Third Epidemiological Analysis of Nasopharyngeal Carcinoma in the Central Region of Japan from 2006 to 2015

 , , and
, , and 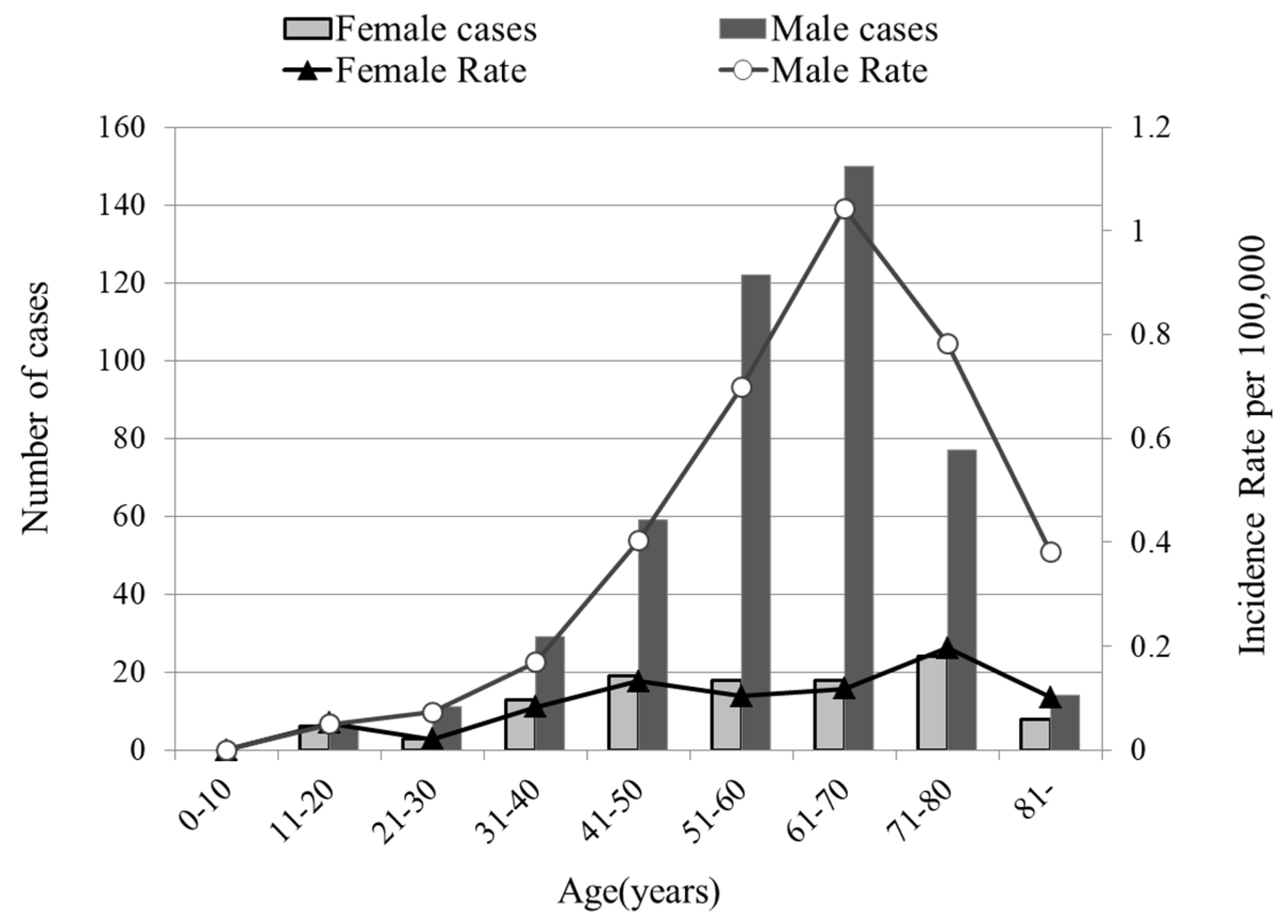{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Number of NPC Patients
2.2. Age-Standardized Annual Incidence of NPC Per 100,000 Individuals
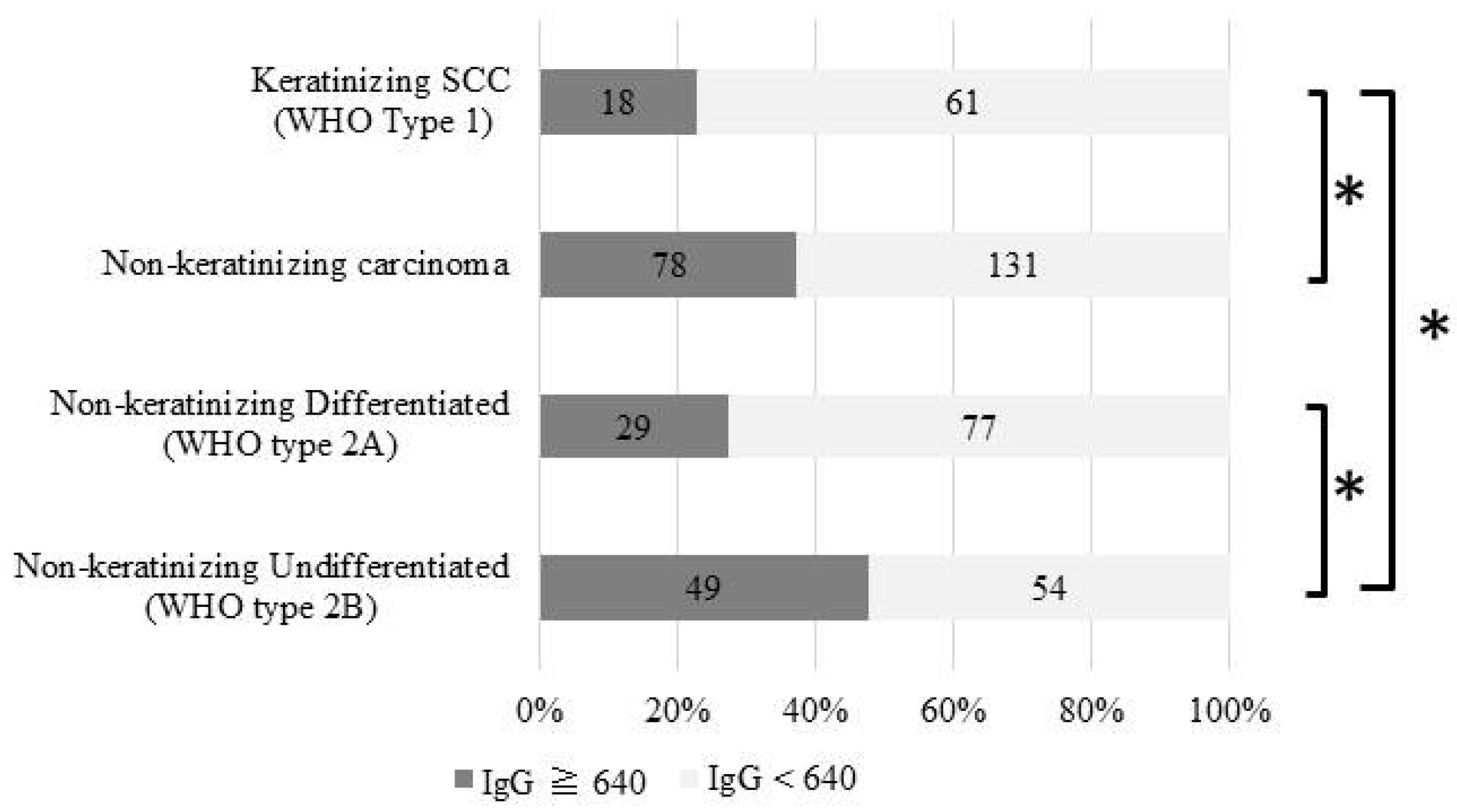
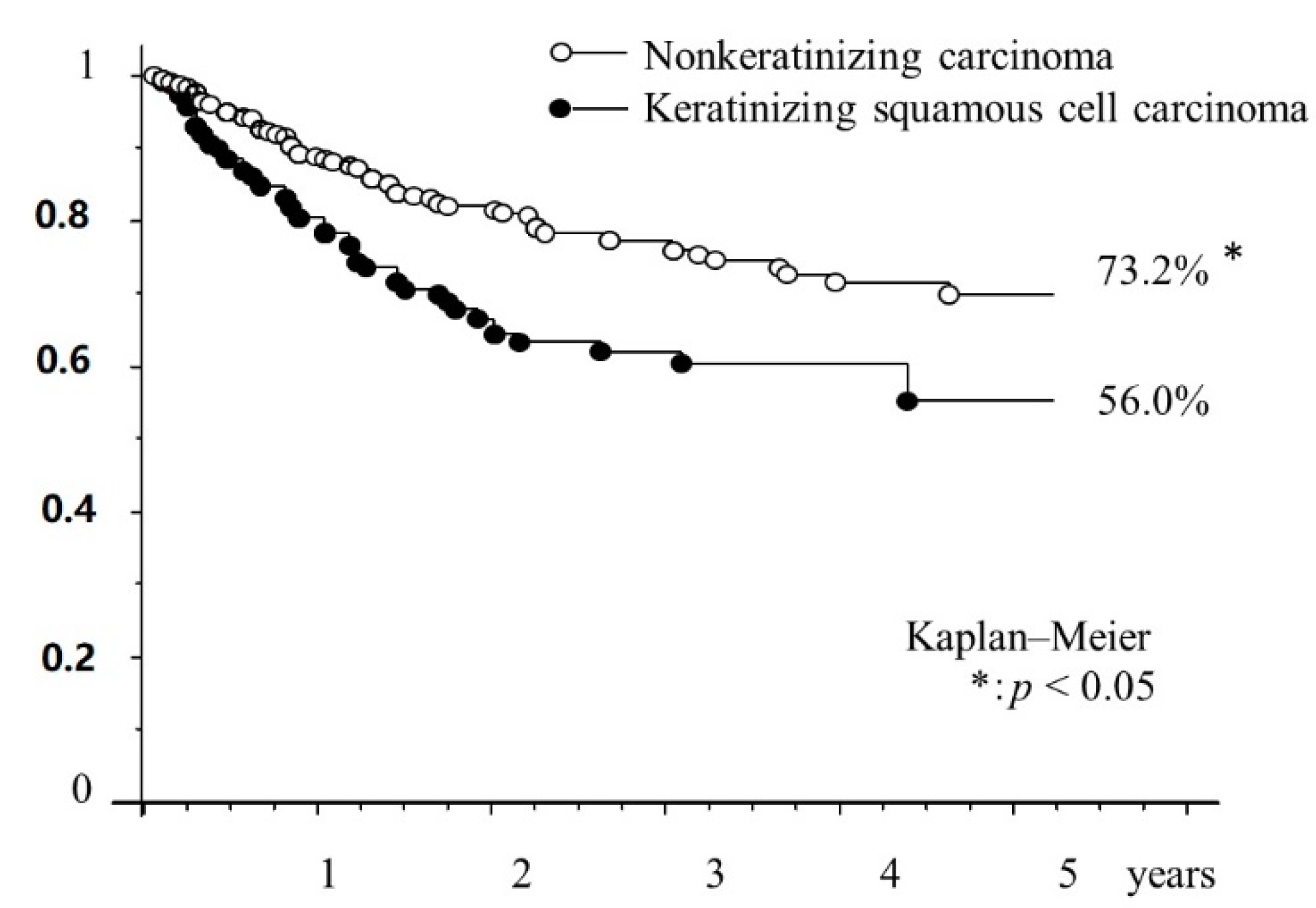
2.3. Patients Histologically Classified according to the 2005 WHO Criteria
2.4. Positive Rates of Serum Antibodies to EBV Antigens
2.5. Anatomical Subsites Based on UICC Criteria
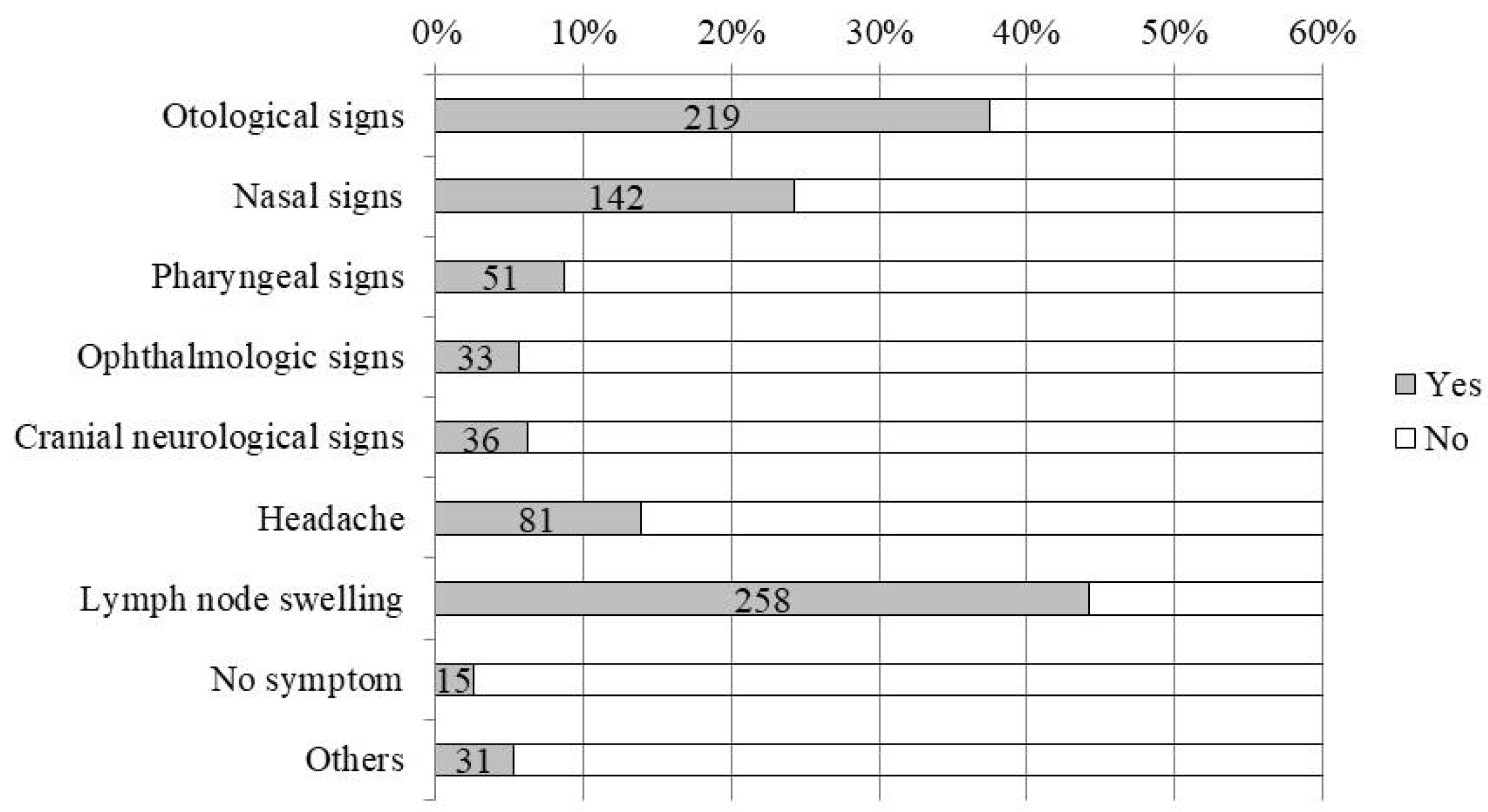
2.6. Clinical Symptoms
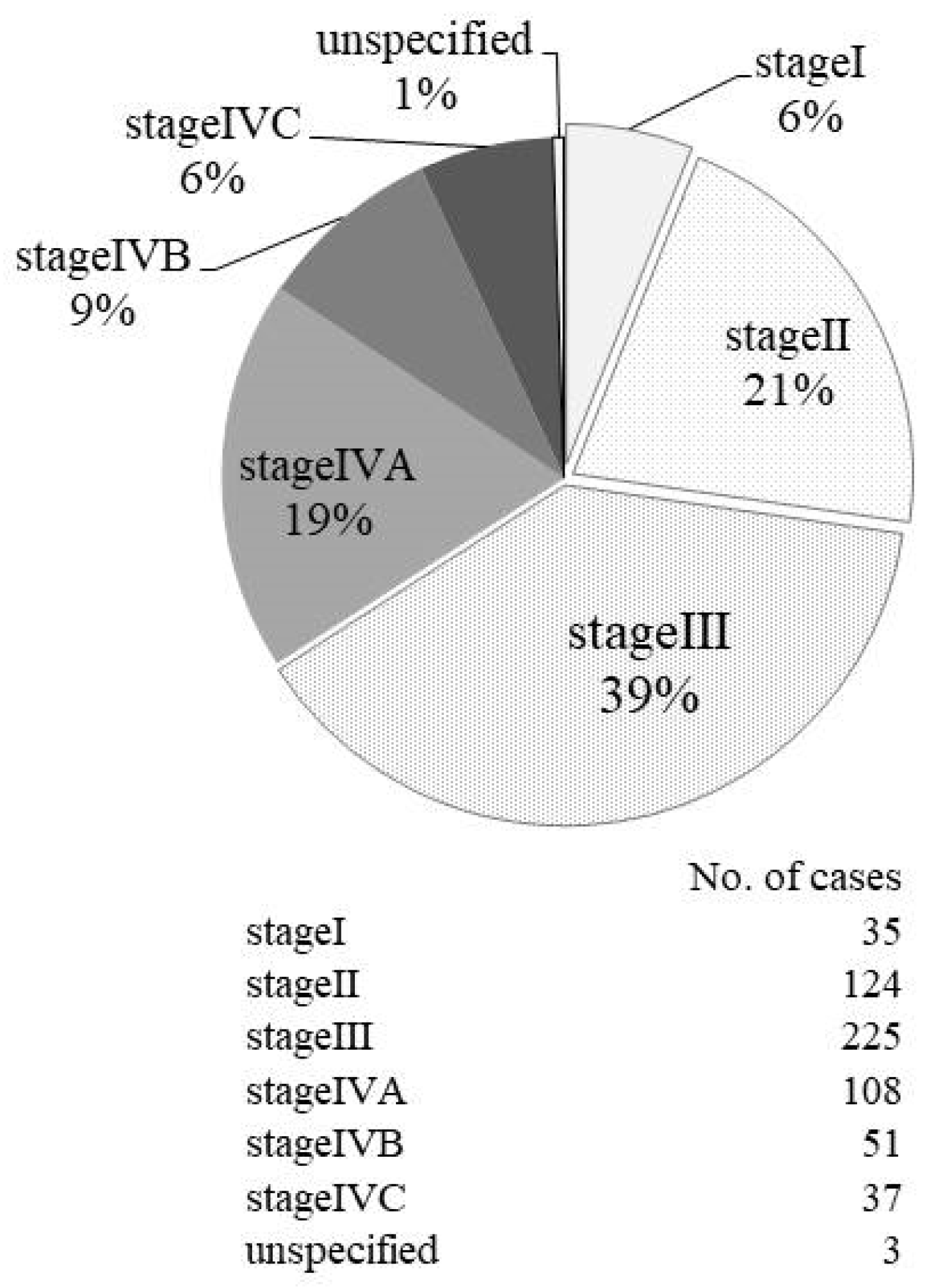
2.7. Patient Staging by UICC TNM Classification
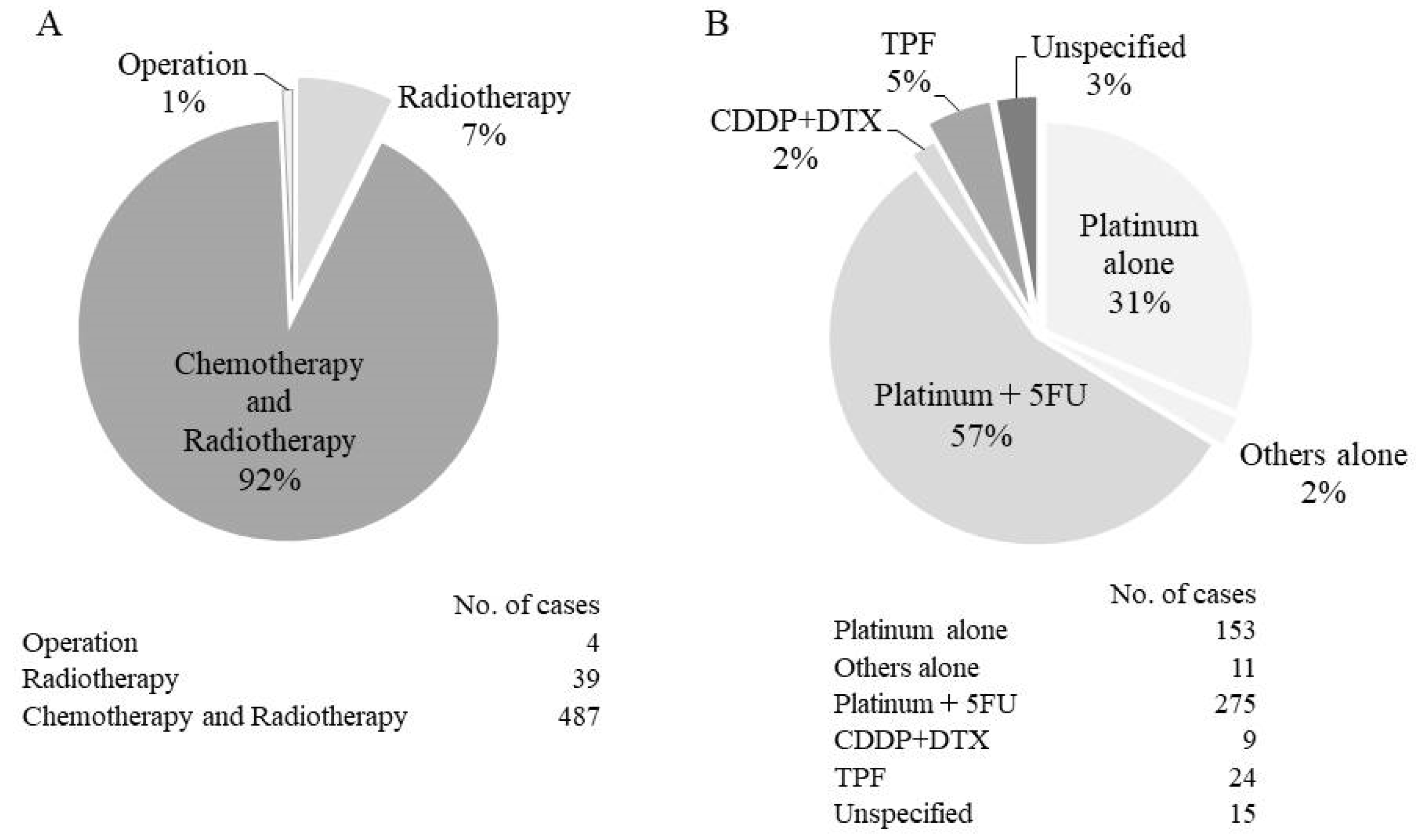
2.8. Treatments
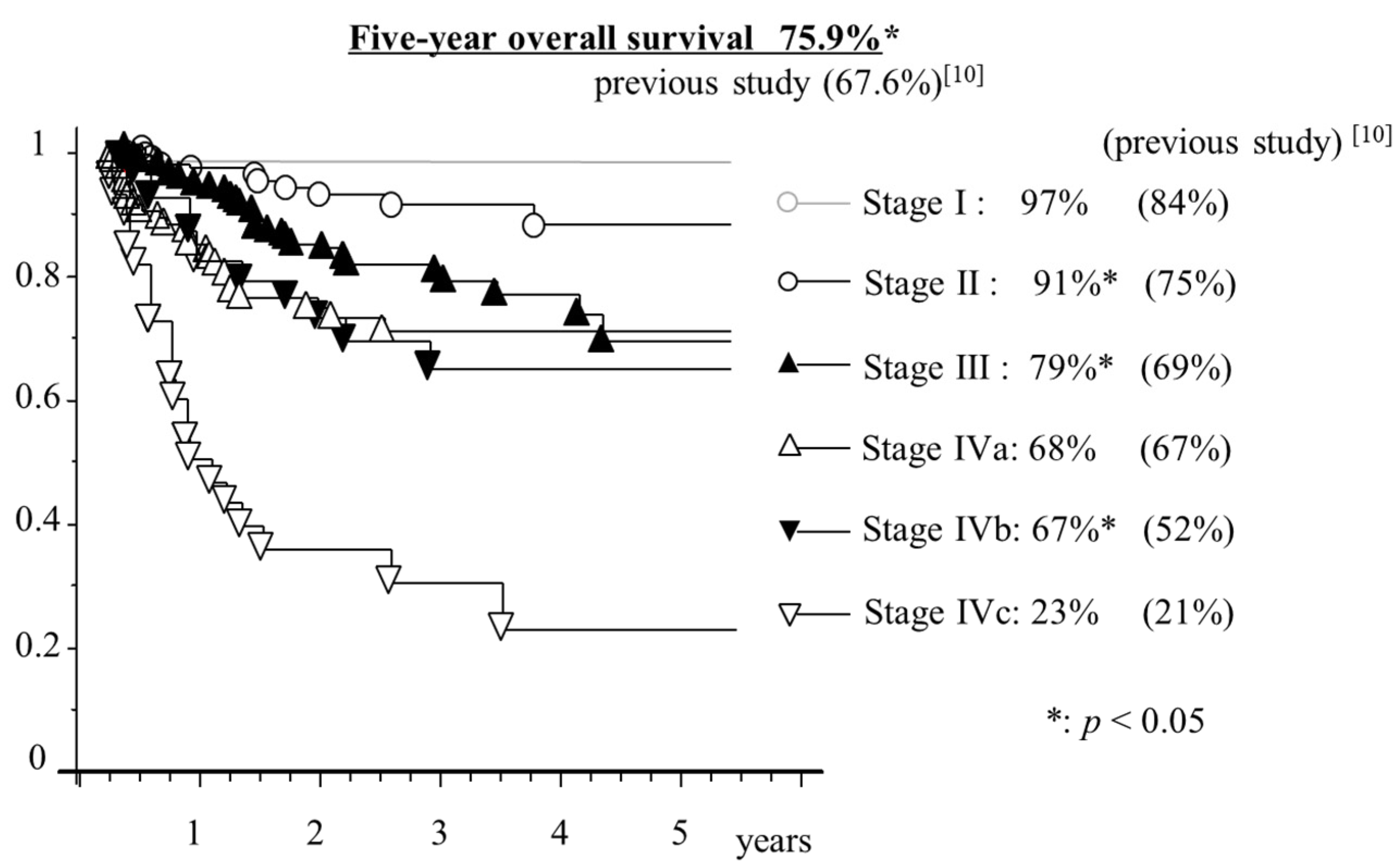
2.9. Analysis of Five-year overall Survival Trends for NPC
2.10. Relationship between Smoking and Incidence of NPC
3. Discussion
4. Materials and Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Wu, S.; Xia, B.; Han, F.; Xie, R.; Song, T.; Lu, L.; Yu, W.; Deng, X.; He, Q.; Zhao, C.; et al. Prognostic nomogram for patients with nasopharyngeal carcinoma after intensity-modulated radiotherapy. PLoS ONE 2015, 10, e0134491. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Li, C.; Pan, L. Nasopharyngeal carcinoma: A review of current updates. Exp. Ther. Med. 2018, 15, 3687–3692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamran, S.C.; Riaz, N.; Lee, N. Nasopharyngeal carcinoma. Surg. Oncol. Clin. N. Am. 2015, 24, 547–561. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.T.; Adami, H.O. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol Biomark. Prev. 2006, 15, 1765–1777. [Google Scholar] [CrossRef] [PubMed]
- Yoshizaki, T.; Ito, M.; Murono, S.; Wakisaka, N.; Kondo, S.; Endo, K. Current understanding and management of nasopharyngeal carcinoma. Auris. Nasus. Larynx 2012, 39, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakanishi, Y.; Wakisaka, N.; Kondo, S.; Endo, K.; Sugimoto, H.; Hatano, M.; Ueno, T.; Ishikawa, K.; Yoshizaki, T. Progression of understanding for the role of Epstein-Barr virus and management of nasopharyngeal carcinoma. Cancer Metastasis Rev. 2017, 36, 435–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Tang, L.L.; Chen, L.; Li, W.F.; Mao, Y.P.; Liu, L.Z.; Lin, A.H.; Li, L.; Ma, J. Promising treatment outcomes of intensity-modulated radiation therapy for nasopharyngeal carcinoma patients with N0 disease according to the seventh edition of the AJCC staging system. BMC Cancer 2012, 12, 68. [Google Scholar] [CrossRef] [PubMed]
