Correlation Analysis per Receptor Status: HER2+ vs HER2–
3.3.4. Correlation Analysis per Receptor Status: TN vs Others
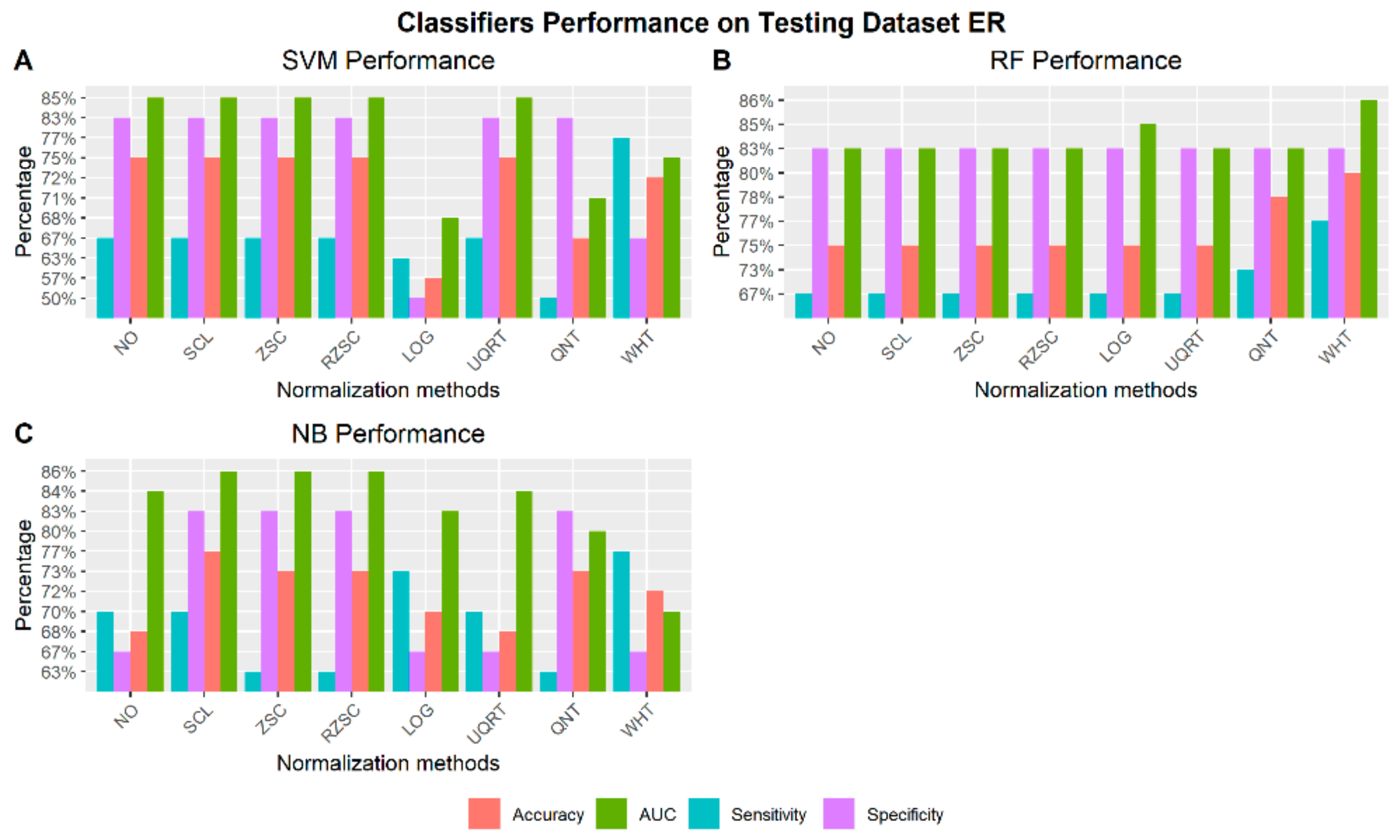
3.4. Machine Learning Per Molecular Classification
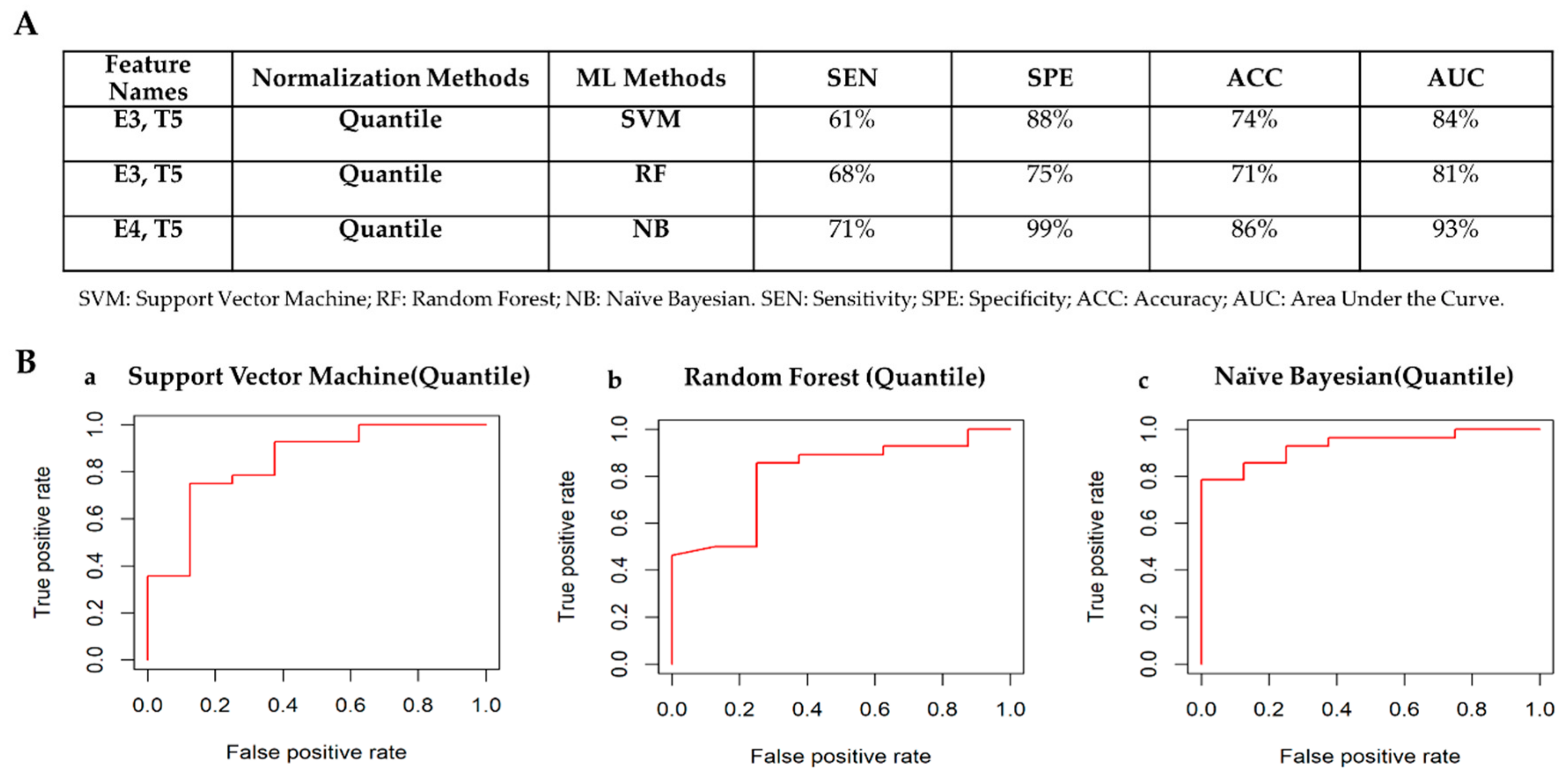
3.4.1. Receptor Status: ER– vs ER+
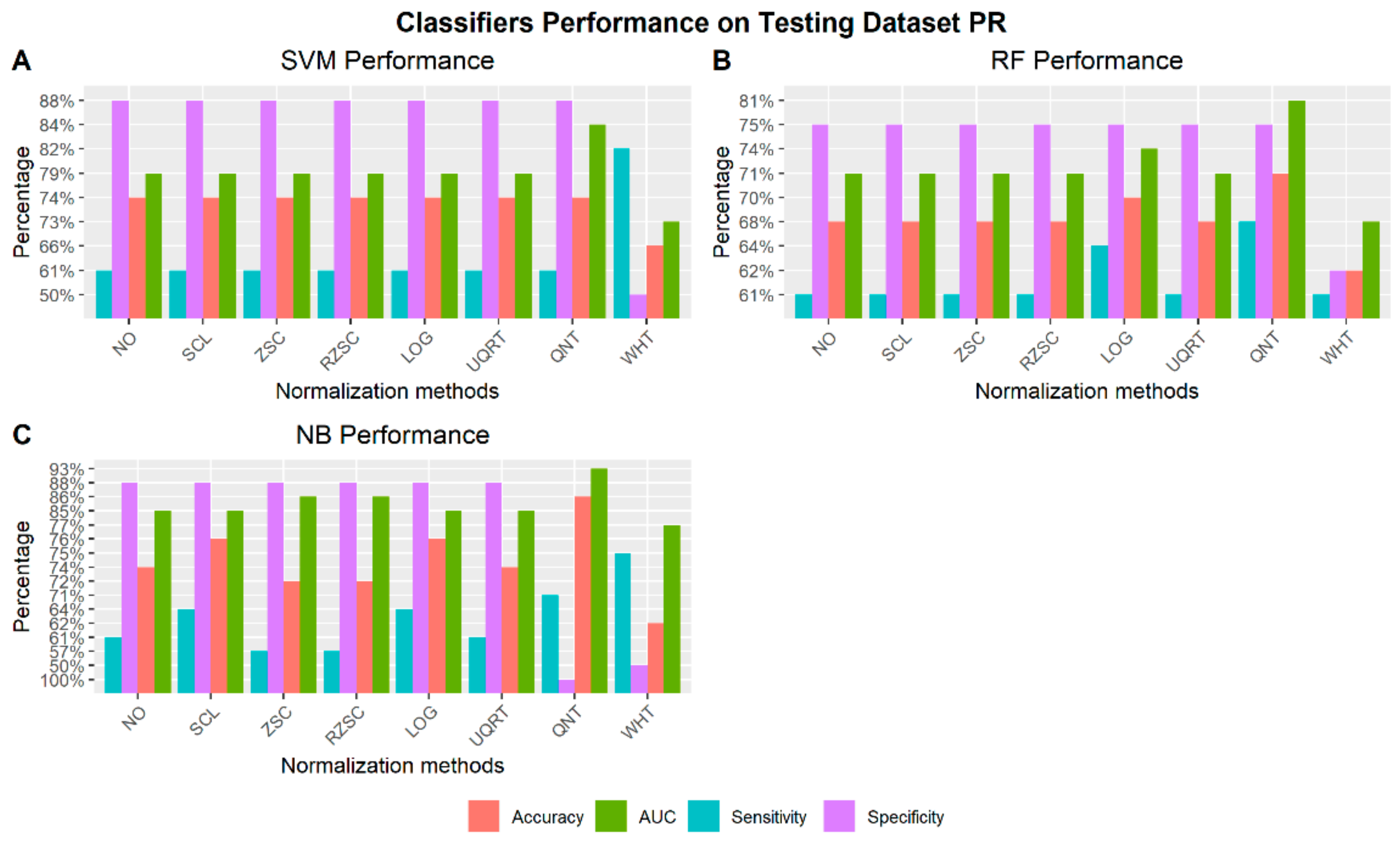
3.4.2. Receptor Status: PR– vs PR+
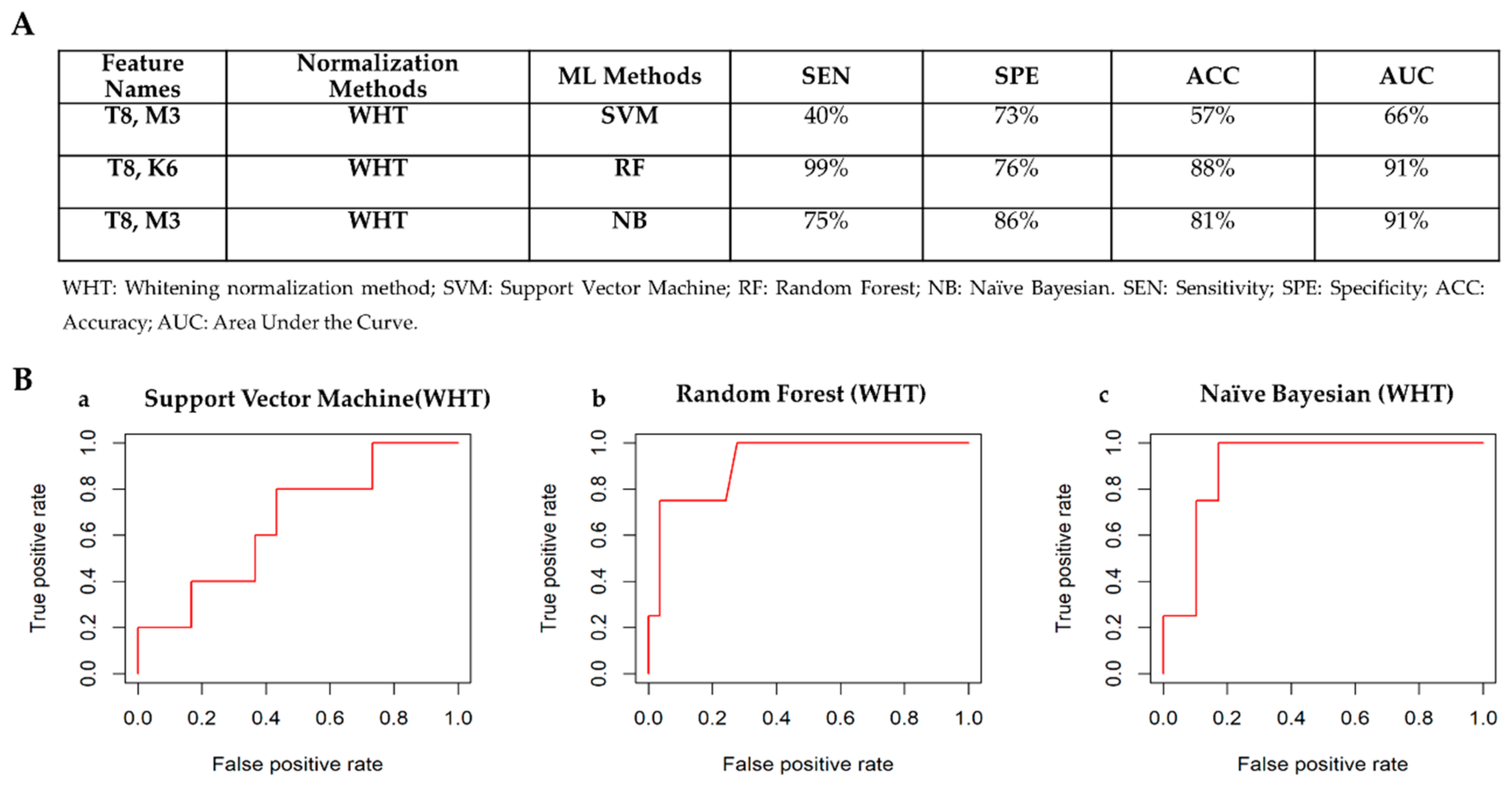
3.4.3. Receptor Status: HER2– vs HER2+
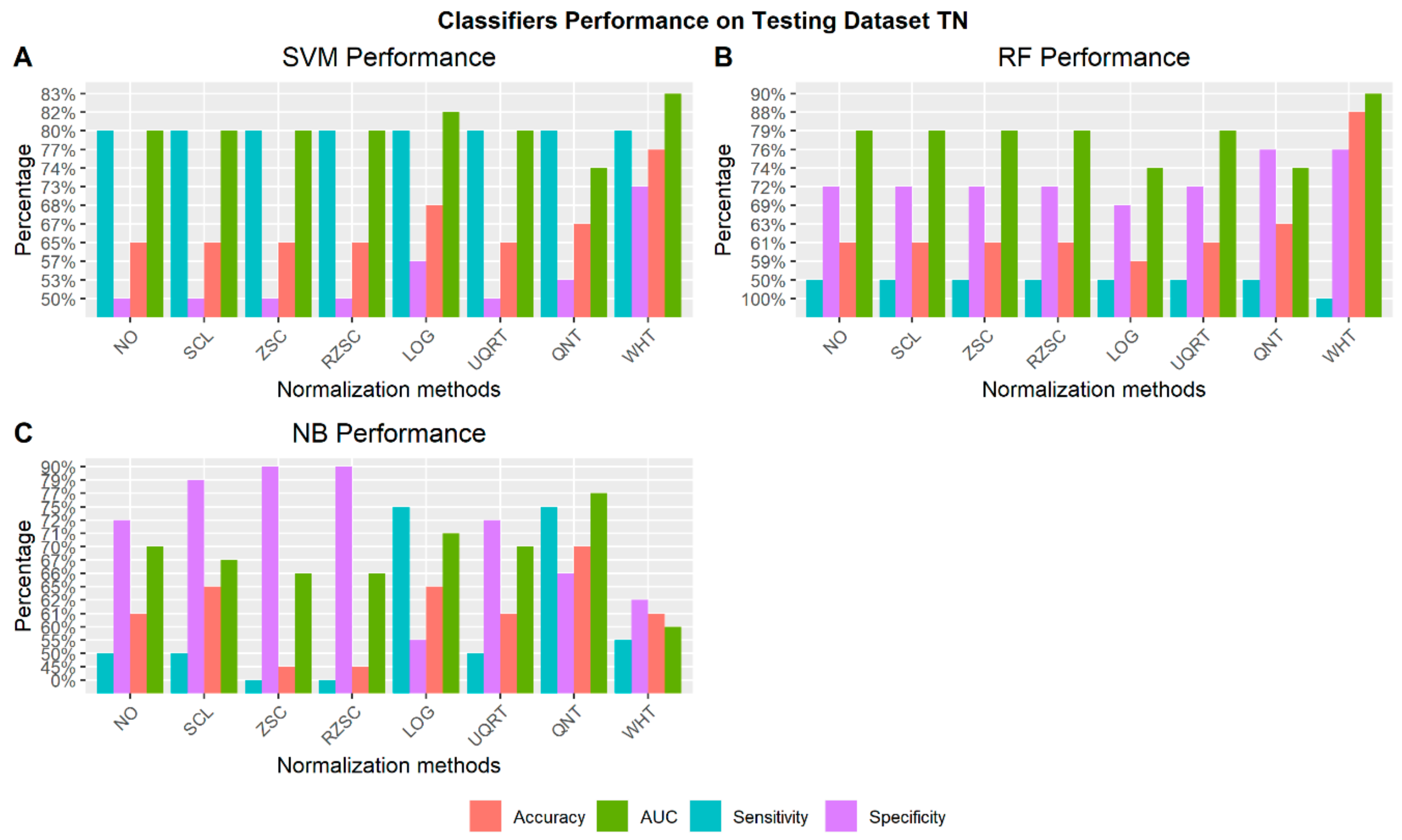
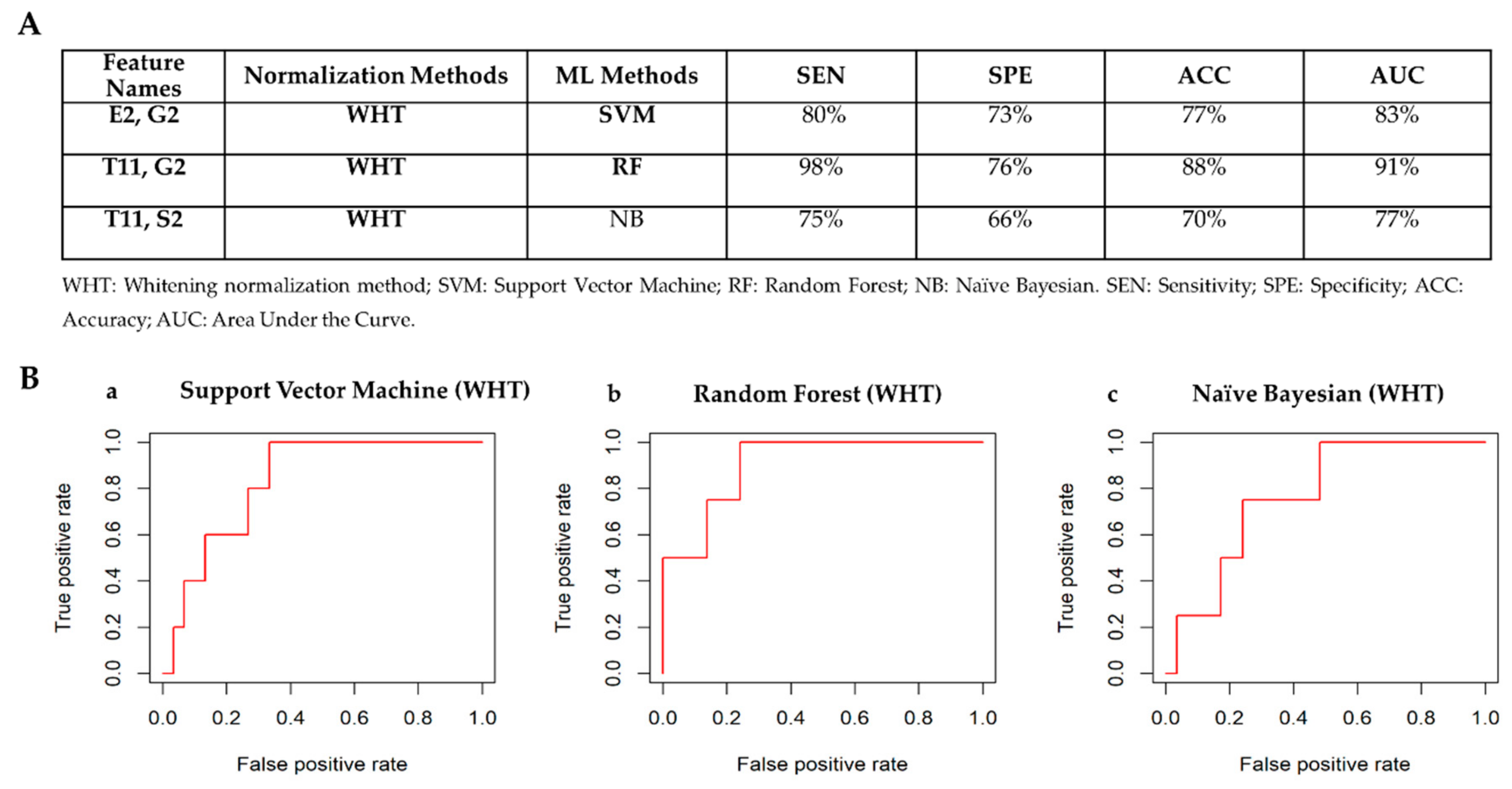
3.4.4. Receptor Status: TN vs Others
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics, 2014. CA Cancer J. Clin. 2014, 64, 9–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiordelisi, M.; Auletta, L.; Meomartino, L.; Basso, L.; Fatone, G.; Salvatore, M.; Mancini, M.; Greco, A. Preclinical Molecular Imaging for Precision Medicine in Breast Cancer Mouse Models. Contrast Media Mol. Imaging 2019, 2019, 8946729. [Google Scholar] [CrossRef] [PubMed]
- Carey, L.A.; Perou, C.M.; Livasy, C.A.; Dressler, L.G.; Cowan, D.; Conway, K.; Karaca, G.; Troester, M.A.; Tse, C.K.; Edmiston, S. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA 2006, 295(21), 2492–2502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voduc, K.D.; Cheang, M.C.; Tyldesley, S.; Gelmon, K.; Nielsen, T.O.; Kennecke, H. Breast cancer subtypes and the risk of local and regional relapse. J. Clin. Oncol. 2010, 28(10), 1684–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metzger-Filho, O.; Sun, Z.; Viale, G.; Price, K.N.; Crivellari, D.; Snyder, R.D.; Gelber, R.D.; Castiglione-Gertsch, M.; Coates, A.S.; Goldhirsch, A. Patterns of recurrence and outcome according to breast cancer subtypes in lymph node–negative disease: Results from International Breast Cancer Study Group Trials VIII and IX. J. Clin. Oncol. 2013, 31(25), 3083. [Google Scholar] [CrossRef] [Green Version]
- Arvold, N.D.; Taghian, A.G.; Niemierko, A.; Raad, R.F.A.; Sreedhara, M.; Nguyen, P.L.; Bellon, J.R.; Wong, J.S.; Smith, B.L.; Harris, J.R. Age, breast cancer subtype approximation, and local recurrence after breast-conserving therapy. J. Clin. Oncol. 2011, 29(29), 3885. [Google Scholar] [CrossRef]
- Li, H.; Zhu, Y.; Burnside, E.S.; Huang, E.; Drukker, K.; Hoadley, K.A.; Fan, C.; Conzen, S.D.; Zuley, M.; Net, J.M. Quantitative MRI radiomics in the prediction of molecular classifications of breast cancer subtypes in the TCGA/TCIA data set. NPJ Breast Cancer 2016, 2, 16012. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Wood, W.C.; Coates, A.S.; Gelber, R.D.; Thürlimann, B.; Senn, H.-J.; Members, P. Strategies for subtypes—dealing with the diversity of breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Ann. Oncol. 2011, 22(8), 1736–1747. [Google Scholar] [CrossRef]
