Effect of Early Management on Pain and Depression in Patients with Pancreatobiliary Cancer: A Randomized Clinical Trial

 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Patients
2.3. Intervention
2.4. Usual Oncology Care
2.5. Patient-Reported Measures
2.6. Statistical Analyses
3. Results
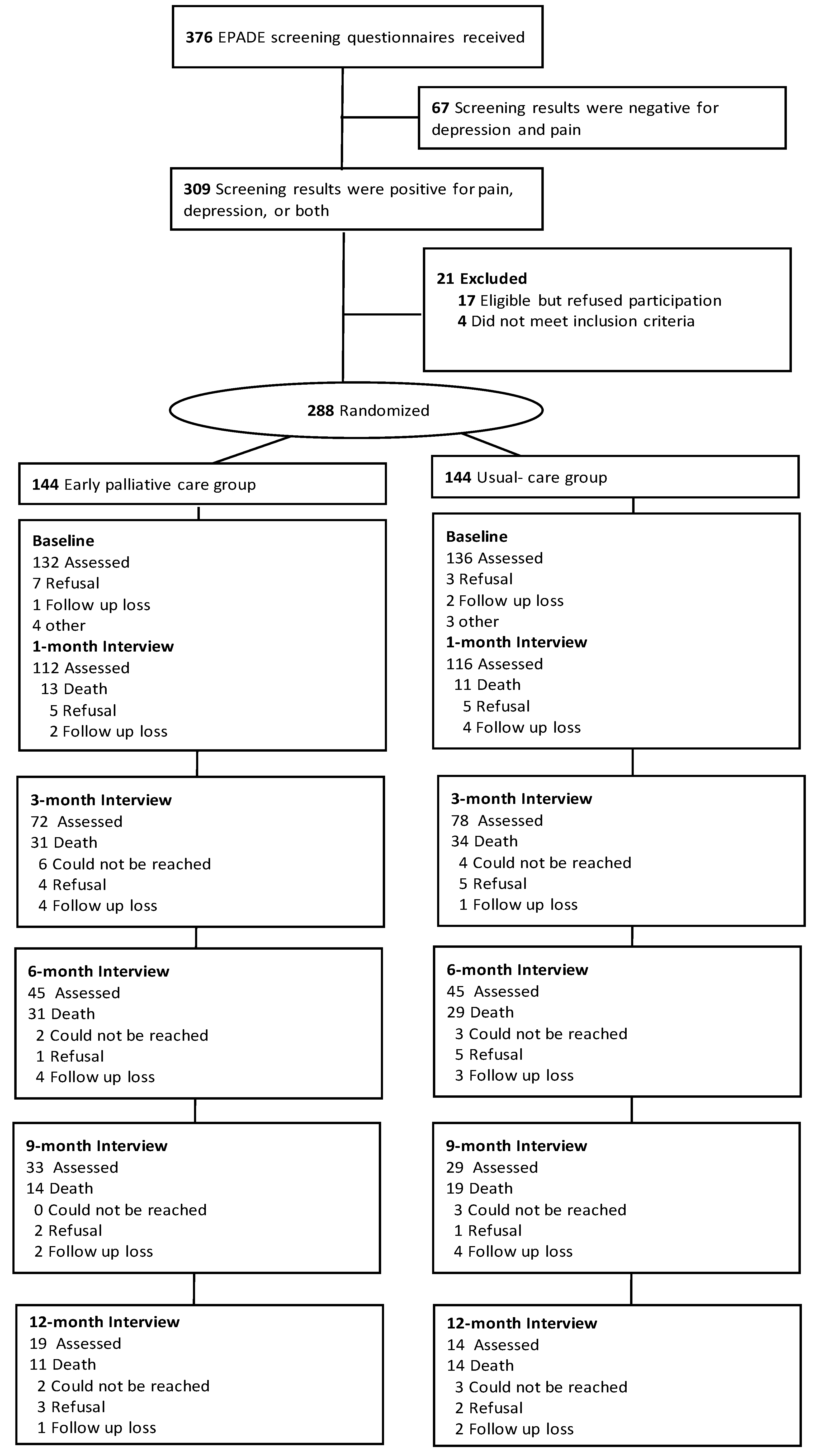
3.1. Participant Enrollment and Baseline Characteristics
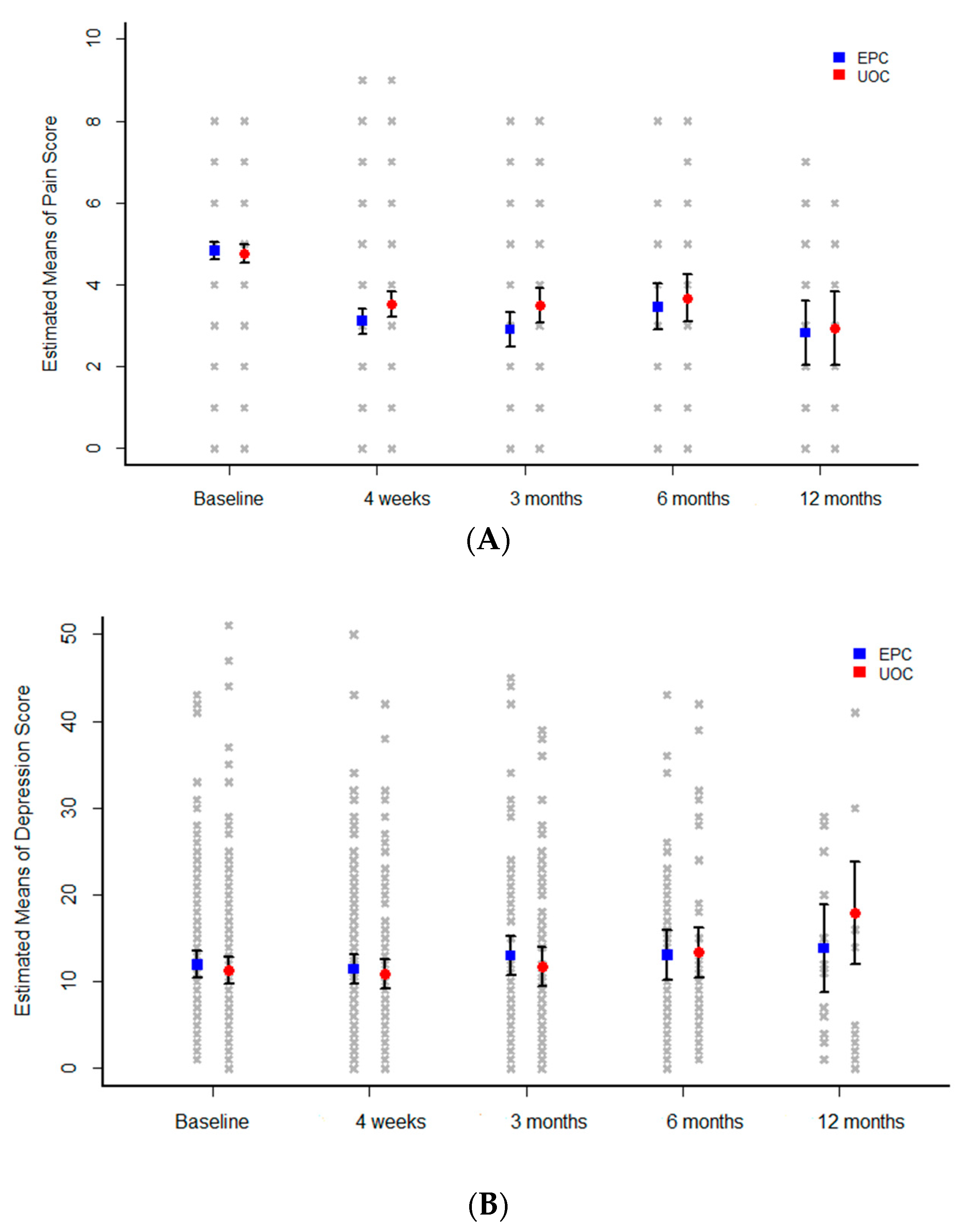
3.2. Pain and Depression-specific Outcomes
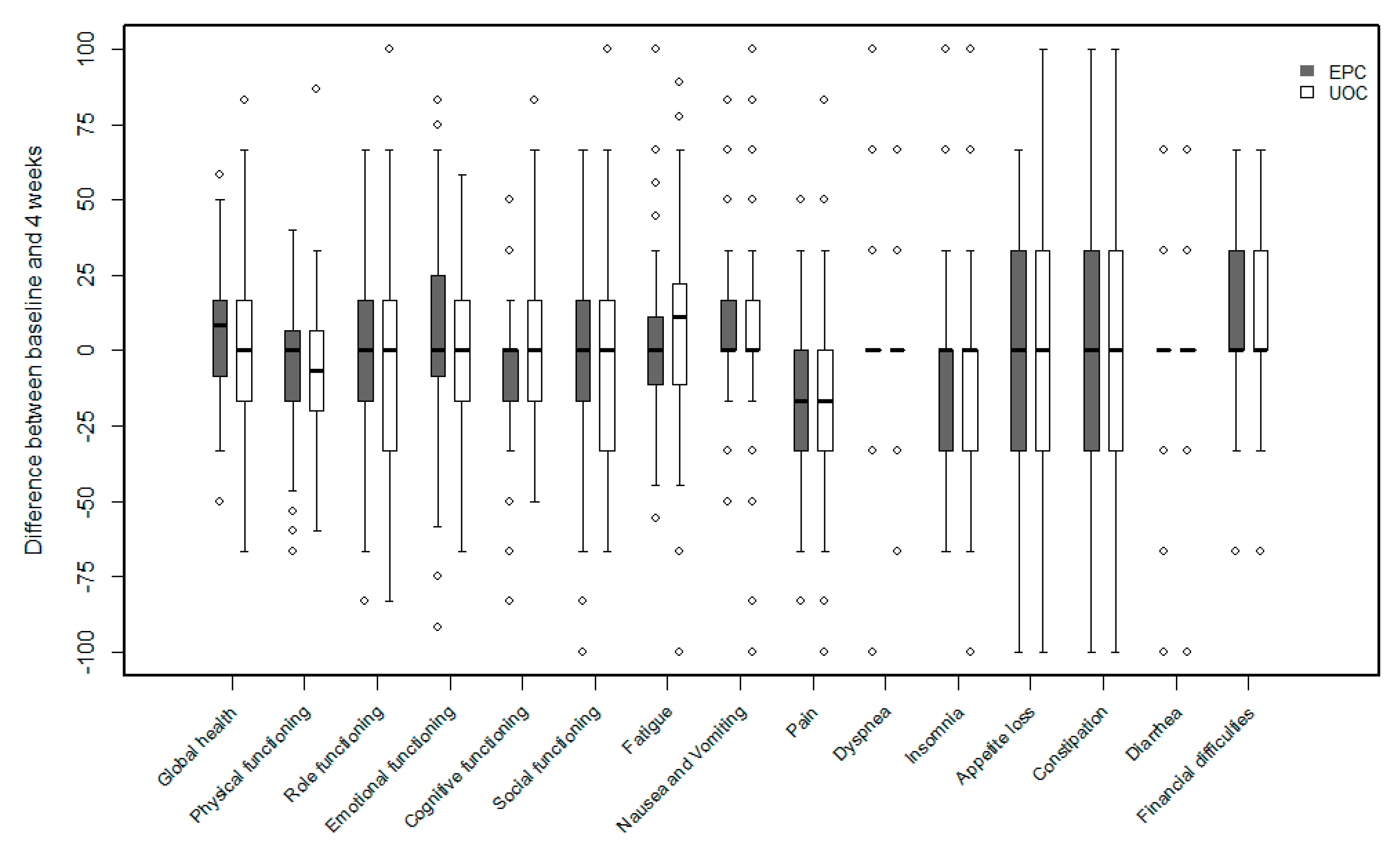
3.3. Health-Related Quality of Life and Cointerventions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Smyth, E.N.; Bapat, B.; Ball, D.E.; Andre, T.; Kaye, J.A. Metastatic pancreatic adenocarcinoma treatment patterns, health care resource use, and outcomes in France and the United Kingdom between 2009 and 2012: A retrospectivesStudy. Clin. Ther. 2015, 37, 1301–1316. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, T.; Hiraoka, T.; Kanemitsu, K.; Takamori, H.; Tanabe, D.; Tashiro, S. Lymphatic spreading pattern of intrahepatic cholangiocarcinoma. Surgery 2001, 129, 401–407. [Google Scholar] [CrossRef]
- American Academy of Hospice and Palliative Medicine; Center to Advance Palliative Care; Hospice and Palliative Nurses Association; Last Acts Partnership; National Hospice and Palliative Care Organization. National Consensus Project for Quality Palliative Care: Clinical Practice Guidelines for quality palliative care, executive summary. J. Palliat. Med. 2004, 7, 611–627. [Google Scholar] [CrossRef] [PubMed]
- Temel, J.S.; Greer, J.A.; Muzikansky, A.; Gallagher, E.R.; Admane, S.; Jackson, V.A.; Dahlin, C.M.; Blinderman, C.D.; Jacobsen, J.; Pirl, W.F.; et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N. Engl. J. Med. 2010, 363, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Temel, J.S.; Greer, J.A.; El-Jawahri, A.; Pirl, W.F.; Park, E.R.; Jackson, V.A.; Back, A.L.; Kamdar, M.; Jacobsen, J.; Chittenden, E.H.; et al. Effects of early integrated palliative care in patients with lung and gastrointestinal cancer: A randomized clinical trial. J. Clin. Oncol. 2017, 35, 834–841. [Google Scholar] [CrossRef]
