
Cerebellar Intermittent Theta-Burst Stimulation and Motor Control Training in Individuals with Cervical Dystonia


Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
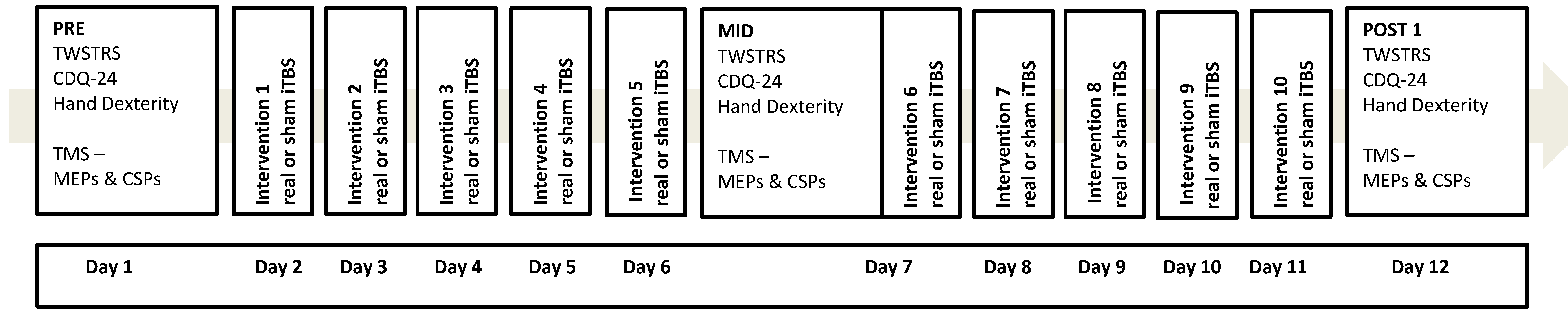
2.2. Experimental Design
2.3. Electromyography (EMG)
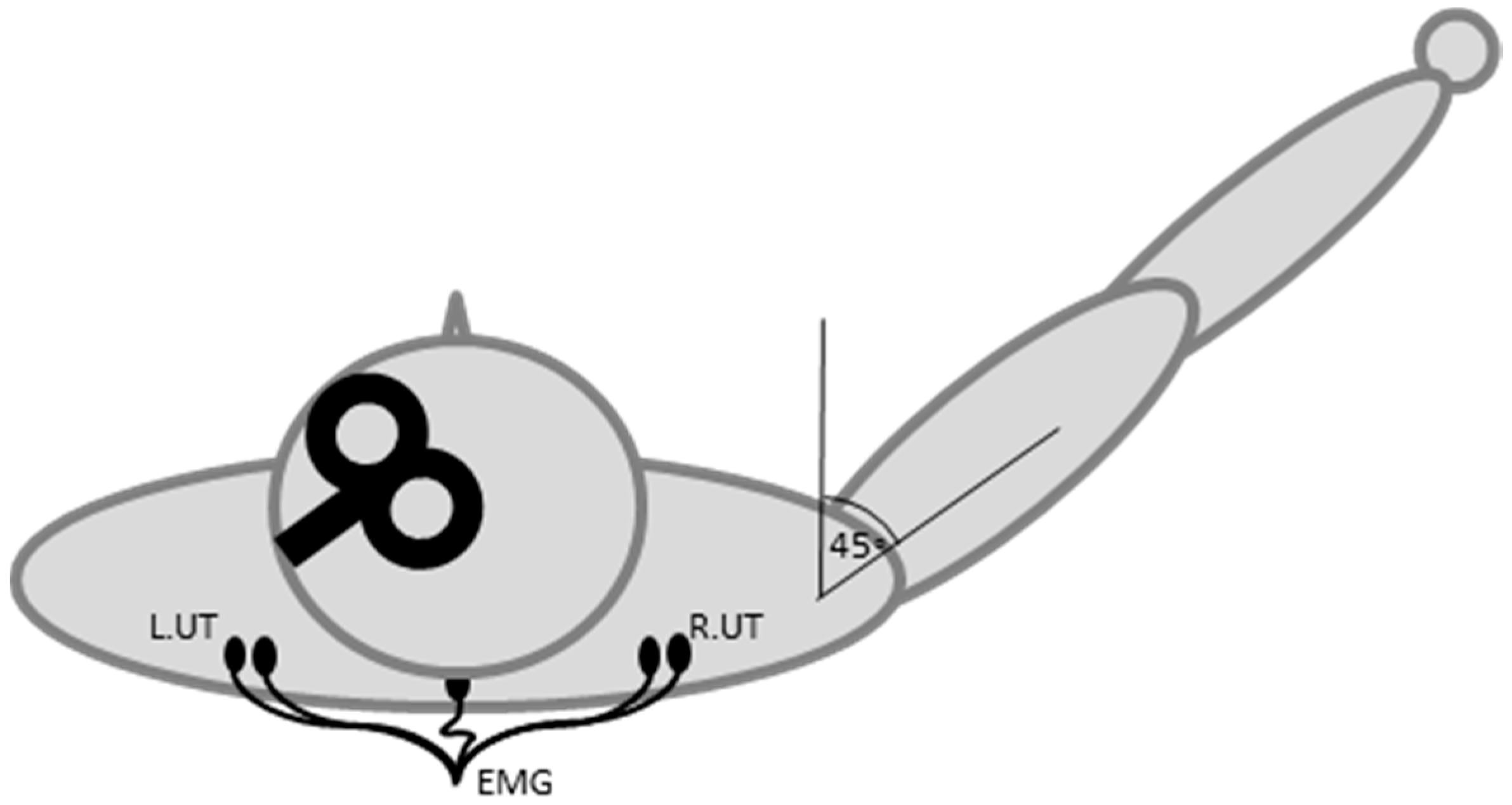
2.4. Transcranial Magnetic Stimulation
2.5. Theta-Burst Stimulation
2.6. Questionnaires and Grooved Pegboard Task
2.7. Data Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Fahn, S. The varied clinical expressions of dystonia. Neurol. Clin. 1984, 2, 541–554. [Google Scholar] [PubMed]
- Albanese, A.; Bhatia, K.; Bressman, S.B.; Delong, M.R.; Fahn, S.; Fung, V.S.; Hallett, M.; Jankovic, J.; Jinnah, H.A.; Klein, C.; et al. Phenomenology and classification of dystonia: A consensus update. Mov. Disord. 2013, 28, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Zetterberg, L.; Aquilonius, S.M.; Lindmark, B. Impact of dystonia on quality of life and health in a Swedish population. Acta Neurol. Scand. 2009, 119, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Jahanshahi, M.; Marsden, C.D. Body concept, disability, and depression in patients with spasmodic torticollis. Behav. Neurol. 1990, 3, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Prudente, C.N.; Pardo, C.A.; Xiao, J.; Hanfelt, J.; Hess, E.J.; Ledoux, M.S.; Jinnah, H.A. Neuropathology of cervical dystonia. Exp. Neurol. 2013, 241, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Jinnah, H.A.; Hess, E.J. A new twist on the anatomy of dystonia: The basal ganglia and the cerebellum? Neurology 2006, 67, 1740–1741. [Google Scholar] [CrossRef] [PubMed]
- Sadnicka, A.; Hoffland, B.S.; Bhatia, K.P.; van de Warrenburg, B.P.; Edwards, M.J. The cerebellum in dystonia—Help or hindrance? Clin. Neurophysiol. 2012, 123, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Song, C.H.; Bernhard, D.; Hess, E.J.; Jinnah, H.A. Subtle microstructural changes of the cerebellum in a knock-in mouse model of DYT1 dystonia. Neurobiol. Dis. 2014, 62, 372–380. [Google Scholar] [CrossRef] [PubMed]
- LeDoux, M.S.; Lorden, J.F.; Ervin, J.M. Cerebellectomy eliminates the motor syndrome of the genetically dystonic rat. Exp. Neurol. 1993, 120, 302–310. [Google Scholar] [CrossRef] [PubMed]
- Raike, R.S.; Pizoli, C.E.; Weisz, C.; van den Maagdenberg, A.M.; Jinnah, H.A.; Hess, E.J. Limited regional cerebellar dysfunction induces focal dystonia in mice. Neurobiol. Dis. 2012, 49C, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Raike, R.S.; Hess, E.J.; Jinnah, H.A. Dystonia and cerebellar degeneration in the leaner mouse mutant. Brain Res. 2015, 1611, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Fremont, R.; Calderon, D.P.; Maleki, S.; Khodakhah, K. Abnormal high-frequency burst firing of cerebellar neurons in rapid-onset dystonia-parkinsonism. J. Neurosci. 2014, 34, 11723–11732. [Google Scholar] [CrossRef] [PubMed]
