Predictive Nomogram for Early Recurrence after Pancreatectomy in Resectable Pancreatic Cancer: Risk Classification Using Preoperative Clinicopathologic Factors

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients Database
2.2. Preoperative Data
2.3. Data Analysis and Statistical Methods
3. Results
3.1. Demographic Features of Preoperative Factors
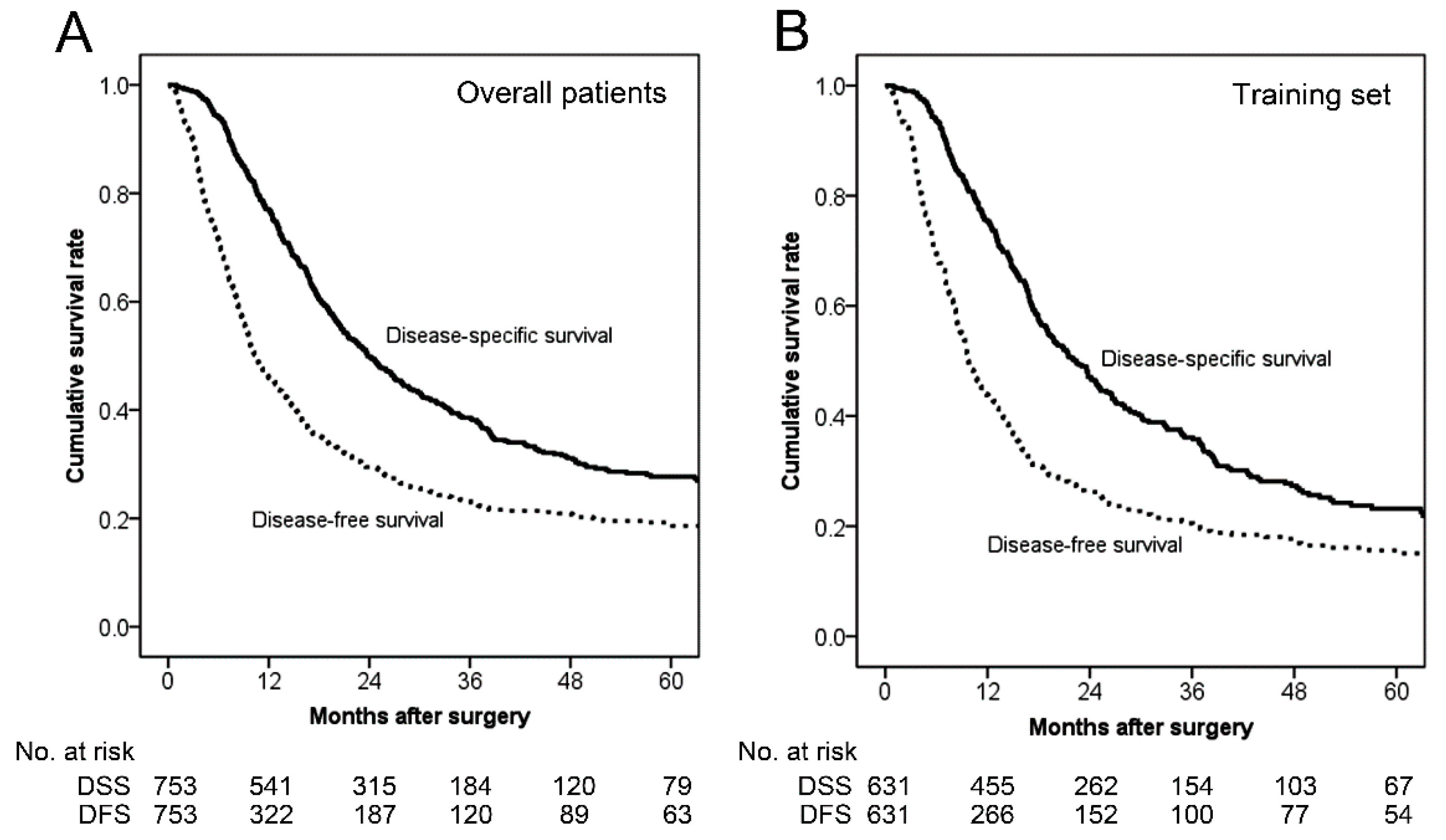
3.2. Survival Analysis
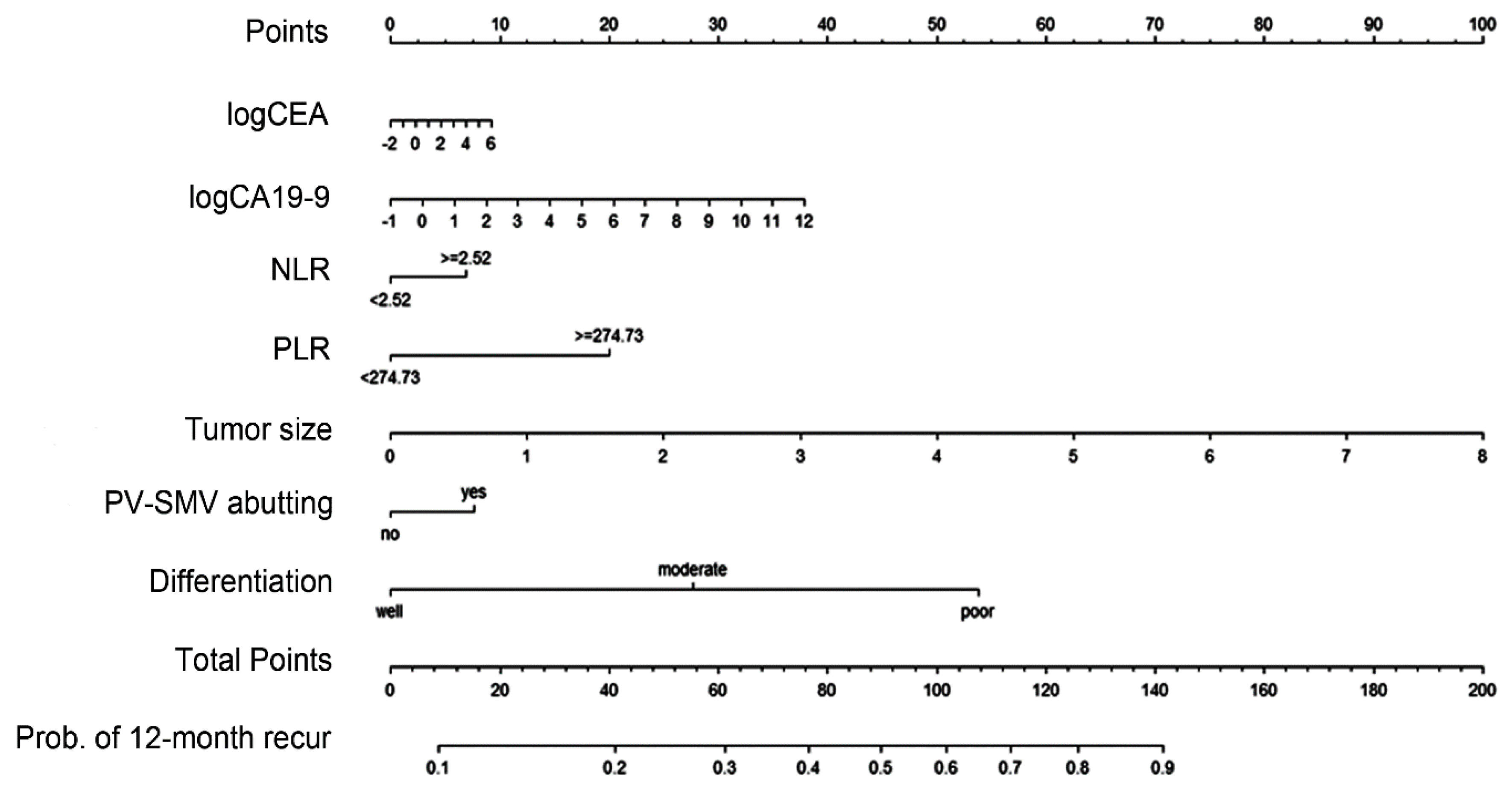
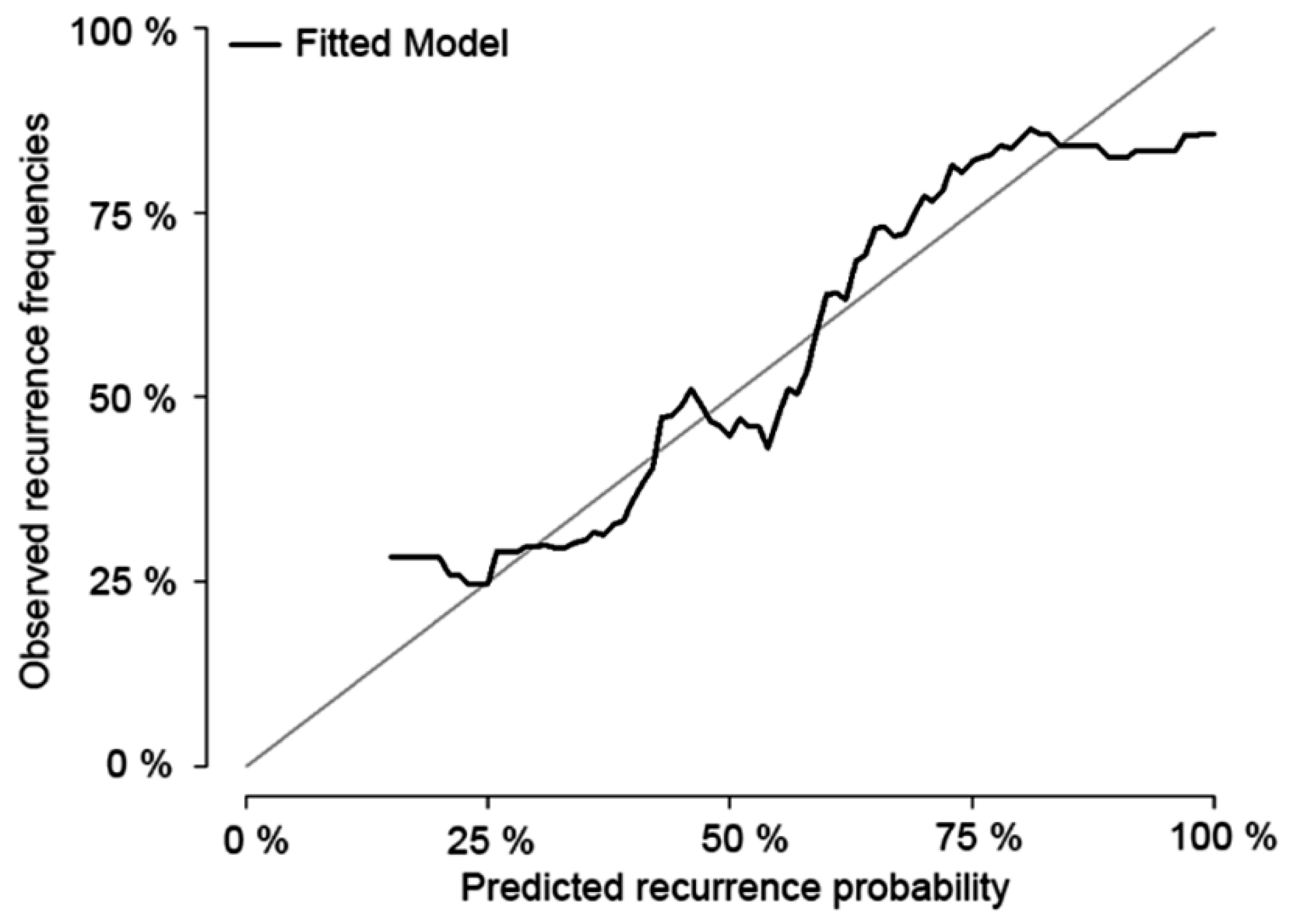
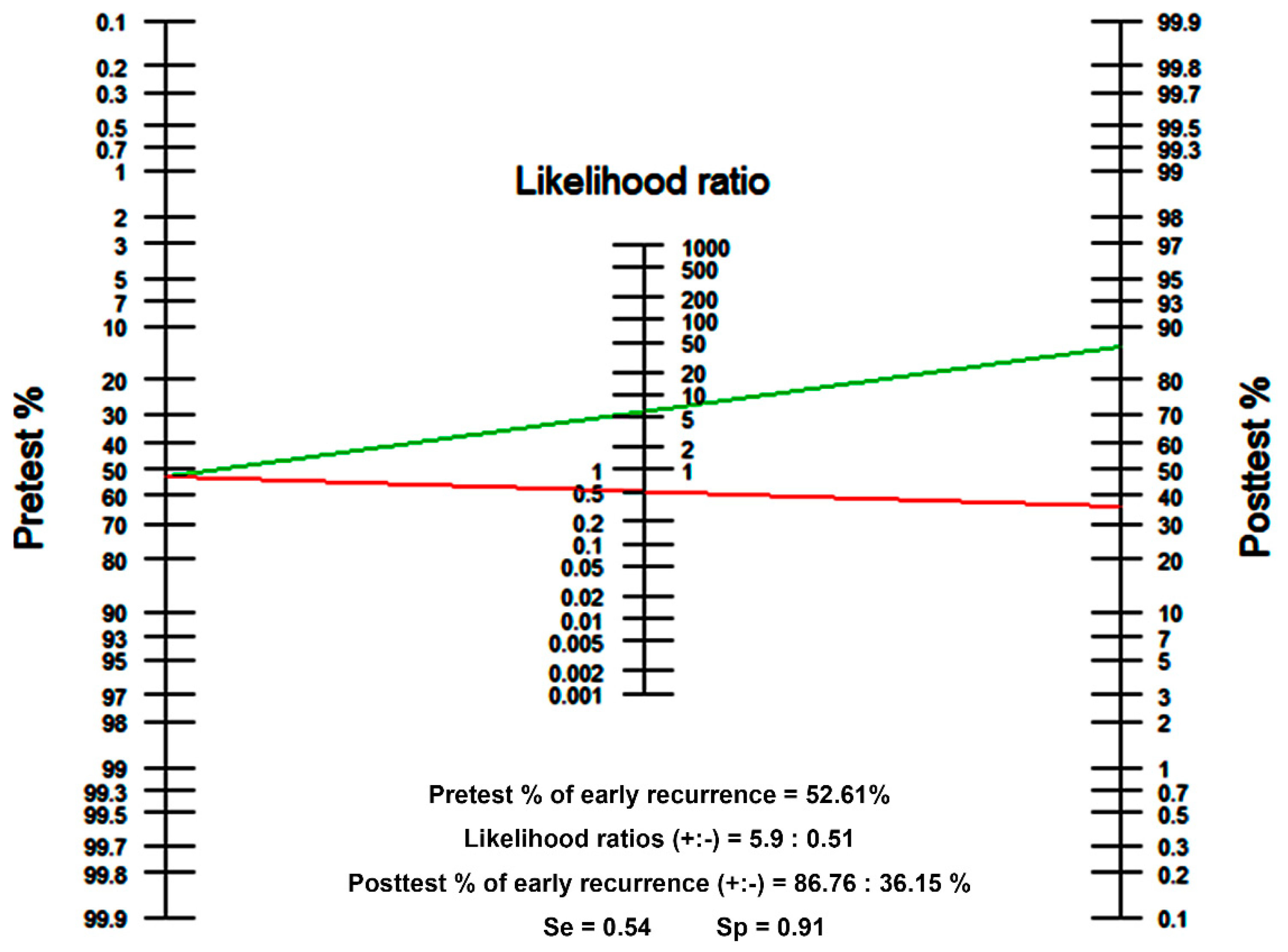
3.3. Preoperative Risk Factors and Establishment of a Nomogram
3.4. Postoperative Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kyu-Won Jung, M.; Lee, E.S. Cancer Statistics in Korea: Incidence, Mortality, Survival, and Prevalence in 2015. Cancer Res. Treat. 2018, 50, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, A.; Calabrò, F.; Sternberg, C.N. Current therapies and advances in the treatment of pancreatic cancer. Crit. Rev. Oncol. Hematol. 2006, 58, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Kim, S.C.; Song, K.-B.; Hwang, D.W.; Lee, J.H.; Park, K.-M.; Lee, Y.-J. Chronologic changes in clinical and survival features of pancreatic ductal adenocarcinoma since 2000: A single-center experience with 2,029 patients. Surgery 2018, 164, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Tempero, M.A.; Malafa, M.P.; Chiorean, E.G.; Czito, B.; Scaife, C.; Narang, A.K.; Fountzilas, C.; Wolpin, B.M.; Al-Hawary, M.; Asbun, H.; et al. Pancreatic Adenocarcinoma, Version 1.2019. J. Natl. Compr. Cancer Netw. 2019, 17, 202–210. [Google Scholar] [CrossRef] [Green Version]
