Colorectal Cancer Presentation and Survival in Young Individuals: A Retrospective Cohort Study

 , and
, and
Abstract
:1. Introduction
2. Results
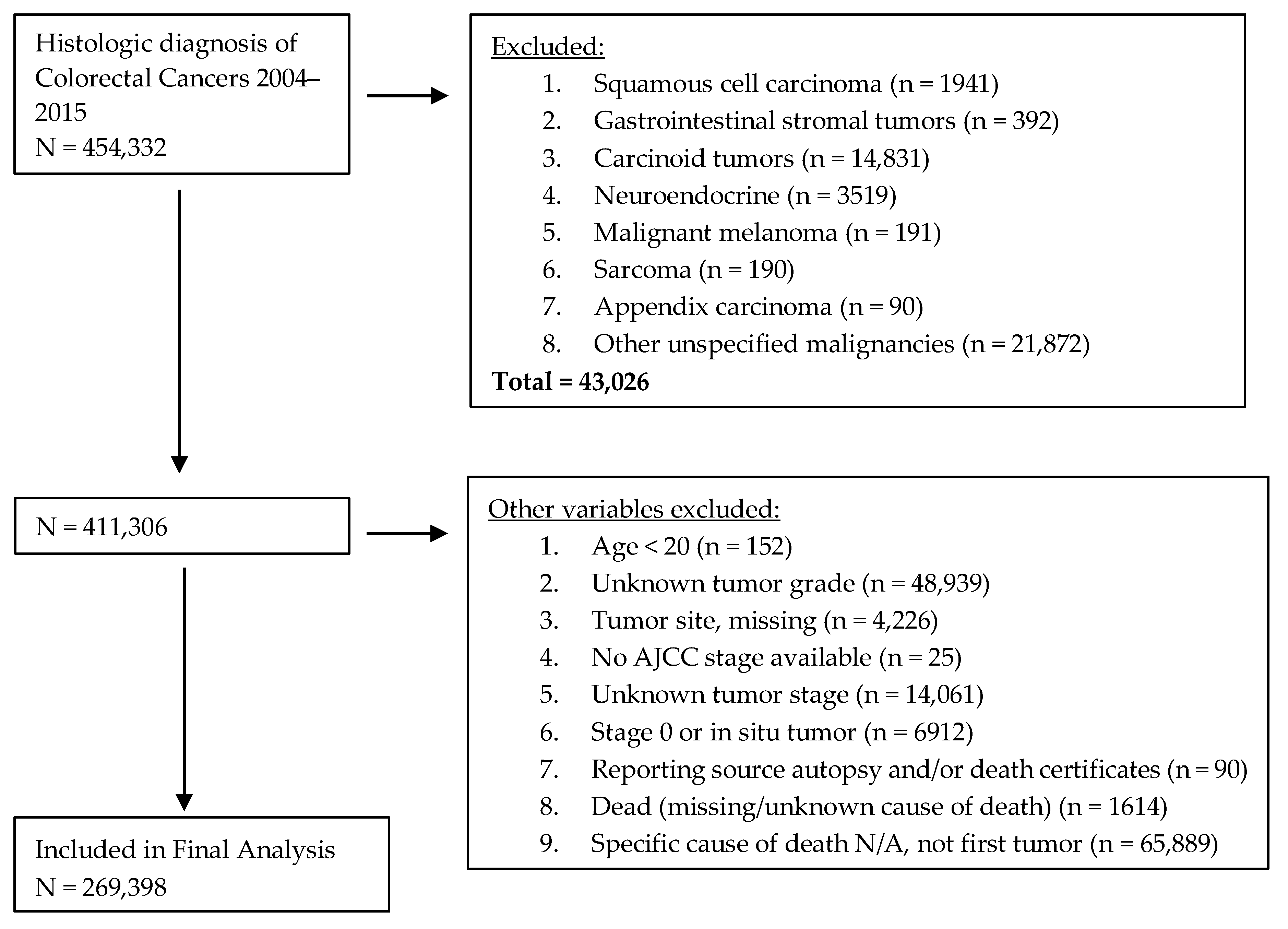
2.1. Study Population
2.2. Patient Characteristics
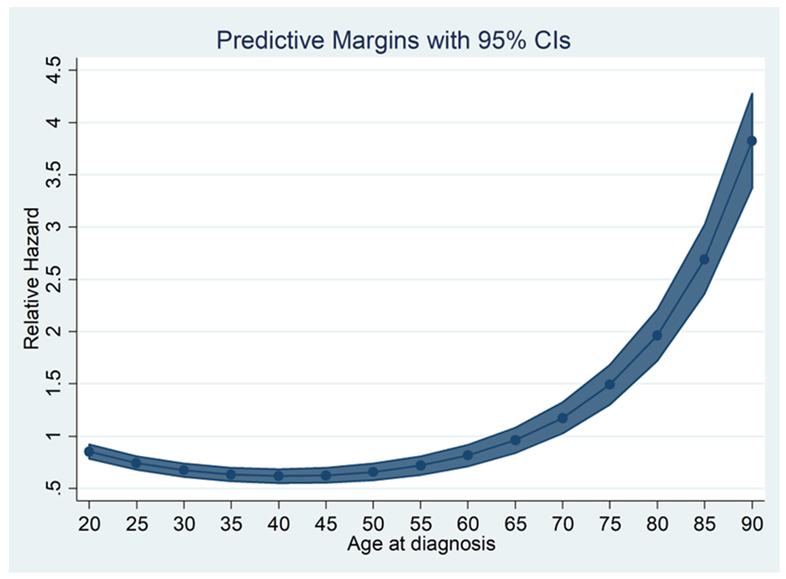
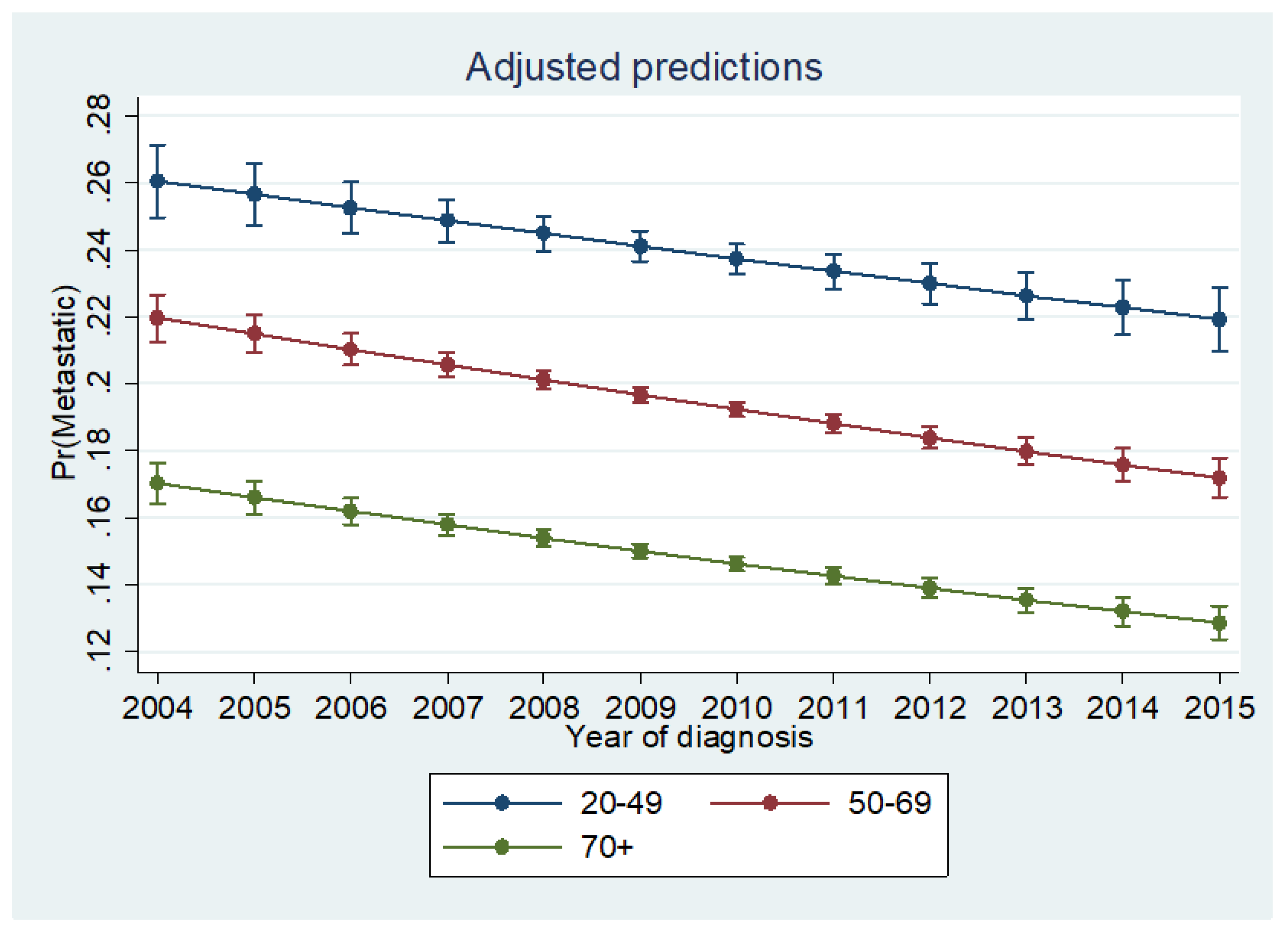
2.3. Likelihood of Metastatic Disease
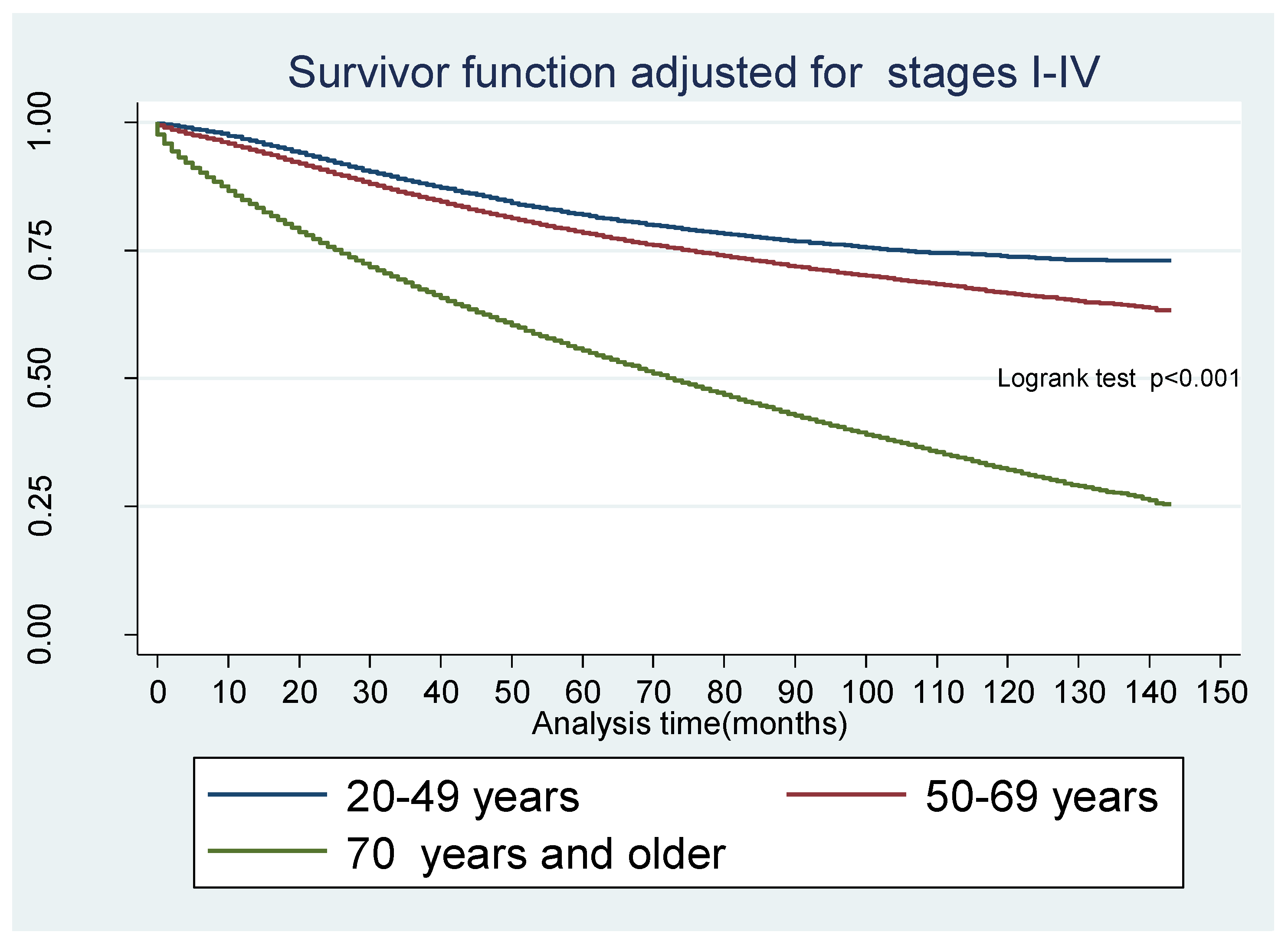
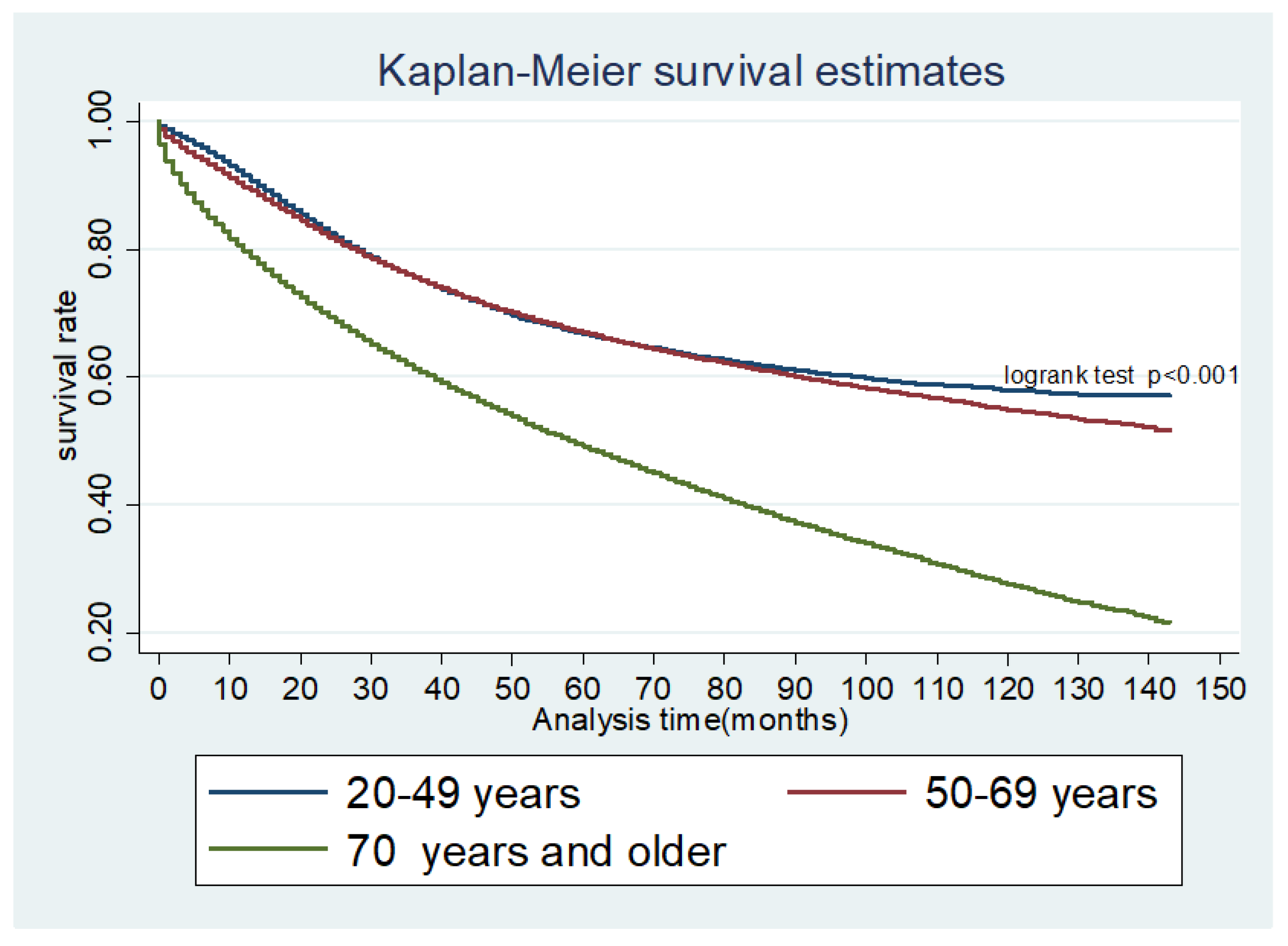
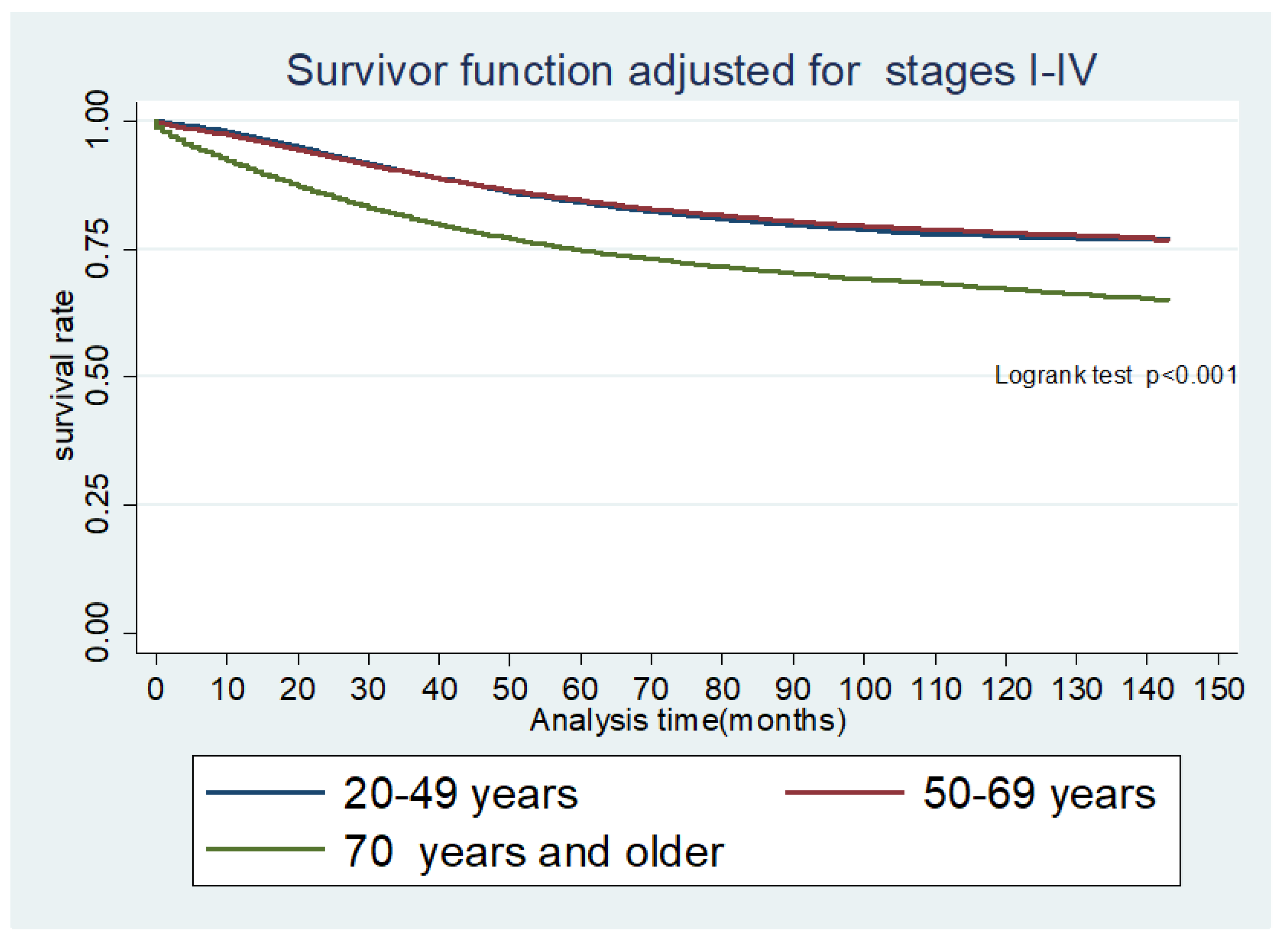
2.4. Overall and CRC-Specific Survival
3. Discussion
4. Materials and Methods
4.1. Study Design and Study Population
4.2. Data Source
4.3. Main Outcome Measures
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- O’Connell, J.B.; Maggard, M.A.; Liu, J.H.; Etzioni, D.A.; Livingston, E.H.; Ko, C.Y. Rates of colon and rectal cancers are increasing in young adults. Am. Surg. 2003, 69, 866–872. [Google Scholar] [PubMed]
- Siegel, R.L.; Jemal, A.; Ward, E.M. Increase in incidence of colorectal cancer among young men and women in the United States. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1695–1698. [Google Scholar] [CrossRef] [PubMed]
- Fairley, T.L.; Cardinez, C.J.; Martin, J.; Alley, L.; Friedman, C.; Edwards, B.; Jamison, P. Colorectal cancer in U.S. adults younger than 50 years of age, 1998–2001. Cancer 2006, 107, 1153–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.; Wang, M.J.; Ping, J. Clinicopathological Features and Survival Outcomes of Colorectal Cancer in Young Versus Elderly: A Population-Based Cohort Study of SEER 9 Registries Data (1988–2011). Medicine 2015, 94, e1402. [Google Scholar] [CrossRef] [PubMed]
- Zbuk, K.; Sidebotham, E.L.; Bleyer, A.; La Quaglia, M.P. Colorectal cancer in young adults. Semin. Oncol. 2009, 36, 439–450. [Google Scholar] [CrossRef] [PubMed]
