Pilot Study of Circulating Tumor Cells in Early-Stage and Metastatic Uveal Melanoma

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Risk Stratification
2.3. Circulating Tumor Cell Analysis
2.4. Statistical Analysis
3. Results
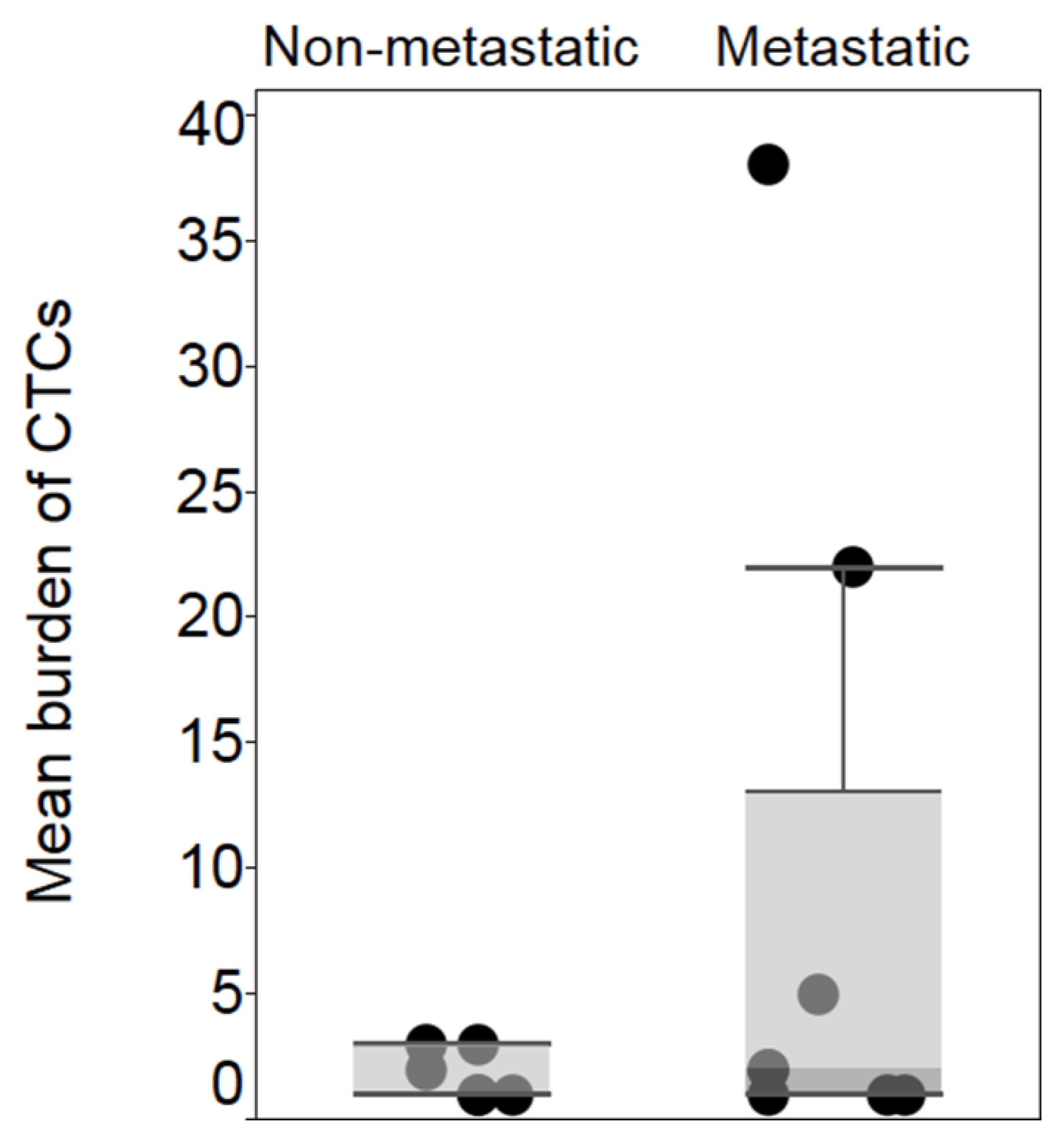
3.1. CTCs Are More Frequently Detected in Metastatic Uveal Melanoma Compared to Early-Stage Uveal Melanoma
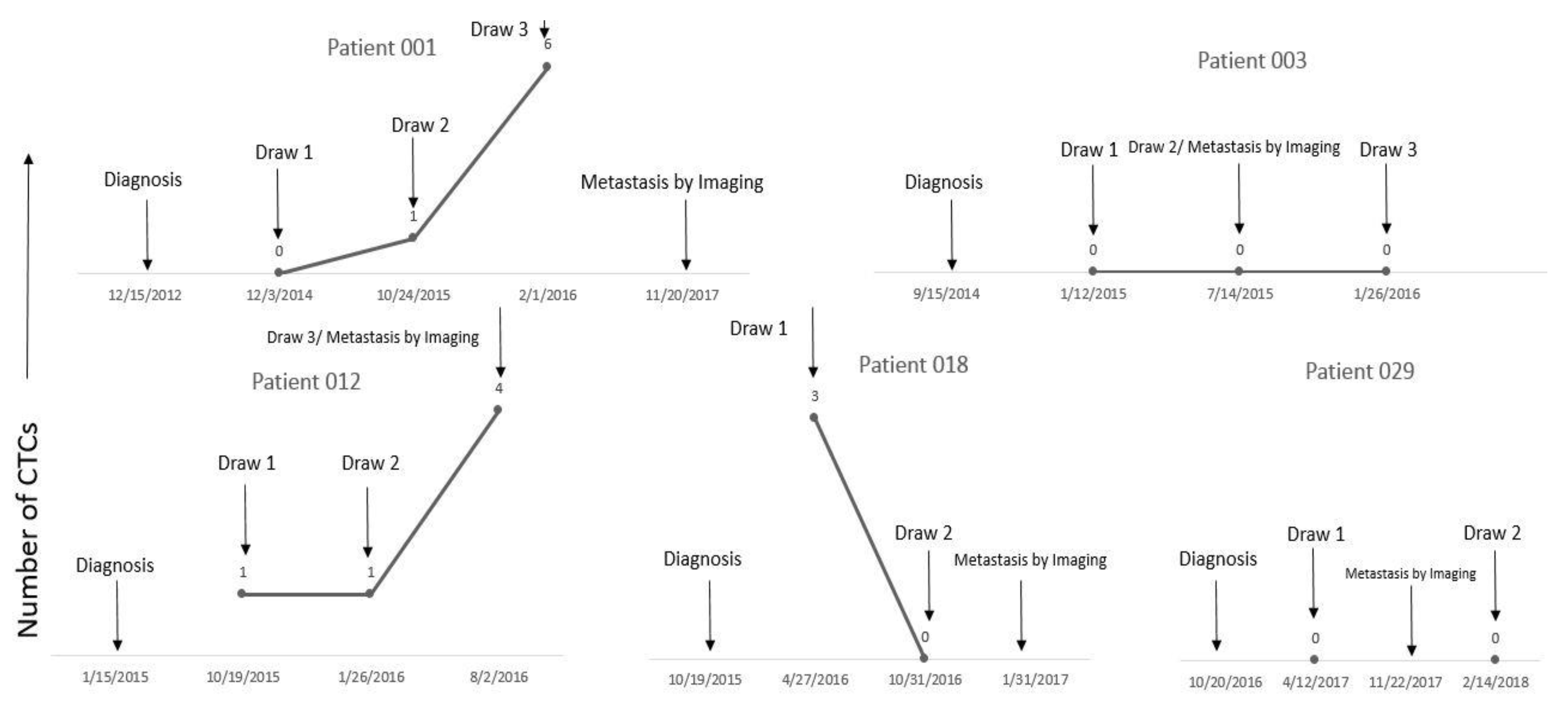
3.2. Presence of CTC Predicts Metastasis Risk in Early-Stage Uveal Melanoma
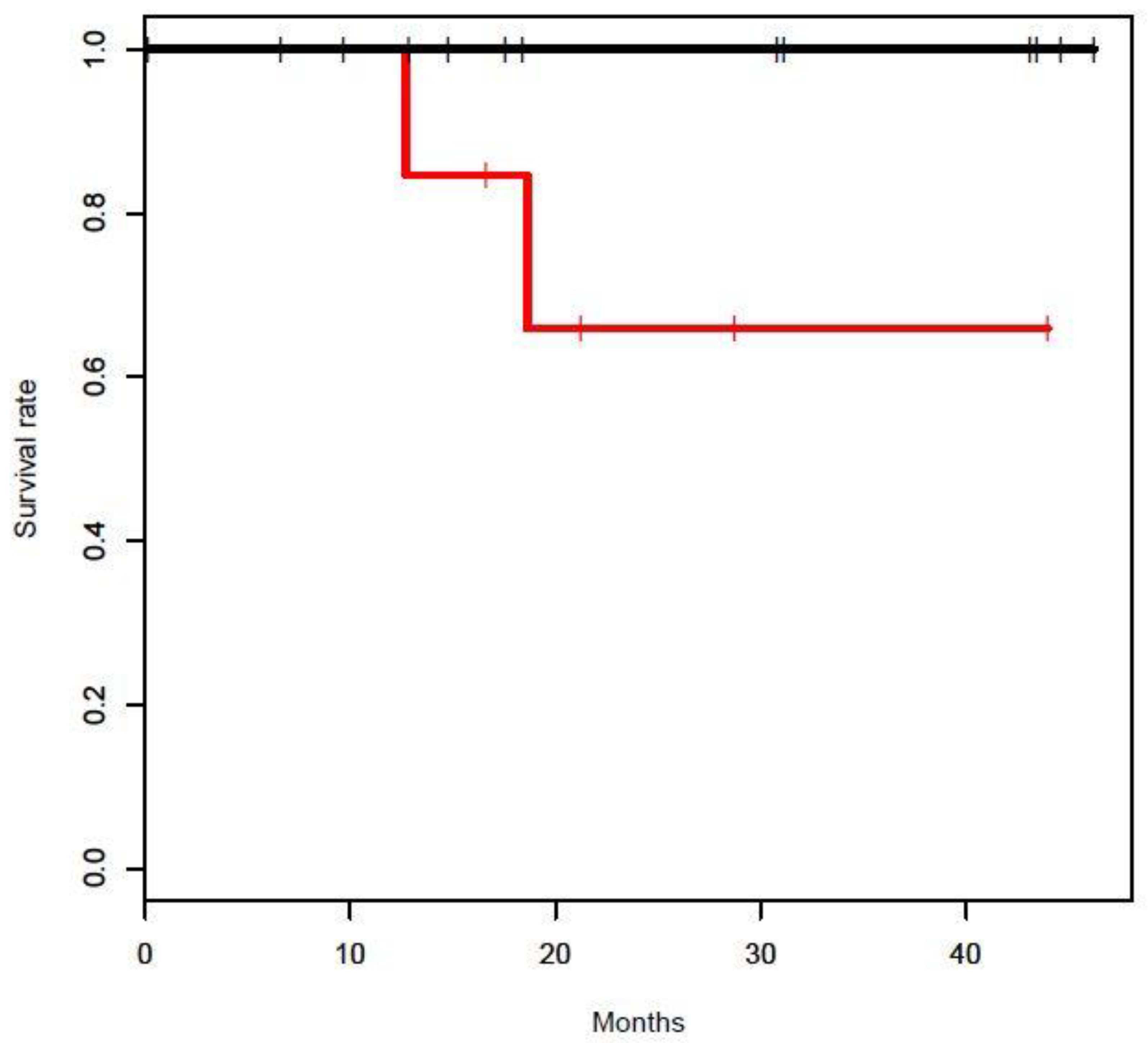
3.3. CTC Detection Is Risk Factor for Increased Mortality in Early-Stage Uveal Melanoma
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chang, A.E.; Karnell, L.H.; Menck, H.R. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: A summary of 84,836 cases from the past decade. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer 1998, 83, 1664–1678. [Google Scholar] [CrossRef]
- Shields, C.L.; Furuta, M.; Thangappan, A.; Nagori, S.; Mashayekhi, A.; Lally, D.R.; Kelly, C.C.; Rudich, D.S.; Nagori, A.V.; Wakade, O.A.; et al. Metastasis of uveal melanoma millimeter-by-millimeter in 8033 consecutive eyes. Arch. Ophthalmol. 2009, 127, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Turell, M.E.; Topham, A.K. Uveal melanoma: Trends in incidence, treatment, and survival. Ophthalmology 2011, 118, 1881–1885. [Google Scholar] [CrossRef] [PubMed]
- Andreoli, M.T.; Mieler, W.F.; Leiderman, Y.I. Epidemiological trends in uveal melanoma. Br. J. Ophthalmol. 2015, 99, 1550–1553. [Google Scholar] [CrossRef] [PubMed]