- Heye, T.; Zausig, N.; Klauss, M.; Singer, R.; Werner, J.; Richter, G.M.; Kauczor, H.-U.; Grenacher, L. CT diagnosis of recurrence after pancreatic cancer: Is there a pattern? World J. Gastroenterol. 2011, 17, 1126–1134. [Google Scholar] [CrossRef]
- Groot, V.P.; Gemenetzis, G.; Blair, A.B.; Rivero-Soto, R.J.; Yu, J.; Javed, A.A.; Burkhart, R.A.; Rinkes, I.H.B.; Molenaar, I.Q.; Cameron, J.L.; et al. Defining and predicting early recurrence in 957 patients with resected pancreatic ductal adenocarcinoma. Ann. Surg. 2019, 269, 1154–1162. [Google Scholar] [CrossRef]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; Fletcher, C.D.; O’Reilly, D.S.J.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. A comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome Study. Eur. J. Cancer 2011, 47, 2633–2641. [Google Scholar] [CrossRef]
- Fagan, T. Nomogram for Bayes’s theorem. N. Engl. J. Med. 1975, 293, e257. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Casadei, R.; Ricci, C.; Pezzilli, R.; Calculli, L.; D’Ambra, M.; Taffurelli, G.; Minni, F. Assessment of complications according to the Clavien-Dindo classification after distal pancreatectomy. JOP 2011, 12, 126–130. [Google Scholar] [PubMed]
