
Perturbation-Induced Protective Arm Responses: Effect of Age, Perturbation-Intensity, and Relationship with Stepping Stability: A Pilot Study


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Statistical Analysis
3. Results
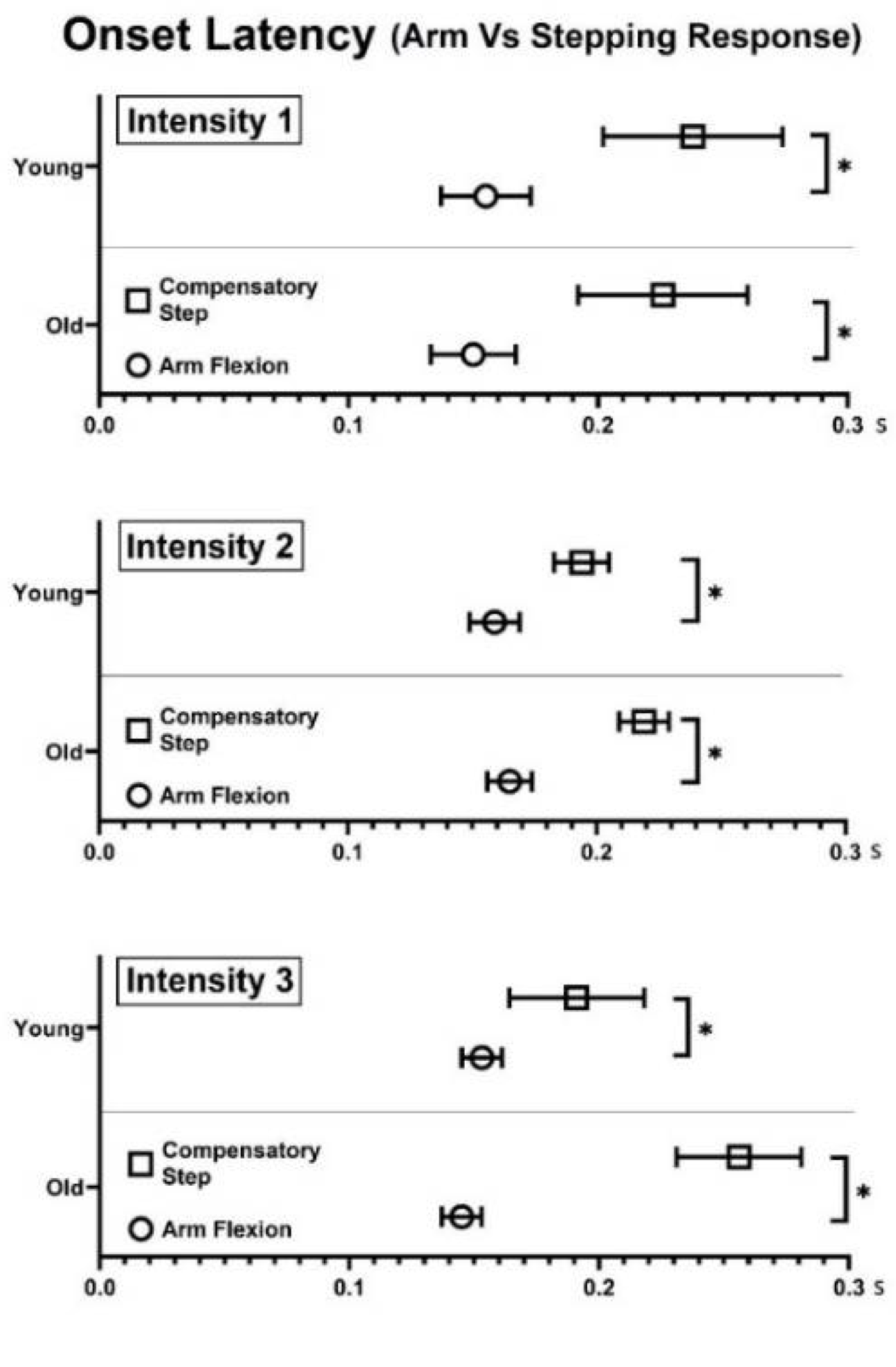
3.1. Onset Latency of Arm Elevation and First Compensatory Step LO
3.2. Displacement and Velocity of Arm Responses
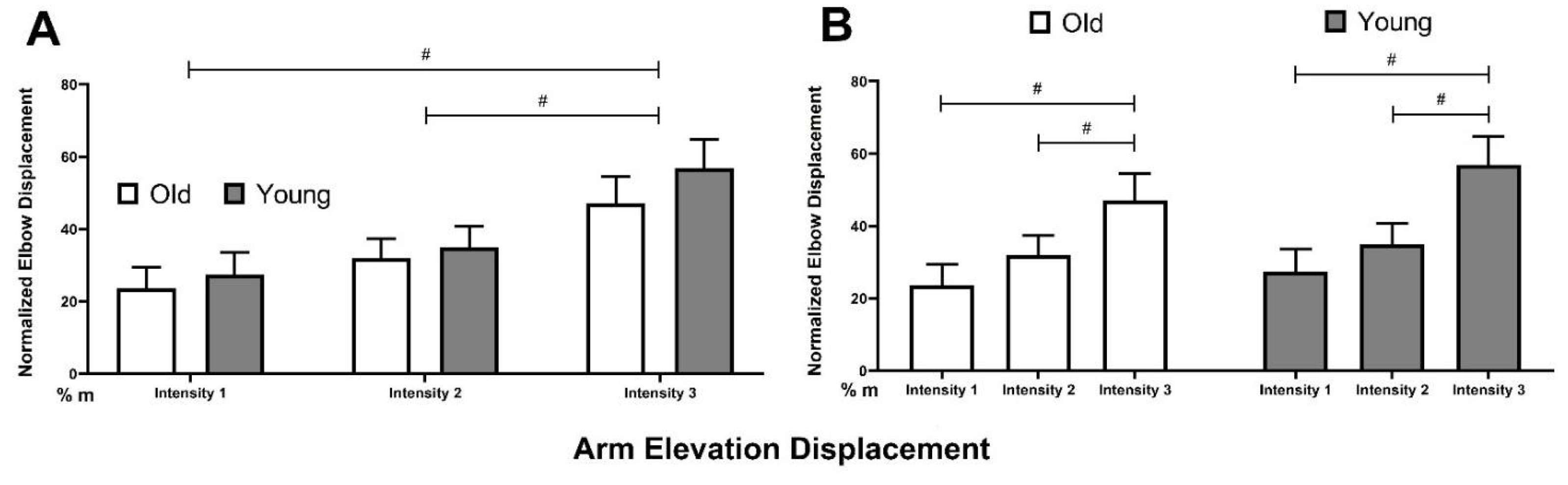
3.2.1. Arm Elevation Displacement
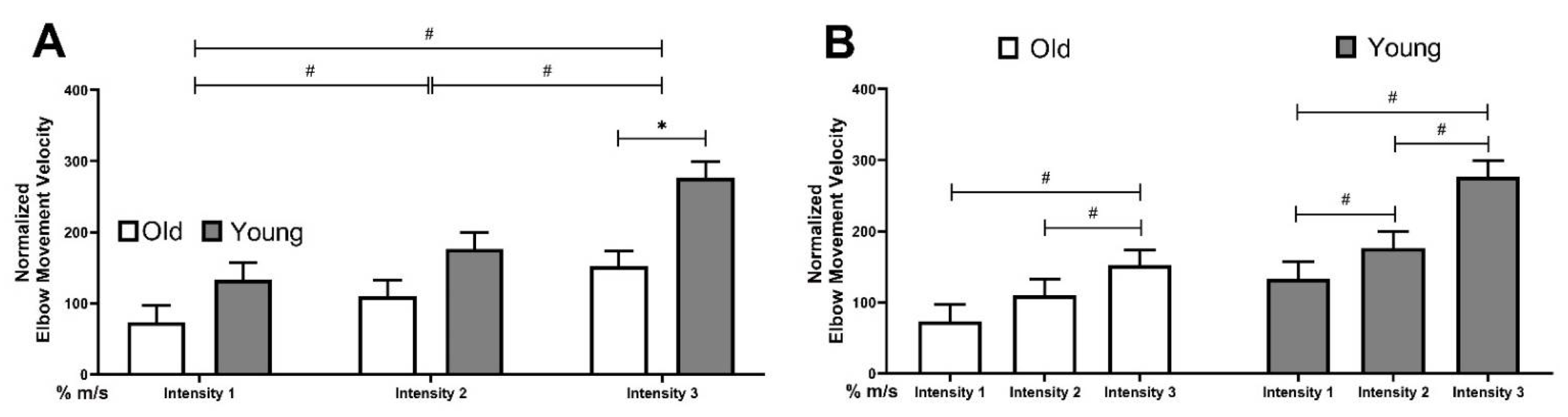
3.2.2. Arm Elevation Velocity
3.3. Relationship between Maximal Arm Elevation and Stepping Stability at TD
4. Discussion
4.1. Age-Related Impairment in the Modulation of Arm Responses
4.2. Correlation between Arm Responses and Compensatory Stepping Stability
4.3. Clinical Significance
4.4. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sattin, R.W. Falls among Older Persons: A Public Health Perspective. Annu. Rev. Public Health 1992, 13, 489–508. [Google Scholar] [CrossRef] [PubMed]
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls and Fall Injuries Among Adults Aged ≥65 Years–United States, 2014. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk Factors for Falls among Elderly Persons Living in the Community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef] [PubMed]
- Alexander, B.H.; Rivara, F.P.; Wolf, M.E. The Cost and Frequency of Hospitalization for Fall-Related Injuries in Older Adults. Am. J. Public Health 1992, 82, 1020–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef] [Green Version]
- Marigold, D.S.; Bethune, A.J.; Patla, A.E. Role of the Unperturbed Limb and Arms in the Reactive Recovery Response to an Unexpected Slip during Locomotion. J. Neurophysiol. 2003, 89, 1727–1737. [Google Scholar] [CrossRef] [Green Version]
- Gholizadeh, H.; Hill, A.; Nantel, J. Effect of Arm Motion on Postural Stability When Recovering from a Slip Perturbation. J. Biomech. 2019, 95, 109269. [Google Scholar] [CrossRef]
- Pijnappels, M.; Kingma, I.; Wezenberg, D.; Reurink, G.; van Dieën, J.H. Armed against Falls: The Contribution of Arm Movements to Balance Recovery after Tripping. Exp. Brain Res. 2010, 201, 689–699. [Google Scholar] [CrossRef] [Green Version]
