
Mental Illness and Amyloid: A Scoping Review of Scientific Evidence over the Last 10 Years (2011 to 2021)

 , , , , ,
, , , , ,
Abstract
:1. Introduction
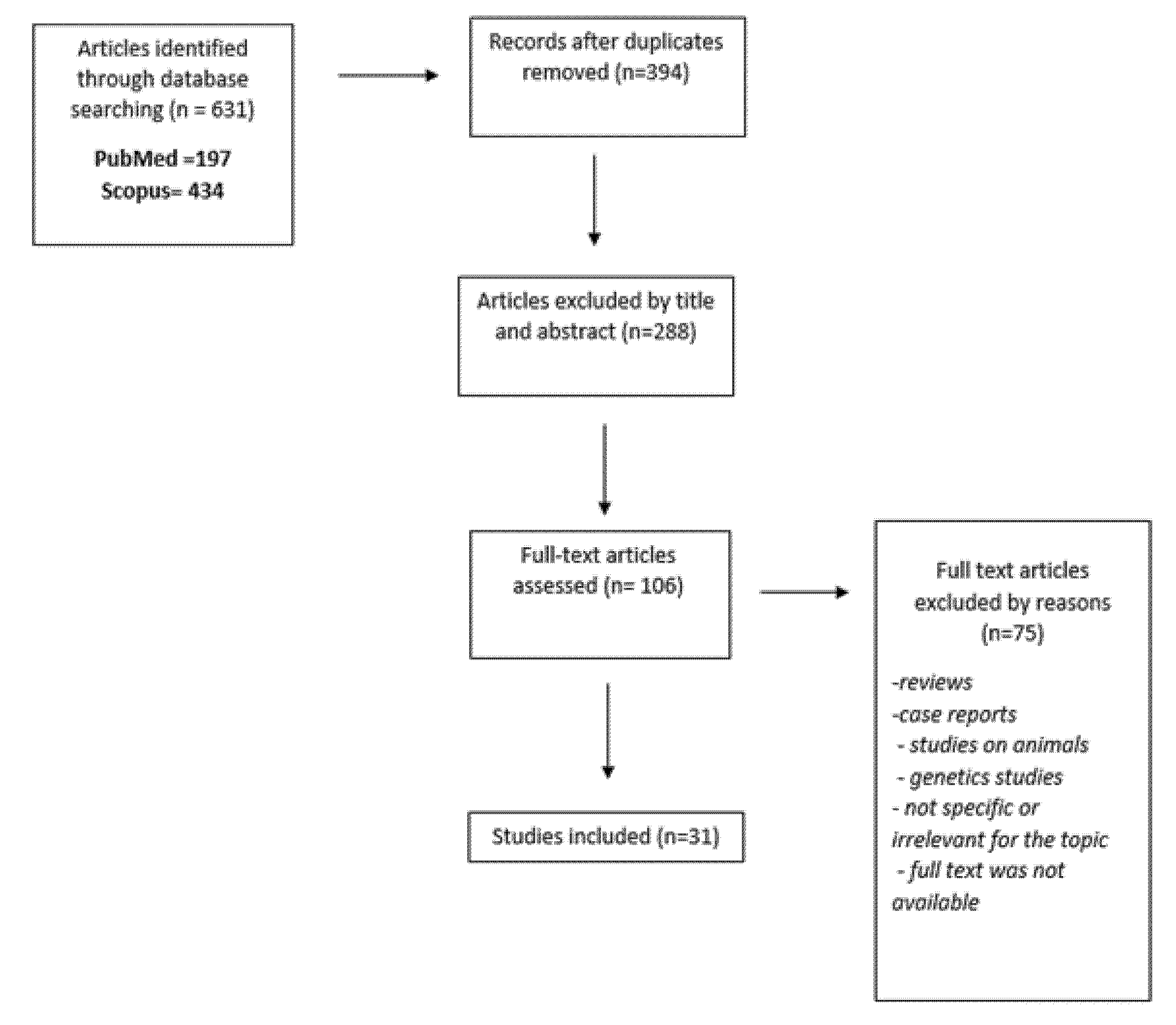
2. Materials and Methods
3. Results
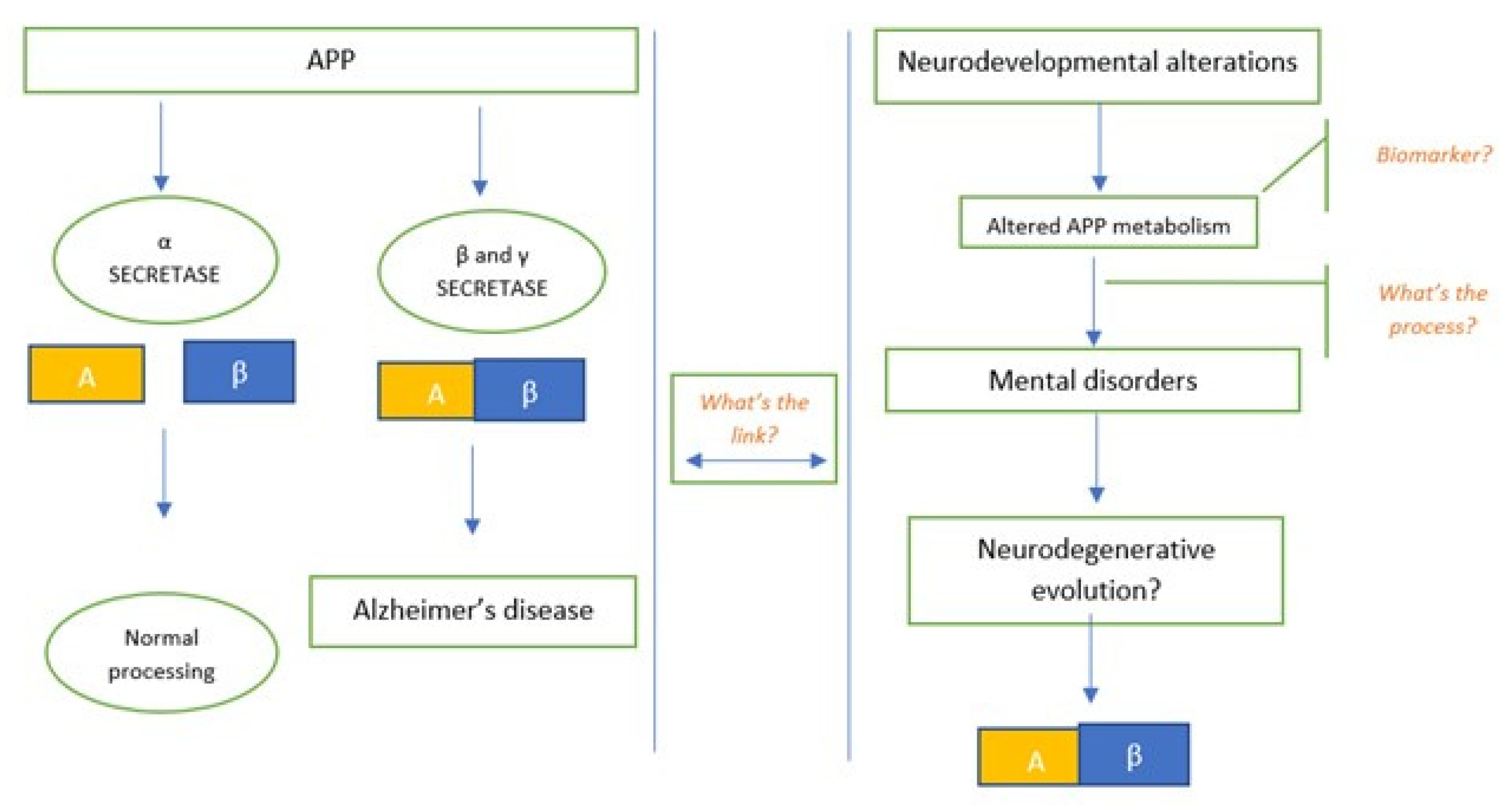
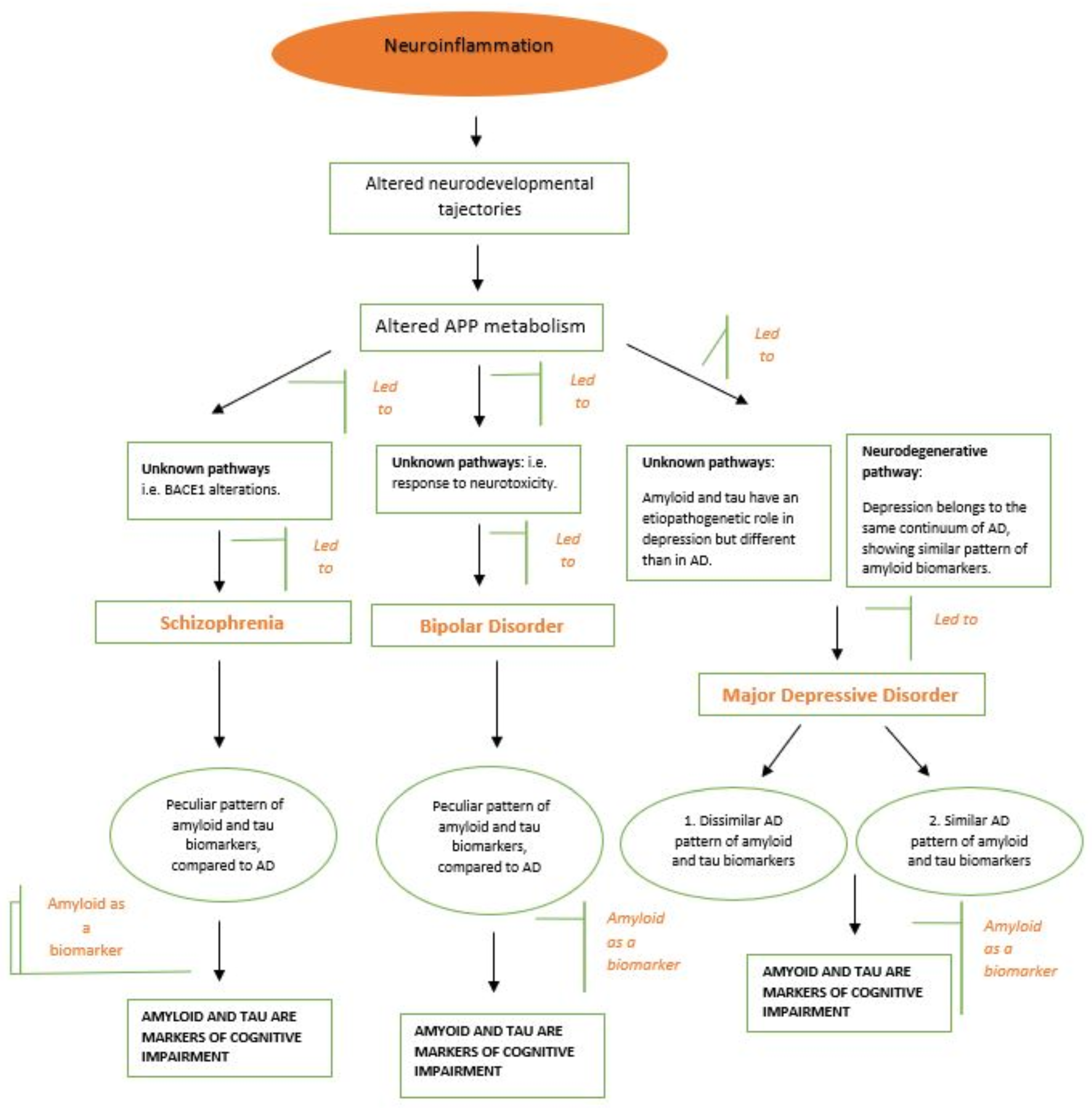
3.1. Mental Illness and Amyloid
3.2. Schizophrenia
3.3. Depression
3.4. Bipolar Disorder
3.5. Postmortem Studies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marshall, M. Roots of mental illness. Nature 2020, 581, 19–21. [Google Scholar] [CrossRef]
- Meyer, J.H.; Cervenka, S.; Kim, M.-J.; Kreisl, W.C.; Henter, I.D.; Innis, R.B. Neuroinflammation in psychiatric disorders: PET imaging and promising new targets. Lancet Psychiatry 2020, 7, 1064–1074. [Google Scholar] [CrossRef]
- Marques, T.R.; Ashok, A.; Pillinger, T.; Veronese, M.; Turkheimer, F.E.; Dazzan, P.; Sommer, I.E.; Howes, O.D. Neuroinflammation in schizophrenia: Meta-analysis of in vivo microglial imaging studies. Psychol. Med. 2019, 49, 2186–2196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, N.; Chen, Y.; Xia, Y.; Dai, J.; Liu, C. Inflammation-related biomarkers in major psychiatric disorders: A cross-disorder assessment of reproducibility and specificity in 43 meta-analyses. Transl. Psychiatry 2019, 9, 233. [Google Scholar] [CrossRef] [PubMed]
- Saccaro, L.; Schilliger, Z.; Dayer, A.; Perroud, N.; Piguet, C. Inflammation, anxiety, and stress in bipolar disorder and borderline personality disorder: A narrative review. Neurosci. Biobehav. Rev. 2021, 127, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Herron, J.W.; Nerurkar, L.; Cavanagh, J. Neuroimmune biomarkers in mental illness. In Biomarkers in Psychiatry; Springer: Berlin/Heidelberg, Germany, 2018; pp. 45–78. [Google Scholar]
- Maeda, J.; Zhang, M.-R.; Okauchi, T.; Ji, B.; Ono, M.; Hattori, S.; Kumata, K.; Iwata, N.; Saido, T.C.; Trojanowski, J.Q.; et al. In Vivo Positron Emission Tomographic Imaging of Glial Responses to Amyloid- and Tau Pathologies in Mouse Models of Alzheimer’s Disease and Related Disorders. J. Neurosci. 2011, 31, 4720–4730. [Google Scholar] [CrossRef] [Green Version]
- Kreisl, W.C.; Kim, M.-J.; Coughlin, J.M.; Henter, I.D.; Owen, D.R.; Innis, R.B. PET imaging of neuroinflammation in neurological disorders. Lancet Neurol. 2020, 19, 940–950. [Google Scholar] [CrossRef]
- Chiang, T.-I.; Hung, Y.-Y.; Wu, M.-K.; Huang, Y.-L.; Kang, H.-Y. TNIP2 mediates GRβ-promoted inflammation and is associated with severity of major depressive disorder. Brain Behav. Immun. 2021, 95, 454–461. [Google Scholar] [CrossRef]
- Bornemann, K.D.; Wiederhold, K.-H.; Pauli, C.; Ermini, F.; Stalder, M.; Schnell, L.; Sommer, B.; Jucker, M.; Staufenbiel, M. Aβ-Induced Inflammatory Processes in Microglia Cells of APP23 Transgenic Mice. Am. J. Pathol. 2001, 158, 63–73. [Google Scholar] [CrossRef]
- Mosher, K.; Wyss-Coray, T. Microglial dysfunction in brain aging and Alzheimer’s disease. Biochem. Pharmacol. 2014, 88, 594–604. [Google Scholar] [CrossRef] [Green Version]
- Wisniewski, H.M.; Wegiel, J.; Wang, K.C.; Lach, B. Ultrastructural studies of the cells forming amyloid in the cortical vessel wall in Alzheimer’s disease. Acta Neuropathol. 1992, 84, 117–127. [Google Scholar] [CrossRef]
- Koike, H.; Iguchi, Y.; Sahashi, K.; Katsuno, M. Significance of Oligomeric and Fibrillar Species in Amyloidosis: Insights into Pathophysiology and Treatment. Molecules 2021, 26, 5091. [Google Scholar] [CrossRef]
