Radiotherapy as a New Player in Immuno-Oncology

Department of Radiation Oncology, Rutgers Cancer Institute of New Jersey, 195 Little Albany St., New Brunswick, NJ 08901, USA
*
Author to whom correspondence should be addressed.
Cancers 2018, 10(12), 515; https://doi.org/10.3390/cancers10120515
Submission received: 7 November 2018
/
Revised: 10 December 2018
/
Accepted: 11 December 2018
/
Published: 14 December 2018
(This article belongs to the Special Issue New Developments in Radiotherapy)
Abstract
:Recent development in radiation biology has revealed potent immunogenic properties of radiotherapy in cancer treatments. However, antitumor immune effects of radiotherapy are limited by the concomitant induction of radiation-dependent immunosuppressive effects. In the growing era of immunotherapy, combining radiotherapy with immunomodulating agents has demonstrated enhancement of radiation-induced antitumor immune activation that correlated with improved treatment outcomes. Yet, how to optimally deliver combination therapy regarding dose-fractionation and timing of radiotherapy is largely unknown. Future prospective testing to fine-tune this promising combination of radiotherapy and immunotherapy is warranted.
Keywords:
radiotherapy; radiation; immunotherapy; combination therapy; cancer; dose-fractionation; timing1. Introduction
The notion that the sole driver of carcinogenesis lies upon genomic instability and oncogenic mutations has long been relinquished. It is well established that tumor immunology involving the three phases of immune response against cancer cells (the three “E”s—elimination, equilibrium, and escape) plays a major role in tumor formation. The immune system is the first line of defense against cells that have transformed and gone rogue via elimination. Cancer cells that have evaded the initial immune assault continue to evolve by Darwinian selection against pressure exerted by the immune system. Ultimately, the final phase of escape from immune surveillance allows the cancer cells to thrive unchecked in an immunosuppressive tumor microenvironment (TME). This has redefined our perception on combating malignancy, as the art of cancer therapy no longer just involves the surgical removal of tumor or destruction of cancer cells by means of radiotherapy and chemotherapy. Rather, a new area of focus is to reinvigorate the antitumor immunity of the host to resume its conquest against cancer cells through immunomodulatory therapies.
Radiotherapy is an essential treatment modality for many malignancies. Classically, radiation kills cancer cells through lethal DNA damage that leads to mitotic catastrophe or apoptosis. The four “R”s of classical radiobiology—reassortment, reoxygenation, repair, and repopulation—constituted the key elements for determining the success or failure of radiation treatment. However, recent advances in radiation biology have uncovered an intricate link between radiotherapy and the immune system. The coveted and previously mysterious abscopal effect, in which local tumor radiation triggers regression of a distant untreated lesion, is now attributed to radiation-induced systemic immune activation, a phenomenon that is underlain by the ability of radiation to elicit an immunogenic form of cell death. As such, Golden and Formenti perceptively postulated that the fifth “R” of radiobiology ought to be “tumor rejection” to highlight the immunological properties of radiotherapy [1]. However, radiotherapy by itself is rarely sufficient to overcome the immunosuppressing nature of tumor cells and the surrounding TME. In this booming era of immuno-oncology, a rational strategy is to utilize immunotherapy to bolster the immunogenic effects of radiotherapy, and vice versa.
In this review, we will discuss in detail the immunogenic mechanisms of radiation and its shortcomings as a stand-alone therapy. We will summarize the available preclinical and clinical evidence of synergy between radiation and various forms of immunotherapy. Furthermore, the importance of dose-fractionation and timing of radiotherapy will be highlighted. Finally, recent clinical trials evaluating the combination of radiation with immunotherapy will be elaborated, with an emphasis on optimizing dose and sequencing of radiotherapy in the combined setting.
2. Pro-Immunogenic Effects of Radiation
The ability of radiation to interact with the immune system was known long before we understood the how and the why. The notion that tumor response to radiation is partly dependent on the availability of T-cells was first demonstrated nearly 30 years ago [2]. Since then, evidence of increased tumor-infiltrating lymphocytes (TILs) after irradiation has been well reported and firmly established the causal relationship between radiotherapy and antitumor T-cell response [3,4,5,6,7,8], which is preceded by dendritic cell activation via tumor antigen presentation [9,10].
Several mechanisms of radiation-induced immunogenic cell death have been brought to light over the past decade. Irradiated cells can release certain danger-associated molecular patterns (DAMPs), such as high mobility group box 1 (HMGB1), heat-shock proteins, uric acid, and adenosine triphosphate (ATP). HMGB1, heat-shock proteins and uric acid can activate toll-like receptor signaling, which leads to dendritic cell maturation and priming of cytotoxic T lymphocytes (CTLs) [11,12,13], while ATP acts through cell surface purinergic receptors to attract macrophages and activate dendritic cells [14,15]. Radiation can also induce the translocation of calreticulin from the endoplasmic reticulum to the cell membrane. Exposure of calreticulin on the tumor cell surface serves as a phagocytotic signal for dendritic cells and macrophages, thereby enhancing the immunogenicity of cell death [16].
Aside from modulating extracellular signaling at the time of cell death to increase immunogenicity, radiation also triggers several phenotypic changes in tumor cells to facilitate immune detection and tumor eradication. Radiation induces expression of several cell surface death receptors that enhances susceptibility of tumor cell death in the presence of immune cells expressing the corresponding ligands. Upregulation of FAS receptor by radiation can be engaged by its specific ligand FAS-L to trigger extrinsic caspase-dependent apoptosis [17,18]. Similarly, radiation-induced death receptor 5 (DR5) sensitizes cancer cells to apoptosis via binding of tumor necrosis factor-related apoptosis-inducing ligand (TRAIL) [19,20,21]. Furthermore, co-stimulatory molecule CD80 and stress-induced NKG2D ligand are promoted by radiation to facilitate tumor cell clearance by T-cells and NK-cells [22,23,24].
Immune-cell infiltration into the TME is a crucial component of antitumor immune response. One mechanism in which tumor vasculature can prevent immune cell extravasation into the TME is through downregulation of adhesion molecules on endothelial cells such as E-selectin, intercellular adhesion molecule (ICAM)-1/2, and vascular cell adhesion molecule (VCAM)-1 [25]. Notably, radiation has been shown to increase the expression of E-selectin and ICAM-1 in human endothelial cells [26,27], thus modifying the tumor vasculature to allow more robust immune-cell infiltration.
Immune-cell permeability across the tumor vascular endothelium is required but not sufficient for infiltration. Cytokine and chemokine milieu in the TME play a crucial role in homing of the immune cells into the tumor. Chemokine CXCL16, as well as CXCL9 and CXCL10 through interferon-γ signaling, is induced by radiation to promote recruitment of CD4+ and CD8+ T-cells [6,28,29]. Radiation also upregulates the release of pro-inflammatory cytokines, including interleukin-1 beta (IL-1β), tumor necrosis factor alpha (TNF-α), and type I and type II interferons (IFNs) to activate antitumor effects of infiltrated immune cells [30,31,32,33].
Efficacy of immune-mediated tumor killing largely hinges on the ability of T-cells to recognize tumor cells as rogue entities. In other words, effective antitumor immunity cannot be realized without robust immune response against tumor-specific antigens, even if successful tumor infiltration of lymphocytes and reversal of immunosuppressive checkpoint regulation were achieved. Indeed, a common mechanism of immune evasion deployed by cancer cells is downregulation of major histocompatibility complex class I (MHC-I) molecules for self-antigen presentation, thereby shrouding their aberrant genetic and phenotypic makeup [34]. Radiotherapy can counteract tumor immune evasion via several means. Irradiated tumor cells upregulate MHC-I to increase tumor detection by host immune system [35,36,37]. Furthermore, radiation damage may enhance presentation of tumor neoantigens to allow for robust antitumor immune activation through a combination of direct tumor cell killing, increased tumor mutational load from radiation-induced genetic instability, and radiation-dependent upregulation of specific tumor antigen expression. Together, this phenomenon is also known as in situ vaccination, which is further enhanced by radiation-induced stimulation of the innate immune system [38,39,40]. Collectively, radiation exhibits pro-immunogenic influences in the irradiated tumor in various aspects of host immune response against malignancy, as depicted in Figure 1.
3. Immunosuppressive Effects of Radiation
Despite having multiple pro-immunogenic properties, radiation can also augment several immunosuppressive effects. The most direct consequence of such is the depletion of antitumor lymphocytes within the irradiated tumor. Lymphocytes are exquisitely sensitive to the cytotoxic effects of ionizing radiation, with LD50 and LD90 (lethal dose of reducing surviving fractions of lymphocytes to 50% and 90%, respectively) of 2 Gy and 3 Gy, respectively [41]. Moreover, with conventional radiotherapy of delivering daily low dose radiation (1.8–2 Gy) over several weeks, mathematical modeling predicted significant radiation exposure to the circulating lymphocytes over the course of treatment, consistent with treatment-related lymphopenia that is commonly seen in irradiated patients [42]. In various cancers, treatment-induced lymphopenia is correlated with poor clinical prognosis, although whether or not this was due to compromised antitumor immunity is unclear [43]. In addition, preclinical studies have revealed differential effects of radiation among lymphocytes, with CTLs being more radiosensitive than regulatory T-cells (Treg). As such, radiotherapy may selectively deplete CD8 effector T-cells and proportionally increase Treg cells, which confer suppressive function within the TME to facilitate tumor escape from immunosurveillance [44,45].
Radiation also induces several immunosuppressive phenotypic changes in the TME through cytokine regulation. Tissue abundance of transforming growth factor-beta (TGF-β), an anti-inflammatory cytokine that suppresses intratumoral immune response, is increased with radiation [46,47]. Irradiated tumors also favor accumulation of immunosuppressive M2-polarized macrophages within the TME, with one study reporting tumor release of chemokine SDF-1α as one underlying mechanism [48,49]. Another study demonstrated that radiation increases expression of colony-stimulating factor 1 (CSF1) [50], a cytokine responsible for shifting macrophages towards M2 polarization and boosting the abundance of Treg and myeloid-derived suppressor cells (MDSCs), representing yet another signaling pathway to maintain the suppressive nature of TME.
Programmed death-ligand 1 (PD-L1), an immune checkpoint ligand that transmits an inhibitory signal to attenuate immune cell proliferation and activation, is upregulated on tumor and immune cells in the TME after irradiation. While one may view this as yet another suppressive attribute of radiation, evidence suggest that modulation of the PD-L1/PD-1 axis in response to radiotherapy may serve as a biomarker for antitumor immune activation. Dovedi et al. demonstrated that IFN-γ produced by activated antitumor CD8 T-cells was responsible for PD-L1 induction on tumor cells, representing an adaptive mechanism for cancer to thwart host reactive immunity [51]. By the same token, radiation can increase PD-1 expression on T-cells and weakens antitumor immunity [52]. However, this immunosuppressive sequela is preceded by successful mounting of T-cell responses against cancer cells, and PD-1 blockade offsets this countermeasure deployed by the tumor [51,52]. Consistent with these findings, PD-1 expression on TILs in HPV-positive head and neck cancer is a favorable prognostic marker and denotes antitumor immune activation after chemoradiotherapy [53].
4. Immune-Mediated Systemic Effects of Radiotherapy
Although radiotherapy is a local treatment, it has long been known to induce systemic effects. Documentation of distant tumor regression after local radiation exists as early as the beginning of the 20th century [54], a phenomenon also known as the abscopal effect. In 2004, Demaria et al. first provided evidence of an immune mechanism underlying the abscopal effect [5], now widely accepted as the culmination of the positive immune-mediated effects of local tumor radiation that primed the host’s immune system to eradicate distant non-irradiated disease of the same origin. Many clinical case reports of radiation-induced abscopal effect have been published over the past decades and are well-summarized in this recent review [55].
Nevertheless, the occurrence of the abscopal effect is exceedingly rare with radiotherapy alone. Given that radiation has both pro-immunogenic and immunosuppressive properties, its overall effect is dictated by the balance between the two opposing forces. While pro-immunogenic effects of radiation presumably dominate over its suppressive effects, a critical threshold of antitumor immunity is generally not realized in the absence of additional immunomodulation. Budhu et al. reported that a specified threshold of antigen-specific CD8 T-cells is required for efficient tumor killing in melanoma cell model, likely underscoring a prevalent challenge of insufficient immune activation with radiotherapy alone [56]. Unequivocally, in this era of increasing use of cancer immunotherapy, reports of abscopal effect have become more common [57]. As a prime example, a case report recounted a patient with metastatic melanoma with progressive disease on ipilimumab, received palliative radiation for a symptomatic paraspinal mass, and showed systemic disease regression after receiving an additional dose of ipilimumab two months after radiotherapy [58]. Accordingly, the crucial role of radiation in effective combinatory cancer therapy is increasingly being recognized.
In preclinical models, immune-mediated radiation effects generated long-lasting antitumor immunity. The development of radiation-induced immune memory is characterized by prolonged host survival and failure of tumor growth after subsequent rechallenge of the same tumor. Adoptive transfer of T-cells from successfully treated mice with radiotherapy into tumor-bearing mice led to tumor regression and extended survival [59,60]. At present, whether radiation alone can elicit persistent immune memory in the clinical setting is unclear. However, in line with the mechanism underlying the abscopal effect, long-lasting antitumor immune memory stimulated by radiotherapy is likely to become more apparent with rising utilization of immunomodulatory agents.
5. Synergy of Radiotherapy and Immunotherapy Combination
Because of the shortcomings of radiotherapy alone as a double-edged sword—having both immunogenic and immunosuppressive effects in the TME—addition of immunotherapy is a good strategy to overcome the inadequacy of radiation to mount a robust antitumor immune response. Preclinical and clinical evidence have demonstrated improved outcomes of radiotherapy in the presence of various types of immunotherapy that modulates different facets of tumor immunity.