- Dietz, V.; Fouad, K.; Bastiaanse, C.M. Neuronal Coordination of Arm and Leg Movements during Human Locomotion. Eur. J. Neurosci. 2001, 14, 1906–1914. [Google Scholar] [CrossRef]
- McIlroy, W.E.; Maki, B.E. Early Activation of Arm Muscles Follows External Perturbation of Upright Stance. Neurosci. Lett. 1995, 184, 177–180. [Google Scholar] [CrossRef]
- Marigold, D.S.; Patla, A.E. Strategies for Dynamic Stability during Locomotion on a Slippery Surface: Effects of Prior Experience and Knowledge. J. Neurophysiol. 2002, 88, 339–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, K.B.; Wang, K.-M.; Kuo, S.-Y. Role of Arm Motion in Feet-in-Place Balance Recovery. J. Biomech. 2015, 48, 3155–3162. [Google Scholar] [CrossRef] [PubMed]
- Roos, P.E.; McGuigan, M.P.; Kerwin, D.G.; Trewartha, G. The Role of Arm Movement in Early Trip Recovery in Younger and Older Adults. Gait Posture 2008, 27, 352–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, S.; van der Burg, J.; van der Meché, F.G.A. Coordination of Movements of the Hindlimbs and Forelimbs in Different Forms of Locomotion in Normal and Decerebrate Cats. Brain Res. 1975, 91, 217–237. [Google Scholar] [CrossRef]
- Ohbayashi, M. The Roles of the Cortical Motor Areas in Sequential Movements. Front. Behav. Neurosci. 2021, 15. [Google Scholar] [CrossRef]
- Patel, P.J.; Bhatt, T. Does Aging with a Cortical Lesion Increase Fall-Risk: Examining Effect of Age versus Stroke on Intensity Modulation of Reactive Balance Responses from Slip-like Perturbations. Neuroscience 2016, 333, 252–263. [Google Scholar] [CrossRef]
- Merrill, Z.; Chambers, A.J.; Cham, R. Arm Reactions in Response to an Unexpected Slip-Impact of Aging. J. Biomech. 2017, 58, 21–26. [Google Scholar] [CrossRef]
- Jeon, W.; Griffin, L.; Hsiao, H.-Y. Effects of Initial Foot Position on Postural Responses to Lateral Standing Surface Perturbations in Younger and Older Adults. Gait Posture 2021, 90, 449–456. [Google Scholar] [CrossRef]
- Hof, A.L.; Gazendam, M.G.J.; Sinke, W.E. The Condition for Dynamic Stability. J. Biomech. 2005, 38, 1–8. [Google Scholar] [CrossRef]
