

Mediating Effect of Loneliness in the Relationship between Depressive Symptoms and Cognitive Frailty in Community-Dwelling Older Adults
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Participants
2.2. Measurement
2.2.1. Cognitive Frailty
2.2.2. Depression Symptoms
2.2.3. Loneliness
2.2.4. Control Variables
2.3. Statistical Analysis
2.4. Ethical Consideration
3. Results
3.1. Characteristics of Participants
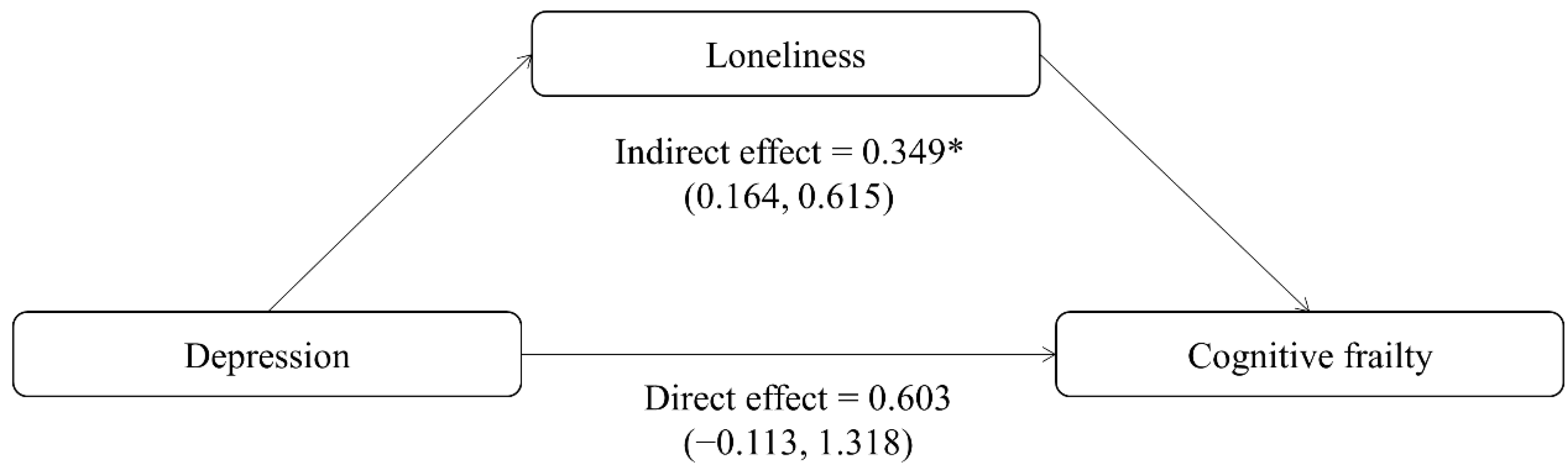
3.2. Effect of Loneliness on the Association between Depression and Cognitive Frailty
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; van Kan, G.A.; Ousset, P.J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Rivan, N.F.M.; Singh, D.K.A.; Shahar, S.; Wen, G.J.; Rajab, N.F.; Din, N.C.; Mahadzir, H.; Kamaruddin, M.Z.A. Cognitive frailty is a robust predictor of falls, injuries, and disability among community-dwelling older adults. BMC Geriatr. 2021, 21, 593. [Google Scholar] [CrossRef]
- Sugimoto, T.; Arai, H.; Sakurai, T. An update on cognitive frailty: Its definition, impact, associated factors and underlying mechanisms, and interventions. Geriatr. Gerontol Int. 2022, 22, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Doi, T.; Lee, S.; Makizako, H.; Chen, L.K.; Arai, H. Cognitive Frailty Predicts Incident Dementia among Community-Dwelling Older People. J. Clin. Med. 2018, 7, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Awata, S.; Watanabe, Y.; Kojima, N.; Osuka, Y.; Motokawa, K.; Sakuma, N.; Inagaki, H.; Edahiro, A.; Hosoi, E.; et al. Cognitive frailty in community-dwelling older Japanese people: Prevalence and its association with falls. Geriatr. Gerontol Int. 2019, 19, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Li, G.; Wang, X.; Zheng, L.; Wang, C.; Wang, C.; Chen, L. Prevalence of cognitive frailty among community-dwelling older adults: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2022, 125, 104112. [Google Scholar] [CrossRef]
- Facal, D.; Burgo, C.; Spuch, C.; Gaspar, P.; Campos-Magdaleno, M. Cognitive Frailty: An Update. Front Psychol. 2021, 12, 813398. [Google Scholar] [CrossRef]
- Vaughan, L.; Corbin, A.L.; Goveas, J.S. Depression and frailty in later life: A systematic review. Clin. Interv. Aging 2015, 10, 1947–1958. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Wang, C.; Qiao, X.; Si, H.; Jin, Y. Sleep quality, depression and frailty among Chinese community-dwelling older adults. Geriatr. Nurs. 2021, 42, 714–720. [Google Scholar] [CrossRef]
- Kwan, R.Y.C.; Leung, A.Y.M.; Yee, A.; Lau, L.T.; Xu, X.Y.; Dai, D.L.K. Cognitive Frailty and Its Association with Nutrition and Depression in Community-Dwelling Older People. J. Nutr. Health Aging 2019, 23, 943–948. [Google Scholar] [CrossRef]
- Yuan, M.; Xu, C.; Fang, Y. The transitions and predictors of cognitive frailty with multi-state Markov model: A cohort study. BMC Geriatr. 2022, 22, 550. [Google Scholar] [CrossRef]
- Yang, F.; Gu, D. Widowhood, widowhood duration, and loneliness among older adults in China. Soc. Sci. Med. 2021, 283, 114179. [Google Scholar] [CrossRef]
