
The Psychological Impact of the COVID-19 Lockdown: A Comparison between Caregivers of Autistic and Non-Autistic Individuals in Italy

 , and
, and
Abstract
:1. Introduction
- (1)
- To compare the levels of psychological wellbeing, family distress, insomnia, and resilience perceived by the caregivers of autistic people during the lockdown in Italy to those perceived by the caregivers of people with other neurodevelopmental disorders and psychiatric or relational disabilities.
- (2)
- To evaluate factors associated with the levels of individual distress reported by caregivers of autistic people during the lockdown.
2. Materials and Methods
2.1. Study Design
2.2. Measures
2.2.1. General Health Questionnaire-12 Items (GHQ-12)
2.2.2. Family Distress Index (FDI)
2.2.3. Insomnia Severity Index (ISI)
2.2.4. Brief Resilient Coping Scale (BRCS)
2.2.5. Activities of Daily Living (ADL)
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Characteristics of Autistic and Non-Autistic Family Members of Study Participants
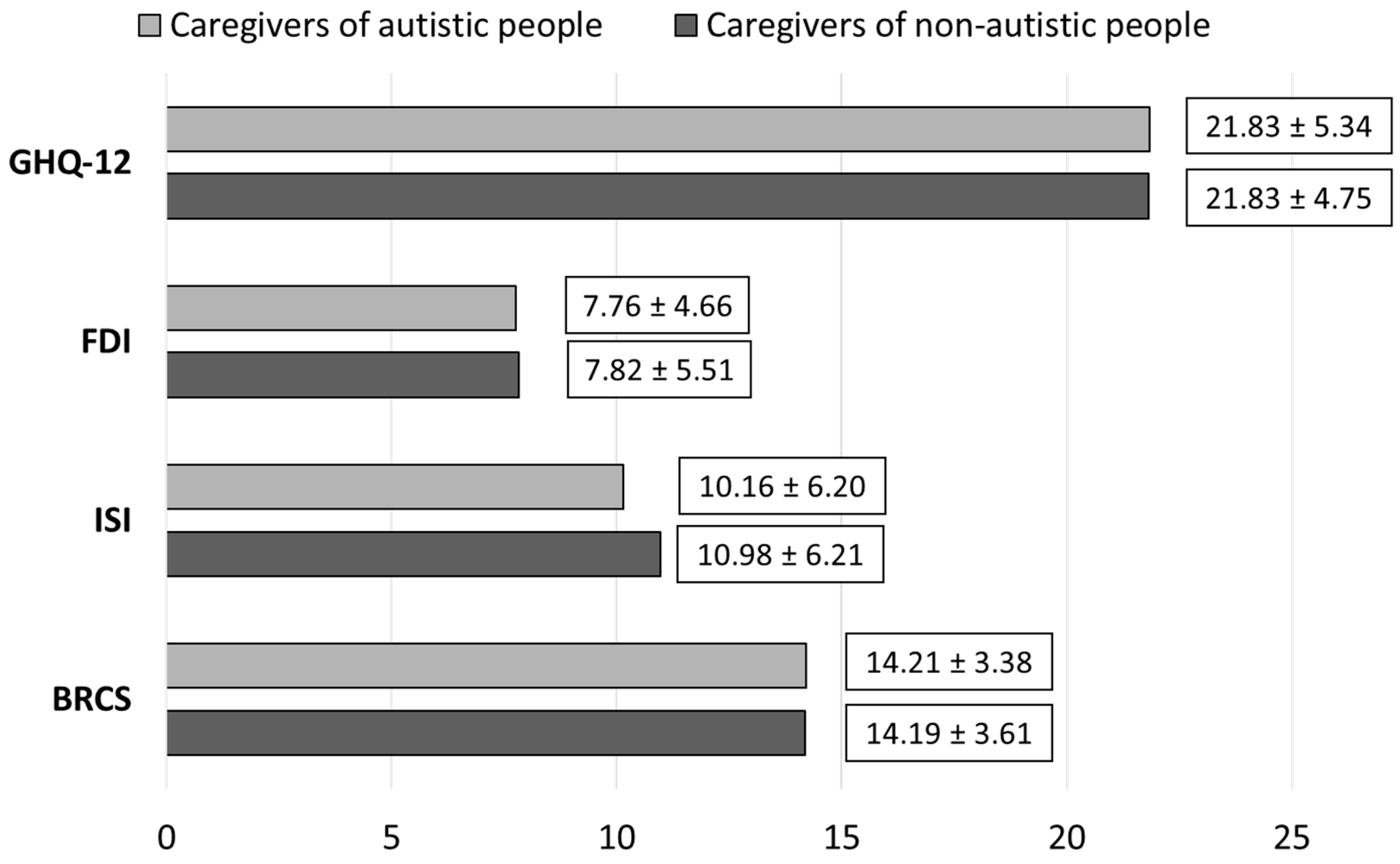
3.3. Differences in Psychological Variables between Caregivers of Autistic and Non-Autistic People
3.4. Predictors of Individual Distress (GHQ-12) among Autistic Caregivers during the Lockdown Period
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Fusar-Poli, L.; Brondino, N.; Rocchetti, M.; Panisi, C.; Provenzani, U.; Damiani, S.; Politi, P. Diagnosing ASD in adults without ID: Accuracy of the ADOS-2 and the ADI-R. J. Autism Dev. Disord. 2017, 47, 3370–3379. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, L.; Brondino, N.; Politi, P.; Aguglia, E. Missed diagnoses and misdiagnoses of adults with autism spectrum disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.P.; Zuckerman, K.E.; Hagen, A.D.; Kriz, D.J.; Duvall, S.W.; Van Santen, J.; Nigg, J.; Fair, D.; Fombonne, E. Aggressive behavior problems in children with autism spectrum disorders: Prevalence and correlates in a large clinical sample. Res. Autism Spectr. Disord. 2014, 8, 1121–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steenfeldt-Kristensen, C.; Jones, C.A.; Richards, C. The prevalence of self-injurious behaviour in autism: A meta-analytic study. J. Autism Dev. Disord. 2020, 50, 3857–3873. [Google Scholar] [CrossRef] [Green Version]
- Guinchat, V.; Cravero, C.; Lefèvre-Utile, J.; Cohen, D. Multidisciplinary treatment plan for challenging behaviors in neurodevelopmental disorders. Handb. Clin. Neurol. 2020, 174, 301–321. [Google Scholar]
- Maenner, M.J.; Shaw, K.A.; Baio, J. Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1. [Google Scholar] [CrossRef] [PubMed]
- Hollocks, M.J.; Lerh, J.W.; Magiati, I.; Meiser-Stedman, R.; Brugha, T.S. Anxiety and depression in adults with autism spectrum disorder: A systematic review and meta-analysis. Psychol. Med. 2019, 49, 559–572. [Google Scholar] [CrossRef]
- Lai, M.-C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- Muskens, J.B.; Velders, F.P.; Staal, W.G. Medical comorbidities in children and adolescents with autism spectrum disorders and attention deficit hyperactivity disorders: A systematic review. Eur. Child Adolesc. Psychiatry 2017, 26, 1093–1103. [Google Scholar] [CrossRef]