- Gnant, M.; Harbeck, N.; Thomssen, C. St. Gallen/Vienna 2017: A brief summary of the consensus discussion about escalation and de-escalation of primary breast cancer treatment. Breast Care 2017, 12(2), 101–106. [Google Scholar] [CrossRef] [Green Version]
- Aerts, H.J. The potential of radiomic-based phenotyping in precision medicine: A review. JAMA Oncol. 2016, 2(12), 1636–1642. [Google Scholar] [CrossRef]
- Wu, J.; Tha, K.K.; Xing, L.; Li, R. Radiomics and radiogenomics for precision radiotherapy. In J. Radiat. Res.; 2018; Volume 59, (Suppl_1), pp. i25–i31. [Google Scholar]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2015, 278(2), 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Li, B.; Sun, X.; Cao, G.; Rubin, D.L.; Napel, S.; Ikeda, D.M.; Kurian, A.W.; Li, R. Heterogeneous enhancement patterns of tumor-adjacent parenchyma at MR imaging are associated with dysregulated signaling pathways and poor survival in breast cancer. Radiology 2017, 285(2), 401–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazurowski, M.A. Radiogenomics: What it is and why it is important. J. Am. Coll. Radiol. 2015, 12(8), 862–866. [Google Scholar] [CrossRef] [PubMed]
- Network, C.G.A. Comprehensive molecular portraits of human breast tumours. Nature 2012, 490(7418), 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M. The Cancer Imaging Archive (TCIA): Maintaining and operating a public information repository. J. Digit. Imag. 2013, 26(6), 1045–1057. [Google Scholar] [CrossRef] [Green Version]
- Zanfardino, M.; Pane, K.; Mirabelli, P.; Salvatore, M.; Franzese, M. TCGA-TCIA Impact on Radiogenomics Cancer Research: A Systematic Review. Intl. J. Mol. Sci. 2019, 20(23), 6033. [Google Scholar] [CrossRef] [Green Version]
- Zanfardino, M.; Franzese, M.; Pane, K.; Cavaliere, C.; Monti, S.; Esposito, G.; Salvatore, M.; Aiello, M. Bringing radiomics into a multi-omics framework for a comprehensive genotype–phenotype characterization of oncological diseases. J. Translat. Med. 2019, 17(1), 337. [Google Scholar] [CrossRef]
- Schiano, C.; Franzese, M.; Pane, K.; Garbino, N.; Soricelli, A.; Salvatore, M.; de Nigris, F.; Napoli, C. Hybrid 18F-FDG-PET/MRI Measurement of Standardized Uptake Value Coupled with Yin Yang 1 Signature in Metastatic Breast Cancer. A Preliminary Study. Cancers 2019, 11(10), 1444. [Google Scholar] [CrossRef] [Green Version]
- Bhooshan, N.; Giger, M.L.; Jansen, S.A.; Li, H.; Lan, L.; Newstead, G.M. Cancerous breast lesions on dynamic contrast-enhanced MR images: Computerized characterization for image-based prognostic markers. Radiology 2010, 254(3), 680–690. [Google Scholar] [CrossRef]
