
Serum Mature BDNF Level Is Associated with Remission Following ECT in Treatment-Resistant Depression

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. ECT Treatment
2.3. Clinical Assessments
2.4. Biological Analyses
2.5. Statistical Analyses
3. Results
3.1. Sample and Clinical Effects of ECT
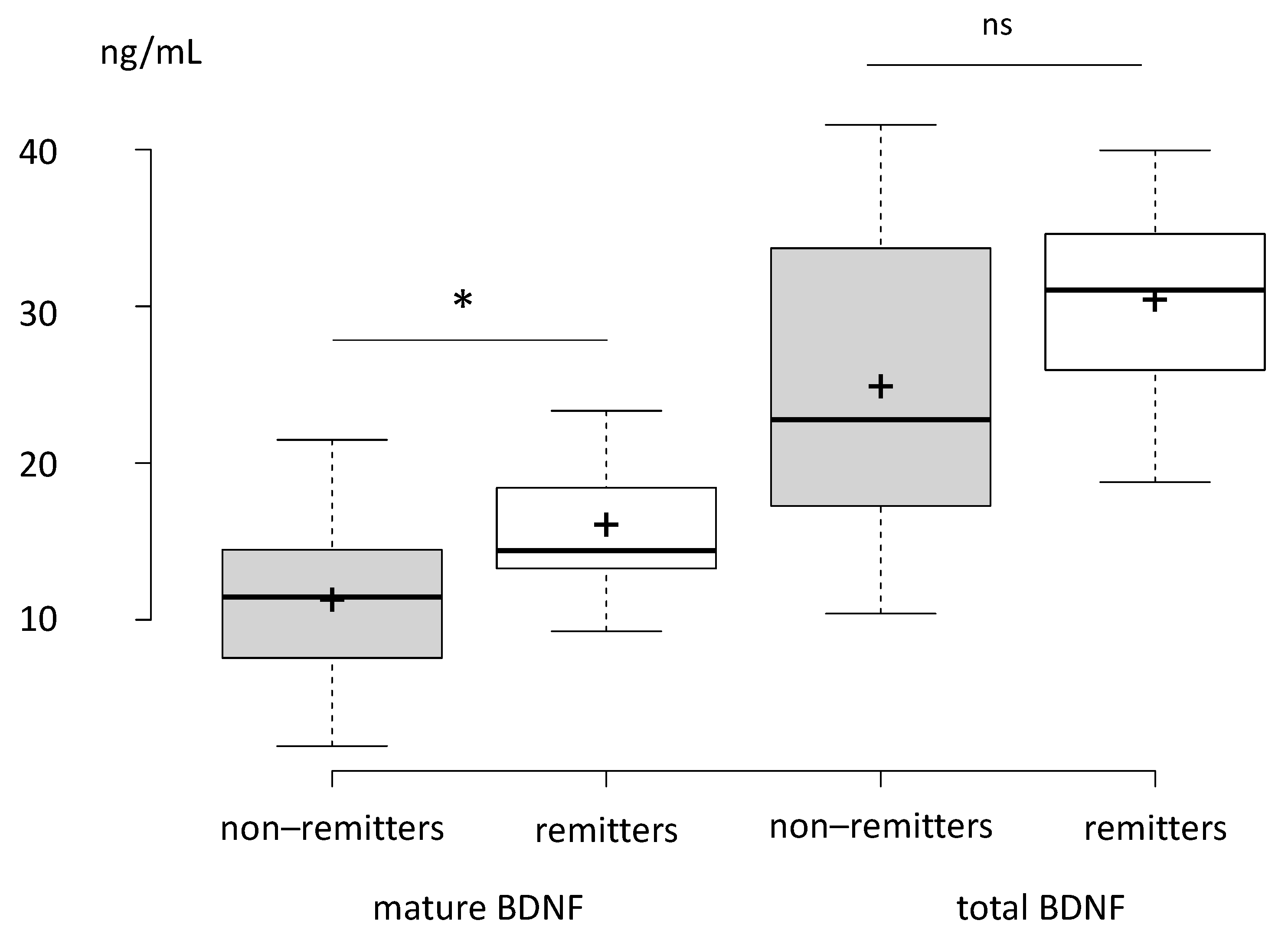
3.2. Comparison of Remitters and Non-Remitters
3.3. Association between Baseline mBDNF Levels and Future Remission
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates, 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf (accessed on 6 December 2021).
