
Extra-Neural Metastases of Late Recurrent Myxopapillary Ependymoma to Left Lumbar Paravertebral Muscles: Case Report and Review of the Literature
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Case History
3.2. Surgical Approach
3.3. Pathological Features
3.4. Epigenetic and Molecular Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, P.; Rastogi, N.; Jain, M.; Chhabra, P. Extraneural metastases in anaplastic ependymoma. J. Cancer Res. Ther. 2007, 3, 102–104. [Google Scholar] [PubMed]
- Zacharoulis, S.; Moreno, L. Ependymoma: An Update. J. Child Neurol. 2009, 24, 1431–1438. [Google Scholar] [CrossRef]
- Messahel, B.; Ashley, S.; Saran, F.; Ellison, D.; Ironside, J.; Phipps, K.; Cox, T.; Chong, W.; Robinson, K.; Picton, S.; et al. Relapsed intracranial ependymoma in children in the UK: Patterns of relapse, survival and therapeutic outcome. Eur. J. Cancer 2009, 45, 1815–1823. [Google Scholar] [CrossRef] [PubMed]
- Archer, T.C.; Pomeroy, S.L. Defining the Molecular Landscape of Ependymomas. Cancer Cell 2015, 27, 613–615. [Google Scholar] [CrossRef] [PubMed]
- Sonneland, P.R.L.; Scheithauer, B.W.; Onofrio, B.M. Myxopapillary ependymoma. A clinicopathologic and immunocytochemical study of 77 cases. Cancer 1985, 56, 883–893. [Google Scholar] [CrossRef]
- Celli, P.; Cervoni, L.; Cantore, G. Ependymoma of the filum terminale: Treatment and prognostic factors in a series of 28 cases. Acta Neurochir. 1993, 124, 99–103. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Gilhuis, H.J.; Kappelle, A.C.; Beute, G.; Wesseling, P.; Grotenhuis, A.; Boerman, R.H. Radiotherapy for partially resected spinal ependymomas: A retrospective study of 60 cases. Oncol. Rep. 2003, 10, 2079–2082. [Google Scholar] [CrossRef]
- Rudà, R.; Reifenberger, G.; Frappaz, D.; Pfister, S.M.; Laprie, A.; Santarius, T.; Roth, P.; Tonn, J.C.; Soffietti, R.; Weller, M.; et al. EANO guidelines for the diagnosis and treatment of ependymal tumors. Neuro-Oncology 2017, 20, 445–456. [Google Scholar] [CrossRef]