- Guo, W.; Li, H.; Zhu, Y.; Lan, L.; Yang, S.; Drukker, K.; Morris, E.A.; Burnside, E.S.; Whitman, G.J.; Giger, M.L. Prediction of clinical phenotypes in invasive breast carcinomas from the integration of radiomics and genomics data. J. Med. Imag. 2015, 2(4), 041007. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, H.; Guo, W.; Drukker, K.; Lan, L.; Giger, M.L.; Ji, Y. Deciphering genomic underpinnings of quantitative MRI-based radiomic phenotypes of invasive breast carcinoma. Sci. Rep. 2015, 5, 17787. [Google Scholar] [CrossRef] [PubMed]
- Giger, M.L.; Karssemeijer, N.; Schnabel, J.A. Breast image analysis for risk assessment, detection, diagnosis, and treatment of cancer. Annu. Rev. Biomed. Eng. 2013, 15, 327–357. [Google Scholar] [CrossRef] [PubMed]
- Bhooshan, N.; Giger, M.; Edwards, D.; Yuan, Y.; Jansen, S.; Li, H.; Lan, L.; Sattar, H.; Newstead, G. Computerized three-class classification of MRI-based prognostic markers for breast cancer. Phys. Med. Biol. 2011, 56(18), 5995. [Google Scholar]
- Grimm, L.J.; Zhang, J.; Mazurowski, M.A. Computational approach to radiogenomics of breast cancer: Luminal A and luminal B molecular subtypes are associated with imaging features on routine breast MRI extracted using computer vision algorithms. J. Magnet. Resonance Imag. 2015, 42(4), 902–907. [Google Scholar] [CrossRef]
- Wu, J.; Cui, Y.; Sun, X.; Cao, G.; Li, B.; Ikeda, D.M.; Kurian, A.W.; Li, R. Unsupervised clustering of quantitative image phenotypes reveals breast cancer subtypes with distinct prognoses and molecular pathways. Clin. Cancer Res. 2017, 23(13), 3334–3342. [Google Scholar] [CrossRef] [Green Version]
- Burnside, E.S.; Drukker, K.; Li, H.; Bonaccio, E.; Zuley, M.; Ganott, M.; Net, J.M.; Sutton, E.J.; Brandt, K.R.; Whitman, G.J. Using computer-extracted image phenotypes from tumors on breast magnetic resonance imaging to predict breast cancer pathologic stage. Cancer 2016, 122(5), 748–757. [Google Scholar] [CrossRef]
- Agner, S.C.; Rosen, M.A.; Englander, S.; Tomaszewski, J.E.; Feldman, M.D.; Zhang, P.; Mies, C.; Schnall, M.D.; Madabhushi, A. Computerized image analysis for identifying triple-negative breast cancers and differentiating them from other molecular subtypes of breast cancer on dynamic contrast-enhanced MR images: A feasibility study. Radiology 2014, 272(1), 91–99. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, K.; Abe, H.; Newstead, G.M.; Egashira, R.; Nakazono, T.; Imaizumi, T.; Irie, H. Intratumoral heterogeneity of the distribution of kinetic parameters in breast cancer: Comparison based on the molecular subtypes of invasive breast cancer. Breast Cancer 2015, 22(5), 496–502. [Google Scholar] [CrossRef]
- Fiordelisi, M.F.; Cavaliere, C.; Auletta, L.; Basso, L.; Salvatore, M. Magnetic Resonance Imaging for Translational Research in Oncology. J. Clin. Med. 2019, 8(11), 1883. [Google Scholar] [CrossRef] [Green Version]