- Kaliki, S.; Shields, C.L. Uveal melanoma: Relatively rare but deadly cancer. Eye 2017, 31, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.K.; Bollin, K.B.; Patel, S.P. Obstacles to improving outcomes in the treatment of uveal melanoma. Cancer 2018, 124, 2693–2703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broggi, G.; Musumeci, G.; Puzzo, L.; Russo, A.; Reibaldi, M.; Ragusa, M.; Longo, A.; Caltabiano, R. Immunohistochemical Expression of ABCB5 as a Potential Prognostic Factor in Uveal Melanoma. Appl. Sci. 2019, 9, 1316. [Google Scholar] [CrossRef]
- Baccelli, I.; Schneeweiss, A.; Riethdorf, S.; Stenzinger, A.; Schillert, A.; Vogel, V.; Klein, C.; Saini, M.; Bauerle, T.; Wallwiener, M.; et al. Identification of a population of blood circulating tumor cells from breast cancer patients that initiates metastasis in a xenograft assay. Nat. Biotechnol. 2013, 31, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Alix-Panabieres, C.; Pantel, K. Clinical Applications of Circulating Tumor Cells and Circulating Tumor DNA as Liquid Biopsy. Cancer Discov. 2016, 6, 479–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suesskind, D.; Ulmer, A.; Schiebel, U.; Fierlbeck, G.; Spitzer, B.; Spitzer, M.S.; Bartz-Schmidt, K.U.; Grisanti, S. Circulating melanoma cells in peripheral blood of patients with uveal melanoma before and after different therapies and association with prognostic parameters: A pilot study. Acta Ophthalmol. 2011, 89, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Tura, A.; Luke, J.; Merz, H.; Reinsberg, M.; Luke, M.; Jager, M.J.; Grisanti, S. Identification of circulating melanoma cells in uveal melanoma patients by dual-marker immunoenrichment. Invest. Ophthalmol. Vis. Sci. 2014, 55, 4395–4404. [Google Scholar] [CrossRef] [PubMed]