- Fujimori, T.; Iwasaki, M.; Nagamoto, Y.; Kashii, M.; Sakaura, H.; Yoshikawa, H. Extraneural Metastasis of Ependymoma in the Cauda Equina. Glob. Spine J. 2013, 3, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Capper, D.; Jones, D.T.W.; Sill, M.; Hovestadt, V.; Schrimpf, D.; Sturm, D.; Koelsche, C.; Sahm, F.; Chavez, L.; Reuss, D.E.; et al. DNA methylation-based classification of central nervous system tumours. Nature 2018, 555, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Zaytseva, M.; Papusha, L.; Novichkova, G.; Druy, A. Molecular Stratification of Childhood Ependymomas as a Basis for Person-alized Diagnostics and Treatment. Cancers 2021, 13, 4954. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, O.; Chapman, R.; Storer, L.C.; Luo, L.; Heath, P.R.; Resar, L.; Cohen, K.J.; Grundy, R.G.; Lourdusamy, A. Integrative molecular characterization of pediatric spinal ependymoma: The UK Children’s Cancer and Leukaemia Group study. Neuro-Oncol. Adv. 2021, 3, vdab043. [Google Scholar] [CrossRef] [PubMed]
- Barton, V.N.; Donson, A.M.; Kleinschmidt-DeMasters, B.K.; Birks, D.K.; Handler, M.H.; Foreman, N.K. Unique Molecular Characteristics of Pediatric Myxopapillary Ependymoma. Brain Pathol. 2010, 20, 560–570. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, K.R.; Lee, S.S.; Urquhart, J.C.; Jonker, B.P. A systematic review of outcome in intramedullary ependymoma and astrocytoma. J. Clin. Neurosci. 2019, 63, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Marchesini, N.; Tommasi, N.; Faccioli, F.; Pinna, G.; Sala, F. Cauda equina ependymomas: Surgical treatment and long-term outcomes in a series of 125 patients. J. Neurosurg. Spine 2022, 36, 452–463. [Google Scholar] [CrossRef]