5.1. Toll-Like Receptor Agonists
Toll-like receptor (TLR) signaling is crucial for activating dendritic cells to cross-prime effector T-cells. TLR agonists function to improve the ability of dendritic cells to present tumor antigens released from radiation cell killing. TLR9, the most extensively studied member of the TLR family, binds to unmethylated cytosine-phosphate-guanosine (CpG) oligodeoxynucleotide from bacterial DNA to induce cellular and humoral immunity. In murine model, TLR9 agonist has been shown to enhance therapeutic effects of radiation by increasing tumor-infiltration of natural killer dendritic cells, which led to fewer metastases and longer survival [61]. Similarly, targeting TLR9 with CpG oligodeoxynucleotide improved tumor response to radiation in preclinical models [62,63,64,65]. In vivo studies also demonstrated therapeutic synergy through combining TLR7/8 activation and irradiation, with combination treatment resulting in inhibition of local tumor growth and metastatic progression [66,67,68,69,70].
Clinically, combination of TLR9 agonist and radiation has shown some success in treatment of lymphomas. In a phase I/II study, 15 patients with stage III-IV relapsing low-grade B-cell lymphoma were treated with intratumoral injection with CpG DNA PF-3512676 and concurrent 4 Gy radiation to a single lesion, resulting in clinical response in 4 patients and stable disease regression in two [71]. In a subsequent phase I/II trial, injection with PF-3512676 was used in mycosis fungoides with 33% response rate, with clinical responders showing greater reduction in Tregs [72]. There are two trials evaluating the combination of TLR7 agonist imiquimod and radiation, one for breast cancer with skin metastases (NCT01421017) and another for diffuse intrinsic pontine glioma (NCT01400672), both with pending results.
5.2. Cytokines
Cytokine signaling is the main mode of communication between immune cells to activate or suppress effector immune functions. Using pro-inflammatory cytokines to bolster effector cytotoxic T-cell functions can potentially overcome radiation-induced suppressive Treg accumulation. However, outcomes so far with combining cytokine therapy with radiation are modest at best.
Interleukin-2 (IL-2) is a cytokine that regulates differentiation and proliferation of T-cells into effector and memory cells when stimulated by antigens. Preclinical studies on combining IL-2 and radiation are lacking. However, building upon the evidence that radiation can augment pro-inflammatory and immunogenic changes, a phase I study of stereotactic body radiation therapy (SBRT) in conjunction with high-dose IL-2 was performed in metastatic melanoma or renal cell carcinoma. Of the 12 patients treated, 8 patients had clinically significant response, and immune monitoring revealed greater proliferation of CD4+ T-cells with effector memory phenotype [73].
IL-12 is another pro-inflammatory cytokine that activates NK cells and cytotoxic CD8+ T-cells, as well as signaling differentiation of naïve CD4+ cells to T-helper 1 cells that can mediate antitumor immune response. Preclinical evaluation of combining radiation with IL-12 therapy is limited. However, one study showed that intratumoral expression of IL-12 led to increased IFN-γ levels and radiosensitizing effects [74]. There are no existing clinical trials testing the efficacy of this combination therapy.
Interferon-α (IFN-α) has broad immunological activities that modulate tumor immunity, including activation of dendritic cells and promotion of survival and expansion of natural killer (NK) cells and cytotoxic T-cells. IFN-α increases radiosensitivity of tumor cells in early in vitro studies [75,76]. A phase II trial showed improved survival in patients with resected pancreatic adenocarcinoma receiving adjuvant combination of chemoradiation and IFN-α compared to those receiving chemoradiation alone [77]. However, IFN-α therapy is highly toxic, leading to premature closure of phase II ACOSOG Trial Z05031 due to grade ≥3 toxicity of 95% [78]. Most recent phase III trial utilizing IFN-α in adjuvant chemoradiation for pancreatic cancer resulted in significant treatment toxicity without improvement in survival [79].
Tumor necrosis factor-α (TNF-α) is a potent inflammatory cytokine that has tumoricidal properties. However, earlier use of systemic TNF-α with concomitant radiotherapy has caused significant immune-related adverse effects and low patient tolerability [80]. TNFerade, a form of gene therapy in which human TNF-α gene controlled by a radiation-inducible promoter is delivered into cancer cells via replication-deficient adenoviral vector, has since been tested with radiotherapy in phase I/II trials with improved toxicity profile [81,82,83,84,85]. These promising results led to a phase III multicenter randomized trial for locally advanced pancreatic cancer patients treated with concurrent fluorouracil and radiation with or without intratumoral TNFerade. Despite being safe and well-tolerated, the addition of TNFerade did not improve overall or progression-free survival in this patient cohort [86].
A novel approach to cytokine therapy is to conjugate cytokines to antibodies or antibody fragments that specifically target tumor-associated antigens. The resulting class of fusion proteins, also known as immunocytokines, is capable of delivering cytokines directly to the tumor sites and avoiding systemic adverse effects that often limit the use of cytokine therapies [87]. Several recent studies have investigated the use of IL-2 immunocytokines with radiotherapy. L19-IL2, an immunocytokine with L19 antibody targeting the EDB-domain of fibronectin that is frequently overexpressed in solid tumors, has been shown to synergize with radiation against C51 murine colon carcinoma in a CD8-dependent manner [88]. Subsequent study by the same group demonstrated abscopal response in the non-irradiated lesions after L19-IL2 and radiation treatment to the index lesions, as well as long-lasting antitumor immunity in cured mice [89]. These encouraging results led to a phase I clinical study of combining L19-IL2 and SBRT in oligometastatic solid tumors (NCT02086721) with pending results. There are also recent reports of success with combining NHS-IL12 immunocytokine that targets necrotic cells with radiotherapy in preclinical models. Eckert et al. first showed that radiation-induced tumor necrosis can enhance intratumoral accumulation of necrosis-targeting NHS-IL12 immunocytokine, followed by a functional study demonstrating abscopal effect and improved survival in humanized mouse model bearing rhabdomyosarcoma xenografts [90,91]. While immunocytokines with TNF-α conjugates are also been tested in preclinical and clinical studies, combination of those agents with radiotherapy has yet to be studied.
5.3. Co-Stimulatory Molecules
After successful priming of tumor antigen-specific T-cells from antigen-presenting dendritic cells, co-stimulatory signaling are required to activate these T-cells to eradicate cancer cells harboring the corresponding antigens. There are two families of ligand/receptor proteins involved in T-cell co-stimulation: (1) B7/CD28 family that includes CD80/CD86 (B7-1/B7-2) ligand binding to CD28 receptor and CD275 (B7-H2) binding to CD278 (ICOS) receptor; and (2) TNF/TNF receptor family that includes ligands (CD40L, OX40L, CD70, and 4-1BBL) and its respective receptors (CD40, OX40, CD27, and 4-1BB). Intriguingly, cancer cells can evolve to hinder these essential stimuli via inhibitory signaling of T-cells (to be further discussed below under Section 5.4).
Recent in vivo studies have shown promising results of combining CD40 stimulation and radiation. Using a pancreatic ductal adenocarcinoma mouse model, Rech et al. revealed synergy between radiation and an agonist αCD40 antibody through distinct mechanisms. Ablative dose of radiation triggers early inflammatory stimulus through upregulation of MHC class I and CD86, while αCD40 causes a late response of altering intratumoral and systemic immunosuppressive myeloid cells, collectively yielding abscopal effect and long-term tumor immunity [92]. In another study using pancreatic cancer models, single fraction of SBRT with agonist αCD40 led to regression of non-irradiated tumor and durable immune memory [93].
OX40 is a potent co-stimulatory molecule on activated T-cells, and OX40 signaling can promote effector T-cell survival and inhibit Treg function, which can be achieved via OX40 ligand binding or stimulation via antibody agonists. Combination of single dose of 20 Gy and intratumoral delivery of activating OX40 antibody in murine lung cancer model resulted in CD8 T-cell dependent tumor killing and tumor immunity [94]. Gough et al. corroborated this finding in murine 3LL-tumor model using high doses of radiation and αOX40 antibody to achieve extended survival and decreased tumor recurrence compared to single treatments alone [95]. Recently, a combination of radiation and OX40 agonist has demonstrated efficacy in anti-PD-1-resistent murine lung tumors to inhibit local and systemic tumor growth [96].
4-1BB, also known as CD137, is the first member of the TNFR family identified as a potential target for cancer immunotherapy. Ligation of 4-1BB receptor on activated T-cells with 4-1BBL or antibody agonist prompts anti-apoptotic signaling to prevent activation-induced cell death and reverse T-cell tolerance [97]. When combined with 4-1BB agonist, antitumor effect of radiation has been shown to be enhanced. Treatment with 4-1BB antibody agonist with radiation in murine lung (M109) and breast (EMT6) carcinoma models significantly delayed tumor progression [98]. With the addition of cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) blockade, the combination of 4-1BB activation and radiation further improved survival in GL261 murine glioma model, which is associated with greater infiltration of CD4+ and CD8+ lymphocytes [99]. Similarly, concomitant inhibition of PD-1 with radiation and 4-1BB agonist enhanced antitumor effect against human BRAF-mutant melanoma [100]. Interestingly, one study showed decreased off-target immune cell activation with 4-1BB aptamer compared to 4-1BB antibody when combined with radiation, while having similar therapeutic effect with both agents, suggesting potential differences in treatment toxicity of targeting the same receptor with varying forms of agonists [101].
To date, clinical experience with combining radiation with co-stimulatory molecules is limited. However, there are several ongoing clinical trials (discussed below, Section 7) that will shed light on the clinical utility of this therapeutic strategy.
5.4. Immune Checkpoint Inhibition
Immune checkpoints are regulatory mechanisms that serve to prevent over-stimulation of activated T-cells, which can lead to autoimmunity. CTLA-4 and PD-1, also members of the B7/CD28 family, are expressed on activated T-cells to act as an “off” switch when bound by ligands CD80/CD86 and PD-L1/PD-L2, respectively. Cancer cells often over-express PD-L1/PD-L2 to exploit the intrinsic mechanism of T-cell inhibition. Antibody antagonists against CTLA-4 and PD-1/PD-L1 attenuate tumor-induced inhibitory signaling, thereby shifting towards T-cell stimulation and bolstering adaptive tumor immunity. Moreover, as previously mentioned, radiotherapy can upregulate PD-1/PD-L1 on tumor and immune cells in the TME, and as such, combining checkpoint inhibition with radiation may nullify this undesired immunosuppressive sequela.
Demaria et al. first reported synergy of radiation and CTLA-4 blockade in a preclinical setting. Using the poorly immunogenic murine 4T1 mammary carcinoma model, this study showed that only combinatory treatment of radiation and CTLA-4 inhibition, but not either treatment alone, exhibited significant survival advantage over control. Furthermore, systemic antitumor immunity was provoked with combined treatment resulting in decreased lung metastases, which required the presence of CD8+ T-cells [102]. In a follow-up study by the same group, abscopal effect of combined radiation and CTLA-4 blockade was demonstrated using bilateral tumor models in which the unirradiated tumors displayed significant growth delay after irradiation of the primary tumors. This systemic effect is CD8-dependent and correlates with increased TILs and tumor-specific IFN-γ-producing T-cells in the unirradiated tumors [7].
The number of prospective clinical investigations assessing safety and efficacy of combined CTLA-4 inhibition and radiotherapy is on the rise. So far, only a few trials have reported results. In a phase I/II study, patients with metastatic castrate-resistant prostate cancer were treated with escalating doses of ipilimumab with or without radiotherapy. Maximum dose tested of 10 mg/kg ipilimumab with 8 Gy radiation to one to three bony metastases showed acceptable toxicity profile, with one-third of patients having stable disease or better [103]. Using the same ipilimumab and radiation dose, a phase III multicenter trial randomized 799 patients with metastatic prostate cancer to ipilimumab versus placebo after radiotherapy to osseous metastases. Although median overall survival of patients receiving ipilimumab only trended higher than those receiving placebo (11.2 vs. 10.0 months, p = 0.053), post-hoc subgroup analysis of patients with good prognostic features demonstrated significant survival benefit with ipilimumab (22.7 vs. 15.8 months, p = 0.0038) [104]. There are also several small prospective studies that reported abscopal responses and improved overall survival in metastatic melanoma patients treated with ipilimumab and radiation to brain and/or visceral metastases [105,106,107,108]. Of interest, a joint clinical and preclinical study in patients with metastatic melanoma implicated T-cell exhaustion from upregulation of tumor PD-L1 expression in the resistance towards treatment with radiation and CTLA-4 antibody. Treatment-induced increase in the PD-1/PD-L1 axis was reproduced in murine melanoma models, and the addition of PD-L1 blockade significantly improved response to radiation and CTLA-4 inhibition [109]. In addition, a recent clinical study shed light on plausible mechanisms underlying favorable responses to combination treatment with radiation and CTLA-4 blockade. A cohort of 39 patients with metastatic NSCLC were treated with radiotherapy to one metastasis with concurrent ipilimumab, with response rate of 18% and disease control in 31% of patients. Increase in IFN-β and T-cell receptor clonal dynamics predicted response to combination therapy, and further characterization of a single responder revealed expansion of two specific T-cell clones that target an immunogenic mutation on a radiation-induced gene, KPNA2. While this intriguing finding supports the hypothesis that radiotherapy can enhance neoantigen exposure to the host immune system, validation in an expanded cohort is warranted. Furthermore, the single-arm nature of this trial precludes the determination of the degree of contribution from either radiotherapy or ipilimumab in the observed immunological effects [110].