- McLean, C.A.; Cherny, R.A.; Fraser, F.W.; Fuller, S.J.; Smith, M.J.; Vbeyreuther, K.; Bush, A.I.; Masters, C.L. Soluble pool of A? amyloid as a determinant of severity of neurodegeneration in Alzheimer’s disease. Ann. Neurol. 1999, 46, 860–866. [Google Scholar] [CrossRef]
- Young-Pearse, T.; Bai, J.; Chang, R.; Zheng, J.B.; LoTurco, J.J.; Selkoe, D.J. A Critical Function for—Amyloid Precursor Protein in Neuronal Migration Revealed by In Utero RNA Interference. J. Neurosci. 2007, 27, 14459–14469. [Google Scholar] [CrossRef] [Green Version]
- Rice, H.C.; Townsend, M.; Bai, J.; Suth, S.; Cavanaugh, W.; Selkoe, D.J.; Young-Pearse, T.L. Pancortins interact with amyloid precursor protein and modulate cortical cell migration. Development 2012, 139, 3986–3996. [Google Scholar] [CrossRef] [Green Version]
- Chung, J.K.; Nakajima, S.; Plitman, E.; Iwata, Y.; Uy, D.; Gerretsen, P.; Caravaggio, F.; Chakravarty, M.M.; Graff-Guerrero, A. Β-Amyloid Burden is Not Associated with Cognitive Impairment in Schizophrenia: A Systematic Review. Am. J. Geriatr. Psychiatry 2016, 24, 923–939. [Google Scholar] [CrossRef] [Green Version]
- Harrington, K.D.; Lim, Y.Y.; Gould, E.; Maruff, P. Amyloid-beta and depression in healthy older adults: A systematic review. Aust. N. Z. J. Psychiatry 2015, 49, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Takamatsu, Y.; Ho, G.; Waragai, M.; Wada, R.; Sugama, S.; Takenouchi, T.; Masliah, E.; Hashimoto, M. Transgenerational Interaction of Alzheimer’s Disease with Schizophrenia through Amyloid Evolvability. J. Alzheimer’s Dis. 2019, 68, 473–481. [Google Scholar] [CrossRef]
- DeLisi, L.E.; Sakuma, M.; Tew, W.; Kushner, M.; Hoff, A.L.; Grimson, R. Schizophrenia as a chronic active brain process: A study of progressive brain structural change subsequent to the onset of schizophrenia. Psychiatry Res. Neuroimaging 1997, 74, 129–140. [Google Scholar] [CrossRef]
- Hidese, S.; Hattori, K.; Sasayama, D.; Tsumagari, T.; Miyakawa, T.; Matsumura, R.; Yokota, Y.; Ishida, I.; Matsuo, J.; Yoshida, S.; et al. Cerebrospinal fluid neuroplasticity-associated protein levels in patients with psychiatric disorders: A multiplex immunoassay study. Transl. Psychiatry 2020, 10, 161. [Google Scholar] [CrossRef] [PubMed]
- Fourier, A.; Formaglio, M.; Kaczorowski, F.; Mollion, H.; Perret-Liaudet, A.; Sauvee, M.; Quadrio, I. A combination of total tau and neurofilaments discriminates between neurodegenerative and primary psychiatric disorders. Eur. J. Neurol. 2020, 27, 1164–1169. [Google Scholar] [CrossRef] [PubMed]
- Frisoni, G.B.; Prestia, A.; Geroldi, C.; Adorni, A.; Ghidoni, R.; Amicucci, G.; Bonetti, M.; Soricelli, A.; Rasser, P.E.; Thompson, P.M.; et al. Alzheimer’s CSF markers in older schizophrenia patients. Int. J. Geriatr. Psychiatry 2011, 26, 640–648. [Google Scholar] [CrossRef]
- Albertini, V.; Benussi, L.; Paterlini, A.; Glionna, M.; Prestia, A.; Bocchio-Chiavetto, L.; Amicucci, G.; Galluzzi, S.; Adorni, A.; Geroldi, C.; et al. Distinct cerebrospinal fluid amyloid-beta peptide signatures in cognitive decline associated with Alzheimer’s disease and schizophrenia. Electrophoresis 2012, 33, 3738–3744. [Google Scholar] [CrossRef] [PubMed]
- Seppälä, T.T.; Louhija, U.-M.; Appelberg, B.; Herukka, S.-K.; Juva, K. Comparison Between Clinical Diagnosis and CSF Biomarkers of Alzheimer Disease in Elderly Patients with Late Onset Psychosis: Helsinki Old Age Psychosis Study (HOPS). Am. J. Geriatr. Psychiatry 2014, 22, 908–916. [Google Scholar] [CrossRef]