- Tokur, D.; Grimmer, M.; Seyfarth, A. Review of Balance Recovery in Response to External Perturbations during Daily Activities. Hum. Mov. Sci. 2020, 69, 102546. [Google Scholar] [CrossRef]
- Vercillo, T.; Carrasco, C.; Jiang, F. Age-Related Changes in Sensorimotor Temporal Binding. Front. Hum. Neurosci. 2017, 11. [Google Scholar] [CrossRef] [Green Version]
- Rivner, M.H.; Swift, T.R.; Malik, K. Influence of Age and Height on Nerve Conduction. Muscle Nerve 2001, 24, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- Baudry, S.; Maerz, A.H.; Enoka, R.M. Presynaptic Modulation of Ia Afferents in Young and Old Adults When Performing Force and Position Control. J. Neurophysiol. 2010, 103, 623–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baudry, S.; Penzer, F.; Duchateau, J. Input-Output Characteristics of Soleus Homonymous Ia Afferents and Corticospinal Pathways during Upright Standing Differ between Young and Elderly Adults. Acta Physiol. 2014, 210, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, S.; Lee, A.; Pai, Y.-C.; Bhatt, T. Treadmill-Gait Slip Training in Community-Dwelling Older Adults: Mechanisms of Immediate Adaptation for a Progressive Ascending-Mixed-Intensity Protocol. Exp. Brain Res. 2019, 237, 2305–2317. [Google Scholar] [CrossRef]
- Lexell, J.; Taylor, C.C.; Sjöström, M. What Is the Cause of the Ageing Atrophy? Total Number, Size and Proportion of Different Fiber Types Studied in Whole Vastus Lateralis Muscle from 15- to 83-Year-Old Men. J. Neurol. Sci. 1988, 84, 275–294. [Google Scholar] [CrossRef]
- Newman, A.B.; Haggerty, C.L.; Goodpaster, B.; Harris, T.; Kritchevsky, S.; Nevitt, M.; Miles, T.P.; Visser, M. The Health, Aging, and Body Composition Research Group Strength and Muscle Quality in a Well-Functioning Cohort of Older Adults: The Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2003, 51, 323–330. [Google Scholar] [CrossRef]
- Petrella, J.K.; Kim, J.; Tuggle, S.C.; Hall, S.R.; Bamman, M.M. Age Differences in Knee Extension Power, Contractile Velocity, and Fatigability. J. Appl. Physiol. 2005, 98, 211–220. [Google Scholar] [CrossRef] [Green Version]
- Hunter, S.K.; Pereira, H.M.; Keenan, K.G. The Aging Neuromuscular System and Motor Performance. J. Appl. Physiol. 2016, 121, 982–995. [Google Scholar] [CrossRef]