- Fremont, R.; Tewari, A.; Khodakhah, K. Aberrant Purkinje cell activity is the cause of dystonia in a shRNA-based mouse model of Rapid Onset Dystonia-Parkinsonism. Neurobiol. Dis. 2015, 82, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Prell, T.; Peschel, T.; Kohler, B.; Bokemeyer, M.H.; Dengler, R.; Gunther, A.; Grosskreutz, J. Structural brain abnormalities in cervical dystonia. BMC Neurosci. 2013, 14, 123. [Google Scholar] [CrossRef] [PubMed]
- Argyelan, M.; Carbon, M.; Niethammer, M.; Ulug, A.M.; Voss, H.U.; Bressman, S.B.; Dhawan, V.; Eidelberg, D. Cerebellothalamocortical connectivity regulates penetrance in dystonia. J. Neurosci. 2009, 29, 9740–9747. [Google Scholar] [CrossRef] [PubMed]
- Carbon, M.; Niethammer, M.; Peng, S.; Raymond, D.; Dhawan, V.; Chaly, T.; Ma, Y.; Bressman, S.; Eidelberg, D. Abnormal striatal and thalamic dopamine neurotransmission: Genotype-related features of dystonia. Neurology 2009, 72, 2097–2103. [Google Scholar] [CrossRef] [PubMed]
- Lerner, R.P.; Niethammer, M.; Eidelberg, D. Understanding the anatomy of dystonia: Determinants of penetrance and phenotype. Curr. Neurol. Neurosci. Rep. 2013, 13, 401. [Google Scholar] [CrossRef] [PubMed]
- Vo, A.; Sako, W.; Niethammer, M.; Carbon, M.; Bressman, S.B.; Ulug, A.M.; Eidelberg, D. Thalamocortical Connectivity Correlates with Phenotypic Variability in Dystonia. Cereb. Cortex 2015, 25, 3086–3094. [Google Scholar] [CrossRef] [PubMed]
- Lehericy, S.; Tijssen, M.A.; Vidailhet, M.; Kaji, R.; Meunier, S. The anatomical basis of dystonia: Current view using neuroimaging. Mov. Disord. 2013, 28, 944–957. [Google Scholar] [CrossRef] [PubMed]
- Teo, J.T.; van de Warrenburg, B.P.; Schneider, S.A.; Rothwell, J.C.; Bhatia, K.P. Neurophysiological evidence for cerebellar dysfunction in primary focal dystonia. J. Neurol. Neurosurg. Psychiatry 2009, 80, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Hoffland, B.S.; Kassavetis, P.; Bologna, M.; Teo, J.T.; Bhatia, K.P.; Rothwell, J.C.; Edwards, M.J.; van de Warrenburg, B.P. Cerebellum-dependent associative learning deficits in primary dystonia are normalized by rTMS and practice. Eur. J. Neurosci. 2013, 38, 2166–2171. [Google Scholar] [CrossRef] [PubMed]
- Hubsch, C.; Roze, E.; Popa, T.; Russo, M.; Balachandran, A.; Pradeep, S.; Mueller, F.; Brochard, V.; Quartarone, A.; Degos, B.; et al. Defective cerebellar control of cortical plasticity in writer’s cramp. Brain 2013, 136 Pt 7, 2050–2062. [Google Scholar] [CrossRef] [PubMed]