- Janjan, N. Improving cancer pain control with NCCN guideline-based analgesic administration: A patient-centered outcome. J. Natl. Compr. Cancer Netw. 2014, 12, 1243–1249. [Google Scholar] [CrossRef]
- Koulouris, A.I.; Banim, P.; Hart, A.R. Pain in patients with pancreatic cancer: Prevalence, mechanisms, management and future developments. Dig. Dis. Sci. 2017, 62, 861–870. [Google Scholar] [CrossRef]
- Wong, G.Y.; Schroeder, D.R.; Carns, P.E.; Wilson, J.L.; Martin, D.P.; Kinney, M.O.; Mantilla, C.B.; Warner, D.O. Effect of neurolytic celiac plexus block on pain relief, quality of life, and survival in patients with unresectable pancreatic cancer: A randomized controlled trial. JAMA 2004, 291, 1092–1099. [Google Scholar] [CrossRef]
- Nagorney, D.M.; Donohue, J.H.; Farnell, M.B.; Schleck, C.D.; Ilstrup, D.M. Outcomes after curative resections of cholangiocarcinoma. Arch. Surg. 1993, 128, 871–877. [Google Scholar] [CrossRef]
- Hartung, T.J.; Brahler, E.; Faller, H.; Harter, M.; Hinz, A.; Johansen, C.; Keller, M.; Koch, U.; Schulz, H.; Weis, J.; et al. The risk of being depressed is significantly higher in cancer patients than in the general population: Prevalence and severity of depressive symptoms across major cancer types. Eur. J. Cancer 2017, 72, 46–53. [Google Scholar] [CrossRef]
- Ahn, E.; Shin, D.W.; Cho, S.I.; Park, S.; Won, Y.J.; Yun, Y.H. Suicide rates and risk factors among Korean cancer patients, 1993-2005. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2097–2105. [Google Scholar] [CrossRef] [PubMed]