- Dierckx, B.; Heijnen, W.T.; van den Broek, W.W.; Birkenhäger, T.K. Efficacy of electroconvulsive therapy in bipolar versus unipolar major depression: A meta-analysis. Bipolar. Disord. 2012, 14, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Al-Harbi, K.S. Treatment-resistant depression: Therapeutic trends, challenges, and future directions. Patient Prefer. Adherence 2012, 6, 369–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keller, M.B. Remission versus response, the new gold standard of antidepressant care. J. Clin. Psychiatry 2004, 65 (Suppl. S4), 53–59. [Google Scholar]
- Carstens, L.; Hartling, C.; Stippl, A.; Domke, A.K.; Herrera-Mendelez, A.L.; Aust, S.; Gärtner, M.; Bajbouj, M.; Grimm, S. A symptom-based approach in predicting ECT outcome in depressed patients employing MADRS single items. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 1275–1284. [Google Scholar] [CrossRef]
- Gärtner, M.; Ghisu, E.; Herrera-Melendez, A.L.; Koslowski, M.; Aust, S.; Asbach, P.; Otte, C.; Regen, F.; Heuser, I.; Borgwardt, K.; et al. Using routine MRI data of depressed patients to predict individual responses to electroconvulsive therapy. Exp. Neurol. 2021, 335, 113505. [Google Scholar] [CrossRef] [PubMed]
- Simon, L.; Blay, M.; Galvao, F.; Brunelin, J. Using EEG to Predict Clinical Response to Electroconvulsive Therapy in Patients With Major Depression: A Comprehensive Review. Front. Psychiatry 2021, 12, 643710. [Google Scholar] [CrossRef]
- Jonckheere, J.; Deloulme, J.C.; Dall’Igna, G.; Chauliac, N.; Pelluet, A.; Nguon, A.S.; Lentini, C.; Brocard, J.; Denarier, E.; Brugière, S.; et al. Short- and long-term efficacy of electroconvulsive stimulation in animal models of depression: The essential role of neuronal survival. Brain Stimul. 2018, 11, 1336–1347. [Google Scholar] [CrossRef] [Green Version]
- Polyakova, M.; Schroeter, M.L.; Elzinga, B.M.; Holiga, S.; Schoenknecht, P.; de Kloet, E.R.; Molendijk, M.L. Brain-Derived Neurotrophic Factor and Antidepressive Effect of Electroconvulsive Therapy: Systematic Review and Meta-Analyses of the Preclinical and Clinical Literature. PLoS ONE 2015, 10, e0141564. [Google Scholar] [CrossRef] [Green Version]
- Brunoni, A.R.; Baeken, C.; Machado-Vieira, R.; Gattaz, W.F.; Vanderhasselt, M.A. BDNF blood levels after electroconvulsive therapy in patients with mood disorders: A systematic review and meta-analysis. World J. Biol. Psychiatry 2014, 15, 411–418. [Google Scholar] [CrossRef]
- Freire, T.F.; Fleck, M.P.; da Rocha, N.S. Remission of depression following electroconvulsive therapy (ECT) is associated with higher levels of brain-derived neurotrophic factor (BDNF). Brain Res. Bull. 2016, 121, 263–269. [Google Scholar] [CrossRef]
- Piccinni, A.; Del Debbio, A.; Medda, P.; Bianchi, C.; Roncaglia, I.; Veltri, A.; Zanello, S.; Massimetti, E.; Origlia, N.; Domenici, L.; et al. Plasma Brain-Derived Neurotrophic Factor in treatment-resistant depressed patients receiving electroconvulsive therapy. Eur. Neuropsychopharmacol. 2009, 19, 349–355. [Google Scholar] [CrossRef]
- Zheng, W.; Cen, Q.; Nie, S.; Li, M.; Zeng, R.; Zhou, S.; Cai, D.; Jiang, M.; Huang, X. Serum BDNF levels and the antidepressant effects of electroconvulsive therapy with ketamine anaesthesia: A preliminary study. PeerJ 2021, 9, e10699. [Google Scholar] [CrossRef]