- Li, A.C.; Xiao, W.W.; Shen, G.Z.; Wang, L.; Xu, A.A.; Cao, Y.Q.; Huang, S.M.; Lin, C.G.; Han, F.; Deng, X.W.; et al. Distant metastasis risk and patterns of nasopharyngeal carcinoma in the era of IMRT: Long-term results and benefits of chemotherapy. Oncotarget 2015, 6, 24511–24521. [Google Scholar] [CrossRef]
- Kimura, Y.; Suzuki, D.; Tokunaga, T.; Takabayashi, T.; Yamada, T.; Wakisaka, N.; Yoshizaki, T.; Murata, H.; Miwa, K.; Shoujaku, H.; et al. Epidemiological analysis of nasopharyngeal carcinoma in the central region of Japan during the period from 1996 to 2005. Auris. Nasus. Larynx 2011, 38, 244–249. [Google Scholar] [CrossRef]
- Takeshita, H.; Furukawa, M.; Fujieda, S.; Shoujaku, H.; Ookura, T.; Sakaguchi, M.; Ito, H.; Mineta, H.; Harada, T.; Matsuura, H.; et al. Epidemiological research into nasopharyngeal carcinoma in the Chubu region of Japan. Auris. Nasus. Larynx 1999, 26, 277–286. [Google Scholar] [CrossRef]
- Cao, S.M.; Simons, M.J.; Qian, C.N. The prevalence and prevention of nasopharyngeal carcinoma in China. Chin. J. Cancer 2011, 30, 114–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.P.; Chan, A.T.C.; Le, Q.T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef]
- Marks, J.E.; Phillips, J.L.; Menck, H.R. The National Cancer Data Base report on the relationship of race and national origin to the histology of nasopharyngeal carcinoma. Cancer 1998, 83, 582–588. [Google Scholar] [CrossRef]