- Lim, J.E.; Chien, M.W.; Earle, C.C. Prognostic factors following curative resection for pancreatic adenocarcinoma: A population-based, linked database analysis of 396 patients. Ann. Surg. 2003, 237, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Kim, S.C.; Hong, S.-M.; Song, K.-B.; Lee, J.H.; Park, K.-M.; Lee, Y.-J. Can statistically determined prognostic factors predict the long-term survival of patients with pancreatic ductal adenocarcinoma following surgical resection? Clinicopathological analysis of 82 long-term survivors. Pancreas 2014, 43, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Brennan, M.F.; Kattan, M.W.; Klimstra, D.; Conlon, K. Prognostic nomogram for patients undergoing resection for adenocarcinoma of the pancreas. Ann. Surg. 2004, 240, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Ferrone, C.R.; Kattan, M.W.; Tomlinson, J.S.; Thayer, S.P.; Brennan, M.F.; Warshaw, A.L. Validation of a postresection pancreatic adenocarcinoma nomogram for disease-specific survival. J. Clin. Oncol. 2005, 23, 7529–7535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, C.; Mao, Y.; Wang, J.; Duan, F.; Lin, X.; Li, S. Nomograms predict long-term survival for patients with periampullary adenocarcinoma after pancreatoduodenectomy. BMC Cancer 2018, 18, e327. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-B.; Zhou, J.; Zhao, F.-Q. A Prognostic Nomogram for Disease-Specific Survival in Patients with Pancreatic Ductal Adenocarcinoma of the Head of the Pancreas Following Pancreaticoduodenectomy. Med. Sci. Monit. 2018, 24, 6313–6321. [Google Scholar] [CrossRef]