- Beasley, A.; Isaacs, T.; Khattak, M.A.; Freeman, J.B.; Allcock, R.; Chen, F.K.; Pereira, M.R.; Yau, K.; Bentel, J.; Vermeulen, T. Clinical Application of Circulating Tumor Cells and Circulating Tumor DNA in Uveal Melanoma. JCO Precis. Oncol. 2018, 2, 1–12. [Google Scholar] [CrossRef]
- Schuster, R.; Bechrakis, N.E.; Stroux, A.; Busse, A.; Schmittel, A.; Scheibenbogen, C.; Thiel, E.; Foerster, M.H.; Keilholz, U. Circulating tumor cells as prognostic factor for distant metastases and survival in patients with primary uveal melanoma. Clin. Cancer Res. 2007, 13, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Plaks, V.; Koopman, C.D.; Werb, Z. Cancer. Circulating tumor cells. Science 2013, 341, 1186–1188. [Google Scholar] [CrossRef] [PubMed]
- Keilholz, U.; Goldin-Lang, P.; Bechrakis, N.E.; Max, N.; Letsch, A.; Schmittel, A.; Scheibenbogen, C.; Heufelder, K.; Eggermont, A.; Thiel, E. Quantitative detection of circulating tumor cells in cutaneous and ocular melanoma and quality assessment by real-time reverse transcriptase-polymerase chain reaction. Clin. Cancer Res. 2004, 10, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.C.; Madic, J.; Mariani, P.; Piperno-Neumann, S.; Rampanou, A.; Servois, V.; Cassoux, N.; Desjardins, L.; Milder, M.; Vaucher, I.; et al. Detection rate and prognostic value of circulating tumor cells and circulating tumor DNA in metastatic uveal melanoma. Int. J. Cancer 