- Bradnam, L.; Barry, C. The role of the trigeminal sensory nuclear complex in the pathophysiology of craniocervical dystonia. J. Neurosci. 2013, 33, 18358–18367. [Google Scholar] [CrossRef] [PubMed]
- Neychev, V.K.; Gross, R.E.; Lehericy, S.; Hess, E.J.; Jinnah, H.A. The functional neuroanatomy of dystonia. Neurobiol. Dis. 2011, 42, 185–201. [Google Scholar] [CrossRef] [PubMed]
- Prudente, C.N.; Hess, E.J.; Jinnah, H.A. Dystonia as a network disorder: What is the role of the cerebellum? Neuroscience 2014, 260, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Niethammer, M.; Carbon, M.; Argyelan, M.; Eidelberg, D. Hereditary dystonia as a neurodevelopmental circuit disorder: Evidence from neuroimaging. Neurobiol. Dis. 2011, 42, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Filip, P.; Lungu, O.V.; Bares, M. Dystonia and the cerebellum: A new field of interest in movement disorders? Clin. Neurophysiol. 2013, 124, 1269–1276. [Google Scholar] [CrossRef] [PubMed]
- Standaert, D.G. Update on the pathology of dystonia. Neurobiol. Dis. 2011, 42, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Fremont, R.; Arteaga-Bracho, E.E.; Khodakhah, K. Short latency cerebellar modulation of the basal ganglia. Nat. Neurosci. 2014, 17, 1767–1775. [Google Scholar] [CrossRef] [PubMed]
- Malone, A.; Manto, M.; Hass, C. Dissecting the links between cerebellum and dystonia. Cerebellum 2014, 13, 666–668. [Google Scholar] [CrossRef] [PubMed]
- Brusa, L.; Ceravolo, R.; Kiferle, L.; Monteleone, F.; Iani, C.; Schillaci, O.; Stanzione, P.; Koch, G. Metabolic changes induced by theta burst stimulation of the cerebellum in dyskinetic Parkinson’s disease patients. Park. Relat. Disord. 2012, 18, 59–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brusa, L.; Ponzo, V.; Mastropasqua, C.; Picazio, S.; Bonni, S.; Di Lorenzo, F.; Iani, C.; Stefani, A.; Stanzione, P.; Caltagirone, C.; et al. Theta burst stimulation modulates cerebellar-cortical connectivity in patients with progressive supranuclear palsy. Brain Stimul. 2014, 7, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Koch, G.; Brusa, L.; Carrillo, F.; Lo Gerfo, E.; Torriero, S.; Oliveri, M.; Caltagirone, C.; Stanzione, P. Cerebellar magnetic stimulation decreases levodopa-induced dyskinesias in Parkinson disease. Neurology 2009, 73, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Bonni, S.; Ponzo, V.; Caltagirone, C.; Koch, G. Cerebellar theta burst stimulation in stroke patients with ataxia. Funct. Neurol. 2014, 29, 41–45. [Google Scholar] [CrossRef]
- Grimaldi, G.; Argyropoulos, G.P.; Boehringer, A.; Celnik, P.; Edwards, M.J.; Ferrucci, R.; Galea, J.M.; Groiss, S.J.; Hiraoka, K.; Kassavetis, P.; et al. Non-invasive cerebellar stimulation—A consensus paper. Cerebellum 2014, 13, 121–138. [Google Scholar] [CrossRef] [PubMed]