- Westlake, K.P.; Wu, Y.; Culham, E.G. Sensory-Specific Balance Training in Older Adults: Effect on Position, Movement, and Velocity Sense at the Ankle. Phys. Ther. 2007, 87, 560–568. [Google Scholar] [CrossRef]
- Westlake, K.P.; Wu, Y.; Culham, E.G. Velocity Discrimination: Reliability and Construct Validity in Older Adults. Hum. Mov. Sci. 2007, 26, 443–456. [Google Scholar] [CrossRef] [PubMed]
- Gariépy, C.; Hasson, C.J.; Emmerik, R.E.A.V.; Caldwell, G.E. Age-related decrease in degrees of freedom in postural control during quiet stance. J. Biomech. 2008, 41 (Suppl. S1), S24. [Google Scholar] [CrossRef]
- Peters, R.M.; McKeown, M.D.; Carpenter, M.G.; Inglis, J.T. Losing Touch: Age-Related Changes in Plantar Skin Sensitivity, Lower Limb Cutaneous Reflex Strength, and Postural Stability in Older Adults. J. Neurophysiol. 2016, 116, 1848–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bent, L.R.; Lowrey, C.R. Single Low-Threshold Afferents Innervating the Skin of the Human Foot Modulate Ongoing Muscle Activity in the Upper Limbs. J. Neurophysiol. 2013, 109, 1614–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freyler, K.; Gollhofer, A.; Colin, R.; Brüderlin, U.; Ritzmann, R. Reactive Balance Control in Response to Perturbation in Unilateral Stance: Interaction Effects of Direction, Displacement and Velocity on Compensatory Neuromuscular and Kinematic Responses. PLoS ONE 2015, 10, e0144529. [Google Scholar] [CrossRef]
- De Souza, C.R.; Betelli, M.T.; Takazono, P.S.; de Oliveira, J.Á.; Coelho, D.B.; Duysens, J.; Teixeira, L.A. Evaluation of Balance Recovery Stability from Unpredictable Perturbations through the Compensatory Arm and Leg Movements (CALM) Scale. PLoS ONE 2019, 14, e0221398. [Google Scholar] [CrossRef]
- Maki, B.E.; Edmondstone, M.A.; McIlroy, W.E. Age-Related Differences in Laterally Directed Compensatory Stepping Behavior. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, 270–277. [Google Scholar] [CrossRef]
- Reimann, H.; Fettrow, T.D.; Thompson, E.D.; Agada, P.; McFadyen, B.J.; Jeka, J.J. Complementary Mechanisms for Upright Balance during Walking. PLoS ONE 2017, 12, e0172215. [Google Scholar] [CrossRef] [Green Version]