- Maffioletti, E.; Gennarelli, M.; Gainelli, G.; Bocchio-Chiavetto, L.; Bortolomasi, M.; Minelli, A. BDNF Genotype and Baseline Serum Levels in Relation to Electroconvulsive Therapy Effectiveness in Treatment-Resistant Depressed Patients. J. ECT 2019, 35, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Lu, B.; Pang, P.T.; Woo, N.H. The yin and yang of neurotrophin action. Nat. Rev. Neurosci. 2005, 6, 603–614. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, K. Brain-derived neurotrophic factor as a biomarker for mood disorders: An historical overview and future directions. Psychiatry Clin. Neurosci. 2010, 64, 341–357. [Google Scholar] [CrossRef]
- Lessmann, V.; Brigadski, T. Mechanisms, locations, and kinetics of synaptic BDNF secretion: An update. Neurosci. Res. 2009, 65, 11–22. [Google Scholar] [CrossRef]
- Nagappan, G.; Zaitsev, E.; Senatorov, V.V.; Yang, J.; Hempstead, B.L.; Lu, B. Control of Extracellular Cleavage of ProBDNF by High Frequency Neuronal Activity. Proc. Natl. Acad. Sci. USA 2009, 106, 1267–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, O.; Psomiades, M.; Rey, R.; Mandairon, N.; Suaud-Chagny, M.F.; Mondino, M.; Brunelin, J. Frontotemporal Transcranial Direct Current Stimulation Decreases Serum Mature Brain-Derived Neurotrophic Factor in Schizophrenia. Brain Sci. 2021, 11, 662. [Google Scholar] [CrossRef]
- Hawley, C.J.; Gale, T.M.; Sivakumaran, T. Hertfordshire Neuroscience Research group. Defining remission by cut off score on the MADRS: Selecting the optimal value. J. Affect. Disord. 2002, 72, 177–184. [Google Scholar] [CrossRef]
- Wolkowitz, O.M.; Wolf, J.; Shelly, W.; Rosser, R.; Burke, H.M.; Lerner, G.K.; Reus, V.I.; Nelson, J.C.; Epel, E.S.; Mellon, S.H. Serum BDNF levels before treatment predict SSRI response in depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 1623–1630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunoni, A.R.; Lopes, M.; Fregni, F. A systematic review and meta-analysis of clinical studies on major depression and BDNF levels: Implications for the role of neuroplasticity in depression. Int. J. Neuropsychopharmacol. 2008, 11, 1169–1180. [Google Scholar] [CrossRef]
- Szegedi, A.; Jansen, W.T.; van Willigenburg, A.P.; van der Meulen, E.; Stassen, H.H.; Thase, M.E. Early improvement in the first 2 weeks as a predictor of treatment outcome in patients with major depressive disorder: A meta-analysis including 6562 patients. J. Clin. Psychiatry 2009, 70, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Tadić, A.; Wagner, S.; Schlicht, K.F.; Peetz, D.; Borysenko, L.; Dreimüller, N.; Hiemke, C.; Lieb, K. The early non-increase of serum BDNF predicts failure of antidepressant treatment in patients with major depression: A pilot study. Prog. Neuropsychopharmacol. Biol. Psychiatry 2011, 35, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Dreimüller, N.; Schlicht, K.F.; Wagner, S.; Peetz, D.; Borysenko, L.; Hiemke, C.; Lieb, K.; Tadić, A. Early reactions of brain-derived neurotrophic factor in plasma (pBDNF) and outcome to acute antidepressant treatment in patients with Major Depression. Neuropharmacology 2012, 62, 264–269. [Google Scholar] [CrossRef]
- Duman, R.S.; Aghajanian, G.K.; Sanacora, G.; Krystal, J.H. Synaptic plasticity and depression: New insights from stress and rapid-acting antidepressants. Nat. Med. 2016, 22, 238–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshida, T.; Ishikawa, M.; Niitsu, T.; Nakazato, M.; Watanabe, H.; Shiraishi, T.; Shiina, A.; Hashimoto, T.; Kanahara, N.; Hasegawa, T.; et al. Hashimoto, K. Decreased serum levels of mature brain-derived neurotrophic factor (BDNF), but not its precursor proBDNF, in patients with major depressive disorder. PLoS ONE 2012, 7, e42676. [Google Scholar] [CrossRef] [Green Version]
- Leal, G.; Comprido, D.; Duarte, C.B. BDNF-induced local protein synthesis and synaptic plasticity. Neuropharmacology 2014, 76 Pt C, 639–656. [Google Scholar] [CrossRef] [Green Version]