2014, 134, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Tura, A.; Merz, H.; Reinsberg, M.; Luke, M.; Jager, M.J.; Grisanti, S.; Luke, J. Analysis of monosomy-3 in immunomagnetically isolated circulating melanoma cells in uveal melanoma patients. Pigment. Cell Melanoma. Res. 2016, 29, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Navin, N.; Hicks, J. Future medical applications of single-cell sequencing in cancer. Genome Med. 2011, 3, 31. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total Patients (n) = 39 | |
|---|---|
| Sex | |
| Male (n) | 17 (44%) |
| Female (n) | 22 (56%) |
| Median age | 52 years (20–83 years) |
| Race | |
| Non-Hispanic White (n) | 39 (100%) |
| Disease status at study enrollment | |
| Early-stage disease (n) | 20 (51%) |
| Class 1 (n) | 2 |
| Class 2 (n) | 13 |
| Unknown (n) | 5 |
| Metastatic (n) | 19 (49%) |
| Mutation analysis (n) | 19 |
| GNAQ (n) | 12 (63%) |
| GNA11 (n) | 5 (27%) |
| Wildtype (n) | 1 (5%) |
| Other (n) | 1 (5%) |
| Median time between diagnosis and blood sampling | 20.35 months |
| Early-stage | 20.10 months |
| Metastatic | 24.65 months |
| Total Study follow up | 16.40 months |
| Early-stage | 16.84 months |
| Metastatic | 14.56 months |
| Early-Stage Uveal Melanoma (n) | 20 |
|---|---|
| No CTC detected (n) | 14 (70%) |
| CTC detected ≥ 1 (n) | 14 (70%) |
| 1 CTC | 3 |
| Class 1 | 1 |
| Class 2 | 2 |
| Unknown | 0 |
| 2 CTCs | 1 |
| Class 1 | 0 |
| Class 2 | 0 |
| Unknown | 1 |
| 3 CTCs | 2 |
| Class 1 | 0 |
| Class 2 | 1 |
| Unknown | 1 |
| Metastatic Uveal Melanoma (n) | 19 |
| No CTC detected (n) | 11 (58%) |