- Tereshkina, E.; Boksha, I.; Prokhorova, T.; Savushkina, O.; Burbaeva, G.; Morozova, M.; Mukaetova-Ladinska, E. Decrease in 130 kDa- amyloid protein precursor protein (APP) and APP protein ratio in schizophrenia platelets. Neurosci. Lett. 2020, 725, 134914. [Google Scholar] [CrossRef]
- Clarke, N.A.; Hartmann, T.; Jones, E.L.; Ballard, C.G.; Francis, P.T. Antipsychotic medication is associated with selective alterations in ventricular cerebrospinal fluid Aβ 40 and tau in patients with intractable unipolar depression. Int. J. Geriatr. Psychiatry 2011, 26, 1283–1291. [Google Scholar] [CrossRef]
- Kranaster, L.; Aksay, S.S.; Bumb, J.M.; Janke, C.; Alonso, A.; Hoyer, C.; Zerr, I.; Schmitz, M.; Hausner, L.; Frölich, L.; et al. Electroconvulsive therapy selectively enhances amyloid β 1–42 in the cerebrospinal fluid of patients with major depression: A prospective pilot study. Eur. Neuropsychopharmacol. 2016, 26, 1877–1884. [Google Scholar] [CrossRef]
- Kranaster, L.; Hoyer, C.; Aksay, S.S.; Bumb, J.M.; Müller, N.; Zill, P.; Schwarz, M.J.; Moll, N.; Lutz, B.; Bindila, L.; et al. Biomarkers for Antidepressant Efficacy of Electroconvulsive Therapy: An Exploratory Cerebrospinal Fluid Study. Neuropsychobiology 2018, 77, 13–22. [Google Scholar] [CrossRef]
- Pomara, N.; Bruno, D.; Osorio, R.; Reichert, C.; Nierenberg, J.; Sarreal, A.S.; Hernando, R.T.; Marmar, C.R.; Wisniewski, T.; Zetterberg, H.; et al. State-dependent alterations in cerebrospinal fluid Aβ42 levels in cognitively intact elderly with late-life major depression. NeuroReport 2016, 27, 1068–1071. [Google Scholar] [CrossRef] [Green Version]
- Reis, T.; Brandão, C.O.; Coutinho, E.S.F.; Engelhardt, E.; Laks, J. Cerebrospinal Fluid Biomarkers in Alzheimer’s Disease and Geriatric Depression: Preliminary Findings from Brazil. CNS Neurosci. Ther. 2012, 18, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Pomara, N.; Bruno, D.; Sarreal, A.S.; Hernando, R.T.; Nierenberg, J.; Petkova, E.; Sidtis, J.J.; Wisniewski, T.M.; Mehta, P.D.; Pratico, D.; et al. Lower CSF Amyloid Beta Peptides and Higher F2-Isoprostanes in Cognitively Intact Elderly Individuals With Major Depressive Disorder. Am. J. Psychiatry 2012, 169, 523–530. [Google Scholar] [CrossRef] [Green Version]
- Baba, H.; Nakano, Y.; Maeshima, H.; Satomura, E.; Kita, Y.; Suzuki, T.; Arai, H. Metabolism of Amyloid-β Protein May Be Affected in Depression. J. Clin. Psychiatry 2011, 73, 115–120. [Google Scholar] [CrossRef]
- Namekawa, Y.; Baba, H.; Maeshima, H.; Nakano, Y.; Satomura, E.; Takebayashi, N.; Nomoto, H.; Suzuki, T.; Arai, H. Heterogeneity of elderly depression: Increased risk of Alzheimer’s disease and Aβ protein metabolism. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 43, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Baba, H.; Yamamoto, K.; Shimada, H.; Yamakawa, Y.; Suzuki, T.; Miki, T.; Arai, H. Serum Levels of Albumin–β-Amyloid Complex in Patients with Depression. Am. J. Geriatr. Psychiatry 2016, 24, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, S.; Baba, H.; Maeshima, H.; Shimano, T.; Inoue, M.; Ichikawa, T.; Shukuzawa, H.; Suzuki, T.; Arai, H. Serum levels and mutual correlations of amyloid β in patients with depression. Geriatr. Gerontol. Int. 2020, 20, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Direk, N.; Schrijvers, E.M.; de Bruijn, R.F.; Mirza, S.; Hofman, A.; Ikram, M.A.; Tiemeier, H. Plasma amyloid β, depression, and dementia in community-dwelling elderly. J. Psychiatr. Res. 2013, 47, 479–485. [Google Scholar] [CrossRef] [Green Version]