- Brondino, N.; Fusar-Poli, L.; Miceli, E.; Di Stefano, M.; Damiani, S.; Rocchetti, M.; Politi, P. Prevalence of medical comorbidities in adults with autism spectrum disorder. J. Gen. Intern. Med. 2019, 34, 1992–1994. [Google Scholar] [CrossRef]
- Lukmanji, S.; Manji, S.A.; Kadhim, S.; Sauro, K.M.; Wirrell, E.C.; Kwon, C.S.; Jetté, N. The co-occurrence of epilepsy and autism: A systematic review. Epilepsy Behav. 2019, 98, 238–248. [Google Scholar] [CrossRef]
- Nollace, L.; Cravero, C.; Abbou, A.; Mazda-Walter, B.; Bleibtreu, A.; Pereirra, N.; Sainte-Marie, M.; Cohen, D.; Giannitelli, M. Autism and COVID-19: A case series in a neurodevelopmental unit. J. Clin. Med. 2020, 9, 2937. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Sörensen, S. Differences between caregivers and noncaregivers in psychological health and physical health: A meta-analysis. Psychol. Aging 2003, 18, 250. [Google Scholar] [CrossRef]
- Bonis, S. Stress and parents of children with autism: A review of literature. Issues Ment. Health Nurs. 2016, 37, 153–163. [Google Scholar] [CrossRef]
- Vohra, R.; Madhavan, S.; Sambamoorthi, U.; St Peter, C. Access to services, quality of care, and family impact for children with autism, other developmental disabilities, and other mental health conditions. Autism 2014, 18, 815–826. [Google Scholar] [CrossRef] [Green Version]
- Derguy, C.; Michel, G.; M’bailara, K.; Roux, S.; Bouvard, M. Assessing needs in parents of children with autism spectrum disorder: A crucial preliminary step to target relevant issues for support programs. J. Intellect. Dev. Disabil. 2015, 40, 156–166. [Google Scholar] [CrossRef]
- D’Agostino, A.; Demartini, B.; Cavallotti, S.; Gambini, O. Mental health services in Italy during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, 385–387. [Google Scholar] [CrossRef]
- Starace, F.; Ferrara, M. COVID-19 disease emergency operational instructions for mental health departments issued by the Italian Society of Epidemiological Psychiatry. Epidemiol. Psychiatr. Sci. 2020, 29, e116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omboni, S. Telemedicine during the COVID-19 in Italy: A missed opportunity? Telemed. E-Health 2020, 26, 973–975. [Google Scholar] [CrossRef] [Green Version]
- Brondino, N.; Damiani, S.; Politi, P. Effective strategies for managing COVID-19 emergency restrictions for adults with severe asd in a daycare center in Italy. Brain Sci. 2020, 10, 436. [Google Scholar] [CrossRef] [PubMed]
- Lim, T.; Tan, M.Y.; Aishworiya, R.; Kang, Y.Q. Autism spectrum disorder and COVID-19: Helping caregivers navigate the pandemic. Ann. Acad. Med. 2020, 49, 384–386. [Google Scholar] [CrossRef]
- Narzisi, A. Handle the autism spectrum condition during coronavirus (COVID-19) stay at home period: Ten tips for helping parents and caregivers of young children. Brain Sci. 2020, 10, 207. [Google Scholar] [CrossRef] [Green Version]