- Troy, K.L.; Donovan, S.J.; Grabiner, M.D. Theoretical Contribution of the Upper Extremities to Reducing Trunk Extension Following a Laboratory-Induced Slip. J. Biomech. 2009, 42, 1339–1344. [Google Scholar] [CrossRef] [Green Version]
- Allum, J.H.J.; Carpenter, M.G.; Honegger, F.; Adkin, A.L.; Bloem, B.R. Age-Dependent Variations in the Directional Sensitivity of Balance Corrections and Compensatory Arm Movements in Man. J. Physiol. 2002, 542, 643–663. [Google Scholar] [CrossRef]
- Horak, F.B.; Henry, S.M.; Shumway-Cook, A. Postural Perturbations: New Insights for Treatment of Balance Disorders. Phys. Ther. 1997, 77, 517–533. [Google Scholar] [CrossRef] [PubMed]
- Belmin, J.; Valensi, P. Diabetic Neuropathy in Elderly Patients. What Can Be Done? Drugs Aging 1996, 8, 416–429. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, R.L.; Sartor, C.D.; Ferreira, J.S.S.P.; Dantas, M.G.B.; Bus, S.A.; Sacco, I.C.N. Protocol for Evaluating the Effects of a Foot-Ankle Therapeutic Exercise Program on Daily Activity, Foot-Ankle Functionality, and Biomechanics in People with Diabetic Polyneuropathy: A Randomized Controlled Trial. BMC Musculoskelet. Disord. 2018, 19, 400. [Google Scholar] [CrossRef] [PubMed] [Green Version]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, W.; Wang, S.; Bhatt, T.; Westlake, K.P. Perturbation-Induced Protective Arm Responses: Effect of Age, Perturbation-Intensity, and Relationship with Stepping Stability: A Pilot Study. Brain Sci. 2022, 12, 953. https://doi.org/10.3390/brainsci12070953
Jeon W, Wang S, Bhatt T, Westlake KP. Perturbation-Induced Protective Arm Responses: Effect of Age, Perturbation-Intensity, and Relationship with Stepping Stability: A Pilot Study. Brain Sciences. 2022; 12(7):953. https://doi.org/10.3390/brainsci12070953
Chicago/Turabian StyleJeon, Woohyoung, Shuaijie Wang, Tanvi Bhatt, and Kelly P. Westlake. 2022. "Perturbation-Induced Protective Arm Responses: Effect of Age, Perturbation-Intensity, and Relationship with Stepping Stability: A Pilot Study" Brain Sciences 12, no. 7: 953. https://doi.org/10.3390/brainsci12070953