- Yamazaki, C.; Tamaoki, T.; Nunomura, A.; Tamai, K.; Yasuda, K.; Motohashi, N. Plasma Amyloid-β and Alzheimer’s Disease-Related Changes in Late-Life Depression. J. Alzheimer’s Dis. 2017, 58, 349–354. [Google Scholar] [CrossRef]
- Zimmermann, R.; Schmitt, H.; Rotter, A.; Sperling, W.; Kornhuber, J.; Lewczuk, P. Transient increase of plasma concentrations of amyloid β peptides after electroconvulsive therapy. Brain Stimul. 2012, 5, 25–29. [Google Scholar] [CrossRef]
- Moriguchi, S.; Takahata, K.; Shimada, H.; Kubota, M.; Kitamura, S.; Kimura, Y.; Tagai, K.; Tarumi, R.; Tabuchi, H.; Meyer, J.H.; et al. Excess tau PET ligand retention in elderly patients with major depressive disorder. Mol. Psychiatry 2020, 1–8. [Google Scholar] [CrossRef]
- Wu, K.-Y.; Hsiao, I.-T.; Chen, C.-H.; Liu, C.-Y.; Hsu, J.-L.; Huang, S.-Y.; Yen, T.-C.; Lin, K.-J. Plasma Aβ analysis using magnetically-labeled immunoassays and PET 18F-florbetapir binding in non-demented patients with major depressive disorder. Sci. Rep. 2018, 8, 2739. [Google Scholar] [CrossRef]
- Wu, K.-Y.; Lin, K.-J.; Chen, C.-H.; Chen, C.-S.; Liu, C.-Y.; Huang, S.-Y.; Yen, T.-C.; Hsiao, I.-T. Diversity of neurodegenerative pathophysiology in nondemented patients with major depressive disorder: Evidence of cerebral amyloidosis and hippocampal atrophy. Brain Behav. 2018, 8, e01016. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.-Y.; Hsiao, I.-T.; Chen, C.-S.; Chen, C.-H.; Hsieh, C.-J.; Wai, Y.-Y.; Chang, C.-J.; Tseng, H.-J.; Yen, T.-C.; Liu, C.-Y.; et al. Increased brain amyloid deposition in patients with a lifetime history of major depression: Evidenced on 18F-florbetapir (AV-45/Amyvid) positron emission tomography. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 714–722. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Kepe, V.; Barrio, J.R.; Siddarth, P.; Manoukian, V.; Elderkin-Thompson, V.; Small, G.W. Protein binding in patients with late-life depression. Arch. Gen. Psychiatry 2011, 68, 1143–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakobsson, J.; Zetterberg, H.; Blennow, K.; Ekman, C.J.; Johansson, A.G.M.; Landén, M. Altered Concentrations of Amyloid Precursor Protein Metabolites in the Cerebrospinal Fluid of Patients with Bipolar Disorder. Neuropsychopharmacology 2012, 38, 664–672. [Google Scholar] [CrossRef] [Green Version]
- Rolstad, S.; Jakobsson, J.; Sellgren, C.; Ekman, C.-J.; Blennow, K.; Zetterberg, H.; Pålsson, E.; Landén, M. Cognitive Performance and Cerebrospinal Fluid Biomarkers of Neurodegeneration: A Study of Patients with Bipolar Disorder and Healthy Controls. PLoS ONE 2015, 10, e0127100. [Google Scholar] [CrossRef] [Green Version]
- Forlenza, O.V.; Aprahamian, I.; Radanovic, M.; Talib, L.L.; Camargo, M.Z.; Stella, F.; Machado-Vieira, R.; Gattaz, W. Cognitive impairment in late-life bipolar disorder is not associated with Alzheimer’s disease pathological signature in the cerebrospinal fluid. Bipolar Disord. 2016, 18, 63–70. [Google Scholar] [CrossRef] [Green Version]
- Piccinni, A.; Origlia, N.; Veltri, A.; Vizzaccaro, C.; Marazziti, D.; Catena-Dell’Osso, M.; Conversano, C.; Moroni, I.; Domenici, L.; Dell’Osso, L. Plasma β-amyloid peptides levels: A pilot study in bipolar depressed patients. J. Affect. Disord. 2012, 138, 160–164. [Google Scholar] [CrossRef]
- Piccinni, A.; Veltri, A.; Vizzaccaro, C.; Dell’Osso, M.C.; Medda, P.; Domenici, L.; Vanelli, F.; Cecchini, M.; Franceschini, C.; Conversano, C.; et al. Plasma Amyloid-β Levels in Drug-Resistant Bipolar Depressed Patients Receiving Electroconvulsive Therapy. Neuropsychobiology 2013, 67, 185–191. [Google Scholar] [CrossRef]