- Paraf, F.; Jothy, S. Colorectal cancer before the age of 40: A case-control study. Dis. Colon Rectum. 2000, 43, 1222–1226. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.F.; Eu, K.W.; Machin, D.; Ho, J.M.; Nyam, D.C.; Leong, A.F.; Ho, Y.H.; Seow-Choen, F. Young age is not a poor prognostic marker in colorectal cancer. Br. J. Surg. 1998, 85, 1255–1259. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.B.; Maggard, M.A.; Liu, J.H.; Etzioni, D.A.; Livingston, E.H.; Ko, C.Y. Do young colon cancer patients have worse outcomes? World J. Surg. 2004, 28, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Wiela-Hojenska, A.; Kowalska, T.; Filipczyk-Cisarz, E.; Łapiński, Ł.; Nartowski, K. Evaluation of the toxicity of anticancer chemotherapy in patients with colon cancer. Adv. Clin. Exp. Med. 2015, 24, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Manjelievskaia, J.; Brown, D.; McGlynn, K.A. Chemotherapy Use and Survival Among Young and Middle-Aged Patients with Colon Cancer. JAMA Surg. 2017, 152, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.L.; Tseng, C.J.; Shiue, Y.L. The impact of young age on the prognosis for colorectal cancer: A population-based study in Taiwan. Jpn. J. Clin. Oncol. 2017, 47, 1010–1018. [Google Scholar] [CrossRef] [PubMed]
- Lieu, C.H.; Renfro, L.A.; de Gramont, A.; Maughan, T.S.; Seymour, M.T.; Saltz, L.; Goldberg, R.M.; Sargent, D.J.; Eckhardt, S.G.; et al. Association of age with survival in patients with metastatic colorectal cancer: Analysis from the ARCAD Clinical Trials Program. J. Clin. Oncol. 2014, 32, 2975–2984. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, L.; Brennan, K.; Karim, S.; Nanji, S.; Patel, S.V.; Booth, C.M. Disease Characteristics, Clinical Management, and Outcomes of Young Patients with Colon Cancer: A Population-based Study. Clin. Colorectal Cancer 2018, 17, e651–e661. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.S.; Piper, M.A.; Perdue, L.A.; Rutter, C.M.; Webber, E.M.; O’Connor, E.; Smith, N.; Whitlock, E.P. Screening for Colorectal Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016, 315, 2576–2594. [Google Scholar] [CrossRef] [PubMed]