- Blaschke, E.; Abe, H. MRI phenotype of breast cancer: Kinetic assessment for molecular subtypes. J. Magnet. Resonance Imag. 2015, 42(4), 920–924. [Google Scholar] [CrossRef]
- Xie, T.; Wang, Z.; Zhao, Q.; Bai, Q.; Zhou, X.; Gu, Y.; Peng, W.; Wang, H. Machine Learning-based Analysis of MR Multiparametric Radiomics for the Subtype Classification of Breast Cancer. Fron. Oncol. 2019, 9, 505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, H.-J.; Ramanathan, A.; Alamudun, F.; Tourassi, G. Deep radiogenomics for predicting clinical phenotypes in invasive breast cancer. In In Proceedings of the 14th International Workshop on Breast Imaging (IWBI 2018), Atlanta, GA, USA, 8–11 July 2018; International Society for Optics and Photonics: Bellingham, WA, USA, 2018; p. 107181H. [Google Scholar]
- Parmar, C.; Barry, J.D.; Hosny, A.; Quackenbush, J.; Aerts, H. Data Analysis Strategies in Medical Imaging. Clin. Cancer Res. 2018, 24(15), 3492–3499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotsiantis, S.; Kanellopoulos, D.; Pintelas, P. Data preprocessing for supervised leaning. Intl. J. Comput. Sci. 2006, 1(2), 111–117. [Google Scholar]
- Rizzo, S.; Botta, F.; Raimondi, S.; Origgi, D.; Fanciullo, C.; Morganti, A.G.; Bellomi, M. Radiomics: The facts and the challenges of image analysis. Eur. Radiol. Exp. 2018, 2(1), 1–8. [Google Scholar] [CrossRef]
- Madabhushi, A.; Udupa, J.K. New methods of MR image intensity standardization via generalized scale. Med. Phys. 2006, 33(9), 3426–3434. [Google Scholar] [CrossRef]
- Nyúl, L.G.; Udupa, J.K. On standardizing the MR image intensity scale. Magnet. Resonance Med. 1999, 42(6), 1072–1081. [Google Scholar]
- Nyúl, L.G.; Udupa, J.K.; Zhang, X. New variants of a method of MRI scale standardization. IEEE Trans. Med. Imag. 2000, 19(2), 143–150. [Google Scholar] [CrossRef]
- Ge, Y.; Udupa, J.K.; Nyul, L.G.; Wei, L.; Grossman, R.I. Numerical tissue characterization in MS via standardization of the MR image intensity scale. J. Magnet. Resonance Imag. 2000, 12(5), 715–721. [Google Scholar] [CrossRef]
- Li, H.; Zhu, Y.; Burnside, E.S.; Drukker, K.; Hoadley, K.A.; Fan, C.; Conzen, S.D.; Whitman, G.J.; Sutton, E.J.; Net, J.M. MR imaging radiomics signatures for predicting the risk of breast cancer recurrence as given by research versions of MammaPrint, Oncotype DX, and PAM50 gene assays. Radiology 2016, 281(2), 382–391. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2012. Available online: http://www.R-project.org (accessed on 2 January 2020).
- Colaprico, A.; Silva, T.C.; Olsen, C.; Garofano, L.; Cava, C.; Garolini, D.; Sabedot, T.S.; Malta, T.M.; Pagnotta, S.M.; Castiglioni, I. TCGAbiolinks: An R/Bioconductor package for integrative analysis of TCGA data. Nucl. Acids Res. 2015, 44(8), e71. [Google Scholar] [CrossRef]