- Gaertner, J.; Siemens, W.; Meerpohl, J.J.; Antes, G.; Meffert, C.; Xander, C.; Stock, S.; Mueller, D.; Schwarzer, G.; Becker, G. Effect of specialist palliative care services on quality of life in adults with advanced incurable illness in hospital, hospice, or community settings: Systematic review and meta-analysis. BMJ 2017, 357, j2925. [Google Scholar] [CrossRef] [PubMed]
- Quill, T.E.; Abernethy, A.P. Generalist plus specialist palliative care--creating a more sustainable model. N. Engl. J. Med. 2013, 368, 1173–1175. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, C.; Swami, N.; Krzyzanowska, M.; Hannon, B.; Leighl, N.; Oza, A.; Moore, M.; Rydall, A.; Rodin, G.; Tannock, I.; et al. Early palliative care for patients with advanced cancer: A cluster-randomised controlled trial. Lancet 2014, 383, 1721–1730. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Belanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Thinh, D.H.Q.; Sriraj, W.; Mansor, M.; Tan, K.H.; Irawan, C.; Kurnianda, J.; Nguyen, Y.P.; Ong-Cornel, A.; Hadjiat, Y.; Moon, H.; et al. Patient and Physician Satisfaction with Analgesic Treatment: Findings from the Analgesic Treatment for Cancer Pain in Southeast Asia (ACE) Study. Pain Res Manag. 2018, 2018, 2193710. [Google Scholar] [CrossRef] [PubMed]
- Nadstawek, J.; Leyendecker, P.; Hopp, M.; Ruckes, C.; Wirz, S.; Fleischer, W.; Reimer, K. Patient assessment of a novel therapeutic approach for the treatment of severe, chronic pain. Int. J. Clin. Pract. 2008, 62, 1159–1167. [Google Scholar] [CrossRef] [Green Version]
- Busner, J.; Targum, S.D. The clinical global impressions scale: Applying a research tool in clinical practice. Psychiatry (Edgmont) 2007, 4, 28–37. [Google Scholar]
- Lewinsohn, P.M.; Seeley, J.R.; Roberts, R.E.; Allen, N.B. Center for Epidemiologic Studies Depression Scale (CES-D) as a screening instrument for depression among community-residing older adults. Psychol. Aging 1997, 12, 277–287. [Google Scholar] [CrossRef]