- Wilson, R.S.; Boyle, P.A.; Capuano, A.W.; Shah, R.C.; Hoganson, G.M.; Nag, S.; Bennett, D.A. Late-life depression is not associated with dementia-related pathology. Neuropsychology 2016, 30, 135–142. [Google Scholar] [CrossRef]
- Saldanha, N.M.; Suemoto, C.K.; Rodriguez, R.D.; Leite, R.E.P.; Nascimento, C.; Ferreti-Rebustini, R.; da Silva, M.M.; Pasqualucci, C.A.; Nitrini, R.; Jacob-Filho, W.; et al. β-amyloid pathology is not associated with depression in a large community sample autopsy study. J. Affect. Disord. 2021, 278, 372–381. [Google Scholar] [CrossRef]
- Savonenko, A.V.; Melnikova, T.; Laird, F.M.; Stewart, K.-A.; Price, D.L.; Wong, P.C. Alteration of BACE1-dependent NRG1/ErbB4 signaling and schizophrenia-like phenotypes in BACE1-null mice. Proc. Natl. Acad. Sci. USA 2008, 105, 5585–5590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbasowa, L.; Heegaard, N.H. A systematic review of amyloid-β peptides as putative mediators of the association between affective disorders and Alzheimer׳s disease. J. Affect. Disord. 2014, 168, 167–183. [Google Scholar] [CrossRef]
- Maughan, B.; Collishaw, S. Development and psychopathology: A life course perspective. In Rutter’s Child and Adolescent Psychiatry; Wiley: Hoboken, NJ, USA, 2015; Volume 6, pp. 1–16. [Google Scholar]
- Nalivaeva, N.N.; Turner, A.J. The amyloid precursor protein: A biochemical enigma in brain development, function and disease. FEBS Lett. 2013, 587, 2046–2054. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Reference | Type of Study | Subjects | Assessment | Main Findings |
|---|---|---|---|---|
| Hidese et al., 2020 | Case–control study | 94 patients with schizophrenia (SCZ), 68 with bipolar disorder (BD), 104 with major depressive disorder (MDD), and 118 healthy controls. | Assessed amyloid precursor protein (APP), BDNF, and other biomarkers. | Decreased CSF APP level in patients with schizophrenia and in those with BD. |
| Fourier et al., 2020 | Case–control study | 64 primary psychiatric patients and 162 patients with neurodegenerative disorders. | t-Tau, p-Tau, Ab42 peptide and neurofilament light chain protein were analysed in CSF. | The combination t-Tau + NfL is an association marker that permits differential diagnosis between psychiatric diseases and neurodegeneration. |
| Tereshkina et al., 2020 | Case–control study | 24 subjects with a diagnosis of acute paranoid schizophrenia (DSM-IV) and 20 controls. | The study analysed changes in amyloid precursor protein (APP). | Altered APP metabolism in schizophrenia. |
| Seppala et al., 2014 | Prospective case–control study. | 51 patients with recent psychotic symptoms and 12 comparison subjects with chronic schizophrenia over 10 years. | Levels of CSF Ab42, tau and p-tau-181 measured by ELISA. | Psychotic patients who had suffered schizophrenia for decades did not display a profile of CSF biomarkers typical for Alzheimer disease. |
| Albertini et al., 2012 | Case–control study | 20 subjects with AD, 11 elderly SCZ patients and 20 cognitively healthy controls. | Levels of CSF Ab40, Ab42, and total and P-tau proteins were determined by ELISA. | Altered APP metabolism in schizophrenia. |
| Frisoni et al., 2011 | Case–control study. | 11 older schizophrenia patients, 20 AD patients and 6 elderly controls. | CSF biomarkers of brain amyloidosis (Abeta42) and neurodegeneration (total and p-tau). | Older schizophrenia patients show a peculiar pattern of CSF Abeta42 and tau concentrations not consistent with neurodegeneration. |