Several preclinical models have also revealed therapeutic synergy of radiation and PD-1/PD-L1 blockade. Treatment of radiation and anti-PD-1 antibody in mouse glioma model improved survival compared to either treatment modality alone. Combined treatment group exhibited increased tumor infiltration of cytotoxic T-cells and decreased Tregs, and glioma tumor cells rechallenged in treated mice failed to grow [111]. Deng et al. observed increase in PD-L1 expression in the TME after radiation, and the addition of PD-L1 inhibition augmented antitumor effect of radiation. Specifically, efficacy of combined treatment is dependent on CD8+ T-cells and correlated with reduction in the immunosuppressive MDSCs [8]. Similar findings were reported by Dovedi et al., which also revealed that upregulation of PD-L1 on tumor cells is induced by IFN-γ secretion from CD8+ T-cells [51]. Subsequent studies further demonstrated that PD-1 blockade enhanced antigen-specific and tumor-specific immunity triggered by radiation [112,113]. In a recent mechanistic study, the authors showed that both the preexisting resident T-cells and infiltrating lymphocytes after combination treatment contributed to tumor regression in in-field and out-of-field tumors [114]. While most studies examined the role of PD-1/PD-L1 axis inhibition in bolstering radiation efficacy, Wang et al. reported that radiotherapy can reverse tumor resistance towards anti-PD-1 therapy through induction of IFN-β and MHC-I expression on tumor cells [115]. Together, the above evidence underscored the importance of modulating the immune status within the TME to optimize efficacy of cancer therapy in the clinic.
Given that ample evidence lent support to the efficacy of combining PD-1/PD-L1 blockade with radiation, an abundant of clinical trials are now ongoing to investigate the utility of this combination in the clinical setting. Several phase I/II trials have established that concomitant PD-1/PD-L1 inhibition with radiotherapy is generally well-tolerated without dose-limiting toxicities [116,117,118,119]. Furthermore, with increasing adoption of ablative radiotherapy for treatment of multiple metastatic foci, Luke et al. demonstrated that multisite SBRT to up to four lesions followed by pembrolizumab within 7 days of SBRT completion was well tolerated [120]. Recently, the phase III PACIFIC trial that randomized locally-advanced unresectable non-small cell lung cancer (NSCLC) patients to either adjuvant durvalumab (anti-PD-L1 antibody) or placebo after chemoradiation demonstrated significant improvement in progression-free survival with durvalumab (median survival 16.8 vs. 5.6 months) [121]. Most recent update of the trial results also showed improved overall survival with patients receiving durvalumab compared to those receiving placebo (2-year overall survival 66.3% vs. 55.6%) [122]. It is interesting to note that the secondary analysis of KEYNOTE-001 trial, a study in which locally advanced or metastatic NSCLC patients were treated with anti-PD-1 pembrolizumab, showed improved survival in patients who received prior radiotherapy. Although this analysis was retrospective in nature and hypothesis-generating, it nevertheless shed light on the potential therapeutic synergy of radiotherapy and PD-1/PD-L1 blockade in the clinical setting [123].
5.5. Macrophage Polarization
Tumor-associated macrophages (TAMs) play important roles in tumorigenesis and contribute to maintaining an immunosuppressive TME in their default state. TAMs are typically pro-tumorigenic and phenotypically resemble M2 macrophages, and reducing tumor-infiltration of macrophages or modifying the polarity of immunosuppressive TAMs towards pro-inflammatory M1 phenotype have shown to impair tumor growth [124]. As previously discussed, radiation also promotes M2 polarization within the irradiated tissues. As such, by reversing the immunosuppressive phenotype of TAMs should augment the immunogenic effects of radiation.
CSF1 is a key cytokine responsible for promoting M2 polarization through CSF1 receptor (CSF1R)-mediated signaling and CSF1R blockade in tumor models led to repolarizing of TAMs to the M1 phenotype [125,126]. Xu et al. provided evidence that CSF1R blockade improved efficacy of radiotherapy against prostate cancer in a murine model, with associated decrease in intratumoral MDSCs and TAMs populations [50]. Furthermore, recent study demonstrated that macrophages can express PD-1 and that PD-1 expression correlated with M2 polarization. Blockade of PD-1/PD-L1 axis enhanced phagocytosis of tumor cells by intratumoral PD-1+ macrophages in vivo and decreased tumor burden [127]. Given that checkpoint inhibition of PD-1/PD-L1 axis is already being widely used, this finding underscores a novel mechanism in which PD-1/PD-L1 blockade can bolster therapeutic effects of radiotherapy.
6. Effect of Radiation Dose and Timing on Immunogenicity
Dose fractionation and timing of radiotherapy are important attributes of treatment efficacy when combining radiation with various forms of immunotherapy. However, there is currently no clear evidence regarding the optimal dose and timing of radiation when utilized with immunotherapy in the clinical setting, highlighting the need for well-designed clinical trials to address this concern.
6.1. Dose per Fraction
Preclinical studies have shown that a wide range of doses per fraction can induce several immunogenic molecular changes in the TME. Major histocompatibility complex class I (MHC-I), which is crucial for antigen presentation from cancer cells to allow for tumor detection by host immune system, can be induced by single radiation doses of 8–25 Gy [29,35,36] or daily doses of 2 Gy/fraction to a total of 50 Gy [128]. Radiation of various doses can also upregulate anti-tumor cytokine expressions, including interferon-beta, interferon-gamma, interleukin-1-beta, chemokine CXCL16, and tumor necrosis factor-alpha [6,29,30,31,129].
Currently, more evidence points towards SBRT/hypofractionated doses as being more immunogenic, although most studies discussed here compared regimens with different biologically effective dose. In B16/OVA murine model, single fraction of 15 Gy to the tumor resulted in greater tumor control and increased activation and infiltration of antitumor T-cells compared to 3 Gy × 5 fractionated doses [3]. Comparing different fractions of delivering a total dose of 15 Gy, Schaue et al. demonstrated greatest tumor response with 7.5 Gy × 2, with associated increase in activated IFN-γ-producing T-cells and relatively low proportions of Tregs [130]. In the setting of combined therapy with CTLA-4 inhibition, Dewan et al. reported that 8 Gy × 3 regimen against TSA mouse breast carcinoma resulted in enhanced tumor response of both irradiated and non-irradiated tumors compared to the two other tested fractionations (20 Gy × 1 and 6 Gy × 5), with frequency of CD8+ T-cell activation proportional to treatment response [7]. Similarly, a single fraction of 12 Gy with concomitant PD-L1 blockade led to effective tumor control and antitumor modulation of immune cell milieu in the TME [8]. Recently, Vanpouille-Box et al. demonstrated systemic antitumor abscopal effect using combined treatment with 8 Gy × 3 and CTLA-4 blockade. Mechanistically, the authors showed that doses between 4 Gy to 12 Gy per fraction upregulates IFN-β production and secretion via the cyclic GMP-AMP synthase (cGAS) and its downstream stimulator of interferon genes (STING) pathway. Notably, doses of >12 Gy per fraction induced Trex1-mediated degradation of cytosolic DNA and abrogated the immunogenic secretion of IFN-β, illustrating that ablative doses of radiation, at least in certain cancer cells, may in fact negate the immunogenicity of tumor cell death [131]. While the evidence above collectively shows antitumor immunogenicity elicited with hypofractionated doses (and perhaps not ablative doses), it is important to note the wide spectrum of doses reported, suggesting that heterogeneity in the optimal dose-per-fraction likely exists among different tumor types.
On the other hand, results for conventional fractionation with low doses per fraction are mixed. As discussed earlier, lymphocytes are very radiosensitive and conventional fractionation often leads to lymphopenia [41,42]. As a case in point, a study comparing SBRT to conventional fractionation radiotherapy in pancreatic cancer revealed that rates of severe lymphopenia were 13.8% versus 71.7%, respectively [132]. Some evidence has also demonstrated immunosuppressive properties of low-dose radiation. In an ex vivo model, macrophages receiving doses of 0.1–0.5 Gy exhibit anti-inflammatory status with reduction in IL-1β secretion and increase in TGF-β expression [133]. In another study, conventional fractionation of 2 Gy × 5 in several cell lines in vitro, compared to 10 Gy × 1, led to induction of TGF-β-associated and IFN-related genes that are conducive of an immunosuppressive TME [134]. On the contrary, other studies have successfully stimulated antitumor immunity with conventional fractionation. An in vivo study using low-dose radiation was effective for normalizing tumor vasculature, which would facilitate the migration of immune cells across the endothelium and into the tumor [135]. Furthermore, low-dose radiation induced M1 macrophage phenotype and subsequently increased T-cell recruitment into the irradiated tumor [135,136]. Two studies from the same group also demonstrated potent T-cell dependent antitumor response with fractionated 2 Gy × 5 with concurrent PD-L1 inhibition [51,114]. These conflicting data underscore the biological complexity of dose-fractionation, which is likely influenced by tumor histology and utilization of different immunotherapies. As an example in which tumor histology can affect radiation outcome, melanin in melanoma cells confer radioprotection by serving as free-radical scavengers, and as such, effective radiotherapy for melanoma typically requires higher dose-per-fraction [137,138]. Therefore, further studies are warranted to systematically identify the optimal doses in specific tumors in combination with specific immunomodulatory agents.
6.2. Timing
There is limited evidence to guide the ideal timing of radiotherapy when used in conjunction with immunotherapy. Depending on the mechanism of actions of the immunomodulatory agents used, the optimal timing of radiotherapy relative to administering immunotherapy is likely to differ.
In a preclinical model, Dovedi et al. determined that PD-L1 blockade is only effective when given concurrently with radiotherapy of 2 Gy × 5, but not sequentially two days after the five-fraction course [51]. This contrasts with the limited clinical evidence available. Subgroup analysis of the PACIFIC trial showed that progression-free survival is higher when patients received durvalumab within 14 days after chemoradiation compared to those who received treatment >14 days after (hazard ratio of 0.39 vs. 0.63) [121]. Secondary analysis of KEYNOTE-001 also reported the observation that patients receiving radiotherapy prior to pembrolizumab had improved median survival of 10.7 months vs. 5.3 months in those without previous radiotherapy, suggesting a possible temporal benefit when radiotherapy precedes PD-1/PD-L1 blockade [123]. Given that PD-L1 expression on tumor and immune cells are upregulated after radiation and serves as a mechanism of resistance by promoting T-cell exhaustion, as previously discussed, inhibition of the PD-1/PD-L1 axis shortly after radiotherapy appears to be reasonable. The contrasting evidence from the above preclinical model may potentially be attributed to the short subtherapeutic radiation regimen used (2 Gy × 5). However, it is possible that moving PD-1/PD-L1 blockade to the concurrent phase may further improve its therapeutic synergy with radiation and is now being investigated in a phase I trial CINJ 031507 in locally advanced NSCLC (NCT02621398).
Study by Young et al. also noted distinct effective radiotherapy timing with other immunotherapy agents. In mice bearing CT26 murine colorectal carcinoma, CTLA-4 blockade was most efficacious when given prior to, rather than after, focal radiation of 20 Gy. On the other hand, OX40 agonist antibody was most effective when administered one day after 20 Gy radiation, with decreased efficacy if given several days before or after radiation [139]. These findings are consistent with known mechanisms of CTLA-4 and OX40 therapies; CTLA-4 inhibition can deplete intratumoral Tregs prior to radiotherapy to mitigate the immunosuppressive TME and enhance immunogenicity of radiation, while OX40 co-stimulatory molecules are upregulated only for a brief period after antigen presentation induced by radiation [140,141]. Although challenging given the complex dynamics of the tumor immune response to combination treatment, further efforts are required to elucidate the optimal temporal relationship of various immunotherapies with radiotherapy in the clinical setting.
7. Ongoing Clinical Trials Assessing Combination of Radiotherapy with Immunotherapy
There are over a hundred clinical trials in the United States that were opened over the last two years designed to investigate different combinations of immunotherapies with radiation. Table 1 summarizes the relevant ongoing trials that were initiated after 1 May 2016; for a listing of earlier trials, see comprehensive reviews by Vacchelli et al. and Bloy et al. [142,143]. Many of the recent trials are phase I trials testing the safety and toxicity of combination therapies with various immunomodulatory agents and dose-fractionations of radiotherapy in different malignancies, which will not be included in Table 1 due to space limitation.
A significant proportion of recent trials utilize a combination of different immunotherapies with radiation, which partly stems from the realization that treatment response rates remain to be limited with radiotherapy combined with single immunotherapy agents (although still an improvement over radiotherapy alone). Inefficacy of combining with single agents could be attributed to the development of resistance against a given checkpoint blockade or the presence of multiple simultaneous immunosuppressive signals within the TME, which can be rescued if the appropriate additional agents were included in the regimens, as eloquently illustrated by Twyman-Saint et al. [109]. Another rationale for combining different immunomodulatory agents is improved therapeutic efficacy compared to single agents alone. In particular, a recent phase I trial NCT03431948 is testing the combination of 4-1BB agonist or CSF1R inhibitor with PD-1 blockade in conjunction with radiotherapy, which stems from preclinical evidence that the immune-activating potential of these agents is more robust in the combinatory setting [100,144]. Of note, many trials also included the use of chemotherapy, often given concurrently with radiotherapy, which may potentially alter the cumulative effects of combination therapy. Discussed separately in another review, certain chemotherapeutic agents can modulate the immune milieu of the TME or trigger immunogenic cell death, which should be considered when designing multi-modality trials [145].