- Incoronato, M.; Grimaldi, A.M.; Mirabelli, P.; Cavaliere, C.; Parente, C.A.; Franzese, M.; Staibano, S.; Ilardi, G.; Russo, D.; Soricelli, A. Circulating miRNAs in Untreated Breast Cancer: An Exploratory Multimodality Morpho-Functional Study. Cancers 2019, 11(6), 876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, S.S.; Wilk, M.B. An analysis of variance test for normality (complete samples). Biometrika, 1965; 52, 3/4, 591–611. [Google Scholar]
- Abdi, H. Z-scores. Encyclopedia of Measurement and Statistics 2007, 3, 1055–1058. [Google Scholar]
- Huynh, H.; Meyer, P. Use of robust z in detecting unstable items in item response theory models. Pract. Assess. Res. Eval. 2010, 15(2), 1–8. [Google Scholar]
- Feng, C.; Wang, H.; Lu, N.; Tu, X.M. Log transformation: Application and interpretation in biomedical research. Stat. Med. 2013, 32(2), 230–239. [Google Scholar] [CrossRef] [PubMed]
- Bullard, J.H.; Purdom, E.; Hansen, K.D.; Dudoit, S. Evaluation of statistical methods for normalization and differential expression in mRNA-Seq experiments. BMC Bioinf. 2010, 11(1), 94. [Google Scholar] [CrossRef] [Green Version]
- Bolstad, B.M.; Irizarry, R.A.; Åstrand, M.; Speed, T.P. A comparison of normalization methods for high density oligonucleotide array data based on variance and bias. Bioinformatics 2003, 19(2), 185–193. [Google Scholar] [CrossRef] [Green Version]
- Hicks, S.C.; Irizarry, R.A. When to use quantile normalization? BioRxiv 2014, 012203. [Google Scholar]
- Kessy, A.; Lewin, A.; Strimmer, K. Optimal whitening and decorrelation. Am. Statist. 2018, 72(4), 309–314. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327(8476), 307–310. [Google Scholar] [CrossRef]
- Castaldo, R.; Melillo, P.; Bracale, U.; Caserta, M.; Triassi, M.; Pecchia, L. Acute mental stress assessment via short term HRV analysis in healthy adults: A systematic review with meta-analysis. Biomed. Signal Process. Control 2015, 18, 370–377. [Google Scholar] [CrossRef] [Green Version]
- Castaldo, R.; Melillo, P.; Izzo, R.; Luca, N.D.; Pecchia, L. Fall Prediction in Hypertensive Patients via Short-Term HRV Analysis. IEEE J. Biomed. Health Inf. 2017, 21(2), 399–406. [Google Scholar] [CrossRef] [PubMed]
- Castaldo, R.; Montesinos, L.; Melillo, P.; James, C.; Pecchia, L. Ultra-short term HRV features as surrogates of short term HRV: A case study on mental stress detection in real life. BMC Med. Inform. Decis. Making 2019, 19(1), 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, M.D.; Smyth, G.K. Moderated statistical tests for assessing differences in tag abundance. Bioinformatics 2007, 23(21), 2881–2887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, K.R.; Koprowski, R.; Skufca, J.D. Machine learning, medical diagnosis, and biomedical engineering research-commentary. BioMed. Eng. OnLine 2014, 13(94), 10.1186. [Google Scholar] [CrossRef] [Green Version]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Provost, F. Machine learning from imbalanced data sets 101. In Proceedings of the AAAI’2000 Workshop on Imbalanced Data Sets; AAAI Press: Menlo Park, CA, USA, 2000; pp. 1–3. [Google Scholar]