| Moriguchi et al., 2020 | Case–control study | 20 patients with major depressive disorder (MDD) and 19 healthy controls. | Patients and controls were examined by PET with a tau radioligand, [11C]PBB3, and an Aβ radioligand, [11C]PiB. | Tau depositions may underlie MDD, especially in patients with psychotic symptoms. |
| Yasuda et al., 2020 | Case–control study | 104 patients with MDD and 138 healthy participants. | Serum levels of Aβ40, Aβ42 and Aβ oligomers were evaluated. | The MDD group had higher Aβ40 and lower Aβ42 serum levels compared with the control group. Possible evolution from depression to dementia mediated by A β42. |
| Saldanha et al., 2020 | Cross-sectional study | 1013 deceased subjects submitted to autopsy, with lifetime history of MDD. | Immunohistochemistry with antibody against β was performed in selected areas. | Neuritic plaque density was associated with clinical dementia but not associated with lifetime or late-life depression (LLD). |
| Kranaster et al., 2019 | Clinical trial study | 12 patients with treatment resistant depressive episode, submitted to electroconvulsive therapy (ECT). | Before the first ECT session and between one and seven days after the last ECT session, all CSF samples were drawn. | Tau protein, Aβ1-40 and neurogranin, were correlated with response to ECT. |
| Wu et al., 2018 | Case–control study | 63 elderly patients with major depressive disorder (MDD), subdivided into those with mild cognitive impairment (MCI) (n = 24) and non-MCI (n = 39) patients, and 22 control subjects. | 18F-florbetapir positron emission tomography imaging used as a biomarker of cerebral amyloidosis and the hippocampal volume used as a biomarker for neurodegeneration. | MCI-MDD patients had significantly higher amyloid deposition and greater hippocampal atrophy, followed by non-MCI MDD patients, as compared to the control subjects. |
| Wu et al., 2018 | Clinical trial | 36 non demented MDD patients. | PET imaging to evaluate amyloid brain deposition and blood sample at the same time to measure the plasma levels of Aβ40 and Aβ42. | Decreased plasma Aβ42 level and a lower Aβ42/Aβ40 ratio, in addition to an increased plasma Aβ40 level, were found to be associated with increased 18F-florbetapir binding in specific cortex areas. |
| Yamazaki et al., 2017 | Clinical trial | 42 patients with depressive episode. | Plasma amyloid levels. | LLD of BD and AD represent a possible clinical continuum and plasma A40 may have a significant role as a predictive biomarker. |
| Pomara et al., 2016 | Clinical trial | 47 patients: 28 with LLMD and 19 healthy controls. | CSF levels of Aβ42, Aβ40, t-tau and p-tau were measured at baseline and at the 3-year follow-up visit. | State-dependent association between CSF Aβ42 and depressive symptoms. |
| Kranaster et al., 2016 | Clinical trial | 12 patients with MDD. | CSF samples were drawn before the first ECT session and between one and seven days after the last ECT session. | Increase of Aβ1-42 after ECT was found in all patients with clinical response to the treatment, but not in those who did not respond. |
| Inoue et al., 2016 | Case–control study | 70 cognitively intact patients with MDD and 81 healthy participants. | Serum Aβ40 and Aβ42 levels were measured. Serum levels of albumin-Aβ complexes (SLAAC) were measured. | SLAAC is decreased in elderly patients with major depression. This decrease was not seen in younger patients. The serum-free Aβ40/Aβ42 ratio was higher in patients with depression even in younger patients. |