However, key issues that are equally important to address lie within the intrinsic properties of radiation—timing of radiotherapy, dose-fractionation, and radiation modalities—as discussed in the previous section. Currently, only a handful of trials are designed to shed light on these subjects and are denoted accordingly in Table 1. Timing of immunotherapy relative to radiotherapy is being assessed in NSCLC patients receiving chemoradiotherapy and pembrolizumab (NCT02621398) and in a metastatic small cell lung cancer cohort treated with SBRT and nivolumab/ipilimumab (NCT03223155). Although both are phase I trials primarily evaluating the feasibility of shifting immunotherapy into the concurrent setting with radiotherapy, their secondary endpoints of comparing the efficacy and immunological changes of sequential vs. concurrent immunotherapy would provide valuable insight on the sequencing of different treatments in combination therapy. High versus low dose-per-fraction radiotherapy in combination with immunotherapy is being evaluated in two phase II trials (NCT02888743 and NCT03085719), which would attempt to address the potential differences in immunogenicity of fraction size clinically. Although whether radiation modality affects the immunogenic properties of radiotherapy is less clear and beyond the scope of this review, several phase I/II trials are testing the feasibility and outcomes of combining different radiation sources with immunotherapy (NCT02913417, NCT03486197, and NCT03325816). As we move forward with the strategy of enhancing radiotherapy through additional immunomodulation, we must address the uncertainty of how to best incorporate radiation in this multi-modality approach.
8. Conclusions
In summary, radiation can be considered as a form of immunological cancer therapy. While radiotherapy alone is unlikely to prevail against tumor evasion from the immune system, synergy of combining radiation with immunotherapy can better harness the immunogenic effects of radiotherapy. While evidence for the use of combination therapy in NSCLC and melanoma is more robust at the time of this review, many clinical trials are underway to ascertain the feasibility and efficacy of combining radiotherapy with immunotherapy in various malignancies. As we advance forward down this promising path of improving the ability to cure cancer with combination therapy, more efforts are necessitated to scrutinize the optimal dose and timing of radiotherapy in the combined setting.
Author Contributions
Writing—original draft preparation, S.-J.W.; writing—review and editing, S.-J.W. and B.H.
Funding
This research was funded by Breast Cancer Research Foundation, grant number BCRF-18-063. The APC was funded by BCRF-18-063.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Golden, E.B.; Formenti, S.C. Is tumor (R)ejection by the immune system the “5th R” of radiobiology? Oncoimmunology 2014, 3, e28133. [Google Scholar] [CrossRef] [PubMed]
- Stone, H.B.; Peters, L.J.; Milas, L. Effect of host immune capability on radiocurability and subsequent transplantability of a murine fibrosarcoma. J. Natl. Cancer Inst. 1979, 63, 1229–1235. [Google Scholar] [PubMed]
- Lugade, A.A.; Moran, J.P.; Gerber, S.A.; Rose, R.C.; Frelinger, J.G.; Lord, E.M. Local radiation therapy of B16 melanoma tumors increases the generation of tumor antigen-specific effector cells that traffic to the tumor. J. Immunol. 2005, 174, 7516–7523. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Auh, S.L.; Wang, Y.; Burnette, B.; Wang, Y.; Meng, Y.; Beckett, M.; Sharma, R.; Chin, R.; Tu, T.; et al. Therapeutic effects of ablative radiation on local tumor require CD8+ T cells: Changing strategies for cancer treatment. Blood 2009, 114, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Demaria, S.; Ng, B.; Devitt, M.L.; Babb, J.S.; Kawashima, N.; Liebes, L.; Formenti, S.C. Ionizing radiation inhibition of distant untreated tumors (abscopal effect) is immune mediated. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, S.; Wang, B.; Kawashima, N.; Braunstein, S.; Badura, M.; Cameron, T.O.; Babb, J.S.; Schneider, R.J.; Formenti, S.C.; Dustin, M.L.; et al. Radiation-induced CXCL16 release by breast cancer cells attracts effector T cells. J. Immunol. 2008, 181, 3099–3107. [Google Scholar] [CrossRef] [PubMed]
- Dewan, M.Z.; Galloway, A.E.; Kawashima, N.; Dewyngaert, J.K.; Babb, J.S.; Formenti, S.C.; Demaria, S. Fractionated but not single-dose radiotherapy induces an immune-mediated abscopal effect when combined with anti-CTLA-4 antibody. Clin. Cancer Res. 2009, 15, 5379–5388. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Liang, H.; Burnette, B.; Beckett, M.; Darga, T.; Weichselbaum, R.R.; Fu, Y.X. Irradiation and anti-PD-L1 treatment synergistically promote antitumor immunity in mice. J. Clin. Investig. 2014, 124, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Schuler, G.; Steinman, R.M. Dendritic cells as adjuvants for immune-mediated resistance to tumors. J. Exp. Med. 1997, 186, 1183–1187. [Google Scholar] [CrossRef] [PubMed]
- Albert, M.L.; Sauter, B.; Bhardwaj, N. Dendritic cells acquire antigen from apoptotic cells and induce class I-restricted CTLs. Nature 1998, 392, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Apetoh, L.; Ghiringhelli, F.; Tesniere, A.; Obeid, M.; Ortiz, C.; Criollo, A.; Mignot, G.; Maiuri, M.C.; Ullrich, E.; Saulnier, P.; et al. Toll-like receptor 4-dependent contribution of the immune system to anticancer chemotherapy and radiotherapy. Nat. Med. 2007, 13, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Zitvogel, L.; Kepp, O.; Kroemer, G. Decoding cell death signals in inflammation and immunity. Cell 2010, 140, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Golden, E.B.; Frances, D.; Pellicciotta, I.; Demaria, S.; Helen Barcellos-Hoff, M.; Formenti, S.C. Radiation fosters dose-dependent and chemotherapy-induced immunogenic cell death. Oncoimmunology 2014, 3, e28518. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.R.; Chekeni, F.B.; Trampont, P.C.; Lazarowski, E.R.; Kadl, A.; Walk, S.F.; Park, D.; Woodson, R.I.; Ostankovich, M.; Sharma, P.; et al. Nucleotides released by apoptotic cells act as a find-me signal to promote phagocytic clearance. Nature 2009, 461, 282–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghiringhelli, F.; Apetoh, L.; Tesniere, A.; Aymeric, L.; Ma, Y.; Ortiz, C.; Vermaelen, K.; Panaretakis, T.; Mignot, G.; Ullrich, E.; et al. Activation of the NLRP3 inflammasome in dendritic cells induces IL-1beta-dependent adaptive immunity against tumors. Nat. Med. 2009, 15, 1170–1178. [Google Scholar] [CrossRef] [PubMed]
- Obeid, M.; Panaretakis, T.; Joza, N.; Tufi, R.; Tesniere, A.; van Endert, P.; Zitvogel, L.; Kroemer, G. Calreticulin exposure is required for the immunogenicity of gamma-irradiation and UVC light-induced apoptosis. Cell Death Differ. 2007, 14, 1848–1850. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, M.; Abrams, S.I.; Camphausen, K.; Liu, K.; Scott, T.; Coleman, C.N.; Hodge, J.W. Irradiation of tumor cells up-regulates Fas and enhances CTL lytic activity and CTL adoptive immunotherapy. J. Immunol. 2003, 170, 6338–6347. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Takahashi, K.; Inanami, O. Induction of apoptosis through the activation of SAPK/JNK followed by the expression of death receptor Fas in X-irradiated cells. J. Radiat. Res. 2003, 44, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Chinnaiyan, A.M.; Prasad, U.; Shankar, S.; Hamstra, D.A.; Shanaiah, M.; Chenevert, T.L.; Ross, B.D.; Rehemtulla, A. Combined effect of tumor necrosis factor-related apoptosis-inducing ligand and ionizing radiation in breast cancer therapy. Proc. Natl. Acad. Sci. USA 2000, 97, 1754–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marini, P.; Schmid, A.; Jendrossek, V.; Faltin, H.; Daniel, P.T.; Budach, W.; Belka, C. Irradiation specifically sensitises solid tumour cell lines to TRAIL mediated apoptosis. BMC Cancer 2005, 5, 5. [Google Scholar] [CrossRef] [PubMed]
- Hori, T.; Kondo, T.; Kanamori, M.; Tabuchi, Y.; Ogawa, R.; Zhao, Q.L.; Ahmed, K.; Yasuda, T.; Seki, S.; Suzuki, K.; et al. Ionizing radiation enhances tumor necrosis factor-related apoptosis-inducing ligand (TRAIL)-induced apoptosis through up-regulations of death receptor 4 (DR4) and death receptor 5 (DR5) in human osteosarcoma cells. J. Orthop. Res. 2010, 28, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Vereecque, R.; Buffenoir, G.; Gonzalez, R.; Cambier, N.; Hetuin, D.; Bauters, F.; Fenaux, P.; Quesnel, B. gamma-ray irradiation induces B7.1 expression in myeloid leukaemic cells. Br. J. Haematol. 2000, 108, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Gasser, S.; Orsulic, S.; Brown, E.J.; Raulet, D.H. The DNA damage pathway regulates innate immune system ligands of the NKG2D receptor. Nature 2005, 436, 1186–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.Y.; Son, Y.O.; Park, S.W.; Bae, J.H.; Chung, J.S.; Kim, H.H.; Chung, B.S.; Kim, S.H.; Kang, C.D. Increase of NKG2D ligands and sensitivity to NK cell-mediated cytotoxicity of tumor cells by heat shock and ionizing radiation. Exp. Mol. Med. 2006, 38, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Bellone, M.; Calcinotto, A. Ways to enhance lymphocyte trafficking into tumors and fitness of tumor infiltrating lymphocytes. Front. Oncol. 2013, 3, 231. [Google Scholar] [CrossRef] [PubMed]
- Hallahan, D.; Kuchibhotla, J.; Wyble, C. Cell adhesion molecules mediate radiation-induced leukocyte adhesion to the vascular endothelium. Cancer Res. 1996, 56, 5150–5155. [Google Scholar] [PubMed]
- Quarmby, S.; Hunter, R.D.; Kumar, S. Irradiation induced expression of CD31, ICAM-1 and VCAM-1 in human microvascular endothelial cells. Anticancer Res. 2000, 20, 3375–3381. [Google Scholar] [PubMed]
- Matsumura, S.; Demaria, S. Up-regulation of the pro-inflammatory chemokine CXCL16 is a common response of tumor cells to ionizing radiation. Radiat. Res. 2010, 173, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Lugade, A.A.; Sorensen, E.W.; Gerber, S.A.; Moran, J.P.; Frelinger, J.G.; Lord, E.M. Radiation-induced IFN-gamma production within the tumor microenvironment influences antitumor immunity. J. Immunol. 2008, 180, 3132–3139. [Google Scholar] [CrossRef] [PubMed]
- Hallahan, D.E.; Spriggs, D.R.; Beckett, M.A.; Kufe, D.W.; Weichselbaum, R.R. Increased tumor necrosis factor alpha mRNA after cellular exposure to ionizing radiation. Proc. Natl. Acad. Sci. USA 1989, 86, 10104–10107. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, H.; Tsuneoka, K.; Dimchev, A.B.; Shikita, M. Induction of the expression of the interleukin-1 beta gene in mouse spleen by ionizing radiation. Radiat. Res. 1993, 133, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.H.; Chiang, C.S.; Tsao, C.Y.; Lin, P.Y.; McBride, W.H.; Wu, C.J. Rapid induction of cytokine gene expression in the lung after single and fractionated doses of radiation. Int. J. Radiat. Biol. 1999, 75, 1421–1427. [Google Scholar] [PubMed]
- Burnette, B.C.; Liang, H.; Lee, Y.; Chlewicki, L.; Khodarev, N.N.; Weichselbaum, R.R.; Fu, Y.X.; Auh, S.L. The efficacy of radiotherapy relies upon induction of type I interferon-dependent innate and adaptive immunity. Cancer Res. 2011, 71, 2488–2496. [Google Scholar] [CrossRef] [PubMed]
- Leone, P.; Shin, E.C.; Perosa, F.; Vacca, A.; Dammacco, F.; Racanelli, V. MHC class I antigen processing and presenting machinery: Organization, function, and defects in tumor cells. J. Natl. Cancer Inst. 2013, 105, 1172–1187. [Google Scholar] [CrossRef] [PubMed]
- Garnett, C.T.; Palena, C.; Chakraborty, M.; Tsang, K.Y.; Schlom, J.; Hodge, J.W. Sublethal irradiation of human tumor cells modulates phenotype resulting in enhanced killing by cytotoxic T lymphocytes. Cancer Res. 2004, 64, 7985–7994. [Google Scholar] [CrossRef] [PubMed]