- Wilt, T.J.; Harris, R.P.; Qaseem, A. Screening for cancer: Advice for high-value care from the American College of Physicians. Ann. Intern. Med. 2015, 162, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Rex, D.K.; Boland, C.R.; Dominitz, J.A.; Giardiello, F.M.; Johnson, D.A.; Kaltenbach, T.; Levin, T.R.; Lieberman, D.; Robertson, D.J. Colorectal Cancer Screening: Recommendations for Physicians and Patients From the U.S. Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2017, 153, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Fedewa, S.A.; Anderson, W.F.; Miller, K.D.; Ma, J.; Rosenberg, P.S.; Jemal, A. Colorectal Cancer Incidence Patterns in the United States, 1974–2013. J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuik, F.E.; Bardou, M.; Kuipers, E.J.; Spaander, M. Increasing incidence of colorectal cancer in young adults in Europe. Presented at UEG Week Vienna, Vienna, Austria, 20–24 October 2018. [Google Scholar]
- Troeung, L.; Sodhi-Berry, N.; Martini, A.; Malacova, E.; Ee, H.; O’Leary, P.; Lansdorp-Vogelaar, I.; Preen, D.B. Increasing Incidence of Colorectal Cancer in Adolescents and Young Adults Aged 15–39 Years in Western Australia 1982–2007: Examination of Colonoscopy History. Front. Public Health 2017, 5, 179. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yang, L.; Du, C.; Fang, X.; Wang, N.; Gu, J. Characteristics and comparison of colorectal cancer incidence in Beijing with other regions in the world. Oncotarget 2017, 8, 24593–24603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambe, P.C.; Jansen, S.; Zirngibl, H. New trend in colorectal cancer in Germany: Are young patients at increased risk for advanced colorectal cancer? World J. Surg. Oncol. 2017, 15, 159. [Google Scholar] [CrossRef] [PubMed]
- Pirzada, M.T.; Ahmed, M.J.; Muzzafar, A.; Nasir, I.U.I.; Shah, M.F.; Khattak, S.; Syed, A.A. Rectal Carcinoma: Demographics and Clinicopathological Features from Pakistani Population Perspective. Cureus 2017, 9, e1375. [Google Scholar] [CrossRef] [PubMed]