- Jang, J.-Y.; Han, Y.; Lee, H.; Kim, S.-W.; Kwon, W.; Lee, K.-H.; Oh, D.-Y.; Chie, E.K.; Lee, J.M.; Heo, J.S.; et al. Oncological benefits of neoadjuvant chemoradiation with gemcitabine versus upfront surgery in patients with borderline resectable pancreatic cancer: A prospective, randomized, open-label, multicenter phase 2/3 trial. Ann. Surg. 2018, 268, 215–222. [Google Scholar] [CrossRef]
- Murphy, J.E.; Wo, J.Y.; Ryan, D.P.; Jiang, W.; Yeap, B.Y.; Drapek, L.C.; Blaszkowsky, L.S.; Kwak, E.L.; Allen, J.N.; Clark, J.W.; et al. Total neoadjuvant therapy with FOLFIRINOX followed by individualized chemoradiotherapy for borderline resectable pancreatic adenocarcinoma: A phase 2 clinical trial. JAMA Oncol. 2018, 4, 963–969. [Google Scholar] [CrossRef] [Green Version]
- Gemenetzis, G.; Groot, V.P.; Blair, A.B.; Laheru, D.A.; Zheng, L.; Narang, A.K.; Fishman, E.K.; Hruban, R.H.; Yu, J.; Burkhart, R.A.; et al. Survival in locally advanced pancreatic cancer after neoadjuvant therapy and surgical resection. Ann. Surg. 2019, 270, 340–347. [Google Scholar] [CrossRef]
- Yoo, C.; Shin, S.H.; Kim, K.-p.; Jeong, J.H.; Chang, H.-M.; Kang, J.H.; Lee, S.S.; Park, D.H.; Song, T.J.; Seo, D.W.; et al. Clinical Outcomes of Conversion Surgery after Neoadjuvant Chemotherapy in Patients with Borderline Resectable and Locally Advanced Unresectable Pancreatic Cancer: A Single-Center, Retrospective Analysis. Cancers 2019, 11, 278. [Google Scholar] [CrossRef] [Green Version]
- Mokdad, A.A.; Minter, R.M.; Zhu, H.; Augustine, M.M.; Porembka, M.R.; Wang, S.C.; Yopp, A.C.; Mansour, J.C.; Choti, M.A.; Polanco, P.M.; et al. Neoadjuvant therapy followed by resection versus upfront resection for resectable pancreatic cancer: A propensity score matched analysis. J. Clin. Oncol. 