- Carioli, G.; Negri, E.; Kawakita, D.; Garavello, W.; La Vecchia, C.; Malvezzi, M. Global trends in nasopharyngeal cancer mortality since 1970 and predictions for 2020: Focus on low-risk areas. Int. J. Cancer 2017, 140, 2256–2264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Lilly-Tariah, O.B.; Somefun, A.O. Malignant tumours of the nasopharynx at Jos University Teaching Hospital, Nigeria. Niger. Postgrad. Med. J. 2003, 10, 99–102. [Google Scholar] [PubMed]
- Sharma, T.D.; Singh, T.T.; Laishram, R.S.; Sharma, L.D.C.; Sunita, A.K.; Imchen, L.T. Nasopharyngeal carcinoma—A clinico-pathological study in a regional cancer centre of northeastern India. Asian Pac. J. Cancer Prev. 2011, 12, 1583–1587. [Google Scholar]
- Wei, W.I.; Sham, J.S.T. Nasopharyngeal carcinoma. Lancet 2005, 365, 2041–2054. [Google Scholar] [CrossRef]
- Abdulamir, A.S.; Hafidh, R.R.; Abdulmuhaimen, N.; Abubakar, F.; Abbas, K.A. The distinctive profile of risk factors of nasopharyngeal carcinoma in comparison with other head and neck cancer types. BMC Public Health 2008, 8, 400. [Google Scholar] [CrossRef]
- Ji, X.; Zhang, W.; Xie, C.; Wang, B.; Zhang, G.; Zhou, F. Nasopharyngeal carcinoma risk by histologic type in central China: impact of smoking, alcohol and family history. Int. J. Cancer 2011, 129, 724–732. [Google Scholar] [CrossRef]