- Koch, G.; Mori, F.; Marconi, B.; Codeca, C.; Pecchioli, C.; Salerno, S.; Torriero, S.; Lo Gerfo, E.; Mir, P.; Oliveri, M.; et al. Changes in intracortical circuits of the human motor cortex following theta burst stimulation of the lateral cerebellum. Clin. Neurophysiol. 2008, 119, 2559–2569. [Google Scholar] [CrossRef] [PubMed]
- Daskalakis, Z.J.; Paradiso, G.O.; Christensen, B.K.; Fitzgerald, P.B.; Gunraj, C.; Chen, R. Exploring the connectivity between the cerebellum and motor cortex in humans. J. Physiol. 2004, 557 Pt 2, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Di Lazzaro, V.; Pilato, F.; Dileone, M.; Profice, P.; Oliviero, A.; Mazzone, P.; Insola, A.; Ranieri, F.; Meglio, M.; Tonali, P.A.; et al. The physiological basis of the effects of intermittent theta burst stimulation of the human motor cortex. J. Physiol. 2008, 586, 3871–3879. [Google Scholar] [CrossRef] [PubMed]
- Di Lazzaro, V.; Pilato, F.; Saturno, E.; Oliviero, A.; Dileone, M.; Mazzone, P.; Insola, A.; Tonali, P.A.; Ranieri, F.; Huang, Y.Z.; et al. Theta-burst repetitive transcranial magnetic stimulation suppresses specific excitatory circuits in the human motor cortex. J. Physiol. 2005, 565 Pt 3, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Z.; Edwards, M.J.; Rounis, E.; Bhatia, K.P.; Rothwell, J.C. Theta burst stimulation of the human motor cortex. Neuron 2005, 45, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Koch, G.; Porcacchia, P.; Ponzo, V.; Carrillo, F.; Caceres-Redondo, M.T.; Brusa, L.; Desiato, M.T.; Arciprete, F.; Di Lorenzo, F.; Pisani, A.; et al. Effects of two weeks of cerebellar theta burst stimulation in cervical dystonia patients. Brain Stimul. 2014, 7, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Bradnam, L.V.; Graetz, L.J.; McDonnell, M.N.; Ridding, M.C. Anodal transcranial direct current stimulation to the cerebellum improves handwriting and cyclic drawing kinematics in focal hand dystonia. Front. Hum. Neurosci. 2015, 9, 286. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin Neurophysiol. 2009, 120, 2008–2039. [Google Scholar] [CrossRef] [PubMed]
- Taves, D.R. Minimization: A new method of assigning patients to treatment and control groups. Clin. Pharmacol. Ther. 1974, 15, 443–453. [Google Scholar] [CrossRef] [PubMed]
- Consky, E.; Lang, A. Clinical Assessments of patients with Cervical Dystonia. In Therapy with Botulinum Toxin; Jankovic, J.H.M., Ed.; Marcel Dekker Inc.: New York, NY, USA, 1994. [Google Scholar]