2016, 35, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Versteijne, E.; Vogel, J.A.; Besselink, M.; Busch, O.; Wilmink, J.; Daams, J.; van Eijck, C.; Groot Koerkamp, B.; Rasch, C.; van Tienhoven, G.; et al. Meta-analysis comparing upfront surgery with neoadjuvant treatment in patients with resectable or borderline resectable pancreatic cancer. Br. J. Surg. 2018, 105, 946–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Overall Patients (n = 753) | Training Set (n = 631) | ||||
|---|---|---|---|---|---|---|
| No or Late Recurrence (n = 359) | Early Recurrence (n = 394) | p | No or Late Recurrence (n = 299) | Early Recurrence (n = 332) | p | |
| Age, years | 0.534 | 0.612 | ||||
| Mean (±SD) | 62.7 (±10.3) | 63.1 (±10.2) | 62.8 (±10.3) | 63.2 (±10.1) | ||
| Sex, n (%) | 0.589 | 0.667 | ||||
| Male | 209 (58.2) | 237 (60.2) | 176 (58.8) | 201 (60.6) | ||
| Female | 150 (41.8) | 150 (41.8) | 123 (41.2) | 131 (39.4) | ||
| BMI, kg/m2 | 0.346 | 0.507 | ||||
| Mean (±SD) | 23.1 (±3.0) | 22.9 (±3.1) | 23.0 (±3.0) | 22.9 (±3.1) | ||
| Underlying DM, n (%) | 0.381 | 0.639 | ||||
| No | 239 (62.9) | 248 (62.9) | 199 (66.5) | 209 (63.0) | ||
| Within 1 year | 43 (12.0) | 54 (13.7) | 40 (13.4) | 49 (14.7) | ||
| Beyond 1 year | 77 (21.4) | 92 (23.4) | 60 (20.1) | 74 (22.3) | ||
| CEA, n (%) | 0.087 | 0.141 | ||||
| Normal (<5.0 ng/m) | 281 (78.8) | 293 (74.4) | 269 (90.0) | 286 (86.1) | ||
| Elevated (≥5.0 ng/m) | 31 (11.6) | 49 (12.4) | 30 (10.0) | 46 (13.9) | ||