- Jaeschke, R.; Singer, J.; Guyatt, G.H. Measurement of health status. ascertaining the minimal clinically important difference. Control Clin. Trials 1989, 10, 407–415. [Google Scholar] [CrossRef]
- Maltoni, M.; Scarpi, E.; Dall’Agata, M.; Zagonel, V.; Berte, R.; Ferrari, D.; Broglia, C.M.; Bortolussi, R.; Trentin, L.; Valgiusti, M.; et al. Systematic versus on-demand early palliative care: Results from a multicentre, randomised clinical trial. Eur. J. Cancer 2016, 65, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Drewes, A.M.; Campbell, C.M.; Ceyhan, G.O.; Delhaye, M.; Garg, P.K.; van Goor, H.; Laquente, B.; Morlion, B.; Olesen, S.S.; Singh, V.K.; et al. Pain in pancreatic ductal adenocarcinoma: A multidisciplinary, international guideline for optimized management. Pancreatology 2018, 18, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Mullady, D.K.; Yadav, D.; Amann, S.T.; O’Connell, M.R.; Barmada, M.M.; Elta, G.H.; Scheiman, J.M.; Wamsteker, E.J.; Chey, W.D.; Korneffel, M.L.; et al. Type of pain, pain-associated complications, quality of life, disability and resource utilisation in chronic pancreatitis: A prospective cohort study. Gut 2011, 60, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.L.; Loscalzo, M.; Trask, P.C.; Zabora, J.; Philip, E.J. Psychological distress in patients with pancreatic cancer—An understudied group. Psychooncology 2010, 19, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Peirce-Sandner, S.; Baron, R.; Bellamy, N.; Burke, L.B.; Chappell, A.; Chartier, K.; Cleeland, C.S.; Costello, A.; et al. Research design considerations for confirmatory chronic pain clinical trials: IMMPACT recommendations. Pain 2010, 149, 177–193. [Google Scholar] [CrossRef]
- Rodin, G.; Lo, C.; Rydall, A.; Shnall, J.; Malfitano, C.; Chiu, A.; Panday, T.; Watt, S.; An, E.; Nissim, R.; et al. Managing Cancer and Living Meaningfully (CALM): A randomized controlled trial of a psychological intervention for patients with advanced cancer. J. Clin. Oncol. 2018, 36, 2422–2432. [Google Scholar] [CrossRef]