- Alexander, C.; Miley, R.; Stynes, S.; Harrison, P.J. Differential control of the scapulothoracic muscles in humans. J. Physiol. 2007, 580 Pt 3, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Rossini, P.M.; Barker, A.T.; Berardelli, A.; Caramia, M.D.; Caruso, G.; Cracco, R.Q.; Dimitrijević, M.R.; Hallett, M.; Katayama, Y.; Lücking, C.H.; et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord and roots: basic principles and procedures for routine clinical application. Report of an IFCN committee. Electroencephalogr. Clin. Neurophysiol. 1994, 91, 79–92. [Google Scholar] [CrossRef]
- Koch, G.; Oliveri, M.; Torriero, S.; Salerno, S.; Lo Gerfo, E.; Caltagirone, C. Repetitive TMS of cerebellum interferes with millisecond time processing. Exp. Brain Res. 2007, 179, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, L.; Fasanelli, M.; Andreatta, O.; Bonifati, D.M.; Barchiesi, G.; Caruana, F. Your actions in my cerebellum: Subclinical deficits in action observation in patients with unilateral chronic cerebellar stroke. Cerebellum 2012, 11, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, A.M.; Chiricozzi, F.R.; Clausi, S.; Lupo, M.; Molinari, M.; Leggio, M.G. The cerebellar cognitive profile. Brain 2011, 134 Pt 12, 3672–3686. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, M.; Sadato, N.; Kochiyama, T.; Nakamura, S.; Naito, E.; Matsunami, K.; Kawashima, R.; Fukuda, H.; Yonekura, Y. Role of the cerebellum in implicit motor skill learning: A PET study. Brain Res. Bull. 2004, 63, 471–483. [Google Scholar] [CrossRef] [PubMed]
- Hardwick, R.M.; Rottschy, C.; Miall, R.C.; Eickhoff, S.B. A quantitative meta-analysis and review of motor learning in the human brain. Neuroimage 2013, 67, 283–297. [Google Scholar] [CrossRef] [PubMed]
- Muller, J.; Wissel, J.; Kemmler, G.; Voller, B.; Bodner, T.; Schneider, A.; Wenning, G.K.; Poewe, W. Craniocervical dystonia questionnaire (CDQ-24): Development and validation of a disease-specific quality of life instrument. J. Neurol. Neurosurg. Psychiatry 2004, 75, 749–753. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, G.M.; Feinn, R. Using Effect Size-or Why the p Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Bradnam, L.V.; Stinear, C.M.; Lewis, G.N.; Byblow, W.D. Task-dependent modulation of inputs to proximal upper limb following transcranial direct current stimulation of primary motor cortex. J. Neurophysiol. 2010, 103, 2382–2389. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L.V.; Stinear, C.M.; Lewis, G.N.; Byblow, W.D. Task-dependent modulation of propriospinal inputs to human shoulder. J. Neurophysiol. 2008, 100, 2109–2114. [Google Scholar] [CrossRef] [PubMed]
- Bradnam, L.; Shanahan, E.M.; Hendy, K.; Reed, A.; Skipworth, T.; Visser, A.; Lennon, S. Afferent inhibition and cortical silent periods in shoulder primary motor cortex and effect of a suprascapular nerve block in people experiencing chronic shoulder pain. Clin. Neurophysiol. 2016, 127, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Silbert, B.I.; Thickbroom, G.W. Conditioning the cortical silent period with paired transcranial magnetic stimulation. Brain Stimul. 2013, 6, 541–544. [Google Scholar] [CrossRef] [PubMed]