- Shorey, S.; Lau, L.S.T.; Tan, J.X.; Ng, E.D.; Aishworiya, R. Families with children with neurodevelopmental disorders during COVID-19: A scoping review. J. Pediatr. Psychol. 2021, 46, 514–525. [Google Scholar] [CrossRef]
- Alonso-Esteban, Y.; López-Ramón, M.F.; Moreno-Campos, V.; Navarro-Pardo, E.; Alcantud-Marín, F. A systematic review on the impact of the social confinement on people with autism spectrum disorder and their caregivers during the COVID-19 pandemic. Brain Sci. 2021, 11, 1389. [Google Scholar] [CrossRef] [PubMed]
- Levante, A.; Petrocchi, S.; Bianco, F.; Castelli, I.; Colombi, C.; Keller, R.; Narzisi, A.; Masi, G.; Lecciso, F. Psychological impact of COVID-19 outbreak on families of children with autism spectrum disorder and typically developing peers: An online survey. Brain Sci. 2021, 11, 808. [Google Scholar] [CrossRef]
- Colizzi, M.; Sironi, E.; Antonini, F.; Ciceri, M.L.; Bovo, C.; Zoccante, L. Psychosocial and behavioral impact of COVID-19 in autism spectrum disorder: An online parent survey. Brain Sci. 2020, 10, 341. [Google Scholar] [CrossRef] [PubMed]
- Pellicano, L.; Brett, S.; Den Houting, J.; Heyworth, M.; Magiati, I.; Steward, R.; Urbanowicz, A.; Stears, M. “I Want to See My Friends”: The Everyday Experiences of Autistic People and Their Families during COVID-19; Macquarie University: Sydney, Australia, 2020. [Google Scholar]
- Mosquera, M.L.; Mandy, W.; Pavlopoulou, G.; Dimitriou, D. Autistic adults’ personal experiences of navigating a social world prior to and during COVID-19 lockdown in spain. Res. Dev. Disabil. 2021, 117, 104057. [Google Scholar] [CrossRef] [PubMed]
- Lugo-Marín, J.; Gisbert-Gustemps, L.; Setien-Ramos, I.; Español-Martín, G.; Ibañez-Jimenez, P.; Forner-Puntonet, M.; Arteaga-Henríquez, G.; Soriano-Día, A.; Duque-Yemail, J.D.; Ramos-Quiroga, J.A. COVID-19 pandemic effects in people with autism spectrum disorder and their caregivers: Evaluation of social distancing and lockdown impact on mental health and general status. Res. Autism Spectr. Disord. 2021, 83, 101757. [Google Scholar] [CrossRef]
- Fusar-Poli, L.; Surace, T.; Meo, V.; Patania, F.; Avanzato, C.; Pulvirenti, A.; Aguglia, E.; Signorelli, M.S. Psychological well-being and family distress of Italian caregivers during the COVID-19 outbreak. J. Community Psychol. 2021. [Google Scholar] [CrossRef]
- Politi, P.; Piccinelli, M.; Wilkinson, G. Reliability, validity and factor structure of the 12-item General Health Questionnaire among young males in Italy. Acta Psychiatr. Scand. 1994, 90, 432–437. [Google Scholar] [CrossRef]
- Piccinelli, M.; Bisoffi, G.; Bon, M.G.; Cunico, L.; Tansella, M. Validity and test-retest reliability of the Italian version of the 12-item General Health Questionnaire in general practice: A comparison between three scoring methods. Compr. Psychiatry 1993, 34, 198–205. [Google Scholar] [CrossRef]
- Castronovo, V.; Galbiati, A.; Marelli, S.; Brombin, C.; Cugnata, F.; Giarolli, L.; Anelli, M.M.; Rinaldi, F.; Ferini-Strambi, L. Validation study of the Italian version of the Insomnia Severity Index (ISI). Neurol. Sci. 2016, 37, 1517–1524. [Google Scholar] [CrossRef]