- Surkalim, D.L.; Luo, M.; Eres, R.; Gebel, K.; van Buskirk, J.; Bauman, A.; Ding, D. The prevalence of loneliness across 113 countries: Systematic review and meta-analysis. BMJ 2022, 376, e067068. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Cacioppo, S. The growing problem of loneliness. Lancet 2018, 391, 426. [Google Scholar] [CrossRef] [Green Version]
- Gale, C.R.; Westbury, L.; Cooper, C. Social isolation and loneliness as risk factors for the progression of frailty: The English Longitudinal Study of Ageing. Age Ageing 2018, 47, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Chew, S.Y. Loneliness experience among cognitively-intact elderly nursing home residents in Singapore—An exploratory mixed methods study. Arch. Gerontol Geriatr. 2022, 98, 104572. [Google Scholar] [CrossRef]
- Sha, S.; Xu, Y.; Chen, L. Loneliness as a risk factor for frailty transition among older Chinese people. BMC Geriatr. 2020, 20, 300. [Google Scholar] [CrossRef]
- Wei, K.; Liu, Y.; Yang, J.; Gu, N.; Cao, X.; Zhao, X.; Jiang, L.; Li, C. Living arrangement modifies the associations of loneliness with adverse health outcomes in older adults: Evidence from the CLHLS. BMC Geriatr. 2022, 22, 59. [Google Scholar] [CrossRef]
- Smith, L.; Bloska, J.; Jacob, L.; Barnett, Y.; Butler, L.; Trott, M.; Odell-Miller, H.; Veronese, N.; Kostev, K.; Bettac, E.L.; et al. Is loneliness associated with mild cognitive impairment in low- and middle-income countries? Int. J. Geriatr. Psychiatry 2021, 36, 1345–1353. [Google Scholar] [CrossRef]
- Wang, H.; Lee, C.; Hunter, S.; Fleming, J.; Brayne, C.; Collaboration, C.C.S. Longitudinal analysis of the impact of loneliness on cognitive function over a 20-year follow-up. Aging Ment. Health 2020, 24, 1815–1821. [Google Scholar] [CrossRef]
- Dahlberg, L.; McKee, K.J.; Frank, A.; Naseer, M. A systematic review of longitudinal risk factors for loneliness in older adults. Aging Ment. Health 2022, 26, 225–249. [Google Scholar] [CrossRef]
- Ojagbemi, A.; Bello, T.; Gureje, O. The roles of depression and social relationships in the onset and course of loneliness amongst Nigerian elders. Int. J. Geriatr. Psychiatry 2021, 36, 547–557. [Google Scholar] [CrossRef]
- Isik, K.; Basogul, C.; Yildirim, H. The relationship between perceived loneliness and depression in the elderly and influencing factors. Perspect. Psychiatr. Care 2021, 57, 351–357. [Google Scholar] [CrossRef]
- Abellan van Kan, G.; Rolland, Y.M.; Morley, J.E.; Vellas, B. Frailty: Toward a clinical definition. J. Am. Med. Dir. Assoc. 2008, 9, 71–72. [Google Scholar] [CrossRef]
- Dong, L.; Qiao, X.; Tian, X.; Liu, N.; Jin, Y.; Si, H.; Wang, C. Cross-Cultural Adaptation and Validation of the FRAIL Scale in Chinese Community-Dwelling Older Adults. J. Am. Med. Dir. Assoc. 2018, 19, 12–17. [Google Scholar] [CrossRef]
- Woo, J.; Leung, J.; Morley, J.E. Comparison of frailty indicators based on clinical phenotype and the multiple deficit approach in predicting mortality and physical limitation. J. Am. Geriatr. Soc. 2012, 60, 1478–1486. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Wang, C.; Zhang, J.; Hu, C.; Wang, Y. Prevalence and Risk Factors for Cognitive Frailty in Aging Hypertensive Patients in China. Brain Sci. 2021, 11, 1018. [Google Scholar] [CrossRef]