- Yu, K.J.; Gao, X.; Chen, C.J.; Yang, X.R.; Diehl, S.R.; Goldstein, A.; Hsu, W.L.; Liang, X.S.; Marti, D.; Liu, M.Y.; et al. Association of human leukocyte antigens with nasopharyngeal carcinoma in high-risk multiplex families in Taiwan. Hum. Immunol. 2009, 70, 910–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hildesheim, A.; Wang, C.P. Genetic predisposition factors and nasopharyngeal carcinoma risk: a review of epidemiological association studies, 2000–2011: Rosetta Stone for NPC: Genetics, viral infection and other environmental factors. Semin. Cancer Biol. 2012, 22, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, R.W.; Imrey, P.B.; Lye, M.S.; Armstrong, M.J.; Yu, M.C.; Sani, S. Nasopharyngeal carcinoma in Malaysian Chinese: Salted fish and other dietary exposures. Int. J. Cancer 1998, 77, 228–235. [Google Scholar] [CrossRef]
- Ward, M.H.; Pan, W.H.; Cheng, Y.J.; Li, F.H.; Brinton, L.A.; Chen, C.J.; Hsu, M.M.; Chen, I.H.; Levine, P.H.; Yang, C.S.; et al. Dietary exposure to nitrite and nitrosamines and risk of nasopharyngeal carcinoma in Taiwan. Int. J. Cancer 2000, 86, 603–609. [Google Scholar] [CrossRef]
- Fang, W.; Zhang, J.; Hong, S.; Zhan, J.; Chen, N.; Qin, T.; Tang, Y.; Zhang, Y.; Kang, S.; Zhou, T.; et al. EBV-driven LMP1 and IFN-γ up-regulate PD-L1 in nasopharyngeal carcinoma: Implications for oncotargeted therapy. Oncotarget 2014, 5, 12189–12202. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, P.; Lee, A.; Marguet, S.; Leclercq, J.; Ng, W.T.; Ma, J.; Chan, A.T.C.; Huang, P.Y.; Benhamou, E.; Zhu, G.; et al. Chemotherapy and radiotherapy in nasopharyngeal carcinoma: An update of the MAC-NPC meta-analysis. Lancet. Oncol. 2015, 16, 645–655. [Google Scholar] [CrossRef]
- Yan, M.; Kumachev, A.; Siu, L.L.; Chan, K.K.W. Chemoradiotherapy regimens for locoregionally advanced nasopharyngeal carcinoma: A Bayesian network meta-analysis. Eur. J. Cancer 2015, 51, 1570–1579. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Li, W.F.; Chen, N.Y.; Zhang, N.; Hu, G.Q.; Xie, F.Y.; Sun, Y.; Chen, X.Z.; Li, J.G.; Zhu, X.D.; et al. Induction chemotherapy plus concurrent chemoradiotherapy versus concurrent chemoradiotherapy alone in locoregionally advanced nasopharyngeal carcinoma: A phase 3, multicentre, randomised controlled trial. Lancet. Oncol. 2016, 17, 1509–1520. [Google Scholar] [CrossRef]
- Chua, M.L.K.; Wee, J.T.S.; Hui, E.P.; Chan, A.T.C. Nasopharyngeal carcinoma. Lancet 2016, 387, 1012–1024. [Google Scholar] [CrossRef]
- Gupta, T.; Kannan, S.; Ghosh-Laskar, S.; Agarwal, J.P. Systematic review and meta-analyses of intensity-modulated radiation therapy versus conventional two-dimensional and three-dimensional radiotherapy in curative-intent management of head and neck squamous cell carcinoma. PLoS ONE 2018, 13, e0200137. [Google Scholar] [CrossRef] [PubMed]