- Scott, R.B.; Rangel, L.E.; Osler, T.M.; Hyman, N.H. Rectal cancer in patients under the age of 50 years: The delayed diagnosis. Am. J. Surg. 2016, 211, 1014–1018. [Google Scholar] [CrossRef] [PubMed]
- Kneuertz, P.J.; Chang, G.J.; Hu, C.Y.; Rodriguez-Bigas, M.A.; Eng, C.; Vilar, E.; Skibber, J.M.; Feig, B.W.; Cormier, J.N.; You, Y.N. Overtreatment of young adults with colon cancer: More intense treatments with unmatched survival gains. JAMA Surg. 2015, 150, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Gopalan, V.; Smith, R.A.; Ho, Y.H.; Lam, A.K. Signet-ring cell carcinoma of the colorectum—Current perspectives and molecular biology. Int. J. Colorectal Dis. 2011, 26, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Foster, A.D.; Sivarapatna, A.; Gress, R.E. The aging immune system and its relationship with cancer. Aging Health 2011, 7, 707–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tammana, V.S.; Laiyemo, A.O. Colorectal cancer disparities: Issues, controversies and solutions. World J. Gastroenterol. 2014, 20, 869–876. [Google Scholar] [CrossRef] [PubMed]
- May, F.P.; Almario, C.V.; Ponce, N.; Spiegel, B.M. Racial minorities are more likely than whites to report lack of provider recommendation for colon cancer screening. Am. J. Gastroenterol. 2015, 110, 1388–1394. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.X.; Gross, C.P.; Soulos, P.R.; Yu, J.B. Estimating the magnitude of colorectal cancers prevented during the era of screening: 1976 to 2009. Cancer 2014, 120, 2893–2901. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Carroll, D.M.; Ogden, C.L.; Curtin, L.R. Prevalence and trends in obesity among US adults, 1999–2008. JAMA 2010, 303, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Frezza, E.E.; Wachtel, M.S.; Chiriva-Internati, M. Influence of obesity on the risk of developing colon cancer. Gut 2006, 55, 285–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Linde, J.A.; Utter, J.; Jeffery, R.W.; Sherwood, N.E.; Pronk, N.P.; Boyle, R.G. Specific food intake, fat and fiber intake, and behavioral correlates of BMI among overweight and obese members of a managed care organization. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 42. [Google Scholar] [CrossRef] [PubMed]
- Hidayat, K.; Yang, C.M.; Shi, B.M. Body fatness at an early age and risk of colorectal cancer. Int. J. Cancer 2018, 142, 729–740. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | EraA (2004–2009) N = 138,650 (%) | EraB (2010–2015) N = 130,748 (%) | p-Value |
|---|---|---|---|
| Age | <0.001 | ||
| 20–49 | 15,502 (11.2) | 16,166(12.4) | |
| 50–69 | 60,288 (43.5) | 62,620 (47.9) | |
| 70+ | 62,860 (45.3) | 51,962 (39.7) | |
| Age (SD) | 66.8 ± 13.8 | 65.5 ± 13.8 | <0.001 |
| Gender | <0.001 | ||
| Female | 67,377 (48.6) | 62,161 (47.5) | |
| Male | 71,273 (51.4) | 68,587 (52.5) | |
| Race | <0.001 | ||
| Hispanic | 12,691 (9.2) | 15,430 (11.8) | |
| American Indian or Alaska Native | 824 (0.6) | 992 (0.8) | |
| Asian or Pacific Islanda | 10,555 (7.6) | 11,483 (8.8) | |
| Black | 15,581 (11.2) | 15,121 (11.6) | |
| Unknown | 338 (0.2) | 631 (0.5) | |
| White | 98,661 (71.2) | 87,091 (66.6) | |
| Health Insurance | <0.001 | ||
| Uninsured | 2193 (1.6) | 4576 (3.6) | |
| Insured | 57,776 (41.7) | 106,695 (81.6) | |
| Medicaid | 7320 (5.3) | 16,993 (13.0) | |
| Unknown | 71,361 (51.5) | 2484 (1.9) | |
| Marital Status | <0.001 | ||
| Married | 76,867 (55.4) | 68,775 (52.6) | |
| Divorced | 12,204 (8.8) | 12,529 (9.6) | |
| Separated/domestic partner | 1269 (0.9) | 1691 (1.3) | |
| Single | 17,950 (13.0) | 21,537 (16.5) | |
| Unknown | 5087 (3.7) | 7153 (5.5) | |
| Widowed | 25,273 (18.2) | 19,063 (14.6) | |
| Geographic Region | <0.001 | ||
| Northeastern | 23,289 (16.8) | 15.54 (15.4) | |
| Midwestern | 13,851 (10.0) | 12,023 (9.2) | |