| CTC detected ≥ 1 (n) | 8 (42%) |
| 1 CTC | 3 |
| 2 CTCs | 2 |
| 5 CTCs | 1 |
| 22 CTCs | 1 |
| 38 CTCs | 1 |
| Patient | Class by Gene Expression | Mutational Analysis | Date of Diagnosis | Date of CTC Detection | Date of Metastasis by Imaging | Vital Status at Study Cutoff |
|---|---|---|---|---|---|---|
| Patient 001 | Class 2 | GNA11 | 12/15/2012 | 12/3/2014 | 11/20/2017 | Alive |
| Patient 003 | Class 2 | GNAQ | 9/15/2014 | CTC never detected | 7/14/2015 | Alive |
| Patient 012 | Class 2 | GNAQ | 1/15/2015 | 10/19/2015 | 8/2/2016 | Deceased |
| Patient 018 | Unknown * | wild-type | 10/19/2015 | 4/27/2016 | 1/31/2017 | Deceased |
| Patient 029 | Class 2 | not tested | 10/20/2016 | CTC never detected | 11/22/2017 | Alive |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anand, K.; Roszik, J.; Gombos, D.; Upshaw, J.; Sarli, V.; Meas, S.; Lucci, A.; Hall, C.; Patel, S. Pilot Study of Circulating Tumor Cells in Early-Stage and Metastatic Uveal Melanoma. Cancers 2019, 11, 856. https://doi.org/10.3390/cancers11060856
Anand K, Roszik J, Gombos D, Upshaw J, Sarli V, Meas S, Lucci A, Hall C, Patel S. Pilot Study of Circulating Tumor Cells in Early-Stage and Metastatic Uveal Melanoma. Cancers. 2019; 11(6):856. https://doi.org/10.3390/cancers11060856
Chicago/Turabian StyleAnand, Kartik, Jason Roszik, Dan Gombos, Joshua Upshaw, Vanessa Sarli, Salyna Meas, Anthony Lucci, Carolyn Hall, and Sapna Patel. 2019. "Pilot Study of Circulating Tumor Cells in Early-Stage and Metastatic Uveal Melanoma" Cancers 11, no. 6: 856. https://doi.org/10.3390/cancers11060856