- Abdulaziz, M.; Mallory, G.W.; Bydon, M.; De la Garza Ramos, R.; Ellis, J.A.; Laack, N.N.; Marsh, W.R.; Krauss, W.E.; Jallo, G.; Gokaslan, Z.L.; et al. Outcomes following myxopapillary ependymoma resection: The importance of capsule integrity. Neurosurg. Focus 2015, 39, E8. [Google Scholar] [CrossRef]
- Bandopadhayay, P.; Silvera, V.M.; Ciarlini, P.D.S.C.; Malkin, H.; Bi, W.L.; Bergthold, G.; Faisal, A.M.; Ullrich, N.J.; Marcus, K.; Scott, R.M.; et al. Myxopapillary ependymomas in children: Imaging, treatment and outcomes. J. Neuro-Oncol. 2015, 126, 165–174. [Google Scholar] [CrossRef]
- Kraetzig, T.; McLaughlin, L.; Bilsky, M.H.; Laufer, I. Metastases of spinal myxopapillary ependymoma: Unique characteristics and clinical management. J. Neurosurg. Spine 2018, 28, 201–208. [Google Scholar] [CrossRef]
- Rezai, A.R.; Woo, H.H.; Lee, M.; Cohen, H.; Zagzag, D.; Epstein, F.J. Disseminated ependymomas of the central nervous system. J. Neurosurg. 1996, 85, 618–624. [Google Scholar] [CrossRef] [Green Version]
- Weber, D.C.; Wang, Y.; Miller, R.; Villa, S.; Zaucha, R.; Pica, A.; Poortmans, P.; Anacak, Y.; Ozygit, G.; Baumert, B.; et al. Long-term outcome of patients with spinal myxopapillary ependymoma: Treatment results from the MD Anderson Cancer Center and institutions from the Rare Cancer Network. Neuro-Oncology 2014, 17, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Tobin, M.K.; Geraghty, J.R.; Engelhard, H.H.; Linninger, A.A.; Mehta, A.I. Intramedullary spinal cord tumors: A review of current and future treatment strategies. Neurosurg. Focus 2015, 39, E14. [Google Scholar] [CrossRef] [PubMed]
- Schild, S.E.; Wong, W.; Nisi, K. In regard to the radiotherapy of myxopapillary ependymomas. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 787. [Google Scholar] [PubMed]
- Lucchesi, K.M.; Grant, R.; Kahle, K.T.; Marks, A.M.; DiLuna, M.L. Primary spinal myxopapillary ependymoma in the pediatric pop-ulation: A study from the Surveillance, Epidemiology, and End Results (SEER) database. J. Neurooncol. 2016, 130, 133–140. [Google Scholar] [CrossRef]