| Western | 69,131 (49.9) | 66,137 (50.6) | |
| Southern | 32,379 (23.4) | 32,273 (24.7) | |
| Tumor Site | <0.001 | ||
| Right sided | 49,460 (35.7) | 46,018 (35.2) | |
| Left sided | 52,435 (37.8) | 47,508 (36.3) | |
| Transverse | 9416 (6.8) | 9042 (6.9) | |
| Rectum | 25,355 (18.3) | 26,164 (20.0) | |
| Large intestine NOS | 1984 (1.4) | 2016 (1.5) | |
| Tumor Grade | <0.001 | ||
| Low | 110,871 (80.0) | 106,357 (81.4) | |
| High | 27,779 (20.0) | 24,391 (18.7) | |
| Tumor Histology | <0.001 | ||
| Mucinous adenocarcinoma | 12,134 (8.8) | 9106 (7.0) | |
| Adenocarcinoma | 124,564 (89.8) | 119,334 (91.3) | |
| Signet ring cell adenocarcinoma | 1367 (1.0) | 1303 (1.0) | |
| Other (mixed, medullary, adenosquamous) | 585 (0.4) | 1005 (0.8) | |
| Treatment by Surgery | <0.001 | ||
| Surgery performed | 129,337 (93.3) | 118,092 (90.3) | |
| No surgery | 7709 (5.6) | 10,699 (8.2) | |
| Patient Refused | 1167 (0.8) | 1206 (0.9) | |
| Unknown | 437 (0.3) | 751 (0.6) | |
| AJCC Clinical Tumor Stage 6th Edition | <0.001 | ||
| I | 34,181 (24.7) | 30,909 (23.6) | |
| II | 39,495 (28.5) | 35,993 (27.5) | |
| III | 40,319 (29.1) | 39,942 (30.6) | |
| IV | 24,655 (17.8) | 23,904 (18.3) |
| Variables | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Age | Ref (20–49) | ||
| 50–69 | 0.73 | 0.70–0.75 | <0.001 |
| 70 and older | 0.49 | 0.47–0.50 | <0.001 |
| Age (continuous) | |||
| Male | 1.04 | 1.02–1.07 | <0.001 |
| Race | Ref (Hispanic) | ||
| American Indian/Alaska Native | 1.10 | 0.96–1.26 | 0.162 |
| Asian or Pacific Islander | 1.04 | 0.99–1.09 | 0.156 |
| Black | 1.26 | 1.20–1.32 | <0.001 |
| Unknown | 0.22 | 0.16–0.29 | <0.001 |
| White | 1.04 | 1.01–1.08 | 0.028 |
| Health Insurance | Ref (Uninsured) | ||
| Insured | 0.78 | 0.73–0.83 | <0.001 |
| Medicaid | 0.96 | 0.89–1.03 | 0.203 |
| Unknown | 0.86 | 0.80–0.92 | <0.001 |
| Marital Status | Ref (Married) | ||
| Divorced | 1.09 | 1.05–1.14 | <0.001 |
| Separated domestic partner | 0.99 | 0.89–1.09 | 0.818 |