| NA | 47 (7.6) | 52 (13.2) | ||||
| CA19-9 | <0.001 | 0.004 | ||||
| Normal (<37 U/mL) | 133 (37.0) | 101 (25.6) | 106 (35.4) | 83 (25.0) | ||
| Elevated (≥37 U/mL) | 219 (61.0) | 290 (73.6) | 193 (64.6) | 249 (75.0) | ||
| NA | 7 (2.0) | 3 (0.8) | ||||
| NLR, n (%) † | 0.016 | 0.014 | ||||
| <2.52 | 281 (78.3) | 278 (70.6) | 224 (74.9) | 219 (66.0) | ||
| ≥2.52 | 78 (21.7) | 116 (29.4) | 75 (25.1) | 113 (34.0) | ||
| PLR, n (%) † | 0.073 | 0.011 | ||||
| <274.73 | 280 (78.0) | 285 (72.3) | 287 (96.9) | 302 (91.0) | ||
| ≥274.73 | 79 (22.0) | 109 (27.7) | 12 (4.0) | 30 (9.0) | ||
| PV-SMV abutment, n (%) | 0.102 | 0.075 | ||||
| No | 271 (75.5) | 276 (70.1) | 227 (76.9) | 231 (69.6) | ||
| Yes | 88 (24.5) | 118 (29.9) | 72 (24.1) | 101 (30.4) | ||
| Tumour size on CT, cm | <0.001 | <0.001 | ||||
| Mean (±SD) | 2.47 (±1.03) | 2.98 (±1.04) | 2.41 (±0.93) | 2.97 (1.05) | ||
| Tumour location | 0.602 | 0.272 | ||||
| Head | 255 (71.0) | 273 (69.3) | 219 (73.2) | 230 (69.3) | ||
| Body or tail | 104 (29.0) | 121 (30.7) | 80 (26.8) | 102 (30.7) | ||
| Differentiation | <0.001 | <0.001 | ||||
| Well | 38 (10.6) | 16 (4.0) | 34 (11.4) | 15 (4.5) | ||
| Moderate | 239 (66.6) | 232 (58.9) | 205 (68.5) | 196 (59.0) | ||
| Poor or undifferentiated | 70 (19.5) | 135 (34.3) | 60 (20.1) | 121 (36.5) | ||
| NA | 12 (3.3) | 11 (2.8) | ||||
| Factors | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|
| p | HR | 95% CI | p | HR | 95% CI | |
| Age, year | 0.23 | 1.003 | 0.93–1.014 | |||
| Sex | ||||||