- Akyurek, S.; Chang, E.L.; Yu, T.K.; Little, D.; Allen, P.K.; McCutcheon, I.; Mahajan, A.; Maor, M.H.; Woo, S.Y. Spinal myxopapillary ep-endymoma outcomes in patients treated with surgery and radiotherapy at M.D. Anderson Cancer Center. J. Neurooncol. 2006, 80, 177–183. [Google Scholar] [CrossRef]
- Agbahiwe, H.C.; Wharam, M.; Batra, S.; Cohen, K.; Terezakis, S.A. Management of pediatric myxopapillary ependymoma: The role of adjuvant radiation. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 421–427. [Google Scholar] [CrossRef]
- Bates, J.E.; Choi, G.; Milano, M.T. Myxopapillary ependymoma: A SEER analysis of epidemiology and outcomes. J. Neuro-Oncol. 2016, 129, 251–258. [Google Scholar] [CrossRef]
- Feldman, W.B.; Clark, A.J.; Safaee, M.; Ames, C.P.; Parsa, A.T. Tumor control after surgery for spinal myxopapillary ependymomas: Distinct outcomes in adults versus children: A systematic review. J. Neurosurg. Spine 2013, 19, 471–476. [Google Scholar] [CrossRef]
- Chamberlain, M.C. Etoposide for recurrent spinal cord ependymoma. Neurology 2002, 58, 1310–1311. [Google Scholar] [CrossRef]
- Chang, S.-I.; Tsai, M.-C.; Tsai, M.-D. An unusual primitive neuroectodermal tumor in the thoracic epidural space. J. Clin. Neurosci. 2010, 17, 261–263. [Google Scholar] [CrossRef]
- Harrison, M.; Jones, A.; Abebe, A. Pulmonary Adenocarcinoma Presenting as Paraspinal Muscle Metastatic Mass. Case Rep. Oncol. Med. 2018, 2018, 5719382. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, A.L.; Ceraldi, C.M.; Wang, T.N.; Granelli, S.G. Anatomic classification system for surgical management of paraspinal tumors. Arch. Surg. 2004, 139, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Bierry, G.; Kremer, S.; Kellner, F.; Abu Eid, M.; Bogorin, A.; Dietemann, J.-L.; Kellner-Weldon, F. Disorders of paravertebral lumbar muscles: From pathology to cross-sectional imaging. Skelet. Radiol. 2008, 37, 967–977. [Google Scholar] [CrossRef] [PubMed]