- Reits, E.A.; Hodge, J.W.; Herberts, C.A.; Groothuis, T.A.; Chakraborty, M.; Wansley, E.K.; Camphausen, K.; Luiten, R.M.; de Ru, A.H.; Neijssen, J.; et al. Radiation modulates the peptide repertoire, enhances MHC class I expression, and induces successful antitumor immunotherapy. J. Exp. Med. 2006, 203, 1259–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newcomb, E.W.; Demaria, S.; Lukyanov, Y.; Shao, Y.; Schnee, T.; Kawashima, N.; Lan, L.; Dewyngaert, J.K.; Zagzag, D.; McBride, W.H.; et al. The combination of ionizing radiation and peripheral vaccination produces long-term survival of mice bearing established invasive GL261 gliomas. Clin. Cancer Res. 2006, 12, 4730–4737. [Google Scholar] [CrossRef] [PubMed]
- Formenti, S.C.; Demaria, S. Radiation therapy to convert the tumor into an in situ vaccine. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 879–880. [Google Scholar] [CrossRef] [PubMed]
- Segal, N.H.; Parsons, D.W.; Peggs, K.S.; Velculescu, V.; Kinzler, K.W.; Vogelstein, B.; Allison, J.P. Epitope landscape in breast and colorectal cancer. Cancer Res. 2008, 68, 889–892. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, T.N.; Schreiber, R.D. Neoantigens in cancer immunotherapy. Science 2015, 348, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, N.; Kusunoki, Y.; Akiyama, M. Radiosensitivity of CD4 or CD8 positive human T-lymphocytes by an in vitro colony formation assay. Radiat. Res. 1990, 123, 224–227. [Google Scholar] [CrossRef] [PubMed]
- Yovino, S.; Kleinberg, L.; Grossman, S.A.; Narayanan, M.; Ford, E. The etiology of treatment-related lymphopenia in patients with malignant gliomas: Modeling radiation dose to circulating lymphocytes explains clinical observations and suggests methods of modifying the impact of radiation on immune cells. Cancer Investig. 2013, 31, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Venkatesulu, B.P.; Mallick, S.; Lin, S.H.; Krishnan, S. A systematic review of the influence of radiation-induced lymphopenia on survival outcomes in solid tumors. Crit. Rev. Oncol./Hematol. 2018, 123, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Jin, S.; Zhang, A.; Zhang, B.; Shi, X.; Wang, J.; Zhao, Y. Gamma-ray resistance of regulatory CD4+CD25+Foxp3+ T cells in mice. Radiat. Res. 2010, 173, 148–157. [Google Scholar] [CrossRef] [PubMed]
- Kachikwu, E.L.; Iwamoto, K.S.; Liao, Y.P.; DeMarco, J.J.; Agazaryan, N.; Economou, J.S.; McBride, W.H.; Schaue, D. Radiation enhances regulatory T cell representation. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Barcellos-Hoff, M.H.; Derynck, R.; Tsang, M.L.; Weatherbee, J.A. Transforming growth factor-beta activation in irradiated murine mammary gland. J. Clin. Investig. 1994, 93, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Jobling, M.F.; Mott, J.D.; Finnegan, M.T.; Jurukovski, V.; Erickson, A.C.; Walian, P.J.; Taylor, S.E.; Ledbetter, S.; Lawrence, C.M.; Rifkin, D.B.; et al. Isoform-specific activation of latent transforming growth factor beta (LTGF-beta) by reactive oxygen species. Radiat. Res. 2006, 166, 839–848. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.S.; Chen, F.H.; Wang, C.C.; Huang, H.L.; Jung, S.M.; Wu, C.J.; Lee, C.C.; McBride, W.H.; Chiang, C.S.; Hong, J.H. Macrophages from irradiated tumors express higher levels of iNOS, arginase-I and COX-2, and promote tumor growth. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.S.; Fu, S.Y.; Wang, S.C.; Yu, C.F.; Chen, F.H.; Lin, C.M.; Hong, J.H. Irradiation promotes an m2 macrophage phenotype in tumor hypoxia. Front. Oncol. 2012, 2, 89. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Escamilla, J.; Mok, S.; David, J.; Priceman, S.; West, B.; Bollag, G.; McBride, W.; Wu, L. CSF1R signaling blockade stanches tumor-infiltrating myeloid cells and improves the efficacy of radiotherapy in prostate cancer. Cancer Res. 2013, 73, 2782–2794. [Google Scholar] [CrossRef] [PubMed]
- Dovedi, S.J.; Adlard, A.L.; Lipowska-Bhalla, G.; McKenna, C.; Jones, S.; Cheadle, E.J.; Stratford, I.J.; Poon, E.; Morrow, M.; Stewart, R.; et al. Acquired resistance to fractionated radiotherapy can be overcome by concurrent PD-L1 blockade. Cancer Res. 2014, 74, 5458–5468. [Google Scholar] [CrossRef] [PubMed]
- Parikh, F.; Duluc, D.; Imai, N.; Clark, A.; Misiukiewicz, K.; Bonomi, M.; Gupta, V.; Patsias, A.; Parides, M.; Demicco, E.G.; et al. Chemoradiotherapy-induced upregulation of PD-1 antagonizes immunity to HPV-related oropharyngeal cancer. Cancer Res. 2014, 74, 7205–7216. [Google Scholar] [CrossRef] [PubMed]
- Badoual, C.; Hans, S.; Merillon, N.; Van Ryswick, C.; Ravel, P.; Benhamouda, N.; Levionnois, E.; Nizard, M.; Si-Mohamed, A.; Besnier, N.; et al. PD-1-expressing tumor-infiltrating T cells are a favorable prognostic biomarker in HPV-associated head and neck cancer. Cancer Res. 2013, 73, 128–138. [Google Scholar] [CrossRef] [PubMed]
- McCulloch, H.D. On the analogy between spontaneous recoveries from cancer and the specific immunity induced by x ray irradiations of the lymphatic glands involved. Br. Med. J. 1908, 2, 1146–1148. [Google Scholar] [CrossRef] [PubMed]
- Brix, N.; Tiefenthaller, A.; Anders, H.; Belka, C.; Lauber, K. Abscopal, immunological effects of radiotherapy: Narrowing the gap between clinical and preclinical experiences. Immunol. Rev. 2017, 280, 249–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budhu, S.; Loike, J.D.; Pandolfi, A.; Han, S.; Catalano, G.; Constantinescu, A.; Clynes, R.; Silverstein, S.C. CD8+ T cell concentration determines their efficiency in killing cognate antigen-expressing syngeneic mammalian cells in vitro and in mouse tissues. J. Exp. Med. 2010, 207, 223–235. [Google Scholar] [CrossRef] [PubMed]
- Reynders, K.; Illidge, T.; Siva, S.; Chang, J.Y.; De Ruysscher, D. The abscopal effect of local radiotherapy: Using immunotherapy to make a rare event clinically relevant. Cancer Treat. Rev. 2015, 41, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Callahan, M.K.; Barker, C.A.; Yamada, Y.; Yuan, J.; Kitano, S.; Mu, Z.; Rasalan, T.; Adamow, M.; Ritter, E.; et al. Immunologic correlates of the abscopal effect in a patient with melanoma. N. Engl. J. Med. 2012, 366, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Teitz-Tennenbaum, S.; Li, Q.; Rynkiewicz, S.; Ito, F.; Davis, M.A.; McGinn, C.J.; Chang, A.E. Radiotherapy potentiates the therapeutic efficacy of intratumoral dendritic cell administration. Cancer Res. 2003, 63, 8466–8475. [Google Scholar] [PubMed]
- Filatenkov, A.; Baker, J.; Mueller, A.M.; Kenkel, J.; Ahn, G.O.; Dutt, S.; Zhang, N.; Kohrt, H.; Jensen, K.; Dejbakhsh-Jones, S.; et al. Ablative Tumor Radiation Can Change the Tumor Immune Cell Microenvironment to Induce Durable Complete Remissions. Clin. Cancer Res. 2015, 21, 3727–3739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Liu, L.; Yu, D.; Kandimalla, E.R.; Sun, H.B.; Agrawal, S.; Guha, C. An in situ autologous tumor vaccination with combined radiation therapy and TLR9 agonist therapy. PLoS ONE 2012, 7, e38111. [Google Scholar] [CrossRef] [PubMed]
- Milas, L.; Mason, K.A.; Ariga, H.; Hunter, N.; Neal, R.; Valdecanas, D.; Krieg, A.M.; Whisnant, J.K. CpG oligodeoxynucleotide enhances tumor response to radiation. Cancer Res. 2004, 64, 5074–5077. [Google Scholar] [CrossRef] [PubMed]
- Mason, K.A.; Ariga, H.; Neal, R.; Valdecanas, D.; Hunter, N.; Krieg, A.M.; Whisnant, J.K.; Milas, L. Targeting toll-like receptor 9 with CpG oligodeoxynucleotides enhances tumor response to fractionated radiotherapy. Clin. Cancer Res. 2005, 11, 361–369. [Google Scholar] [PubMed]
- Chamoto, K.; Takeshima, T.; Wakita, D.; Ohkuri, T.; Ashino, S.; Omatsu, T.; Shirato, H.; Kitamura, H.; Togashi, Y.; Nishimura, T. Combination immunotherapy with radiation and CpG-based tumor vaccination for the eradication of radio- and immuno-resistant lung carcinoma cells. Cancer Sci. 2009, 100, 934–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerkovnik, P.; Novakovic, B.J.; Stegel, V.; Novakovic, S. Tumor vaccine composed of C-class CpG oligodeoxynucleotides and irradiated tumor cells induces long-term antitumor immunity. BMC Immunol. 2010, 11, 45. [Google Scholar] [CrossRef] [PubMed]
- Dewan, M.Z.; Vanpouille-Box, C.; Kawashima, N.; DiNapoli, S.; Babb, J.S.; Formenti, S.C.; Adams, S.; Demaria, S. Synergy of topical toll-like receptor 7 agonist with radiation and low-dose cyclophosphamide in a mouse model of cutaneous breast cancer. Clin. Cancer Res. 2012, 18, 6668–6678. [Google Scholar] [CrossRef] [PubMed]
- Dovedi, S.J.; Melis, M.H.; Wilkinson, R.W.; Adlard, A.L.; Stratford, I.J.; Honeychurch, J.; Illidge, T.M. Systemic delivery of a TLR7 agonist in combination with radiation primes durable antitumor immune responses in mouse models of lymphoma. Blood 2013, 121, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Adlard, A.L.; Dovedi, S.J.; Telfer, B.A.; Koga-Yamakawa, E.; Pollard, C.; Honeychurch, J.; Illidge, T.M.; Murata, M.; Robinson, D.T.; Jewsbury, P.J.; et al. A novel systemically administered Toll-like receptor 7 agonist potentiates the effect of ionizing radiation in murine solid tumor models. Int. J. Cancer 2014, 135, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Scholch, S.; Rauber, C.; Tietz, A.; Rahbari, N.N.; Bork, U.; Schmidt, T.; Kahlert, C.; Haberkorn, U.; Tomai, M.A.; Lipson, K.E.; et al. Radiotherapy combined with TLR7/8 activation induces strong immune responses against gastrointestinal tumors. Oncotarget 2015, 6, 4663–4676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, J.H.; Lee, H.J.; Ko, H.J.; Yoon, B.I.; Choe, J.; Kim, K.C.; Hahn, T.W.; Han, J.A.; Choi, S.S.; Jung, Y.M.; et al. The TLR7 agonist imiquimod induces anti-cancer effects via autophagic cell death and enhances anti-tumoral and systemic immunity during radiotherapy for melanoma. Oncotarget 2017, 8, 24932–24948. [Google Scholar] [CrossRef] [PubMed]
- Brody, J.D.; Ai, W.Z.; Czerwinski, D.K.; Torchia, J.A.; Levy, M.; Advani, R.H.; Kim, Y.H.; Hoppe, R.T.; Knox, S.J.; Shin, L.K.; et al. In situ vaccination with a TLR9 agonist induces systemic lymphoma regression: A phase I/II study. J. Clin. Oncol. 2010, 28, 4324–4332. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Gratzinger, D.; Harrison, C.; Brody, J.D.; Czerwinski, D.K.; Ai, W.Z.; Morales, A.; Abdulla, F.; Xing, L.; Navi, D.; et al. In situ vaccination against mycosis fungoides by intratumoral injection of a TLR9 agonist combined with radiation: A phase 1/2 study. Blood 2012, 119, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Seung, S.K.; Curti, B.D.; Crittenden, M.; Walker, E.; Coffey, T.; Siebert, J.C.; Miller, W.; Payne, R.; Glenn, L.; Bageac, A.; et al. Phase 1 study of stereotactic body radiotherapy and interleukin-2—Tumor and immunological responses. Sci. Transl. Med. 2012, 4, 137ra174. [Google Scholar] [CrossRef] [PubMed]
- Sedlar, A.; Kranjc, S.; Dolinsek, T.; Cemazar, M.; Coer, A.; Sersa, G. Radiosensitizing effect of intratumoral interleukin-12 gene electrotransfer in murine sarcoma. BMC Cancer 2013, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.Y.; Keng, P.C. Inhibition of cell growth in synchronous human hypernephroma cells by recombinant interferon alpha-D and irradiation. J. Interferon Res. 1983, 3, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Kardamakis, D.; Gillies, N.E.; Souhami, R.L.; Bewerley, P.C. Recombinant human interferon alpha-2b enhances the radiosensitivity of small cell lung cancer in vitro. Anticancer Res. 1989, 9, 1041–1044. [Google Scholar] [PubMed]
- Nukui, Y.; Picozzi, V.J.; Traverso, L.W. Interferon-based adjuvant chemoradiation therapy improves survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. Am. J. Surg. 2000, 179, 367–371. [Google Scholar] [CrossRef]