- Zagrebelsky, M.; Korte, M. Form follows function: BDNF and its involvement in sculpting the function and structure of synapses. Neuropharmacology 2014, 76 Pt C, 628–638. [Google Scholar] [CrossRef]
- Enomoto, S.; Shimizu, K.; Nibuya, M.; Suzuki, E.; Nagata, K.; Kondo, T. Activated brain-derived neurotrophic factor/TrkB signaling in rat dorsal and ventral hippocampi following 10-day electroconvulsive seizure treatment. Neurosci. Lett. 2017, 660, 45–50. [Google Scholar] [CrossRef]
- Ma, Z.; Zang, T.; Birnbaum, S.G.; Wang, Z.; Johnson, J.E.; Zhang, C.L.; Parada, L.F. TrkB dependent adult hippocampal progenitor differentiation mediates sustained ketamine antidepressant response. Nat. Commun. 2017, 8, 1668. [Google Scholar] [CrossRef] [Green Version]
- Brunelin, J.; Iceta, S.; Plaze, M.; Gaillard, R.; Simon, L.; Suaud-Chagny, M.F.; Galvao, F.; Poulet, E. The Combination of Propofol and Ketamine Does Not Enhance Clinical Responses to Electroconvulsive Therapy in Major Depression-The Results From the KEOpS Study. Front. Pharmacol. 2020, 11, 562137. [Google Scholar] [CrossRef]
- Petrides, G.; Fink, M.; Husain, M.M.; Knapp, R.G.; Rush, A.J.; Mueller, M.; Rummans, T.A.; O’Connor, K.M.; Rasmussen, K.G., Jr.; Bernstein, H.J.; et al. ECT remission rates in psychotic versus nonpsychotic depressed patients: A report from CORE. J. ECT 2001, 17, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Prudic, J.; Olfson, M.; Marcus, S.C.; Fuller, R.B.; Sackeim, H.A. Effectiveness of electroconvulsive therapy in community settings. Biol. Psychiatry 2004, 55, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, R.; Kishi, T.; Hori, H.; Atake, K.; Katsuki, A.; Nakano-Umene, W.; Ikenouchi-Sugita, A.; Iwata, N.; Nakamura, J. Serum proBDNF/BDNF and response to fluvoxamine in drug-naïve first-episode major depressive disorder patients. Ann. Gen. Psychiatry 2014, 13, 19. [Google Scholar] [CrossRef] [Green Version]
- Ryan, K.M.; Dunne, R.; McLoughlin, D.M. BDNF plasma levels and genotype in depression and the response to electroconvulsive therapy. Brain Stimul. 2018, 11, 1123–1131. [Google Scholar] [CrossRef]
- Pan, W.; Banks, W.A.; Kastin, A.J. Permeability of the blood-brain barrier to neurotrophins. Brain Res. 1998, 788, 87–94. [Google Scholar] [CrossRef]
- Dell’Osso, L.; Del Debbio, A.; Veltri, A.; Bianchi, C.; Roncaglia, I.; Carlini, M.; Massimetti, G.; Catena Dell’Osso, M.; Vizzaccaro, C.; Marazziti, D.; et al. Associations between brain-derived neurotrophic factor plasma levels and severity of the illness, recurrence and symptoms in depressed patients. Neuropsychobiology 2010, 62, 207–212. [Google Scholar] [CrossRef]
- Guilloux, J.P.; Douillard-Guilloux, G.; Kota, R.; Wang, X.; Gardier, A.M.; Martinowich, K.; Tseng, G.C.; Lewis, D.A.; Sibille, E. Molecular evidence for BDNF- and GABA-related dysfunctions in the amygdala of female subjects with major depression. Mol. Psychiatry 2012, 17, 1130–1142. [Google Scholar] [CrossRef] [Green Version]
- Molendijk, M.L.; Spinhoven, P.; Polak, M.; Bus, B.A.; Penninx, B.W.; Elzinga, B.M. Serum BDNF concentrations as peripheral manifestations of depression: Evidence from a systematic review and meta-analyses on 179 associations (N = 9484). Mol. Psychiatry 2014, 19, 791–800. [Google Scholar] [CrossRef]
- Reinhart, V.; Bove, S.E.; Volfson, D.; Lewis, D.A.; Kleiman, R.J.; Lanz, T.A. Evaluation of TrkB and BDNF transcripts in prefrontal cortex, hippocampus, and striatum from subjects with schizophrenia, bipolar disorder, and major depressive disorder. Neurobiol. Dis. 2015, 77, 220–227. [Google Scholar] [CrossRef]