| Forlenza et al., 2016 | Case–control study | 72 older adults: patients with BD and mild cognitive impairment (BDMCI) (n = 16), patients with dementia due to AD (n = 17), patients with amnestic MCI (aMCI; n = 14), and cognitively healthy older adults (control group; n = 25). | CSF concentrations of Ab1-42, T-tau and P < -tau were determined. | Cognitively impaired patients with BD do not display the so-called AD bio-signature in the CSF. |
| Wilson et al., 2016 | Longitudinal clinical-pathologic study | 1965 older participants. | Assess beta-amyloid plaques and tau-tangles in 8 brain regions post-mortem. | Results do not support the hypothesis that major depression is related to neurodegenerative or cerebrovascular conditions underlying late-life dementia. |
| Wu et al., 2014 | Case–control study | 25 depressed patients and 11 nondepressed comparison subjects who did not meet the diagnostic criteria for AD or mild cognitive impairment. | 18F-florbetapir used for amyloid PET data acquisition. | Increased 18F-florbetapir uptake in specific brain regions in patients with late-life depression relative to comparison subjects. |
| Direk et al., 2013 | Longitudinal population-based cohort study | 980 participants evaluated for depressive symptoms. | Researchers’ longitudinal association between Aβ levels and depressive symptoms after excluding participants with dementia during follow-up. | Cross-sectional association between high plasma Aβ levels and clinically relevant depressive symptoms in the elderly is due to prodromal dementia. Aβ peptides may play a distinct role on depression etiology. |
| Namekawa et al., 2013 | Case–control study | 89 inpatients with MDD divided into two groups based on age at onset of MDD: <60 years and ≥60 years, 111 healthy controls. | Evaluated serum Aβ40 and Aβ42 levels, the Aβ40/Aβ42 ratio. | The serum Aβ40/Aβ42 ratio was significantly higher in elderly patients with both early-onset and late-onset MDD than in age-matched controls. |
| Pomara et al., 2012 | Case–control study | 28 cognitively intact patients with major depression and 19 healthy controls. | Analysed CSF levels of amyloid beta 40 and 42. | Elderly, cognitively intact individuals with major depressive disorder have reductions in CSF levels of amyloid beta 42 similar to individuals with Alzheimer’s disease or mild cognitive impairment. |
| Reis et al., 2012 | Case–control study | 52 with a diagnosis of MDD, AD, and healthy controls. | Measurement of CSF P-tau181, T-tau, and Aβ42 was performed using commercial assays (ELISA). | CSF Aβ42 levels were significantly lower and T--tau levels were significantly higher in AD patients as compared to MDD and control groups. Aβ42/T--tau and Aβ42/P--tau ratios were significantly lower in AD patients as compared to the MDD and healthy groups. |
| Baba et al., 2012 | Case–control study | 93 patients with major depressive disorder (MDD) and 413 healthy controls. | Serum Aβ40 and Aβ42 levels, Aβ40/Aβ42 ratio, and other clinical and biological factors were compared between controls. | Serum Aβ40/Aβ42 ratio was significantly higher in MDD patients than in the controls. |
| Kumar et al., 2011 | A cross-section neuroimaging study | 20 patients with MDD and 19 healthy control individuals. | [(18)F]FDDNP binding (PET measurement for amyloid and tau) in critical brain regions. | [(18)F]FDDNP binding was significantly higher overall and in the posterior cingulate and lateral temporal regions in the MDD group, compared to the controls. |