- Sinclair, V.G.; Wallston, K.A. The development and psychometric evaluation of the Brief Resilient Coping Scale. Assessment 2004, 11, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Kocalevent, R.-D.; Zenger, M.; Hinz, A.; Klapp, B.; Brähler, E. Resilient coping in the general population: Standardization of the Brief Resilient Coping sSale (BRCS). Health Qual. Life Outcomes 2017, 15, 251. [Google Scholar] [CrossRef]
- McCubbin, M.; McCubbin, H. Resiliency in families: A conceptual model of family adjustment and adaptation in response to stress and crises. Family Assessment: Resiliency, Coping and Adaptation: Inventories for Research and Practice; University of Wisconsin-Madison: Madison, WI, USA, 1996; pp. 1–64. [Google Scholar]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged: The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Banks, M.H.; Clegg, C.W.; Jackson, P.R.; Kemp, N.J.; Stafford, E.M.; Wall, T.D. The use of the general health questionnaire as an indicator of mental health in occupational studies. J. Occup. Psychol. 1980, 53, 187–194. [Google Scholar] [CrossRef]
- Bratås, O.; Grønning, K.; Forbord, T. Psychometric properties of the hospital anxiety and depression scale and the general health questionnaire-20 in copd inpatients. Scand. J. Caring Sci. 2014, 28, 413–420. [Google Scholar] [CrossRef]
- Fonseca, G.; Crespo, C.; McCubbin, L.D.; Areia, N.; Relvas, A.P. Psychometric study of the Portuguese version of the Family Distress Index (FDI). Fam. Syst. Health 2018, 36, 159. [Google Scholar] [CrossRef]
- Asbury, K.; Fox, L.; Deniz, E.; Code, A.; Toseeb, U. How is COVID-19 affecting the mental health of children with special educational needs and disabilities and their families? J. Autism Dev. Disord. 2021, 51, 1772–1780. [Google Scholar] [CrossRef]
- Fitzgerald, M.; Birkbeck, G.; Matthews, P. Maternal burden in families with children with autistic spectrum disorder. Ir. J. Psychol. 2002, 23, 2–17. [Google Scholar]
- Lounds, J.; Seltzer, M.M.; Greenberg, J.S.; Shattuck, P.T. Transition and change in adolescents and young adults with autism: Longitudinal effects on maternal well-being. Am. J. Ment. Retard. 2007, 112, 401–417. [Google Scholar] [CrossRef]
- Lenzo, V.; Quattropani, M.C.; Musetti, A.; Zenesini, C.; Freda, M.F.; Lemmo, D.; Vegni, E.; Borghi, L.; Plazzi, G.; Castelnuovo, G.; et al. Resilience contributes to low emotional impact of the COVID-19 outbreak among the general population in Italy. Front. Psychol. 2020, 11, 576485. [Google Scholar] [CrossRef]
- Sampogna, G.; Del Vecchio, V.; Giallonardo, V.; Luciano, M.; Albert, U.; Carmassi, C.; Carrà, G.; Cirulli, F.; Dell’Osso, B.; Menculini, G.; et al. What is the role of resilience and coping strategies on the mental health of the general population during the COVID-19 pandemic? Results from the Italian multicentric COMET study. Brain Sci. 2021, 11, 1231. [Google Scholar] [CrossRef] [PubMed]