- Gohil, V.B.; Klapman, J.B. Endoscopic palliation of pancreatic cancer. Curr. Treat. Opt. Gastroenterol. 2017, 15, 333–348. [Google Scholar] [CrossRef]
- Amr, Y.M.; Makharita, M.Y. Neurolytic sympathectomy in the management of cancer pain-time effect: A prospective, randomized multicenter study. J. Pain Symptom Manag. 2014, 48, 944–956. [Google Scholar] [CrossRef]
- Wyse, J.M.; Carone, M.; Paquin, S.C.; Usatii, M.; Sahai, A.V. Randomized, double-blind, controlled trial of early endoscopic ultrasound-guided celiac plexus neurolysis to prevent pain progression in patients with newly diagnosed, painful, inoperable pancreatic cancer. J. Clin. Oncol. 2011, 29, 3541–3546. [Google Scholar] [CrossRef]
- Oh, T.K.; Lee, W.J.; Woo, S.M.; Kim, N.W.; Yim, J.; Kim, D.H. Impact of celiac plexus neurolysis on survival in patients with unresectable pancreatic cancer: A retrospective, propensity score matching analysis. Pain Physician 2017, 20, E357–E365. [Google Scholar]
- Wyse, J.M.; Chen, Y.I.; Sahai, A.V. Celiac plexus neurolysis in the management of unresectable pancreatic cancer: When and how? World J. Gastroenterol. 2014, 20, 2186–2192. [Google Scholar] [CrossRef] [PubMed]
- Rabow, M.W.; Petzel, M.Q.B.; Adkins, S.H. Symptom management and palliative care in pancreatic cancer. Cancer J. 2017, 23, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Ferrell, B.R.; Temel, J.S.; Temin, S.; Alesi, E.R.; Balboni, T.A.; Basch, E.M.; Firn, J.I.; Paice, J.A.; Peppercorn, J.M.; Phillips, T.; et al. Integration of palliative care into standard oncology care: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 96–112. [Google Scholar] [CrossRef] [PubMed]