| Male | Reference | |||||
| Female | 0.68 | 0.955 | 0.766–1.190 | |||
| BMI, kg/m2 | 0.60 | 0.990 | 0.956–1.027 | |||
| DM | ||||||
| No | Reference | |||||
| within 1 year | 0.48 | 1.119 | 0.820–1.528 | |||
| beyond 1 year | 0.44 | 1.110 | 0.851–1.447 | |||
| logCEA | 0.04 | 1.150 | 1.008–1.312 | 0.69 | 1.027 | 0.897–1.177 |
| logCA19-9 | <0.001 | 1.113 | 1.056–1.174 | 0.015 | 1.039 | 0.975–1.107 |
| NLR † | ||||||
| <2.52 | Reference | Reference | ||||
| ≥2.52 | 0.019 | 1.313 | 1.046–1.648 | 0.20 | 1.175 | 0.918–1.503 |
| PLR † | ||||||
| <274.73 | Reference | Reference | ||||
| ≥274.73 | 0.004 | 1.748 | 1.200–2.545 | 0.028 | 1.590 | 1.501-2.405 |
| Tumor size in CT, cm | <0.001 | 1.351 | 1.240–1.472 | <0.001 | 1.337 | 1.222-1.463 |
| PV-SMV abutment | ||||||
| No | Reference | Reference | ||||
| Yes | 0.047 | 1.268 | 1.003–1.602 | 0.140 | 1.195 | 0.943–1.514 |
| Tumor location | ||||||
| Head | Reference | |||||
| Body or Tail | 0.32 | 1.125 | 0.891–1.420 | |||
| Differentiation | ||||||
| Well | Reference | Reference | ||||
| Moderate | 0.020 | 1.867 | 1.104–3.156 | 0.017 | 1.904 | 1.123–3.228 |
| Poor or undifferentiated | <0.001 | 3.399 | 1.986–5.817 | <0.001 | 3.490 | 2.032–5.995 |
| Factors | No or Late Recurrence (n = 299) | Early Recurrence (n = 332) | p |
|---|---|---|---|
| T stage, n (%) | <0.001 | ||
| T1 | 90(30.1) | 46(13.9) | |
| T2 | 185(61.9) | 215(64.8) | |
| T3 | 24(8.0) | 70(21.1) | |
| T4 | 0(0.0) | 1(0.3) | |
| N stage, n (%) | <0.001 | ||
| N0 | 130(43.5) | 93(28.0) | |
| N1 | 129(43.1) | 135(40.7) | |