- Vapnik, V.N. Statistical Learning Theory; Wiley: New York, NY, USA, 1998; p. 736. [Google Scholar]
- Quinlan, J.R. C4.5: Programs For Machine Learning; Morgan Kaufmann Publishers: San Mateo, CA, USA, 1993. [Google Scholar]
- Nguyen, C.; Wang, Y.; Nguyen, H.N. Random forest classifier combined with feature selection for breast cancer diagnosis and prognostic. J. Biomed. Sci. Eng. 2013, 6(05), 551. [Google Scholar] [CrossRef]
- Kononenko, I. Semi-Naive Bayesian Classifier; European Working Session on Learning; Springer: Dordrecht, The Netherlands, 1991; pp. 206–219. [Google Scholar]
- Kohl, M. Performance measures in binary classification. Intl. J. Stat. Med. Res. 2012, 1(1), 79–81. [Google Scholar] [CrossRef]
- Loh, H.-Y.; Norman, B.P.; Lai, K.-S.; Rahman, N.M.A.N.A.; Alitheen, N.B.M.; Osman, M.A. The Regulatory Role of MicroRNAs in Breast Cancer. Intl. J. Mol. Sci. 2019, 20(19), 4940. [Google Scholar] [CrossRef] [Green Version]
- Changyong, F.; Hongyue, W.; Naiji, L.; Tian, C.; Hua, H.; Ying, L. Log-transformation and its implications for data analysis. Shanghai Arch. Psychiat. 2014, 26(2), 105. [Google Scholar]
- Haga, A.; Takahashi, W.; Aoki, S.; Nawa, K.; Yamashita, H.; Abe, O.; Nakagawa, K. Standardization of imaging features for radiomics analysis. J. Med. Invest. 2019, 66((1.2)), 35–37. [Google Scholar] [CrossRef]
- Panayides, A.S.; Pattichis, M.S.; Leandrou, S.; Pitris, C.; Constantinidou, A.; Pattichis, C.S. Radiogenomics for precision medicine with a big data analytics perspective. IEEE J. Biomed. Health Inform. 2018, 23(5), 2063–2079. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Baek, H.M.; Nalcioglu, O.; Su, M.Y. Estrogen receptor and breast MR imaging features: A correlation study. J. Magnet. Resonance Imag. 2008, 27(4), 825–833. [Google Scholar] [CrossRef] [Green Version]
- Koukourakis, M.I.; Manolas, C.; Minopoulos, G.; Giatromanolaki, A.; Sivridis, E. Angiogenesis relates to estrogen receptor negativity, c-erbB-2 overexpression and early relapse in node-negative ductal carcinoma of the breast. Intl. J. Surg. Pathol. 2003, 11(1), 29–34. [Google Scholar] [CrossRef]
- Fuckar, D.; Dekanic, A.; Stifter, S.; Mustac, E.; Krstulja, M.; Dobrila, F.; Jonjic, N. VEGF expression is associated with negative estrogen receptor status in patients with breast cancer. Intl. J. Surg. Pathol. 2006, 14(1), 49–55. [Google Scholar] [CrossRef] [PubMed]