- Hoyl, M.T.; Alessi, C.A.; Harker, J.O.; Josephson, K.R.; Pietruszka, F.M.; Koelfgen, M.; Mervis, J.R.; Fitten, L.J.; Rubenstein, L.Z. Development and testing of a five-item version of the Geriatric Depression Scale. J. Am. Geriatr. Soc. 1999, 47, 873–878. [Google Scholar] [CrossRef]
- Rinaldi, P.; Mecocci, P.; Benedetti, C.; Ercolani, S.; Bregnocchi, M.; Menculini, G.; Catani, M.; Senin, U.; Cherubini, A. Validation of the five-item geriatric depression scale in elderly subjects in three different settings. J. Am. Geriatr. Soc. 2003, 51, 694–698. [Google Scholar] [CrossRef]
- Hays, R.D.; DiMatteo, M.R. A short-form measure of loneliness. J. Pers. Assess 1987, 51, 69–81. [Google Scholar] [CrossRef]
- Russell, D.W. UCLA Loneliness Scale (Version 3): Reliability, validity, and factor structure. J. Pers. Assess 1996, 66, 20–40. [Google Scholar] [CrossRef]
- Ren, L.; Chang, L.; Kang, Y.; Zhao, Y.; Chen, F.; Pei, L. Gender-Specific Association Between Sleep Duration and Body Mass Index in Rural China. Front. Endocrinol. 2022, 13, 877100. [Google Scholar] [CrossRef]
- Hou, P.; Xue, H.P.; Mao, X.E.; Li, Y.N.; Wu, L.F.; Liu, Y.B. Inflammation markers are associated with frailty in elderly patients with coronary heart disease. Aging 2018, 10, 2636–2645. [Google Scholar] [CrossRef]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef] [Green Version]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. The diagnostic validity of the Athens Insomnia Scale. J. Psychosom. Res. 2003, 55, 263–267. [Google Scholar] [CrossRef]
- Mackinnon, D.P.; Dwyer, J.H. Estimating mediated effects in prevention studies. Eval. Rev. 1993, 17, 144–158. [Google Scholar] [CrossRef]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Zhang, T.; Ren, Y.; Shen, P.; Jiang, S.; Yang, Y.; Wang, Y.; Li, Z.; Yang, Y. Prevalence and Associated Risk Factors of Cognitive Frailty: A Systematic Review and Meta-Analysis. Front. Aging Neurosci 2021, 13, 755926. [Google Scholar] [CrossRef]
- Zhao, D.; Li, J.; Fu, P.; Hao, W.; Yuan, Y.; Yu, C.; Jing, Z.; Wang, Y.; Zhou, C. Cognitive frailty and suicidal ideation among Chinese rural empty-nest older adults: Parent-child geographic proximity as a possible moderator? J. Affect. Disord. 2021, 282, 348–353. [Google Scholar] [CrossRef]
- Li, C.L.; Chang, H.Y.; Stanaway, F.F. Combined effects of frailty status and cognitive impairment on health-related quality of life among community dwelling older adults. Arch. Gerontol Geriatr. 2020, 87, 103999. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Pardo, E.; Facal, D.; Campos-Magdaleno, M.; Pereiro, A.X.; Juncos-Rabadan, O. Prevalence of Cognitive Frailty, Do Psychosocial-Related Factors Matter? Brain Sci. 2020, 10, 968. [Google Scholar] [CrossRef] [PubMed]
- Lotfaliany, M.; Hoare, E.; Jacka, F.N.; Kowal, P.; Berk, M.; Mohebbi, M. Variation in the prevalence of depression and patterns of association, sociodemographic and lifestyle factors in community-dwelling older adults in six low- and middle-income countries. J. Affect Disord. 2019, 251, 218–226. [Google Scholar] [CrossRef]