| Single | 1.06 | 1.02–1.09 | 0.001 |
| Unknown | 0.77 | 0.73–0.82 | <0.001 |
| Widowed | 0.93 | 0.90–0.97 | <0.001 |
| EraA | Ref (EraA) | ||
| EraB | 0.93 | 0.91–0.95 | <0.001 |
| Geographic Region (Northeastern) | Ref (Northeastern) | ||
| Midwestern | 1.02 | 0.98–1.07 | 0.356 |
| Western | 1.02 | 0.99–1.05 | 0.237 |
| Southern | 1.05 | 1.02–1.09 | 0.005 |
| Tumor Site | Ref (Right sided) | ||
| Left sided | 1.06 | 1.03–1.09 | <0.001 |
| Transverse | 0.96 | 0.91–1.00 | 0.055 |
| Rectum | 0.50 | 0.48–0.52 | <0.001 |
| Large intestine NOS | 1.63 | 1.51–1.77 | <0.001 |
| Tumor Grade | Ref (Low) | ||
| High | 2.12 | 2.07–2.18 | <0.001 |
| Tumor Histology | Ref (Mucinous adenocarcinoma) | ||
| Adenocarcinoma | 0.84 | 0.81–0.87 | <0.001 |
| Signet ring cell adenocarcinoma | 1.13 | 1.02–1.24 | 0.019 |
| Other (mixed, medullary, adenosquamous) | 0.99 | 0.87–1.12 | 0.846 |
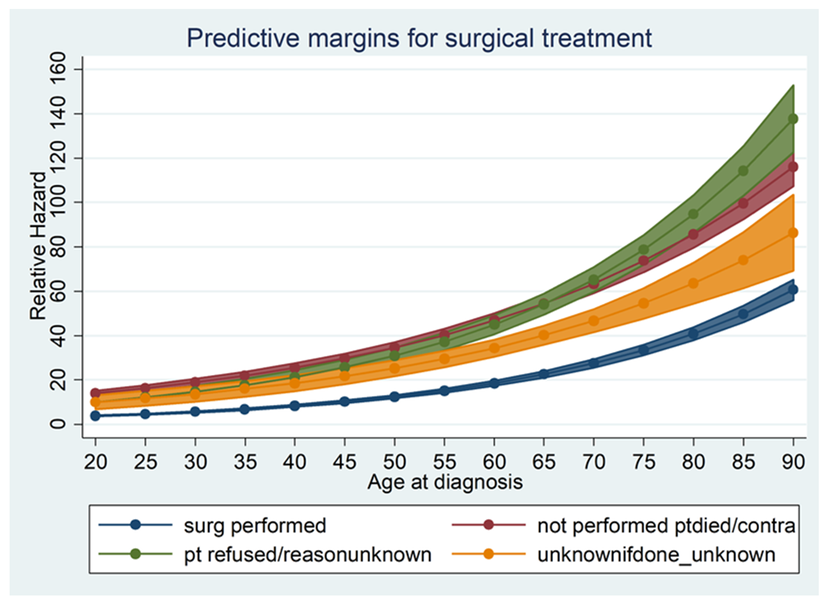
| Treatment by Surgery | Ref (Surgery performed) | ||
| No surgery | 23.14 | 22.27–24.05 | <0.001 |
| Patient Refused | 6.72 | 6.16–7.33 | <0.001 |
| Unknown | 4.54 | 4.00–5.16 | <0.001 |
| Variables | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Age | Ref (20–49) | ||
| 50–69 | 1.21 | 1.19–1.24 | <0.001 |
| 70 and older | 2.63 | 2.57–2.69 | <0.001 |
| Male | 1.20 | 1.18–1.22 | <0.001 |
| Race | Ref (Hispanic) | ||
| American Indian/Alaska Native | 1.09 | 1.00–1.18 | 0.040 |
| Asian or Pacific Islander | 0.90 | 0.88–0.93 | <0.001 |
| Black | 1.17 | 1.14–1.21 | <0.001 |
| Unknown | 0.23 | 0.17–0.29 | <0.001 |
| White | 1.04 | 1.02–1.07 | <0.001 |
| Health Insurance | Ref (Uninsured) | ||
| Insured | 0.78 | 0.75–0.82 | <0.001 |
| Medicaid | 1.06 | 1.01–1.11 | 0.016 |
| Unknown | 0.86 | 0.82–0.89 | <0.001 |
| Marital Status | Ref (Married) | ||
| Divorced | 1.24 | 1.22–1.27 | <0.001 |
| Separated Domestic partner | 1.26 | 1.19–1.34 | <0.001 |
| Single | 1.33 | 1.30–1.35 | <0.001 |
| Unknown | 1.09 | 1.05–1.12 | <0.001 |