- Rom, D.M. A sequentially rejective test procedure based on a modified Bonferroni inequality. Biometrika 1990, 77, 663–665. [Google Scholar] [CrossRef]
- Volkmann, J.; Mueller, J.; Deuschl, G.; Kuhn, A.A.; Krauss, J.K.; Poewe, W.; Timmermann, L.; Falk, D.; Kupsch, A.; Kivi, A.; et al. Pallidal neurostimulation in patients with medication-refractory cervical dystonia: A randomised, sham-controlled trial. Lancet Neurol. 2014, 13, 875–884. [Google Scholar] [CrossRef]
- Boyce, M.J.; Canning, C.G.; Mahant, N.; Morris, J.; Latimer, J.; Fung, V.S. Active exercise for individuals with cervical dystonia: A pilot randomized controlled trial. Clin. Rehabil. 2013, 27, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Bradnam, L.V.; Frasca, J.; Kimberley, T.J. Direct current stimulation of primary motor cortex and cerebellum and botulinum toxin a injections in a person with cervical dystonia. Brain Stimul. 2014, 7, 909–911. [Google Scholar] [CrossRef] [PubMed]
- Truong, D.; Brodsky, M.; Lew, M.; Brashear, A.; Jankovic, J.; Molho, E.; Orlova, O.; Timerbaeva, S. Global Dysport Cervical Dystonia Study Group. Long-term efficacy and safety of botulinum toxin type A (Dysport) in cervical dystonia. Park. Relat. Disord. 2010, 16, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Truong, D.; Duane, D.D.; Jankovic, J.; Singer, C.; Seeberger, L.C.; Comella, C.L.; Lew, M.F.; Rodnitzky, R.L.; Danisi, F.O.; Sutton, J.P.; et al. Efficacy and safety of botulinum type A toxin (Dysport) in cervical dystonia: Results of the first US randomized, double-blind, placebo-controlled study. Mov. Disord. 2005, 20, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, H.H.; Pagan, F.; Danisi, F.; Greeley, D.; Jankovic, J.; Verma, A.; Sethi, K.; Pappert, E. Prospective Study Evaluating IncobotulinumtoxinA for Cervical Dystonia or Blepharospasm: Interim Results from the First 145 Subjects with Cervical Dystonia. Tremor Other Hyperkinet. Mov. (N.Y.) 2013, 3. [Google Scholar] [CrossRef]
- Koch, G. Repetitive transcranial magnetic stimulation: A tool for human cerebellar plasticity. Funct. Neurol. 2010, 25, 159–163. [Google Scholar] [PubMed]
- Ugawa, Y.; Uesaka, Y.; Terao, Y.; Hanajima, R.; Kanazawa, I. Magnetic stimulation over the cerebellum in humans. Ann. Neurol. 1995, 37, 703–713. [Google Scholar] [CrossRef] [PubMed]