- Tang, T.; Jiang, J.; Tang, X. Prevalence of depressive symptoms among older adults in mainland China: A systematic review and meta-analysis. J. Affect Disord. 2021, 293, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, Y.C.; Chen, C.Y.; Hsiao, Y.C.; Lin, C.C. A longitudinal, cross-lagged panel analysis of loneliness and depression among community-based older adults. J. Elder. Abuse Negl. 2019, 31, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Flores, M.E.; Forjaz, M.J.; Fernandez-Mayoralas, G.; Rojo-Perez, F.; Martinez-Martin, P. Factors associated with loneliness of noninstitutionalized and institutionalized older adults. J. Aging Health 2011, 23, 177–194. [Google Scholar] [CrossRef]
- Ojagbemi, A.; Gureje, O. Social relationships and the association of loneliness with major depressive disorder in the Ibadan study of aging. World Soc. Psychiatry 2019, 1, 82–88. [Google Scholar] [CrossRef]
- Ge, L.; Yap, C.W.; Heng, B.H. Associations of social isolation, social participation, and loneliness with frailty in older adults in Singapore: A panel data analysis. BMC Geriatr. 2022, 22, 26. [Google Scholar] [CrossRef]
- Vancampfort, D.; Lara, E.; Smith, L.; Rosenbaum, S.; Firth, J.; Stubbs, B.; Hallgren, M.; Koyanagi, A. Physical activity and loneliness among adults aged 50 years or older in six low- and middle-income countries. Int. J. Geriatr. Psychiatry 2019, 34, 1855–1864. [Google Scholar] [CrossRef]
- Lynch, D.H.; Spangler, H.B.; Franz, J.R.; Krupenevich, R.L.; Kim, H.; Nissman, D.; Zhang, J.; Li, Y.Y.; Sumner, S.; Batsis, J.A. Multimodal Diagnostic Approaches to Advance Precision Medicine in Sarcopenia and Frailty. Nutrients 2022, 14, 1384. [Google Scholar] [CrossRef]
- Pegorari, M.S.; Silva, C.F.R.; Araujo, F.C.; Silva, J.S.D.; Ohara, D.G.; Matos, A.P.; Matos, A.P.; Pinto, A. Factors associated with social isolation and loneliness in community-dwelling older adults during pandemic times: A cross-sectional study. Rev. Soc. Bras. Med. Trop. 2021, 54, e01952020. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N.; Stern, Y. Cognitive reserve and lifestyle. J. Clin. Exp. Neuropsychol. 2003, 25, 625–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lara, E.; Martin-Maria, N.; De la Torre-Luque, A.; Koyanagi, A.; Vancampfort, D.; Izquierdo, A.; Miret, M. Does loneliness contribute to mild cognitive impairment and dementia? A systematic review and meta-analysis of longitudinal studies. Ageing Res. Rev. 2019, 52, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Furtado, G.E.; Caldo, A.; Rieping, T.; Filaire, E.; Hogervorst, E.; Teixeira, A.M.B.; Ferreira, J.P. Physical frailty and cognitive status over-60 age populations: A systematic review with meta-analysis. Arch. Gerontol. Geriatr. 2018, 78, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Cruwys, T.; Haslam, C.; Rathbone, J.A.; Williams, E.; Haslam, S.A.; Walter, Z.C. Groups 4 Health versus cognitive-behavioural therapy for depression and loneliness in young people: Randomised phase 3 non-inferiority trial with 12-month follow-up. Br. J. Psychiatry 2022, 220, 140–147. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total | Cognitive Frailty | X2/t | p-Value | |