- Picozzi, V.J.; Abrams, R.A.; Decker, P.A.; Traverso, W.; O’Reilly, E.M.; Greeno, E.; Martin, R.C.; Wilfong, L.S.; Rothenberg, M.L.; Posner, M.C.; et al. Multicenter phase II trial of adjuvant therapy for resected pancreatic cancer using cisplatin, 5-fluorouracil, and interferon-alfa-2b-based chemoradiation: ACOSOG Trial Z05031. Ann. Oncol. 2011, 22, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.; Abel, U.; Debus, J.; Harig, S.; Hoffmann, K.; Herrmann, T.; Bartsch, D.; Klein, J.; Mansmann, U.; Jager, D.; et al. Open-label, multicenter, randomized phase III trial of adjuvant chemoradiation plus interferon Alfa-2b versus fluorouracil and folinic acid for patients with resected pancreatic adenocarcinoma. J. Clin. Oncol. 2012, 30, 4077–4083. [Google Scholar] [CrossRef] [PubMed]
- Hallahan, D.E.; Vokes, E.E.; Rubin, S.J.; O’Brien, S.; Samuels, B.; Vijaykumar, S.; Kufe, D.W.; Phillips, R.; Weichselbaum, R.R. Phase I dose-escalation study of tumor necrosis factor-alpha and concomitant radiation therapy. Cancer J. Sci. Am. 1995, 1, 204–209. [Google Scholar] [PubMed]
- Mundt, A.J.; Vijayakumar, S.; Nemunaitis, J.; Sandler, A.; Schwartz, H.; Hanna, N.; Peabody, T.; Senzer, N.; Chu, K.; Rasmussen, C.S.; et al. A Phase I trial of TNFerade biologic in patients with soft tissue sarcoma in the extremities. Clin. Cancer Res. 2004, 10, 5747–5753. [Google Scholar] [CrossRef] [PubMed]
- Citrin, D.; Camphausen, K.; Wood, B.J.; Quezado, M.; Denobile, J.; Pingpank, J.F.; Royal, R.E.; Alexander, H.R.; Seidel, G.; Steinberg, S.M.; et al. A pilot feasibility study of TNFerade biologic with capecitabine and radiation therapy followed by surgical resection for the treatment of rectal cancer. Oncology 2010, 79, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Hecht, J.R.; Farrell, J.J.; Senzer, N.; Nemunaitis, J.; Rosemurgy, A.; Chung, T.; Hanna, N.; Chang, K.J.; Javle, M.; Posner, M.; et al. EUS or percutaneously guided intratumoral TNFerade biologic with 5-fluorouracil and radiotherapy for first-line treatment of locally advanced pancreatic cancer: A phase I/II study. Gastrointest. Endosc. 2012, 75, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.J.; Reid, T.; Senzer, N.; Swisher, S.; Pinto, H.; Hanna, N.; Chak, A.; Soetikno, R. Phase I evaluation of TNFerade biologic plus chemoradiotherapy before esophagectomy for locally advanced resectable esophageal cancer. Gastrointest. Endosc. 2012, 75, 1139–1146. [Google Scholar] [CrossRef] [PubMed]
- Seiwert, T.Y.; Darga, T.; Haraf, D.; Blair, E.A.; Stenson, K.; Cohen, E.E.; Salama, J.K.; Villaflor, V.; Witt, M.E.; Lingen, M.W.; et al. A phase I dose escalation study of Ad GV.EGR.TNF.11D (TNFerade Biologic) with concurrent chemoradiotherapy in patients with recurrent head and neck cancer undergoing reirradiation. Ann. Oncol. 2013, 24, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.M.; Wild, A.T.; Wang, H.; Tran, P.T.; Chang, K.J.; Taylor, G.E.; Donehower, R.C.; Pawlik, T.M.; Ziegler, M.A.; Cai, H.; et al. Randomized phase III multi-institutional study of TNFerade biologic with fluorouracil and radiotherapy for locally advanced pancreatic cancer: Final results. J. Clin. Oncol. 2013, 31, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Neri, D.; Sondel, P.M. Immunocytokines for cancer treatment: Past, present and future. Curr. Opin. Immunol. 2016, 40, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Zegers, C.M.; Rekers, N.H.; Quaden, D.H.; Lieuwes, N.G.; Yaromina, A.; Germeraad, W.T.; Wieten, L.; Biessen, E.A.; Boon, L.; Neri, D.; et al. Radiotherapy combined with the immunocytokine L19-IL2 provides long-lasting antitumor effects. Clin. Cancer Res. 2015, 21, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Rekers, N.H.; Olivo Pimentel, V.; Yaromina, A.; Lieuwes, N.G.; Biemans, R.; Zegers, C.M.L.; Germeraad, W.T.V.; Van Limbergen, E.J.; Neri, D.; Dubois, L.J.; et al. The immunocytokine L19-IL2: An interplay between radiotherapy and long-lasting systemic anti-tumour immune responses. Oncoimmunology 2018, 7, e1414119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckert, F.; Schmitt, J.; Zips, D.; Krueger, M.A.; Pichler, B.J.; Gillies, S.D.; Strittmatter, W.; Handgretinger, R.; Schilbach, K. Enhanced binding of necrosis-targeting immunocytokine NHS-IL12 after local tumour irradiation in murine xenograft models. Cancer Immunol. Immunother. 2016, 65, 1003–1013. [Google Scholar] [CrossRef] [PubMed]
- Eckert, F.; Jelas, I.; Oehme, M.; Huber, S.M.; Sonntag, K.; Welker, C.; Gillies, S.D.; Strittmatter, W.; Zips, D.; Handgretinger, R.; et al. Tumor-targeted IL-12 combined with local irradiation leads to systemic tumor control via abscopal effects in vivo. Oncoimmunology 2017, 6, e1323161. [Google Scholar] [CrossRef] [PubMed]
- Rech, A.J.; Dada, H.; Kotzin, J.J.; Henao-Mejia, J.; Minn, A.J.; Twyman-Saint Victor, C.; Vonderheide, R.H. Radiotherapy and CD40 Activation Separately Augment Immunity to Checkpoint Blockade in Cancer. Cancer Res. 2018, 78, 4282–4291. [Google Scholar] [CrossRef] [PubMed]
- Yasmin-Karim, S.; Bruck, P.T.; Moreau, M.; Kunjachan, S.; Chen, G.Z.; Kumar, R.; Grabow, S.; Dougan, S.K.; Ngwa, W. Radiation and Local Anti-CD40 Generate an Effective in situ Vaccine in Preclinical Models of Pancreatic Cancer. Front. Immunol. 2018, 9, 2030. [Google Scholar] [CrossRef] [PubMed]
- Yokouchi, H.; Yamazaki, K.; Chamoto, K.; Kikuchi, E.; Shinagawa, N.; Oizumi, S.; Hommura, F.; Nishimura, T.; Nishimura, M. Anti-OX40 monoclonal antibody therapy in combination with radiotherapy results in therapeutic antitumor immunity to murine lung cancer. Cancer Sci. 2008, 99, 361–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gough, M.J.; Crittenden, M.R.; Sarff, M.; Pang, P.; Seung, S.K.; Vetto, J.T.; Hu, H.M.; Redmond, W.L.; Holland, J.; Weinberg, A.D. Adjuvant therapy with agonistic antibodies to CD134 (OX40) increases local control after surgical or radiation therapy of cancer in mice. J. Immunother. 2010, 33, 798–809. [Google Scholar] [CrossRef] [PubMed]
- Niknam, S.; Barsoumian, H.B.; Schoenhals, J.E.; Jackson, H.L.; Yanamandra, N.; Caetano, M.S.; Li, A.; Younes, A.I.; Cadena, A.; Cushman, T.R.; et al. Radiation Followed by OX40 Stimulation Drives Local and Abscopal Antitumor Effects in an Anti-PD1-Resistant Lung Tumor Model. Clin. Cancer Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.E.; Kovacsovics-Bankowski, M.; Weinberg, A.D. The TNFRs OX40, 4–1BB, and CD40 as targets for cancer immunotherapy. Curr. Opin. Immunol. 2013, 25, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Shi, W.; Siemann, D.W. Augmented antitumor effects of radiation therapy by 4-1BB antibody (BMS-469492) treatment. Anticancer Res. 2006, 26, 3445–3453. [Google Scholar] [PubMed]
- Belcaid, Z.; Phallen, J.A.; Zeng, J.; See, A.P.; Mathios, D.; Gottschalk, C.; Nicholas, S.; Kellett, M.; Ruzevick, J.; Jackson, C.; et al. Focal radiation therapy combined with 4-1BB activation and CTLA-4 blockade yields long-term survival and a protective antigen-specific memory response in a murine glioma model. PLoS ONE 2014, 9, e101764. [Google Scholar] [CrossRef] [PubMed]
- Kroon, P.; Gadiot, J.; Peeters, M.; Gasparini, A.; Deken, M.A.; Yagita, H.; Verheij, M.; Borst, J.; Blank, C.U.; Verbrugge, I. Concomitant targeting of programmed death-1 (PD-1) and CD137 improves the efficacy of radiotherapy in a mouse model of human BRAFV600-mutant melanoma. Cancer Immunol. Immunother. 2016, 65, 753–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benaduce, A.P.; Brenneman, R.; Schrand, B.; Pollack, A.; Gilboa, E.; Ishkanian, A. 4-1BB Aptamer-Based Immunomodulation Enhances the Therapeutic Index of Radiation Therapy in Murine Tumor Models. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 458–461. [Google Scholar] [CrossRef] [PubMed]
- Demaria, S.; Kawashima, N.; Yang, A.M.; Devitt, M.L.; Babb, J.S.; Allison, J.P.; Formenti, S.C. Immune-mediated inhibition of metastases after treatment with local radiation and CTLA-4 blockade in a mouse model of breast cancer. Clin. Cancer Res. 2005, 11, 728–734. [Google Scholar] [PubMed]
- Slovin, S.F.; Higano, C.S.; Hamid, O.; Tejwani, S.; Harzstark, A.; Alumkal, J.J.; Scher, H.I.; Chin, K.; Gagnier, P.; McHenry, M.B.; et al. Ipilimumab alone or in combination with radiotherapy in metastatic castration-resistant prostate cancer: Results from an open-label, multicenter phase I/II study. Ann. Oncol. 2013, 24, 1813–1821. [Google Scholar] [CrossRef] [PubMed]
- Kwon, E.D.; Drake, C.G.; Scher, H.I.; Fizazi, K.; Bossi, A.; van den Eertwegh, A.J.; Krainer, M.; Houede, N.; Santos, R.; Mahammedi, H.; et al. Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): A multicentre, randomised, double-blind, phase 3 trial. Lancet. Oncol. 2014, 15, 700–712. [Google Scholar] [CrossRef]
- Grimaldi, A.M.; Simeone, E.; Giannarelli, D.; Muto, P.; Falivene, S.; Borzillo, V.; Giugliano, F.M.; Sandomenico, F.; Petrillo, A.; Curvietto, M.; et al. Abscopal effects of radiotherapy on advanced melanoma patients who progressed after ipilimumab immunotherapy. Oncoimmunology 2014, 3, e28780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandra, R.A.; Wilhite, T.J.; Balboni, T.A.; Alexander, B.M.; Spektor, A.; Ott, P.A.; Ng, A.K.; Hodi, F.S.; Schoenfeld, J.D. A systematic evaluation of abscopal responses following radiotherapy in patients with metastatic melanoma treated with ipilimumab. Oncoimmunology 2015, 4, e1046028. [Google Scholar] [CrossRef] [PubMed]
- Theurich, S.; Rothschild, S.I.; Hoffmann, M.; Fabri, M.; Sommer, A.; Garcia-Marquez, M.; Thelen, M.; Schill, C.; Merki, R.; Schmid, T.; et al. Local Tumor Treatment in Combination with Systemic Ipilimumab Immunotherapy Prolongs Overall Survival in Patients with Advanced Malignant Melanoma. Cancer Immunol. Res. 2016, 4, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Knisely, J.P.; Yu, J.B.; Flanigan, J.; Sznol, M.; Kluger, H.M.; Chiang, V.L. Radiosurgery for melanoma brain metastases in the ipilimumab era and the possibility of longer survival. J. Neurosurg. 2012, 117, 227–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twyman-Saint Victor, C.; Rech, A.J.; Maity, A.; Rengan, R.; Pauken, K.E.; Stelekati, E.; Benci, J.L.; Xu, B.; Dada, H.; Odorizzi, P.M.; et al. Radiation and dual checkpoint blockade activate non-redundant immune mechanisms in cancer. Nature 2015, 520, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Formenti, S.C.; Rudqvist, N.P.; Golden, E.; Cooper, B.; Wennerberg, E.; Lhuillier, C.; Vanpouille-Box, C.; Friedman, K.; Ferrari de Andrade, L.; Wucherpfennig, K.W.; et al. Radiotherapy induces responses of lung cancer to CTLA-4 blockade. Nat. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Zeng, J.; See, A.P.; Phallen, J.; Jackson, C.M.; Belcaid, Z.; Ruzevick, J.; Durham, N.; Meyer, C.; Harris, T.J.; Albesiano, E.; et al. Anti-PD-1 blockade and stereotactic radiation produce long-term survival in mice with intracranial gliomas. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Park, S.S.; Dong, H.; Liu, X.; Harrington, S.M.; Krco, C.J.; Grams, M.P.; Mansfield, A.S.; Furutani, K.M.; Olivier, K.R.; Kwon, E.D. PD-1 Restrains Radiotherapy-Induced Abscopal Effect. Cancer Immunol. Res. 2015, 3, 610–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharabi, A.B.; Nirschl, C.J.; Kochel, C.M.; Nirschl, T.R.; Francica, B.J.; Velarde, E.; Deweese, T.L.; Drake, C.G. Stereotactic Radiation Therapy Augments Antigen-Specific PD-1-Mediated Antitumor Immune Responses via Cross-Presentation of Tumor Antigen. Cancer Immunol. Res. 2015, 3, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Dovedi, S.J.; Cheadle, E.J.; Popple, A.L.; Poon, E.; Morrow, M.; Stewart, R.; Yusko, E.C.; Sanders, C.M.; Vignali, M.; Emerson, R.O.; et al. Fractionated Radiation Therapy Stimulates Antitumor Immunity Mediated by Both Resident and Infiltrating Polyclonal T-cell Populations when Combined with PD-1 Blockade. Clin. Cancer Res. 2017, 23, 5514–5526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Schoenhals, J.E.; Li, A.; Valdecanas, D.R.; Ye, H.; Zang, F.; Tang, C.; Tang, M.; Liu, C.G.; Liu, X.; et al. Suppression of Type I IFN Signaling in Tumors Mediates Resistance to Anti-PD-1 Treatment That Can Be Overcome by Radiotherapy. Cancer Res. 2017, 77, 839–850. [Google Scholar] [CrossRef] [PubMed]