- Arpino, G.; Weiss, H.; Lee, A.V.; Schiff, R.; De Placido, S.; Osborne, C.K.; Elledge, R.M. Estrogen receptor–positive, progesterone receptor–negative breast cancer: Association with growth factor receptor expression and tamoxifen resistance. J. Nat. Cancer Inst. 2005, 97(17), 1254–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youk, J.H.; Son, E.J.; Chung, J.; Kim, J.-A.; Kim, E.-k. Triple-negative invasive breast cancer on dynamic contrast-enhanced and diffusion-weighted MR imaging: Comparison with other breast cancer subtypes. Eur. Radiol. 2012, 22(8), 1724–1734. [Google Scholar] [CrossRef]
- Peterson, R.A.; Cavanaugh, J.E. Ordered quantile normalization: A semiparametric transformation built for the cross-validation era. J. Appl. Stat. 2019, 1–16. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number |
|---|---|
| Breast Cancer Types | |
| Ductal carcinoma | 79 |
| Lobular carcinoma | 10 |
| Mixed | 2 |
| Molecular Receptor Status | |
| Estrogen Receptor (ER) | |
| Positive | 76 |
| Negative | 15 |
| Progesterone Receptor (PR) | |
| Positive | 71 |
| Negative | 20 |
| Human Epidermal Growth Factor Receptor 2 (HER2) | |
| Positive | 12 |
| Negative | 74 |
| Triple Negative (TN) | |
| Triple negative (ER–, PR–, HER2–) | 12 |
| Others | 74 |
| Measure | Formula |
|---|---|
| Total Classification Accuracy (ACC) | |
| Sensitivity (SEN) | |
| Specificity (SPE) | |
| Area Under the Curve (AUC) | - |
| Non-Normalized | Scaling | Z-Score | Robust Z-Score | LOG | Quantile | Upper Quartile | WHT | |
|---|---|---|---|---|---|---|---|---|
| Feature Names | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) |
| T5 | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) | 0.287 (↓) |
| T11 | 0.031 (↓↓) | 0.031 (↓↓) | 0.031 (↓↓) | 0.031 (↓↓) | 0.031 (↓↓) | 0.031 (↓↓) | 0.031 (↓↓) | 0.002 (↓↓) |
| S1 | 0.003 (↑↑) | 0.003 (↑↑) | 0.003 (↑↑) | 0.003 (↑↑) | 0.003 (↑↑) | 0.003 (↑↑) | 0.003 (↑↑) | 0.688 (↑) |
| S2 | 0.003 (↑↑) | 0.003 (↑↑) | 0.003 (↑↑) | 0.003 (↑↑) | 0.003 (↑↑) | 0.003 (↑↑) | 0.003 (↑↑) | 0.004 (↑↑) |
| S3 | 0.011 (↑↑) | 0.011 (↑↑) | 0.011 (↑↑) | 0.011 (↑↑) | 0.011 (↑↑) | 0.011 (↑↑) | 0.011 (↑↑) | 0.524 (↓) |
| G3 | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) | 0.029 (↓↓) |
| Non-Normalized | Scaling | Z-Score | Robust Z-Score | LOG | Quantile | Upper Quartile | WHT | |
|---|---|---|---|---|---|---|---|---|
| Feature Names | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) |
| E3 | 0.021 (↓↓) | 0.021 (↓↓) | 0.021 (↓↓) | 0.021 (↓↓) | 0.021 (↓↓) | 0.021 (↓↓) | 0.021 (↓↓) | 0.418 (↑) |
| E4 | 0.038 (↓↓) | 0.038 (↓↓) | 0.038 (↓↓) | 0.038 (↓↓) | 0.038 (↓↓) | 0.038 (↓↓) | 0.038 (↓↓) | 0.867 (↑) |
| T2 | 0.071 (↓) | 0.071 (↓) | 0.071 (↓) | 0.071 (↓) | 0.071 (↓) | 0.071 (↓) | 0.071 (↓) | 0.046 (↓↓) |