- Onal, C.; Ozyar, E. In regards to Sze et al.: Primary tumor volume of nasopharyngeal carcinoma: Prognostic significance for local control (Int. J. Radiat. Oncol. Biol. Phys 2004, 59, 21–27). Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 629. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Ho, H.C.; Lee, M.S.; Hsiao, S.H.; Hwang, J.H.; Hung, S.K.; Chou, P. Primary tumor volume of nasopharyngeal carcinoma: Significance for survival. Auris. Nasus. Larynx 2008, 35, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Lu, J.J.; Gu, Y.; Zhu, G.; Hu, C.; He, S. Prognostic impact of primary tumor volume in patients with nasopharyngeal carcinoma treated by definitive radiation therapy. Laryngoscope 2008, 118, 1206–1210. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Lin, C.Y.; Xie, S.H.; Chen, G.H.; Lu, Y.Q.; Ling, W.; Huang, Q.H.; Liu, Q.; Cao, S.M. Smoking can increase nasopharyngeal carcinoma risk by repeatedly reactivating Epstein-Barr Virus: An analysis of a prospective study in southern China. Cancer Med. 2019, 8, 2561–2571. [Google Scholar] [CrossRef]
- Wei, K.R.; Zheng, R.S.; Zhang, S.W.; Liang, Z.H.; Li, Z.M.; Chen, W.Q. Nasopharyngeal carcinoma incidence and mortality in China, 2013. Chin. J. Cancer 2017, 36, 90. [Google Scholar] [CrossRef]