- Barker, C.A.; Postow, M.A.; Kronenberg, S.A.; Ma, J.; Yamada, Y.; Beal, K.; Chan, T.A.; Callahan, M.K.; Wolchok, J.D. Concurrent Radiation Therapy (RT), Ipilimumab (Ipi) and/or Nivolumab (Nivo) on a Phase 1 Clinical Trial. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, S210–S211. [Google Scholar] [CrossRef]
- Levy, A.; Massard, C.; Soria, J.C.; Deutsch, E. Concurrent irradiation with the anti-programmed cell death ligand-1 immune checkpoint blocker durvalumab: Single centre subset analysis from a phase 1/2 trial. Eur. J. Cancer 2016, 68, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Duffy, A.G.; Makarova-Rusher, O.V.; Kleiner, D.E.; Alewine, C.; Figg, W.D.; Steinberg, S.M.; Levy, E.B.; Krishnasamy, V.P.; Wood, B.J.; Citrin, D.E.; et al. A pilot study of immune checkpoint inhibition in combination with radiation therapy in patients with metastatic pancreatic cancer. J. Clin. Oncol. 2017, 35. [Google Scholar] [CrossRef]
- Lin, S.H.; Lin, Y.; Price, J.; Parker, M.; Gomez, D.R.; Welsh, J.W.; Komaki, R.; Kurie, J.M.; Simon, G.R.; Blumenschein, G.R.; et al. DETERRED: PD-L1 blockade to evaluate the safety of lung cancer therapy using carboplatin, paclitaxel, and radiation combined with MPDL3280A (atezolizumab). J. Clin. Oncol. 2017, 35, 3064. [Google Scholar] [CrossRef]
- Luke, J.J.; Lemons, J.M.; Karrison, T.G.; Pitroda, S.P.; Melotek, J.M.; Zha, Y.; Al-Hallaq, H.A.; Arina, A.; Khodarev, N.N.; Janisch, L.; et al. Safety and Clinical Activity of Pembrolizumab and Multisite Stereotactic Body Radiotherapy in Patients With Advanced Solid Tumors. J. Clin. Oncol. 2018, 36, 1611–1618. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Shaverdian, N.; Lisberg, A.E.; Bornazyan, K.; Veruttipong, D.; Goldman, J.W.; Formenti, S.C.; Garon, E.B.; Lee, P. Previous radiotherapy and the clinical activity and toxicity of pembrolizumab in the treatment of non-small-cell lung cancer: A secondary analysis of the KEYNOTE-001 phase 1 trial. Lancet Oncol. 2017, 18, 895–903. [Google Scholar] [CrossRef]
- Aras, S.; Zaidi, M.R. TAMeless traitors: Macrophages in cancer progression and metastasis. Br. J. Cancer 2017, 117, 1583–1591. [Google Scholar] [CrossRef] [PubMed]
- Pyonteck, S.M.; Akkari, L.; Schuhmacher, A.J.; Bowman, R.L.; Sevenich, L.; Quail, D.F.; Olson, O.C.; Quick, M.L.; Huse, J.T.; Teijeiro, V.; et al. CSF-1R inhibition alters macrophage polarization and blocks glioma progression. Nat. Med. 2013, 19, 1264–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, Y.; Knolhoff, B.L.; Meyer, M.A.; Nywening, T.M.; West, B.L.; Luo, J.; Wang-Gillam, A.; Goedegebuure, S.P.; Linehan, D.C.; DeNardo, D.G. CSF1/CSF1R blockade reprograms tumor-infiltrating macrophages and improves response to T-cell checkpoint immunotherapy in pancreatic cancer models. Cancer Res. 2014, 74, 5057–5069. [Google Scholar] [CrossRef] [PubMed]
- Gordon, S.R.; Maute, R.L.; Dulken, B.W.; Hutter, G.; George, B.M.; McCracken, M.N.; Gupta, R.; Tsai, J.M.; Sinha, R.; Corey, D.; et al. PD-1 expression by tumour-associated macrophages inhibits phagocytosis and tumour immunity. Nature 2017, 545, 495–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauser, S.H.; Calorini, L.; Wazer, D.E.; Gattoni-Celli, S. Radiation-enhanced expression of major histocompatibility complex class I antigen H-2Db in B16 melanoma cells. Cancer Res. 1993, 53, 1952–1955. [Google Scholar] [PubMed]
- Deng, L.; Liang, H.; Xu, M.; Yang, X.; Burnette, B.; Arina, A.; Li, X.D.; Mauceri, H.; Beckett, M.; Darga, T.; et al. STING-Dependent Cytosolic DNA Sensing Promotes Radiation-Induced Type I Interferon-Dependent Antitumor Immunity in Immunogenic Tumors. Immunity 2014, 41, 843–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaue, D.; Ratikan, J.A.; Iwamoto, K.S.; McBride, W.H. Maximizing tumor immunity with fractionated radiation. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 1306–1310. [Google Scholar] [CrossRef] [PubMed]
- Vanpouille-Box, C.; Alard, A.; Aryankalayil, M.J.; Sarfraz, Y.; Diamond, J.M.; Schneider, R.J.; Inghirami, G.; Coleman, C.N.; Formenti, S.C.; Demaria, S. DNA exonuclease Trex1 regulates radiotherapy-induced tumour immunogenicity. Nat. Commun. 2017, 8, 15618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wild, A.T.; Herman, J.M.; Dholakia, A.S.; Moningi, S.; Lu, Y.; Rosati, L.M.; Hacker-Prietz, A.; Assadi, R.K.; Saeed, A.M.; Pawlik, T.M.; et al. Lymphocyte-Sparing Effect of Stereotactic Body Radiation Therapy in Patients With Unresectable Pancreatic Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 571–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wunderlich, R.; Ernst, A.; Rodel, F.; Fietkau, R.; Ott, O.; Lauber, K.; Frey, B.; Gaipl, U.S. Low and moderate doses of ionizing radiation up to 2 Gy modulate transmigration and chemotaxis of activated macrophages, provoke an anti-inflammatory cytokine milieu, but do not impact upon viability and phagocytic function. Clin. Exp. Immunol. 2015, 179, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.H.; Cook, J.A.; Chandramouli, G.V.; DeGraff, W.; Yan, H.; Zhao, S.; Coleman, C.N.; Mitchell, J.B.; Chuang, E.Y. Gene expression profiling of breast, prostate, and glioma cells following single versus fractionated doses of radiation. Cancer Res. 2007, 67, 3845–3852. [Google Scholar] [CrossRef] [PubMed]
- Klug, F.; Prakash, H.; Huber, P.E.; Seibel, T.; Bender, N.; Halama, N.; Pfirschke, C.; Voss, R.H.; Timke, C.; Umansky, L.; et al. Low-dose irradiation programs macrophage differentiation to an iNOS(+)/M1 phenotype that orchestrates effective T cell immunotherapy. Cancer Cell 2013, 24, 589–602. [Google Scholar] [CrossRef] [PubMed]
- Prakash, H.; Klug, F.; Nadella, V.; Mazumdar, V.; Schmitz-Winnenthal, H.; Umansky, L. Low doses of gamma irradiation potentially modifies immunosuppressive tumor microenvironment by retuning tumor-associated macrophages: Lesson from insulinoma. Carcinogenesis 2016, 37, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Brozyna, A.A.; Jozwicki, W.; Roszkowski, K.; Filipiak, J.; Slominski, A.T. Melanin content in melanoma metastases affects the outcome of radiotherapy. Oncotarget 2016, 7, 17844–17853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sniegocka, M.; Podgorska, E.; Plonka, P.M.; Elas, M.; Romanowska-Dixon, B.; Szczygiel, M.; Zmijewski, M.A.; Cichorek, M.; Markiewicz, A.; Brozyna, A.A.; et al. Transplantable Melanomas in Hamsters and Gerbils as Models for Human Melanoma. Sensitization in Melanoma Radiotherapy-From Animal Models to Clinical Trials. Int. J. Mol. Sci. 2018, 19, 1048. [Google Scholar] [CrossRef] [PubMed]
- Young, K.H.; Baird, J.R.; Savage, T.; Cottam, B.; Friedman, D.; Bambina, S.; Messenheimer, D.J.; Fox, B.; Newell, P.; Bahjat, K.S.; et al. Optimizing Timing of Immunotherapy Improves Control of Tumors by Hypofractionated Radiation Therapy. PLoS ONE 2016, 11, e0157164. [Google Scholar] [CrossRef] [PubMed]
- Simpson, T.R.; Li, F.; Montalvo-Ortiz, W.; Sepulveda, M.A.; Bergerhoff, K.; Arce, F.; Roddie, C.; Henry, J.Y.; Yagita, H.; Wolchok, J.D.; et al. Fc-dependent depletion of tumor-infiltrating regulatory T cells co-defines the efficacy of anti-CTLA-4 therapy against melanoma. J. Exp. Med. 2013, 210, 1695–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, D.E.; Prell, R.A.; Thalhofer, C.J.; Hurwitz, A.A.; Weinberg, A.D. Engagement of OX40 enhances antigen-specific CD4(+) T cell mobilization/memory development and humoral immunity: Comparison of alphaOX-40 with alphaCTLA-4. J. Immunol. 2001, 167, 6804–6811. [Google Scholar] [CrossRef] [PubMed]
- Vacchelli, E.; Bloy, N.; Aranda, F.; Buque, A.; Cremer, I.; Demaria, S.; Eggermont, A.; Formenti, S.C.; Fridman, W.H.; Fucikova, J.; et al. Trial Watch: Immunotherapy plus radiation therapy for oncological indications. Oncoimmunology 2016, 5, e1214790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloy, N.; Pol, J.; Manic, G.; Vitale, I.; Eggermont, A.; Galon, J.; Tartour, E.; Zitvogel, L.; Kroemer, G.; Galluzzi, L. Trial Watch: Radioimmunotherapy for oncological indications. Oncoimmunology 2014, 3, e954929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannarile, M.A.; Weisser, M.; Jacob, W.; Jegg, A.M.; Ries, C.H.; Ruttinger, D. Colony-stimulating factor 1 receptor (CSF1R) inhibitors in cancer therapy. J. Immunother. Cancer 2017, 5, 53. [Google Scholar] [CrossRef] [PubMed]
- Garg, A.D.; More, S.; Rufo, N.; Mece, O.; Sassano, M.L.; Agostinis, P.; Zitvogel, L.; Kroemer, G.; Galluzzi, L. Trial watch: Immunogenic cell death induction by anticancer chemotherapeutics. Oncoimmunology 2017, 6, e1386829. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Pro-immunogenic and immunosuppressive properties of radiation. Radiation promotes tumor immunogenicity by release of danger-associated molecular patterns (DAMPs) to attract and activate immune cells, translocation of calreticulin to the cell surface to serve as a phagocytotic signal, upregulation of death receptors and ligands (TRAIL, FAS, and DR 4/5), release of various pro-inflammatory cytokines, increase in MHC I expression to facilitate antigen presentation, and neoantigen formation. Low-dose radiation to the tumor vasculature can also induce ICAM-1 and E-selectin expression on endothelial cells to promote extravasation of immune cells into the tumor microenvironment (TME). On the other hand, immunosuppressive effects of radiation include lymphopenia due to cytotoxic effects of radiation on lymphocytes, proportional increase in Tregs, M2 polarization of macrophages, secretion of anti-inflammatory cytokine TGF-β, and induction of PD-L1 expression on tumor cells. Abbreviations: HMGB1 = high mobility group box 1; HSP = heat shock protein; ATP = adenosine triphosphate; TRAIL = tumor necrosis factor-related apoptosis-inducing ligand; DR4/5 = death receptor 4/5; IL-1β = interleukin 1β; TNF-α = tumor necrosis factor α; MHC I = major histocompatibility complex class I; ICAM-1 = intercellular adhesion molecule 1; Mφ2 = M2 macrophage; TGF-β = transforming growth factor β; PD-L1 = programmed death ligand 1.
Figure 1.
Pro-immunogenic and immunosuppressive properties of radiation. Radiation promotes tumor immunogenicity by release of danger-associated molecular patterns (DAMPs) to attract and activate immune cells, translocation of calreticulin to the cell surface to serve as a phagocytotic signal, upregulation of death receptors and ligands (TRAIL, FAS, and DR 4/5), release of various pro-inflammatory cytokines, increase in MHC I expression to facilitate antigen presentation, and neoantigen formation. Low-dose radiation to the tumor vasculature can also induce ICAM-1 and E-selectin expression on endothelial cells to promote extravasation of immune cells into the tumor microenvironment (TME). On the other hand, immunosuppressive effects of radiation include lymphopenia due to cytotoxic effects of radiation on lymphocytes, proportional increase in Tregs, M2 polarization of macrophages, secretion of anti-inflammatory cytokine TGF-β, and induction of PD-L1 expression on tumor cells. Abbreviations: HMGB1 = high mobility group box 1; HSP = heat shock protein; ATP = adenosine triphosphate; TRAIL = tumor necrosis factor-related apoptosis-inducing ligand; DR4/5 = death receptor 4/5; IL-1β = interleukin 1β; TNF-α = tumor necrosis factor α; MHC I = major histocompatibility complex class I; ICAM-1 = intercellular adhesion molecule 1; Mφ2 = M2 macrophage; TGF-β = transforming growth factor β; PD-L1 = programmed death ligand 1.