- Hutt, E.; Da Silva, A.; Bogart, E.; Le Lay-Diomande, S.; Pannier, D.; Delaine-Clisant, S.; Le Deley, M.C.; Adenis, A. Impact of early palliative care on overall survival of patients with metastatic upper gastrointestinal cancers treated with first-line chemotherapy: A randomised phase III trial. BMJ Open 2018, 8, e015904. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | EPC (n = 144) | UOC (n = 144) | p-Value |
|---|---|---|---|
| Age, year | 66.00 (40.00–86.00) | 67.00 (42.00–89.00) | 0.6954 |
| Male | 64 (44.44) | 65 (45.14) | 0.9057 |
| Primary tumor site | 0.9738 | ||
| Pancreatic cancer | 110 (76.39) | 109 (6.22) | |
| Biliary cancer | 34 (23.61) | 34 (23.78) | |
| Metastasis | 0.8396 | ||
| No | 17 (11.81) | 18 (12.59) | |
| Yes | 127 (88.19) | 125 (87.41) | |
| Symptom type | 0.9902 | ||
| Pain only | 105 (72.92) | 106 (73.61) | |
| Depression only | 5 (3.47) | 5 (3.47) | |
| Pain and depression | 34 (23.61) | 33 (22.92) | |
| Kamofsky performance rating scales | 70.00 (50.00–90.00) | 70.00 (50.00–100.00) | 0.8566 |
| Pain score | 4.00 (0.00–9.00) | 4.00 (0.00–8.00) | 0.8035 |
| Depression score | 9.00 (1.00–43.00) | 8.00 (0.00–51.00) | 0.2089 |
| Variables | ITT Set (N = 288) | Modified ITT Set (N = 277) | ||||
|---|---|---|---|---|---|---|
| EPC | UOC | p-Value | EPC | UOC | p-Value | |
| Pain | 0.4194 | 0.4616 | ||||
| <50% | 98 (70.50) | 104 (74.82) | 94 (69.63) | 98 (73.68) | ||
| ≥50% | 41 (29.50) | 35 (25.18) | 41 (30.37) | 35 (26.32) | ||
| Depression | 0.5732 | 0.5691 | ||||
| <50% | 27 (69.23) | 24 (63.16) | 26 (68.42) | 23 (62.16) | ||
| ≥50% | 12 (30.77) | 14 (36.84) | 12 (31.58) | 14 (37.84) | ||
| Variables | ITT set (n = 288) | Modified ITT set (n = 277) | ||||
|---|---|---|---|---|---|---|
| EPC | UOC | p-Value | EPC | UOC | p-Value | |
| Pain | 0.0404 | 0.0364 | ||||
| <3 score | 68 (48.92) | 85 (61.15) | 64 (47.41) | 80 (60.15) | ||
| ≥3 score | 71 (51.08) | 54 (38.85) | 71 (52.59) | 53 (39.85) | ||
| Depression | 0.9234 | 0.9206 | ||||
| <15 score | 23 (58.97) | 22 (57.89) | 22 (57.89) | 21 (56.76) | ||