- Wippold, F.J., 2nd; Smirniotopoulos, J.G.; Moran, C.J.; Suojanen, J.N.; Vollmer, D.G. MR imaging of myxopapillary ependymoma: Findings and value to determine extent of tumor and its relation to intraspinal structures. AJR Am. J. Roentgenol. 1995, 165, 1263–1267. [Google Scholar] [CrossRef]
- Shih, R.Y.; Koeller, K.K. Intramedullary Masses of the Spinal Cord: Radiologic-Pathologic Correlation. RadioGraphics 2020, 40, 1125–1145. [Google Scholar] [CrossRef]
- Koeller, K.K.; Rosenblum, R.S.; Morrison, A.L. Neoplasms of the Spinal Cord and Filum Terminale: Radiologic-Pathologic Correlation. RadioGraphics 2000, 20, 1721–1749. [Google Scholar] [CrossRef]
- Berberat, J.; Grobholz, R.; Boxheimer, L.; Rogers, S.; Remonda, L.; Roelcke, U. Differentiation Between Calcification and Hemorrhage in Brain Tumors Using Susceptibility-Weighted Imaging: A Pilot Study. AJR Am. J. Roentgenol. 2014, 202, 847–850. [Google Scholar] [CrossRef]
- Adams, L.C.; Bressem, K.; Böker, S.M.; Bender, Y.Y.; Nörenberg, D.; Hamm, B.; Makowski, M.R. Diagnostic performance of susceptibil-ity-weighted magnetic resonance imaging for the detection of calcifications: A systematic review and meta-analysis. Sci Rep. 2017, 7, 15506. [Google Scholar] [CrossRef]
- Batich, K.A.; Riedel, R.F.; Kirkpatrick, J.P.; Tong, B.C.; Eward, W.C.; Tan, C.L.; Pittman, P.D.; McLendon, R.E.; Peters, K.B. Recurrent Extradural Myxopapillary Ependymoma with Oligometastatic Spread. Front. Oncol. 2019, 9, 1322. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Immunohistochemical Marker | Result |
|---|---|
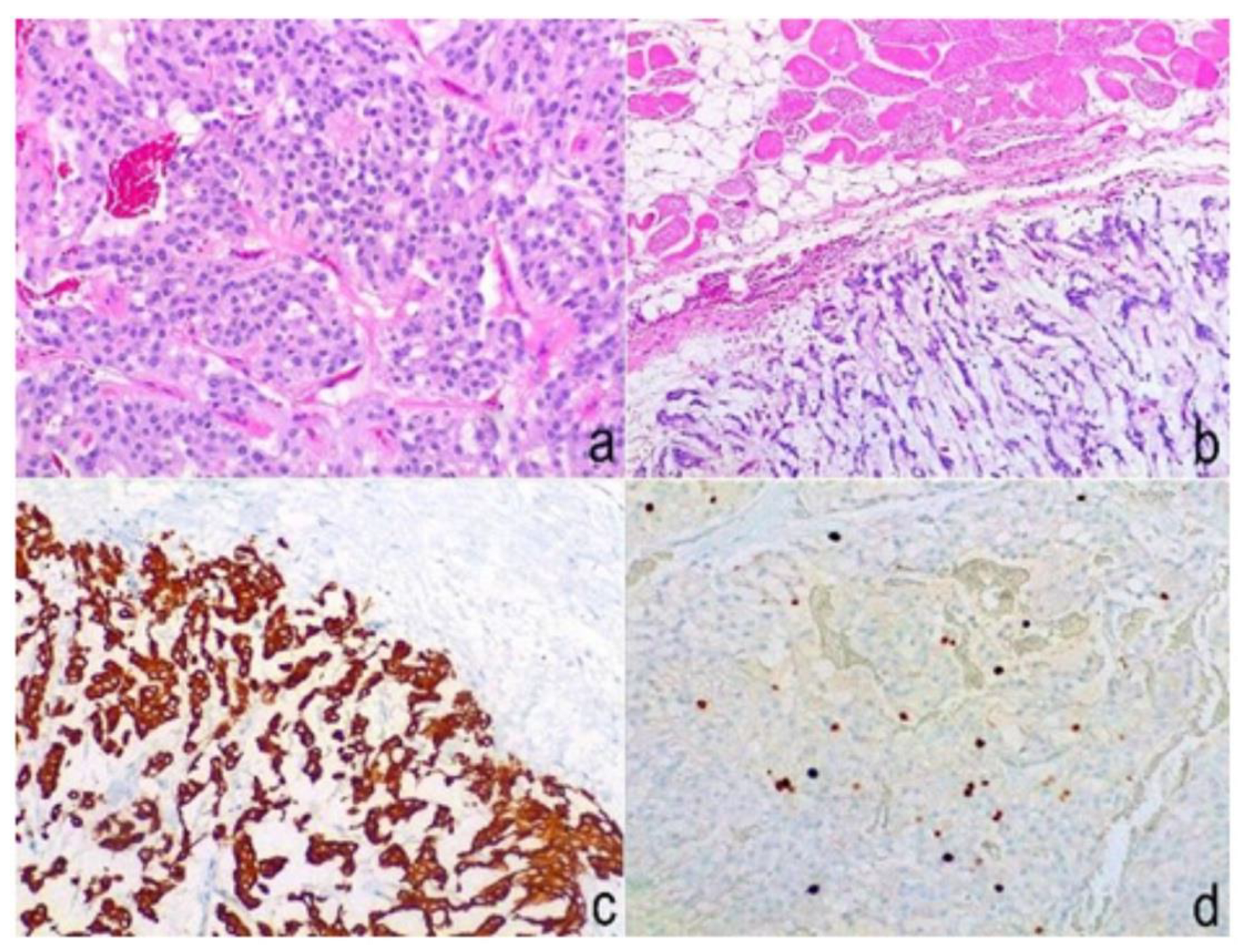
| GFAP | Present |
| pS100 | Present |
| Cytokeratin-pan | Absent |
| Cytokeratin 5/6 | Absent |
| EMA | Absent |
| p40 | Absent |
| Ki67 | <10% |
| Author and Year | Age | Sex | Origin | Histology | Metastases | Latency of Extra-Axial Metastasis Occurrence |