| N2 | 40(13.4) | 104(31.3) | |
| Postoperative complications *, n (%) | 0.101 | ||
| No or Grade I | 175(58.5) | 216(65.1) | |
| Grade II or above | 124(41.5) | 116(34.9) | |
| Resection margin, n (%) | 0.246 | ||
| R0 | 232(77.6) | 270(81.3) | |
| R1 | 67(22.4) | 62(18.7) | |
| Adjuvant therapy, n (%) | 0.338 | ||
| No | 97(32.4) | 126(37.9) | |
| Yes | 200(66.9) | 205(61.8) | |
| NA | 2(0.7) | 1(0.3) | |
| Recurrence pattern, n (%) | <0.001 | ||
| No | 151 | ||
| Locoregional † | 53(36.1) | 68(20.4) | |
| Systemic ‡ | 94(63.9) | 265(79.6) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, N.; Han, I.W.; Ryu, Y.; Hwang, D.W.; Heo, J.S.; Choi, D.W.; Shin, S.H. Predictive Nomogram for Early Recurrence after Pancreatectomy in Resectable Pancreatic Cancer: Risk Classification Using Preoperative Clinicopathologic Factors. Cancers 2020, 12, 137. https://doi.org/10.3390/cancers12010137
Kim N, Han IW, Ryu Y, Hwang DW, Heo JS, Choi DW, Shin SH. Predictive Nomogram for Early Recurrence after Pancreatectomy in Resectable Pancreatic Cancer: Risk Classification Using Preoperative Clinicopathologic Factors. Cancers. 2020; 12(1):137. https://doi.org/10.3390/cancers12010137
Chicago/Turabian StyleKim, Naru, In Woong Han, Youngju Ryu, Dae Wook Hwang, Jin Seok Heo, Dong Wook Choi, and Sang Hyun Shin. 2020. "Predictive Nomogram for Early Recurrence after Pancreatectomy in Resectable Pancreatic Cancer: Risk Classification Using Preoperative Clinicopathologic Factors" Cancers 12, no. 1: 137. https://doi.org/10.3390/cancers12010137