| T4 | 0.049 (↑↑) | 0.049 (↑↑) | 0.049 (↑↑) | 0.049 (↑↑) | 0.049 (↑↑) | 0.049 (↑↑) | 0.049 (↑↑) | 0.178 (↑) |
| T5 | 0.004 (↓↓) | 0.004 (↓↓) | 0.004 (↓↓) | 0.004 (↓↓) | 0.004 (↓↓) | 0.004 (↓↓) | 0.004 (↓↓) | 0.02 (↓↓) |
| T6 | 0.02 (↑↑) | 0.02 (↑↑) | 0.02 (↑↑) | 0.02 (↑↑) | 0.02 (↑↑) | 0.02 (↑↑) | 0.02 (↑↑) | 0.303 (↑) |
| S2 | 0.175 (↑) | 0.175 (↑) | 0.175 (↑) | 0.175 (↑) | 0.175 (↑) | 0.175 (↑) | 0.175 (↑) | 0.021 (↑↑) |
| Non-Normalized | Scaling | Z-Score | Robust Z-Score | LOG | Quantile | Upper Quartile | WHT | |
|---|---|---|---|---|---|---|---|---|
| Feature Names | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) |
| K6 | 0.054 (↑) | 0.054 (↑) | 0.054 (↑) | 0.054 (↑) | 0.054 (↑) | 0.054 (↑) | 0.054 (↑) | 0.008 (↑↑) |
| T8 | 0.414 (↑) | 0.414 (↑) | 0.414 (↑) | 0.414 (↑) | 0.414 (↑) | 0.414 (↑) | 0.414 (↓) | 0.025 (↑↑) |
| M3 | 0.393 (↑) | 0.393 (↑) | 0.393 (↑) | 0.393 (↑) | 0.393 (↑) | 0.393 (↑) | 0.393 (↑) | 0.048 (↑↑) |
| Non- Normalized | Scaling | Z-Score | Robust Z-Score | LOG | Quantile | Upper Quartile | WHT | |
|---|---|---|---|---|---|---|---|---|
| Feature Names | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) | Pval (Trend) |
| E2 | 0.048 (↑↑) | 0.048 (↑↑) | 0.048 (↑↑) | 0.048 (↑↑) | 0.048 (↑↑) | 0.048 (↑↑) | 0.048 (↑↑) | 0.035 (↑↑) |
| T6 | 0.107 (↑) | 0.107 (↑) | 0.107 (↑) | 0.107 (↑) | 0.107 (↑) | 0.107 (↑) | 0.107 (↑) | 0.024 (↑↑) |
| T11 | 0.078 (↓) | 0.078 (↓) | 0.078 (↓) | 0.078 (↓) | 0.078 (↓) | 0.078 (↓) | 0.078 (↓) | 0.024 (↓↓) |
| G2 | 0.048 (↑↑) | 0.048 (↑↑) | 0.048 (↑↑) | 0.048 (↑↑) | 0.048 (↑↑) | 0.048 (↑↑) | 0.048 (↑↑) | 0.019 (↑↑) |
| S1 | 0.01 (↑↑) | 0.01 (↑↑) | 0.01 (↑↑) | 0.01 (↑↑) | 0.01 (↑↑) | 0.01 (↑↑) | 0.01 (↑↑) | 0.458 (↑) |
| S2 | 0.01 (↑↑) | 0.01 (↑↑) | 0.01 (↑↑) | 0.01 (↑↑) | 0.01 (↑↑) | 0.01 (↑↑) | 0.01 (↑↑) | 0.021 (↑↑) |
| S3 | 0.012 (↑↑) | 0.012 (↑↑) | 0.012 (↑↑) | 0.012 (↑↑) | 0.012 (↑↑) | 0.012 (↑↑) | 0.012 (↑↑) | 0.259 (↑) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castaldo, R.; Pane, K.; Nicolai, E.; Salvatore, M.; Franzese, M. The Impact of Normalization Approaches to Automatically Detect Radiogenomic Phenotypes Characterizing Breast Cancer Receptors Status. Cancers 2020, 12, 518. https://doi.org/10.3390/cancers12020518
Castaldo R, Pane K, Nicolai E, Salvatore M, Franzese M. The Impact of Normalization Approaches to Automatically Detect Radiogenomic Phenotypes Characterizing Breast Cancer Receptors Status. Cancers. 2020; 12(2):518. https://doi.org/10.3390/cancers12020518
Chicago/Turabian StyleCastaldo, Rossana, Katia Pane, Emanuele Nicolai, Marco Salvatore, and Monica Franzese. 2020. "The Impact of Normalization Approaches to Automatically Detect Radiogenomic Phenotypes Characterizing Breast Cancer Receptors Status" Cancers 12, no. 2: 518. https://doi.org/10.3390/cancers12020518