- Cejalvo, E.; Martí-Vilar, M.; Merino-Soto, C.; Aguirre-Morales, M.T. Caregiving role and psychosocial and individual factors: A systematic review. Healthcare 2021, 9, 1690. [Google Scholar] [CrossRef]
- Distelberg, B.J.; Martin, A.V.S.; Borieux, M.; Oloo, W.A. Multidimensional family resilience assessment: The individual, family, and community resilience (IFCR) profile. J. Hum. Behav. Soc. Environ. 2015, 25, 552–570. [Google Scholar] [CrossRef]
- Iacob, C.I.; Avram, E.; Cojocaru, D.; Podina, I.R. Resilience in familial caregivers of children with developmental disabilities: A meta-analysis. J. Autism Dev. Disord. 2020, 50, 4053–4068. [Google Scholar] [CrossRef]
- Chakurian, D. Resilience in family caregivers of adults with autism spectrum disorder: An integrative review of the literature. Innov. Aging 2021, 5, 817–818. [Google Scholar] [CrossRef]
- Lai, M.-C.; Szatmari, P. Resilience in autism: Research and practice prospects. Autism 2019, 23, 539–541. [Google Scholar] [CrossRef] [Green Version]
- Bekhet, A.K.; Johnson, N.L.; Zauszniewski, J.A. Resilience in family members of persons with autism spectrum disorder: A review of the literature. Issues Ment. Health Nurs. 2012, 33, 650–656. [Google Scholar] [CrossRef] [PubMed]
- Ameis, S.H.; Lai, M.-C.; Mulsant, B.H.; Szatmari, P. Coping, fostering resilience, and driving care innovation for autistic people and their families during the COVID-19 pandemic and beyond. Mol. Autism 2020, 11, 61. [Google Scholar] [CrossRef]


{kind=link}
| Caregivers of Autistic People (N = 141) | Caregivers of Non-Autistic People (N = 242) | t/χ2 | p-Value | |
|---|---|---|---|---|
| Age, mean ± SD | 45.53 ± 8.89 | 51.84 ± 11.87 | −5.48 | <0.001 * |
| Gender, female (%) | 132 (93.62) | 218 (90.08) | 1.41 | 0.23 |
| Region, n (%) | 0.07 | 0.97 | ||
| Northern Italy | 75 (53.19) | 128 (52.89) | ||
| Central Italy | 25 (17.73) | 41 (16.94) | ||
| Southern Italy | 41 (29.08) | 73 (30.16) | ||
| Education, n (%) | 1.55 | 0.67 | ||
| Primary or middle school | 24 (17.02) | 34 (14.05) | ||
| High school | 72 (51.06) | 117 (48.35) | ||
| Graduate or post-graduate | 45 (31.91) | 91 (37.60) | ||
| Occupation, n (%) | 13.95 | 0.003 * | ||
| Employed | 94 (66.67) | 146 (60.33) | ||
| Unemployed | 39 (27.66) | 50 (20.66) | ||
| Retired | 8 (5.67) | 43 (17.77) | ||
| Student | 0 (0) | 3 (1.24) | ||
| N of current household members, n (%) | 11.58 | 0.009 * | ||
| 2 | 11 (7.80) | 44 (18.18) | ||
| 3 | 47 (33.33) | 92 (38.02) | ||
| 4 | 60 (42.55) | 80 (33.06) | ||
| 5 or more | 23 (16.31) | 26 (10.74) | ||
| Psychiatric disorder, n (%) | 6 (4.25) | 21 (8.68) | 2.66 | 0.10 |
| Autistic People (N = 141) | Non-Autistic People (N = 242) | t/χ2 | p-Value | |
|---|---|---|---|---|
| Age of family member, n (%) | 37.31 | <0.001 * | ||
| Children (<18 yo) | 98 (69.50) | 94 (38.84) | ||
| Adults (18–64 yo) | 43 (30.50) | 132 (54.54) | ||
| Older Adults (≥65 yo) | 0 (0) | 16 (6.61) | ||
| Gender of family member, n (%) | 11.52 | 0.001 * | ||
| Female | 26 (18.44) | 84 (34.71) | ||
| Male | 115 (81.56) | 158 (65.29) | ||