|---|---|---|---|---|---|---|
| Weiss et al., 1955 | 22 | M | CE | MPE | Retroperitoneum, lungs, liver, hilar and tracheobronchial lymph node, mediastinum, IVC, pleura, chest wall, diaphragm, pelvis | 10 years |
| Sharma et al., 1956 | 29 | M | CE | MPE | Lungs, liver, mediastinum, paraaortic lymph node, IVC, pleura | 4 years |
| Peterson et al., 1961 | 28 | F | CE | E | Lungs, liver, vertebrae, paraaortic and tracheobronchial lymph node, mediastinum, IVC, pleura | 17 years |
| Rubinstein et al., 1970 | 17 | F | CE | E | Lung, lymph node, pleura, pelvis, rib, 4° ventricle | 29 years |
| Wight et al., 1973 | 20 | M | CE | MPE | Para aortic lymph node, pleura, pelvis, rib, homerus | 38 years |
| Mavroudis et al., 1977 | 7 | M | CE | E | Lungs | 30 years |
| Morris et al., 1983 | 10 | F | CE/conus | E | Lungs, inguinal lymph node | 11 years |
| Newton et al., 1992 | 37 | M | CE | MPE | Lungs, pleura | <1 year |
| Newton et al., 1992 | 16 | M | CE | MPE | Abdomen (ventricular-peritoneal shunt) | 22 years |
| Farrier et al., 1994 | 23 | M | TL | E | Vertebrae, bone marrow | 12 years |
| Graf et al., 1999 | 15 | M | CE/conus | MPE | Lungs, liver, abdominal and mediastinal lymph node, pleura, chest wall | 40 years |
| Rickert et al., 1999 | 55 | F | CE | MPE | Lungs | 12 years |
| Vega-Orozco et al., 2011 | 22 | M | CE | MPE | Inguinal lymph node | 5 years |
| Fujimori et al., 2012 | 28 | M | CE | E | Lung, abdominal lymph node, IVC, pelvis | 20 years |
| Myxopapillary Ependymoma Metastasis | Lipoma | Liposarcoma | Rhabdomyosarcoma | Intramuscular Myxoma | |
|---|---|---|---|---|---|
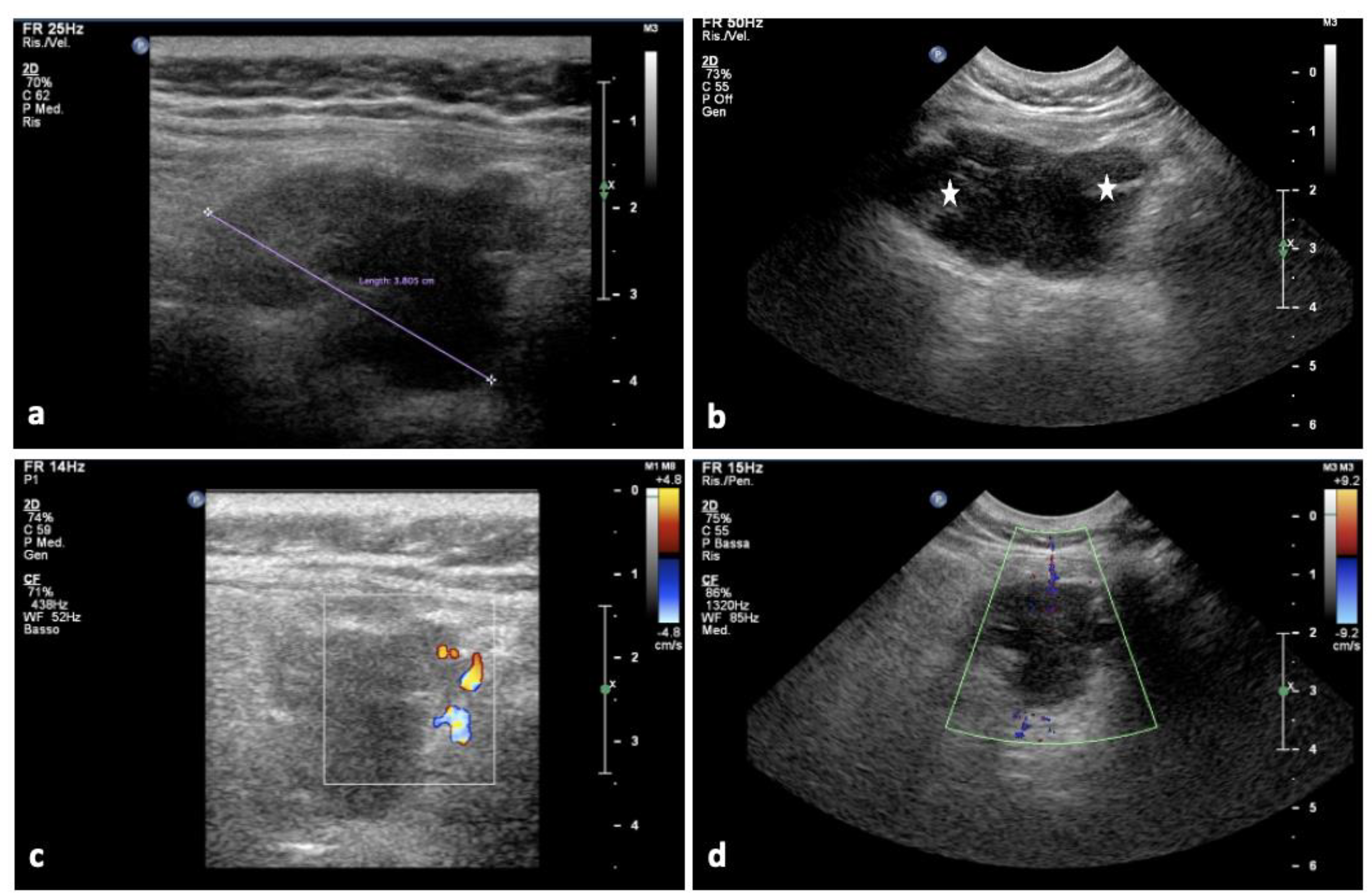
| U/S | Hypo-anechoic formation with poly lobate margins | Hyperechoic relative to the adjacent muscle | Heterogenous, multi-lobulated, typically well-defined mass of variable ultrasonographic appearance | Non-specific; hypoechoic | Well-defined hypoechoic mass; hyperechoic rim (the bright rim sign) |