| ≥15 score | 16 (41.03) | 16 (42.11) | 16 (42.11) | 16 (43.24) | ||
| Variables | Baseline | 1 Month | p-Value † | Diff | p-Value ‡ |
|---|---|---|---|---|---|
| Assessment of pain intensity | 0.0318 | ||||
| EPC | 4.00 (0.00–9.00) | 3.00 (0.00–8.00) | <0.0001 | −1.50 (−6.00–4.00) | |
| UOC | 4.00 (0.00–8.00) | 4.00 (0.00–9.00) | <0.0001 | −1.00 (−6.00–3.00) | |
| Assessment of sleep disturbance | 0.3157 | ||||
| EPC | 7.50 (0.00–23.00) | 5.00 (0.00–27.00) | 0.0112 | −2.00 (−19.00–26.00) | |
| UOC | 6.00 (0.00–24.00) | 5.00 (0.00–23.00) | 0.1493 | −1.00 (−16.00–18.00) |
| Variables | EPC | UOC | p-Value |
|---|---|---|---|
| Satisfaction with pain control | 2.00 (1.00–4.00) | 2.00 (1.00–5.000) | 0.0260 |
| Investigator’s global assessment | 3.00 (1.00–5.00) | 3.00 (1.00–5.00) | 0.0027 |
| Patient’s global assessment | 2.00 (1.00–5.00) | 3.00 (1.00–5.00) | 0.0005 |
| CGI-I | 3.00 (1.00–5.00) | 3.00 (1.00–5.00) | 0.0383 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woo, S.M.; Song, M.K.; Lee, M.; Joo, J.; Kim, D.H.; Kim, J.-H.; Han, S.-S.; Park, S.-J.; Kim, T.H.; Lee, W.J. Effect of Early Management on Pain and Depression in Patients with Pancreatobiliary Cancer: A Randomized Clinical Trial. Cancers 2019, 11, 79. https://doi.org/10.3390/cancers11010079
Woo SM, Song MK, Lee M, Joo J, Kim DH, Kim J-H, Han S-S, Park S-J, Kim TH, Lee WJ. Effect of Early Management on Pain and Depression in Patients with Pancreatobiliary Cancer: A Randomized Clinical Trial. Cancers. 2019; 11(1):79. https://doi.org/10.3390/cancers11010079
Chicago/Turabian StyleWoo, Sang Myung, Mi Kyung Song, Meeyoung Lee, Jungnam Joo, Dae Hyun Kim, Jong-Heun Kim, Sung-Sik Han, Sang-Jae Park, Tae Hyun Kim, and Woo Jin Lee. 2019. "Effect of Early Management on Pain and Depression in Patients with Pancreatobiliary Cancer: A Randomized Clinical Trial" Cancers 11, no. 1: 79. https://doi.org/10.3390/cancers11010079