|---|---|---|---|---|---|
| No | Yes | ||||
| Observations | 527 (100.0) | 423 (80.3) | 104 (19.7) | ||
| Depression symptoms | 12.774 | <0.001 | |||
| Without depression symptoms | 475 (90.1) | 391 (82.3) | 84 (17.7) | ||
| With depression symptoms | 52 (9.9) | 32 (61.5) | 20 (38.5) | ||
| Loneliness | 14.2 ± 4.3 | 13.7 ± 4.1 | 16.0 ± 4.4 | −4.953 | <0.001 |
| Gender | 0.012 | 0.914 | |||
| Male | 261 (49.5) | 209 (80.1) | 52 (19.9) | ||
| Female | 266 (50.5) | 214 (80.5) | 52 (19.5) | ||
| Age | 2.396 | 0.122 | |||
| (60–69) years | 279 (52.9) | 231 (82.8) | 48 (17.2) | ||
| ≥70 years | 248 (47.1) | 192 (77.4) | 56 (22.6) | ||
| BMI (kg/m2) | 7.852 | 0.005 | |||
| 18.5–23.9 | 364 (69.1) | 304 (83.5) | 60 (16.5) | ||
| <18.5 or >23.9 | 163 (30.9) | 119 (73.0) | 44 (27.0) | ||
| Education | 0.092 | 0.761 | |||
| Primary school or below | 316 (60.0) | 255 (80.7) | 61 (19.3) | ||
| Junior high school and above | 211 (40.0) | 168 (79.6) | 43 (20.4) | ||
| Marital status | 0.002 | 0.966 | |||
| Married | 386 (73.2) | 310 (80.3) | 76 (19.7) | ||
| Single | 141 (26.8) | 113 (80.1) | 28 (19.9) | ||
| Household arrangement | 20.337 | <0.001 | |||
| Empty-nest elderly | 89 (16.9) | 56 (62.9) | 33 (37.1) | ||
| Non-empty-nest elderly | 438 (83.1) | 367 (83.8) | 71 (16.2) | ||
| Monthly income (CNY) | 21.332 | <0.001 | |||
| <2000 | 350 (66.4) | 261 (74.6) | 89 (25.4) | ||
| ≥2000 | 177 (33.6) | 162 (91.5) | 15 (8.5) | ||
| Cigarette smoking | 4.465 | 0.035 | |||
| No | 415 (78.7) | 341 (82.2) | 74 (17.8) | ||
| Yes | 112 (21.3) | 82 (73.2) | 30 (26.8) | ||
| Alcohol drinking | 1.822 | 0.177 | |||
| No | 373 (70.8) | 305 (81.8) | 68 (18.2) | ||
| Yes | 154 (29.2) | 118 (76.6) | 36 (23.4) | ||
| Polypharmacy | 8.875 | 0.003 | |||
| No | 349 (66.2) | 293 (84.0) | 56 (16.0) | ||
| Yes | 178 (33.8) | 130 (73.0) | 48 (27.0) | ||
| Annual check-up | 0.196 | 0.658 | |||
| No | 146 (27.7) | 119 (81.5) | 27 (18.5) | ||
| Yes | 381 (72.3) | 304 (79.8) | 77 (20.2) | ||
| Sleep disorder | 36.153 | <0.001 | |||
| No | 300 (56.9) | 268 (89.3) | 32 (10.7) | ||
| Yes | 227 (43.1) | 155 (68.3) | 72 (31.7) | ||
| Characteristics | B | SE | β | p-Value | VIF Value |
|---|---|---|---|---|---|
| Depression symptoms | |||||
| Without depression symptoms | |||||
| With depression symptoms | 2.855 | 0.585 | 0.200 | <0.001 | 1.032 |
| Gender | |||||
| Male | |||||
| Female | −0.104 | 0.397 | −0.012 | 0.794 | 1.338 |
| Age | |||||
| (60–69) years | |||||
| ≥70 years | −0.038 | 0.364 | −0.004 | 0.917 | 1.119 |
| BMI (kg/m2) | |||||
| 18.5–23.9 | |||||
| <18.5 or >23.9 | 1.025 | 0.380 | 0.111 | 0.007 | 1.047 |
| Education | |||||
| Primary school or below | |||||
| Junior high school and above | −1.269 | 0.384 | −0.146 | 0.001 | 1.203 |
| Marital status | |||||
| Married | |||||
| Single | −0.803 | 0.459 | −0.083 | 0.081 | 1.404 |
| Household arrangement | |||||
| Empty-nest elderly | |||||
| Non-empty-nest elderly | −0.084 | 0.511 | −0.007 | 0.869 | 1.245 |
| Monthly income (CNY) | |||||
| <2000 | |||||