| Zimmermann et al., 2012 | Clinical trial | 13 patients. | Plasma concentrations of amyloid b (Ab) peptides before ECT, within 30 min after, and 24 h after ECT treatment. | Increase of the plasma concentrations of all four peptides within 30 min after the ECT, followed by the normalization of the peptides concentrations 2 h after the ECT. |
| Clarke et al., 2011 | Cross-sectional study | 32 patients with resistant MDD divided into two groups according to treatment with antipsychotics. | CSF tau and amyloid concentrations. | Increments of Ab 1–40 and total levels of tau in V-CSF, in patients with treatment-resistant MDD receiving antipsychotics compared to those individuals not receiving antipsychotic treatment. |
| Rolstand et al., 2015 | Case–control study | 82 euthymic bipolar disorder patients and 71 healthy controls. | CSF concentrations of total and phosphorylated tau, amyloid beta (Aβ)1-42, ratios of Aβ42/40 and Aβ42/38, soluble amyloid precursor protein α and β, and neurofilament light chain protein. | CSF biomarkers of neurodegeneration were associated with cognitive performance in euthymic bipolar disorder, but not in healthy controls. |
| Piccinni et al., 2013 | Clinical trial | 25 patients suffering from bipolar I or II depressive episodes with or without psychotic symptoms according to DSM-IV-TR criteria. | Aβ40 and Aβ42 were measured by ELISA assay in patients before (T0) and 1 week after (T1) the end of ECT. | Low Aβ40/Aβ42 ratio might characterize a subgroup of depressed patients who respond to ECT, while higher values of this parameter seem to be typical of more severe cases of patients with cognitive impairment. |
| Jakobsson et al., 2013 | Randomized controlled trial | 139 bipolar patients and 71 healthy controls. | Neuropsychological assessments+ Analysis of the CSF concentrations of sAPP-a and sAPP-b, and Ab38, Ab40, and Ab42, hyperphosphorylated-Tau (P-tau), totaltau (T-tau), and Ab1-42. | Amyloid precursor protein metabolism is altered in bipolar disorder. |
| Piccinni et al., 2012 | Case–control study | 16 patients with bipolar depression type I or II and 16 control subjects. | Levels of Aβ40 and Aβ42 were measured by using specific ELISA kits. | Patients presented significantly lower plasma Aβ42 levels and higher Aβ40/Aβ42 ratio, as compared with control subjects. Positive correlation between the Aβ40/Aβ42 ratio and the number of affective episodes. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pandolfo, G.; Iannuzzo, F.; Genovese, G.; Bruno, A.; Pioggia, G.; Baldari, S.; Gangemi, S. Mental Illness and Amyloid: A Scoping Review of Scientific Evidence over the Last 10 Years (2011 to 2021). Brain Sci. 2021, 11, 1352. https://doi.org/10.3390/brainsci11101352
Pandolfo G, Iannuzzo F, Genovese G, Bruno A, Pioggia G, Baldari S, Gangemi S. Mental Illness and Amyloid: A Scoping Review of Scientific Evidence over the Last 10 Years (2011 to 2021). Brain Sciences. 2021; 11(10):1352. https://doi.org/10.3390/brainsci11101352
Chicago/Turabian StylePandolfo, Gianluca, Fiammetta Iannuzzo, Giovanni Genovese, Antonio Bruno, Giovanni Pioggia, Sergio Baldari, and Sebastiano Gangemi. 2021. "Mental Illness and Amyloid: A Scoping Review of Scientific Evidence over the Last 10 Years (2011 to 2021)" Brain Sciences 11, no. 10: 1352. https://doi.org/10.3390/brainsci11101352