- Delamarre, L.; Galvao, F.; Gohier, B.; Poulet, E.; Brunelin, J. How Much Do Benzodiazepines Matter for Electroconvulsive Therapy in Patients With Major Depression? J. ECT 2019, 35, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Redlich, R.; Opel, N.; Grotegerd, D.; Dohm, K.; Zaremba, D.; Bürger, C.; Münker, S.; Mühlmann, L.; Wahl, P.; Heindel, W.; et al. Prediction of Individual Response to Electroconvulsive Therapy via Machine Learning on Structural Magnetic Resonance Imaging Data. JAMA Psychiatry 2016, 73, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Kellner, C.H.; Knapp, R.; Husain, M.M.; Rasmussen, K.; Sampson, S.; Cullum, M.; McClintock, S.M.; Tobias, K.G.; Martino, C.; Mueller, M.; et al. Bifrontal, bitemporal and right unilateral electrode placement in ECT: Randomised trial. Br. J. Psychiatry 2010, 196, 226–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Demographic and Clinical Characteristics | |
|---|---|
| n | 23 |
| Age (years) | 58.0 ± 14.6 |
| Sex (male/female) | 11/12 |
| Education (years) | 12.7 ± 4.6 |
| MADRS10 score at baseline | 37.6 ± 5.8 |
| Illness duration (months) | 212.7 ± 197.8 |
| Current episode duration (months) | 16.9 ± 12.5 |
| Number of previous hospitalizations | 2.3 ± 1.5 |
| Non-Remitters | Remitters | p Value | |
|---|---|---|---|
| n | 16 | 7 | |
| Female | 9 (56.2%) | 3 (42.9%) | 0.7 |
| Age | 57.6 (16.7) | 59.1 (9.4) | 0.9 |
| Education | 13.5 (12.0, 16.5) | 11.0 (9.0, 13.0) | 0.2 |
| Length of chronic depression (months) | 114.0 (17.5, 330.0) | 180.0 (144.0, 420.0) | 0.2 |
| Length of the actual episode (months) | 12.0 (6.0, 18.5) | 24.0 (7.5, 30.0) | 0.4 |
| Number of past hospitalizations | 2.0 (1.0, 3.0) | 2.0 (1.5, 3.0) | >0.9 |
| MADRS10 (baseline) | 39.0 (35.8, 42.2) | 34.0 (31.5, 37.5) | 0.13 |
| Number of ECT | 15.5 (14.0, 19.2) | 12.0 (11.5, 14.5) | 0.08 |
| Delta MADRS10 post ECT/baseline | −19.0 (−22.2, −13.8) | −29.0 (−35.5, −23.0) | 0.005 |
| Baseline total BDNF (ng/mL) | 22.78 (18.62, 31.73) | 31.04 (25.94, 34.62) | 0.2 |
| Baseline mature BDNF (ng/mL) | 11.45 (8.28, 14.26) | 14.41 (13.28, 18.41) | 0.047 |
| Associated medication | |||
| First generation antipsychotic | 26% | 21.70% | ns |
| atypical antipsychotic | 26% | 0% | ns |
| Other antipsychotic | 8.70% | 8.70% | ns |
| SNRI | 17.40% | 13% | ns |
| SSRI | 17.40% | 0% | ns |
| Hydroxyzine | 13% | 8.70% | ns |
| Tricyclics | 17.40% | 0% | ns |
| Characteristic | OR1 | 95% CI 1 | p-Value |
|---|---|---|---|
| mBDNF baseline | 1.38 | 1.07–2.02 | 0.04 |
| Age | 1.01 | 0.92–1.11 | 0.8 |
| Sex Female | — | — | |
| Male | 6.29 | 0.51–162 | 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Psomiades, M.; Mondino, M.; Galvão, F.; Mandairon, N.; Nourredine, M.; Suaud-Chagny, M.-F.; Brunelin, J. Serum Mature BDNF Level Is Associated with Remission Following ECT in Treatment-Resistant Depression. Brain Sci. 2022, 12, 126. https://doi.org/10.3390/brainsci12020126
Psomiades M, Mondino M, Galvão F, Mandairon N, Nourredine M, Suaud-Chagny M-F, Brunelin J. Serum Mature BDNF Level Is Associated with Remission Following ECT in Treatment-Resistant Depression. Brain Sciences. 2022; 12(2):126. https://doi.org/10.3390/brainsci12020126
Chicago/Turabian StylePsomiades, Marion, Marine Mondino, Filipe Galvão, Nathalie Mandairon, Mikail Nourredine, Marie-Françoise Suaud-Chagny, and Jérôme Brunelin. 2022. "Serum Mature BDNF Level Is Associated with Remission Following ECT in Treatment-Resistant Depression" Brain Sciences 12, no. 2: 126. https://doi.org/10.3390/brainsci12020126