| Widowed | 1.46 | 1.43–1.49 | <0.001 |
| Era (EraA) | Ref (EraA) | ||
| EraB (2010–2015) | 0.96 | 0.95–0.98 | <0.001 |
| Geographic Region | Ref (Northeastern) | ||
| Midwestern | 1.04 | 1.02–1.07 | <0.001 |
| Western | 1.03 | 1.01–1.05 | 0.002 |
| Southern | 1.12 | 1.10–1.14 | <0.001 |
| Tumor Site | Ref (Right sided) | ||
| Left sided | 0.91 | 0.90–0.92 | <0.001 |
| Transverse | 0.99 | 0.97–1.02 | 0.543 |
| Rectum | 0.90 | 0.89–0.92 | <0.001 |
| Large intestine NOS | 1.14 | 1.09–1.20 | <0.001 |
| Tumor Grade | Ref (low) | ||
| High | 1.44 | 1.42–1.46 | <0.001 |
| Tumor Histology | Ref (Mucinous adenocarcinoma) | ||
| Adenocarcinoma | 0.86 | 0.84–0.88 | <0.001 |
| Signet ring cell adenocarcinoma | 1.34 | 1.27–1.41 | <0.001 |
| Other (mixed, medullary, adenosquamous) | 1.12 | 1.04–1.20 | 0.004 |
| Treatment by Surgery | Ref (Surgery performed) | ||
| No surgery | 2.42 | 2.37–2.47 | <0.001 |
| Patient refused | 2.54 | 2.41–2.67 | <0.001 |
| Unknown | 1.77 | 1.63–1.92 | <0.001 |
| AJCC Clinical Tumor Stage 6th Edition | Ref (stage 1–3) | ||
| Stage IV | 5.07 | 5.00–5.15 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ulanja, M.B.; Beutler, B.D.; Rishi, M.; Ogala, C.; Patterson, D.R.; Gullapalli, N.; Ambika, S. Colorectal Cancer Presentation and Survival in Young Individuals: A Retrospective Cohort Study. Cancers 2018, 10, 472. https://doi.org/10.3390/cancers10120472
Ulanja MB, Beutler BD, Rishi M, Ogala C, Patterson DR, Gullapalli N, Ambika S. Colorectal Cancer Presentation and Survival in Young Individuals: A Retrospective Cohort Study. Cancers. 2018; 10(12):472. https://doi.org/10.3390/cancers10120472
Chicago/Turabian StyleUlanja, Mark B., Bryce D. Beutler, Mohit Rishi, Chioma Ogala, Darryll R. Patterson, Nageshwara Gullapalli, and Santhosh Ambika. 2018. "Colorectal Cancer Presentation and Survival in Young Individuals: A Retrospective Cohort Study" Cancers 10, no. 12: 472. https://doi.org/10.3390/cancers10120472