- Wakai, K.; Seki, N.; Tamakoshi, A.; Kondo, T.; Nishino, Y.; Ito, Y.; Suzuki, K.; Ozasa, K.; Watanabe, Y.; Ohno, Y.; et al. Decrease in risk of lung cancer death in males after smoking cessation by age at quitting: Findings from the JACC study. Jpn. J. Cancer Res. 2001, 92, 821–828. [Google Scholar] [CrossRef]







© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kanno, M.; Narita, N.; Fujimoto, Y.; Wakisaka, N.; Yoshizaki, T.; Kodaira, T.; Makita, C.; Sato, Y.; Yamazaki, K.; Wakaoka, T.; et al. Third Epidemiological Analysis of Nasopharyngeal Carcinoma in the Central Region of Japan from 2006 to 2015. Cancers 2019, 11, 1180. https://doi.org/10.3390/cancers11081180
Kanno M, Narita N, Fujimoto Y, Wakisaka N, Yoshizaki T, Kodaira T, Makita C, Sato Y, Yamazaki K, Wakaoka T, et al. Third Epidemiological Analysis of Nasopharyngeal Carcinoma in the Central Region of Japan from 2006 to 2015. Cancers. 2019; 11(8):1180. https://doi.org/10.3390/cancers11081180
Chicago/Turabian StyleKanno, Masafumi, Norihiko Narita, Yasushi Fujimoto, Naohiro Wakisaka, Tomokazu Yoshizaki, Takeshi Kodaira, Chiyoko Makita, Yuichiro Sato, Keisuke Yamazaki, Takanori Wakaoka, and et al. 2019. "Third Epidemiological Analysis of Nasopharyngeal Carcinoma in the Central Region of Japan from 2006 to 2015" Cancers 11, no. 8: 1180. https://doi.org/10.3390/cancers11081180