- Todorov, B.; Kros, L.; Shyti, R.; Plak, P.; Haasdijk, E.D.; Raike, R.S.; Frants, R.R.; Hess, E.J.; Hoebeek, F.E.; De Zeeuw, C.I. Purkinje cell-specific ablation of Cav2.1 channels is sufficient to cause cerebellar ataxia in mice. Cerebellum 2012, 11, 246–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jorntell, H.; Hansel, C. Synaptic memories upside down: bidirectional plasticity at cerebellar parallel fiber-Purkinje cell synapses. Neuron 2006, 52, 227–238. [Google Scholar] [CrossRef] [PubMed]
- Lamont, M.G.; Weber, J.T. The role of calcium in synaptic plasticity and motor learning in the cerebellar cortex. Neurosci. Biobehav. Rev. 2012, 36, 1153–1162. [Google Scholar] [CrossRef] [PubMed]
- Hoogendam, J.M.; Ramakers, G.M.; Di Lazzaro, V. Physiology of repetitive transcranial magnetic stimulation of the human brain. Brain Stimul. 2010, 3, 95–118. [Google Scholar] [CrossRef] [PubMed]
- Cardenas-Morales, L.; Nowak, D.A.; Kammer, T.; Wolf, R.C.; Schonfeldt-Lecuona, C. Mechanisms and applications of theta-burst rTMS on the human motor cortex. Brain Topogr. 2010, 22, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, A.G.; Zee, D.S.; Jinnah, H.A. Oscillatory head movements in cervical dystonia: Dystonia, tremor, or both? Mov. Disord. 2015, 30, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, A.G.; Wong, A.L.; Zee, D.S.; Jinnah, H.A. Keeping your head on target. J. Neurosci. 2013, 33, 11281–11295. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, A.G.; Wong, A.; Zee, D.S.; Jinnah, H.A. Why are voluntary head movements in cervical dystonia slow? Park. Relat. Disord. 2015, 21, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Doeltgen, S.H.; Young, J.; Bradnam, L.V. Anodal Direct Current Stimulation of the Cerebellum Reduces Cerebellar Brain Inhibition but Does Not Influence Afferent Input from the Hand or Face in Healthy Adults. Cerebellum 2015. [Google Scholar] [CrossRef] [PubMed]
- Bologna, M.; Di Biasio, F.; Conte, A.; Iezzi, E.; Modugno, N.; Berardelli, A. Effects of cerebellar continuous theta burst stimulation on resting tremor in Parkinson’s disease. Park. Relat. Disord. 2015, 21, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Bologna, M.; Rocchi, L.; Leodori, G.; Paparella, G.; Conte, A.; Kahn, N.; Fabbrini, G.; Berardelli, A. Cerebellar continuous theta burst stimulation in essential tremor. Cerebellum 2015, 14, 133–141. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (year) | Sex | Dystonia Type | Time since Dystonia onset (year) | TWSTRS 0-85 | CDQ24 0-96 | BTXN |
|---|---|---|---|---|---|---|
| Real iTBS Group | ||||||
| 46 | F | Left Rotation | 10 | 58.8 | 48.9 | Yes |
| 58 | F | Right Rotation | 15 | 40.3 | 31.3 | No |
| 63 | F | Right Rotation | 8 | 45.0 | 17.7 | No |
| 57 | M | Right Rotation | 3 | 30.3 | 33.3 | Yes |
| 42 | F | Left Rotation/Right Side Flexion | 4 | 48.3 | 44.8 | No |
| 38 | M | Right Rotation | 2 | 23.8 | 34.4 | Yes |