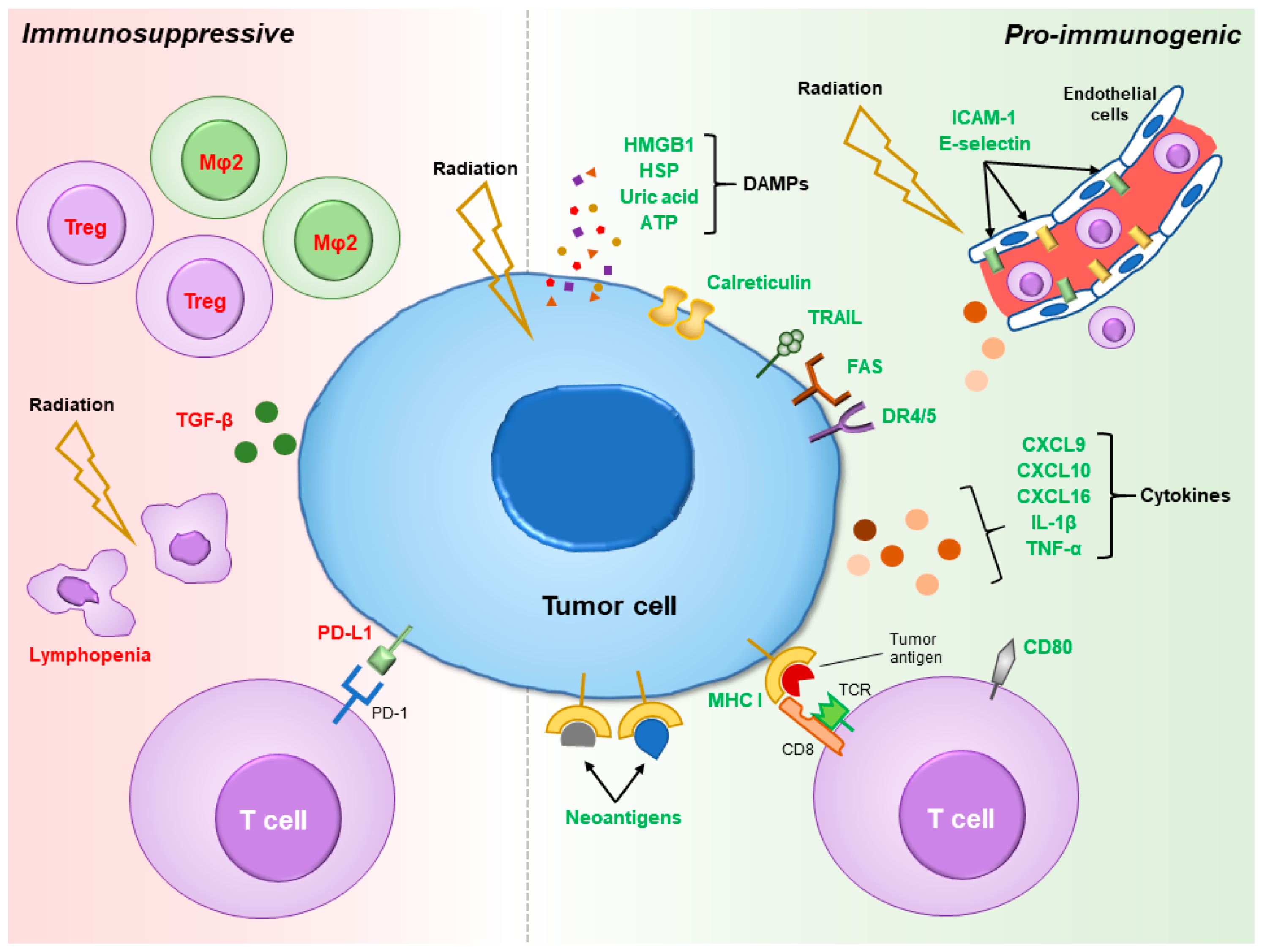{kind=link}
Table 1.
Recently initiated clinical trials for combining radiotherapy and immunotherapy.
| Immune Target | Indication | Drug | Phase | Status | Type of RT | Combined with Other Therapies | Clinical Trial # |
|---|---|---|---|---|---|---|---|
| PD-1 | Breast | Pembrolizumab | II | R | EBRT | None | NCT03051672 |
| Carcinoma unknown primary | Pembrolizumab | II | R | HFRT | None | NCT03396471 | |
| Esophago-gastric | Nivolumab | I/II | R | CFRT | Carboplatin/paclitaxel | NCT03278626 | |
| Pembrolizumab | II | R | CFRT | Carboplatin/paclitaxel | NCT03064490 | ||
| Pembrolizumab | II | R | CFRT | Capecitabine | NCT03257163 | ||
| Pembrolizumab | II | R | EBRT | None | NCT02830594 | ||
| GBM | Pembrolizumab | II | NYR | CFRT | None | NCT03661723 | |
| Pembrolizumab | II | R | CFRT | Temozolomide/HSPPC-96 | NCT03018288 | ||
| REGN2810 | I/II | R | EBRT | Temozolomide/gene therapy | NCT03491683 | ||
| HNSCC | Nivolumab | II | NYR | CFRT | None | NCT03715946 | |
| Nivolumab | II | R | CFRT | None | NCT03521570 | ||
| Nivolumab | I/II | R | HFRT | None | NCT03247712 | ||
| Pembrolizumab | II | NYR | CFRT | None | NCT03383094 | ||
| Pembrolizumab | II | R | CFRT/HFRT | None | NCT03085719 d | ||
| Pembrolizumab | II | R | CFRT | None | NCT03057613 | ||
| Pembrolizumab | III | R | CFRT | Cisplatin | NCT03040999 | ||
| Pembrolizumab | II | R | CFRT | Cisplatin | NCT02777385 | ||
| Pembrolizumab | I/II | R | CFRT | Cisplatin | NCT02759575 | ||
| Hodgkin lymphoma | Pembrolizumab | II | R | CFRT | Multiple chemotherapy cocktails | NCT03407144 | |
| Pembrolizumab | II | R | CFRT | None | NCT03179917 | ||
| Kidney | Nivolumab | II | R | SBRT | None | NCT02781506 | |
| Melanoma | Pembrolizumab | I/II | R | CFRT | A-dmDT390-bisFv (UCHT1) immunotoxin | NCT02990416 | |
| Merkel Cell carcinoma | Pembrolizumab | II | R | SBRT | None | NCT03304639 | |
| Nasophary-ngeal carcinoma | Nivolumab | II | R | CFRT | Cisplatin | NCT03267498 | |
| Lymphoma | Pembrolizumab | II | R | CFRT | None | NCT03210662 | |
| NSCLC | Nivolumab | II | R | SBRT | None | NCT03110978 | |
| Pembrolizumab | II | R | CFRT | Carboplatin/paclitaxel/cisplatin/pemetrexed | NCT03631784 | ||
| Pembrolizumab | II | R | CFRT | None | NCT03523702 | ||
| Pembrolizumab | II | R | SBRT | None | NCT03217071 | ||
| Pembrolizumab | I | R | CFRT | Carboplatin/paclitaxel | NCT02621398 t | ||
| Pancreatic | Nivolumab | II | R | SBRT | Cyclophosphamide/GVAX pancreas vaccine | NCT03161379 | |
| Pediatric | REGN2810 | I/II | R | CFRT/HFRT | None | NCT03690869 | |
| Prostate | Nivolumab | I/II | R | CFRT + HDRB | ADT | NCT03543189 | |
| Rectal | Pembrolizumab | II | R | CFRT | Capecitabine/fluorouracil/leucovorin/oxaliplatin | NCT02921256 | |
| SCLC | Nivolumab | I/II | R | 177Lu-DOTA0-Tyr3-Octreotate | None | NCT03325816 m | |
| Pembrolizumab | II | R | CFRT | Cisplatin/carboplatin/etoposide | NCT02934503 | ||
| Sarcoma | Pembrolizumab | I/II | R | CFRT | None | NCT03338959 | |
| Pembrolizumab | II | R | CFRT | None | NCT03092323 | ||
| Urothelial carcinoma | Nivolumab | II | R | CFRT | None | NCT03421652 | |
| Pembrolizumab | II | NYR | Neutron EBRT | None | NCT03486197 m | ||
| Pembrolizumab | II | NYR | HFRT | None | NCT03419130 | ||
| PD-L1 | Cervical | Atezolizumab | II | NYR | SBRT | None | NCT03614949 |
| Esophago-gastric | Durvalumab | II | R | CFRT | Carboplatin/paclitaxel | NCT02962063 | |
| GBM | Atezolizumab | I/II | R | CFRT | Temozolomide | NCT03174197 | |
| Avelumab | II | R | HFRT | None | NCT02968940 | ||
| HNSCC | Avelumab | III | R | CBRT | Cisplatin | NCT02952586 | |
| Lymphoma | Atezolizumab | II | R | CFRT | None | NCT03465891 | |
| Mesothelioma | Avelumab | I/II | R | SBRT | None | NCT03399552 | |
| Metastatic brain (breast) | Atezolizumab | II | R | SRS | None | NCT03483012 | |
| NSCLC | Avelumab | I/II | R | SBRT | None | NCT03050554 | |
| Durvalumab | II | NYR | SBRT | None | NCT03589547 | ||
| Durvalumab | I/II | R | SBRT | None | NCT03148327 | ||
| Durvalumab | II | R | SBRT | None | NCT02904954 | ||
| Ovarian | Avelumab | II | R | SBRT | None | NCT03312114 | |
| Pancreatic | Durvalumab | I/II | R | SBRT | None | NCT03245541 | |
| Urothelial carcinoma | Durvalumab | I/II | R | HFRT | BCG | NCT03317158 | |
| Durvalumab | I/II | R | CFRT | None | NCT02891161 | ||
| Others | Lymphoma | TLR9 agonist SD-101 | I/II | R | CFRT | Ibrutinib | NCT02927964 |
| Combo | Esophago-gastric | Nivolumab Relatlimab | I/II | NYR | SBRT | None | NCT03610711 |
| GBM | Avelumab Epacadostat | I/II | NYR | CFRT | Bevacizumab | NCT03532295 | |
| Ipilimumab Nivolumab | II | R | HFRT | None | NCT03367715 | ||
| Hepato-biliary carcinoma | Durvalumab Tremelimumab | II | R | EBRT | None | NCT03482102 | |
| HNSCC | Durvalumab Tremelimumab | I/II | R | SBRT | None | NCT03618134 | |
| Durvalumab Tremelimumab | I/II | R | SBRT | None | NCT03522584 | ||
| Kidney | Ipilimumab Nivolumab | II | R | SBRT | None | NCT03065179 | |
| Lymphoma | Anti-OX40 antibody BMS 986178 SD-101 | I | R | CFRT | None | NCT03410901 | |
| Epacadostat SD-101 | I/II | R | EBRT | None | NCT03322384 | ||
| Melanoma | Ipilimumab Nivolumab | II | R | HFRT | None | NCT03646617 | |
| Merkel Cell carcinoma | Ipilimumab Nivolumab | II | R | SBRT | None | NCT03071406 | |
| NSCLC | Atezolizumab Nivolumab Pembrolizumab | II | R | HFRT/SBRT | None | NCT03176173 | |
| Durvalumab Tremelimumab | II | R | CFRT | None | NCT03237377 | ||
| Intralesional IL-2 Nivolumab Pembrolizumab | I | R | HFRT | None | NCT03224871 | ||
| Ipilimumab Nivolumab | I/II | NYR | CFRT | Platinum-based chemotherapy | NCT03663166 | ||
| Ipilimumab Nivolumab | I/II | R | HFRT | None | NCT03168464 | ||
| Pancreatic | Cabiralizumab Nivolumab | II | R | SBRT | None | NCT03599362 | |
| Prostate | Pembrolizumab SD-101 | II | R | SBRT | Leuprolide/abiraterone/prednisone | NCT03007732 | |
| Rectal | Epacadostat Pembrolizumab | I/II | NYR | CFRT | Capecitabine/oxaliplatin | NCT03516708 | |
| Sarcoma | Durvalumab Tremelimumab | I/II | R | CFRT | None | NCT03116529 | |
| Ipilimumab Nivolumab | II | R | CFRT | None | NCT03307616 | ||
| SCLC | Ipilimumab Nivolumab | I | R | SBRT | None | NCT03223155 t | |
| Urothelial carcinoma | Durvalumab Tremelimumab | II | NYR | CFRT | None | NCT03601455 | |
| Uveal melanoma | Ipilimumab Nivolumab | I/II | R | Yttrium 90 | None | NCT02913417 m | |
| Multiple sites | Atezolizumab Nivolumab | II | R | HFRT | None | NCT03115801 | |
| Atezolizumab Nivolumab Pembrolizumab | II | R | HFRT | Nelfinavir | NCT03050060 | ||
| Atezolizumab Nivolumab Pembrolizumab | II | R | SBRT | None | NCT03313804 | ||
| Cabiralizumab Nivolumab Urelumab | I | R | SBRT | None | NCT03431948 | ||
| Durvalumab Tremelimumab | II | R | CFRT/HFRT | None | NCT02888743 d | ||
| Ipilimumab Nivolumab | II | R | EBRT | None | NCT03104439 | ||
| Pembrolizumab ADV/HSV-tk | II | R | SBRT | Valacyclovir | NCT03004183 | ||
| Pembrolizumab IL-2 | I/II | NYR | HFRT | None | NCT03474497 |
Abbreviations: RT = radiotherapy; GBM = glioblastoma; HNSCC = head & neck squamous cell carcinoma; NSCLC = non-small cell lung cancer; SCLC = small cell lung cancer; TLR9 = toll-like receptor 9; IL-2 = interleukin 2; R = recruiting; NYR = not yet recruiting; EBRT = external beam radiotherapy (fractionation unspecified); HFRT = hypofractionated radiotherapy; CFRT = conventionally-fractionated radiotherapy; SBRT = stereotactic body radiotherapy; HDRB = high-dose rate brachytherapy; SRS = stereotactic radiosurgery; BCG = Bacillus Calmette–Guérin therapy. d Trials comparing different dose-fractionation, t Trials evaluating timing of immunotherapy, m Trials assessing unique radiation modalities combined with immunotherapy.
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wang, S.-J.; Haffty, B. Radiotherapy as a New Player in Immuno-Oncology. Cancers 2018, 10, 515. https://doi.org/10.3390/cancers10120515
AMA Style
Wang S-J, Haffty B. Radiotherapy as a New Player in Immuno-Oncology. Cancers. 2018; 10(12):515. https://doi.org/10.3390/cancers10120515
Chicago/Turabian StyleWang, Shang-Jui, and Bruce Haffty. 2018. "Radiotherapy as a New Player in Immuno-Oncology" Cancers 10, no. 12: 515. https://doi.org/10.3390/cancers10120515
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.