| ≥2000 | −1.576 | 0.413 | −0.175 | <0.001 | 1.292 |
| Cigarette smoking | |||||
| No | |||||
| Yes | 0.924 | 0.479 | 0.089 | 0.054 | 1.304 |
| Alcohol drinking | |||||
| No | |||||
| Yes | −0.080 | 0.444 | −0.009 | 0.858 | 1.386 |
| Polypharmacy | |||||
| No | |||||
| Yes | −0.541 | 0.370 | −0.060 | 0.144 | 1.037 |
| Annual check-up | |||||
| No | |||||
| Yes | 1.399 | 0.418 | 0.147 | 0.001 | 1.185 |
| Sleep disorder | |||||
| No | |||||
| Yes | −0.108 | 0.378 | −0.013 | 0.775 | 1.187 |
| Characteristics | Model without Mediators | Model with Mediators | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Depression symptoms | ||||||
| Without depression symptoms | ||||||
| With depression symptoms | 2.35 | 1.16–4.78 | 0.018 | 1.83 | 0.89–3.74 | 0.099 |
| Loneliness | 1.13 | 1.06–1.20 | <0.001 | |||
| Gender | ||||||
| Male | ||||||
| Female | 1.25 | 0.71–2.23 | 0.439 | 1.29 | 0.72–2.33 | 0.392 |
| Age | ||||||
| (60–69) years | ||||||
| ≥70 years | 2.01 | 1.19–3.38 | 0.009 | 2.11 | 1.24–3.59 | 0.006 |
| BMI (kg/m2) | ||||||
| 18.5–23.9 | ||||||
| <18.5 or >23.9 | 1.95 | 1.16–3.28 | 0.012 | 1.76 | 1.03–2.98 | 0.037 |
| Education | ||||||
| Primary school or below | ||||||
| Junior high school and above | 1.72 | 1.00–2.97 | 0.051 | 2.16 | 1.23–3.82 | 0.008 |
| Marital status | ||||||
| Married | ||||||
| Single | 0.44 | 0.23–0.85 | 0.013 | 0.47 | 0.24–0.89 | 0.021 |
| Household arrangement | ||||||
| Empty-nest elderly | ||||||
| Non-empty-nest elderly | 0.29 | 0.15–0.54 | <0.001 | 0.30 | 0.15–0.57 | <0.001 |
| Monthly income (CNY) | ||||||
| <2000 | ||||||
| ≥2000 | 0.31 | 0.16–0.61 | 0.001 | 0.36 | 0.18–0.70 | 0.003 |
| Cigarette smoking | ||||||
| No | ||||||
| Yes | 1.67 | 0.88–3.16 | 0.114 | 1.54 | 0.81–2.93 | 0.192 |
| Alcohol drinking | ||||||
| No | ||||||
| Yes | 1.15 | 0.62–2.16 | 0.657 | 1.21 | 0.64–2.27 | 0.564 |
| Polypharmacy | ||||||
| No | ||||||
| Yes | 1.64 | 1.00–2.71 | 0.052 | 1.83 | 1.09–3.05 | 0.022 |
| Annual check-up | ||||||
| No | ||||||
| Yes | 0.92 | 0.52–1.64 | 0.784 | 0.78 | 0.43–1.40 | 0.398 |
| Sleep disorder | ||||||
| No | ||||||
| Yes | 4.75 | 2.76–8.18 | <0.001 | 5.34 | 3.04–9.37 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hou, P.; Xue, H.; Zhang, Y.; Ping, Y.; Zheng, Y.; Wang, Y.; Yao, Z.; Xie, X.; Dai, H.; Liu, Y. Mediating Effect of Loneliness in the Relationship between Depressive Symptoms and Cognitive Frailty in Community-Dwelling Older Adults. Brain Sci. 2022, 12, 1341. https://doi.org/10.3390/brainsci12101341
Hou P, Xue H, Zhang Y, Ping Y, Zheng Y, Wang Y, Yao Z, Xie X, Dai H, Liu Y. Mediating Effect of Loneliness in the Relationship between Depressive Symptoms and Cognitive Frailty in Community-Dwelling Older Adults. Brain Sciences. 2022; 12(10):1341. https://doi.org/10.3390/brainsci12101341
Chicago/Turabian StyleHou, Ping, Huiping Xue, Yu Zhang, Yujie Ping, Yijiang Zheng, Yan Wang, Zhenshuai Yao, Xinyi Xie, Hua Dai, and Yongbing Liu. 2022. "Mediating Effect of Loneliness in the Relationship between Depressive Symptoms and Cognitive Frailty in Community-Dwelling Older Adults" Brain Sciences 12, no. 10: 1341. https://doi.org/10.3390/brainsci12101341