| 51 | F | Right Rotation | 4 | 42.5 | 54.1 | Yes |
| 49 | M | Left Rotation | 5 | 44.0 | 51.04 | Yes |
| Mean ± SD | ||||||
| 50.5 ± 8.5 | 6.4 ± 4.4 | 41.6 ± 10.7 | 39.4 ± 12.4 | |||
| Sham iTBS Group | ||||||
| 72 | M | Left Rotation | 8 | 38.0 | 20.8 | Yes |
| 66 | F | Left Rotation | 5 | 47.5 | 50 | No |
| 43 | M | Left SideFlexion/Flexion | 2 | 44.5 | 57.3 | Yes |
| 62 | M | Left Rotation | 3 | 40.3 | 38.5 | Yes |
| 28 | F | Right Rotation | 5 | 26.3 | 13.5 | Yes |
| 62 | F | Left Rotation | 12 | 70.0 | 51.1 | Yes |
| 48 | F | Left Rotation | 3 | 27.5 | 42.7 | Yes |
| 46 | F | Right Rotation | 30 | 42.75 | 81.25 | No |
| Mean ± SD | ||||||
| 53.4 ± 14.6 | 8.5 ± 9.3 | 42.1 ± 13.6 | 44.4 ± 21.21 | |||
| Pre | Mid | Effect Size | Post 1 | Effect Size | Post 2 | Effect Size | Post 3 | Effect Size | |
|---|---|---|---|---|---|---|---|---|---|
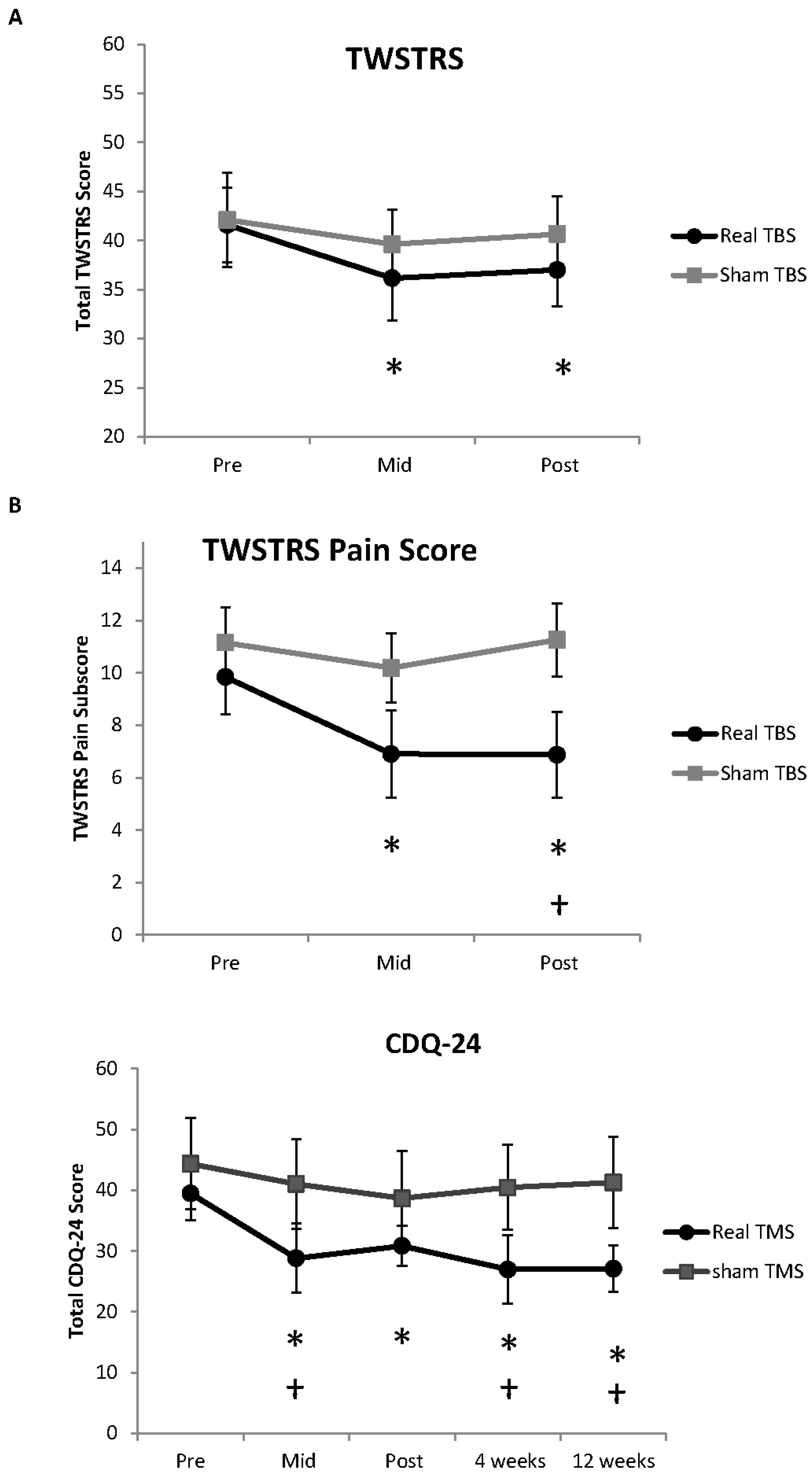
| TWSTRS | 41.59 ± 3.8 | 36.12 ± 4.3 | 0.48 (S) | 37.0 ± 3.7 | 0.43 (S) | N/A | N/A | ||
| TWSTRS Pain | 9.84375 ± 1.4 | 6.90625 ± 1.7 | 0.67 (M) | 6.875 ± 1.6 | 0.68 (M) | N/A | N/A | ||
| CDQ-24 | 39.45 ± 4.4 | 28.81 ± 4.3 | 0.74 (M) | 30.84 ± 3.4 | 0.78 (M) | 26.89 ± 5.7 | 0.88 (L) | 27.09 ± 3.8 | 1.06 (L) |
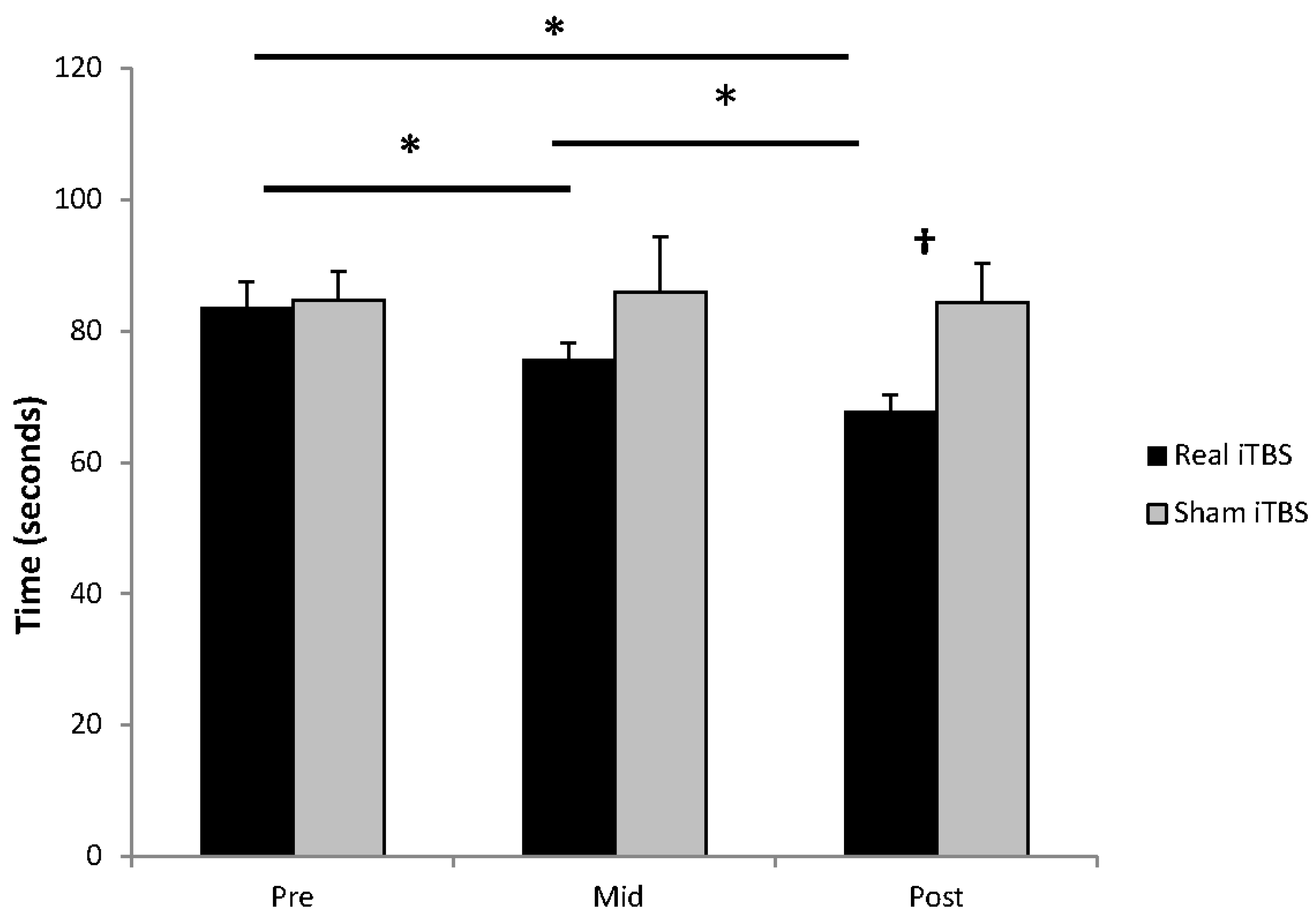
| Pegboard (seconds) | 83.63 ± 3.8 | 75.75 ± 2.4 | 0.87 (L) | 67.88 ± 2.5 | 1.74 (L) | N/A | N/A |
| Contralateral Upper Trapezius | Ipsilateral Upper Trapezius | |||||
|---|---|---|---|---|---|---|
| MEP area (mV.S) | Pre | Mid | Post | Pre | Mid | Post |
| Real iTBS | 1.85 ± 0.37 | 1.35 ± 0.21 | 1.34 ± 0.22 | 1.69 ± 0.17 | 2.15 ± 0.43 | 1.64 ± 0.30 |
| Sham iTBS | 1.53 ± 0.21 | 1.62 ± 0.23 | 1.66 ± 0.28 | 1.93 ± 0.42 | 1.84 ± 0.27 | 2.09 ± 0.44 |
| CSP length (ms) | Pre | Mid | Post | Pre | Mid | Post |
| Real iTBS | 95.71 ± 9.93 | 85.04 ± 8.02 | 90.79 ± 5.98 | 111.73 ± 7.64 | 105.81 ± 10.47 | 107.42 ± 10.25 |
| Sham iTBS | 90.04 ± 8.93 | 77.88 ± 5.72 | 81.44 ± 4.86 | 96.32 ± 9.63 | 93.56 ± 7.12 | 108.62 ± 12.83 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bradnam, L.V.; McDonnell, M.N.; Ridding, M.C. Cerebellar Intermittent Theta-Burst Stimulation and Motor Control Training in Individuals with Cervical Dystonia. Brain Sci. 2016, 6, 56. https://doi.org/10.3390/brainsci6040056
Bradnam LV, McDonnell MN, Ridding MC. Cerebellar Intermittent Theta-Burst Stimulation and Motor Control Training in Individuals with Cervical Dystonia. Brain Sciences. 2016; 6(4):56. https://doi.org/10.3390/brainsci6040056
Chicago/Turabian StyleBradnam, Lynley V., Michelle N. McDonnell, and Michael C. Ridding. 2016. "Cerebellar Intermittent Theta-Burst Stimulation and Motor Control Training in Individuals with Cervical Dystonia" Brain Sciences 6, no. 4: 56. https://doi.org/10.3390/brainsci6040056