| Relationship with family member, n (%) | 25.80 | <0.001 * | ||
| Parent | 138 (97.87) | 193 (79.75) | ||
| Child | 0 (0) | 18 (7.44) | ||
| Spouse | 0 (0) | 9 (3.72) | ||
| Sibling | 3 (2.13) | 21 (8.68) | ||
| ADL, mean ± SD | 3.35 ± 1.84 | 4.32 ± 2.15 | 4.48 | <0.001 * |
| Duration of caregiving, n (%) | 4.31 | 0.36 | ||
| Less than 1 year | 6 (4.25) | 10 (4.13) | ||
| 1 to 3 years | 12 (8.51) | 21 (8.68) | ||
| 3 to 5 years | 20 (14.18) | 19 (7.85) | ||
| 5 to 10 years | 34 (24.11) | 57 (23.55) | ||
| More than 10 years | 69 (48.93) | 135 (55.78) | ||
| Daily duration of caregiving, n (%) | 22.90 | <0.001 * | ||
| Less than 3 h | 5 (3.55) | 39 (16.12) | ||
| 3 to 5 h | 9 (6.38) | 31 (12.81) | ||
| 5 to 10 h | 32 (22.69) | 59 (24.38) | ||
| More than 10 h | 95 (67.38) | 113 (46.69) | ||
| Variation of efforts, n (%) | 4.19 | 0.38 | ||
| Much increased | 43 (30.50) | 63 (26.03) | ||
| Slightly increased | 71 (50.35) | 114 (47.11) | ||
| Unchanged | 24 (17.02) | 55 (22.73) | ||
| Slightly decreased | 3 (2.13) | 7 (2.89) | ||
| Much decreased | 0 (0) | 3 (1.24) |
| Variables | B (95% CI) | Beta | t | p-Value |
|---|---|---|---|---|
| Gender | 2.09 (−1.40, 5.58) | 0.10 | 1.19 | 0.24 |
| Age | 0.13 (−0.007, 0.26) | 0.21 | 1.87 | 0.06 |
| Resilience (BRCS) | −0.49 (−0.73, −0.25) | −0.31 | −4.00 | <0.001 * |
| Gender of family member (reference: Male) | −0.67 (−2.85, 1.50) | −0.05 | −0.61 | 0.54 |
| Age of family member (reference: Adult) | 4.13 (1.56, 6.69) | 0.36 | 3.18 | 0.002 * |
| Associated intellectual disability | −1.98 (−4.30, 0.34) | −0.13 | −1.69 | 0.09 |
| Activities of Daily Living (ADL) | −0.17 (0–66, 0.32) | −0.06 | −0.67 | 0.50 |
| Total duration of caregiving (reference: More than 10 years) | ||||
| 5 to 10 years | −0.02 (−2.44, 2.40) | −0.002 | −0.02 | 0.99 |
| Less than five years | −0.37 (−2.86, 2.11) | −0.03 | −0.29 | 0.77 |
| Daily hours of caregiving (reference: More than 10 h) | ||||
| 5 to 10 h | 0.14 (−1.95, 2.22) | 0.01 | 0.13 | 0.90 |
| Less than 5 h | −2.09 (−5.17, 0.98) | −0.12 | −1.35 | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fusar-Poli, L.; Martinez, M.; Surace, T.; Meo, V.; Patania, F.; Avanzato, C.; Signorelli, M.S.; Aguglia, E. The Psychological Impact of the COVID-19 Lockdown: A Comparison between Caregivers of Autistic and Non-Autistic Individuals in Italy. Brain Sci. 2022, 12, 116. https://doi.org/10.3390/brainsci12010116
Fusar-Poli L, Martinez M, Surace T, Meo V, Patania F, Avanzato C, Signorelli MS, Aguglia E. The Psychological Impact of the COVID-19 Lockdown: A Comparison between Caregivers of Autistic and Non-Autistic Individuals in Italy. Brain Sciences. 2022; 12(1):116. https://doi.org/10.3390/brainsci12010116
Chicago/Turabian StyleFusar-Poli, Laura, Miriam Martinez, Teresa Surace, Valeria Meo, Federica Patania, Chiara Avanzato, Maria Salvina Signorelli, and Eugenio Aguglia. 2022. "The Psychological Impact of the COVID-19 Lockdown: A Comparison between Caregivers of Autistic and Non-Autistic Individuals in Italy" Brain Sciences 12, no. 1: 116. https://doi.org/10.3390/brainsci12010116