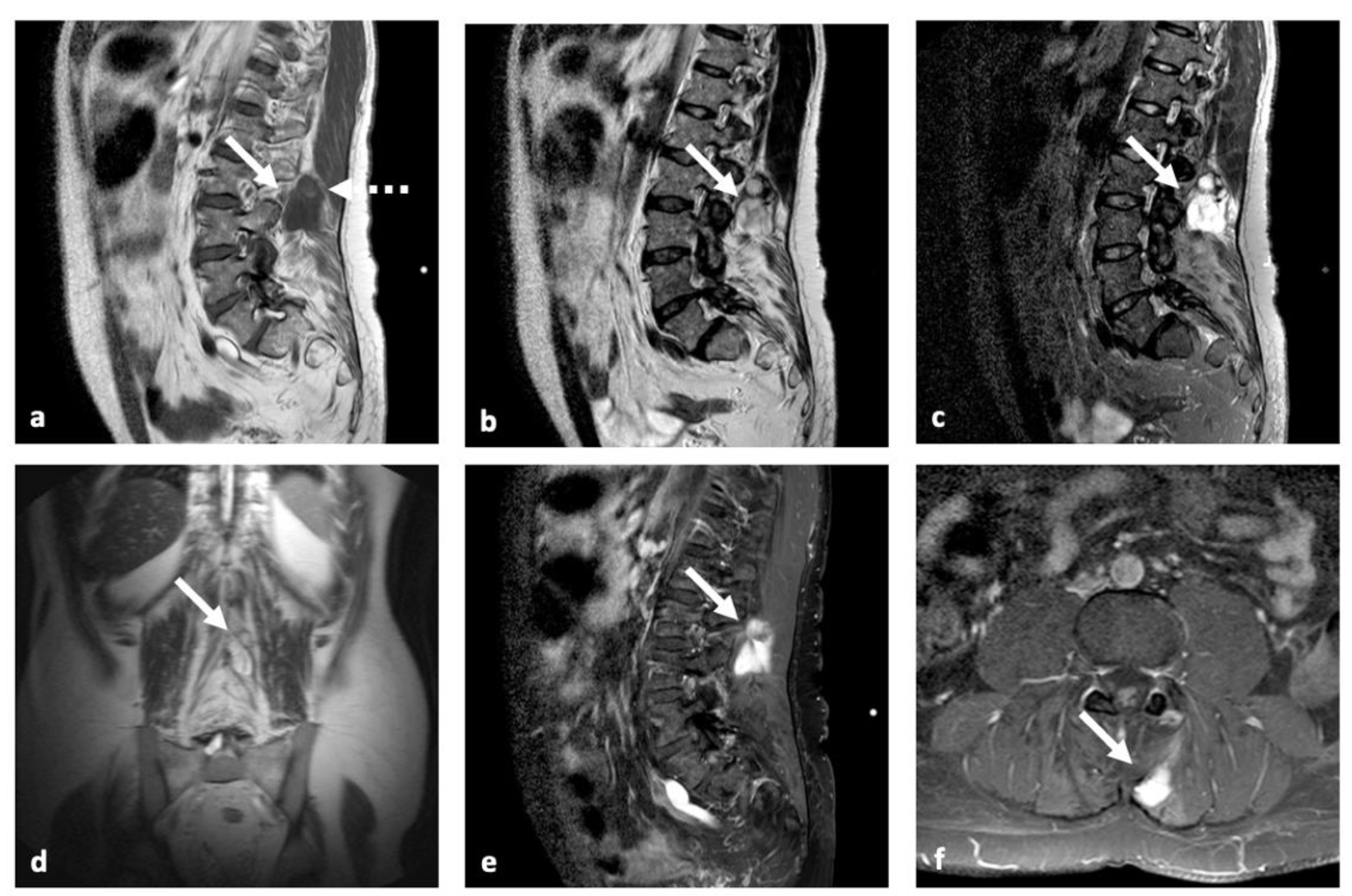
| MRI | Nonspecific: low SI on T1w; high SI on T2w; variable C.E. | Identical to fat; no C.E. | Adipose areas; non adipose areas: low SI on T1w, high SI on T2w, variable C.E. | Nonspecific: intermediate SI on both T1w and T2w | Low to intermediate SI on T1w; high SI on T2w; a small rim of fat and edema in adjacent muscles; variable C.E. |
| CT | Heterogenous mass; sometimes calcifications | Identical to fat; no C.E. | Heterogeneous attenuation; thick septa (>2 mm) | Nonspecific: heterogenous mass; calcifications; bone involvement: ill-defined, lytic metastasis | Homogeneous mass with attenuation higher than water and lower than muscles; sometimes mild C.E. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mastantuoni, C.; Tortora, F.; Tafuto, R.; Tortora, M.; Briganti, F.; Franca, R.A.; Della Monica, R.; Cuomo, M.; Chiariotti, L.; Esposito, F.; et al. Extra-Neural Metastases of Late Recurrent Myxopapillary Ependymoma to Left Lumbar Paravertebral Muscles: Case Report and Review of the Literature. Brain Sci. 2022, 12, 1227. https://doi.org/10.3390/brainsci12091227
Mastantuoni C, Tortora F, Tafuto R, Tortora M, Briganti F, Franca RA, Della Monica R, Cuomo M, Chiariotti L, Esposito F, et al. Extra-Neural Metastases of Late Recurrent Myxopapillary Ependymoma to Left Lumbar Paravertebral Muscles: Case Report and Review of the Literature. Brain Sciences. 2022; 12(9):1227. https://doi.org/10.3390/brainsci12091227
Chicago/Turabian StyleMastantuoni, Ciro, Fabio Tortora, Roberto Tafuto, Mario Tortora, Francesco Briganti, Raduan Ahmed Franca, Rosa Della Monica, Mariella Cuomo, Lorenzo Chiariotti, Felice Esposito, and et al. 2022. "Extra-Neural Metastases of Late Recurrent Myxopapillary Ependymoma to Left Lumbar Paravertebral Muscles: Case Report and Review of the Literature" Brain Sciences 12, no. 9: 1227. https://doi.org/10.3390/brainsci12091227