
The Neurobiological Basis of Cognitive Side Effects of Electroconvulsive Therapy: A Systematic Review

 , , ,
, , ,
Abstract
:1. Introduction
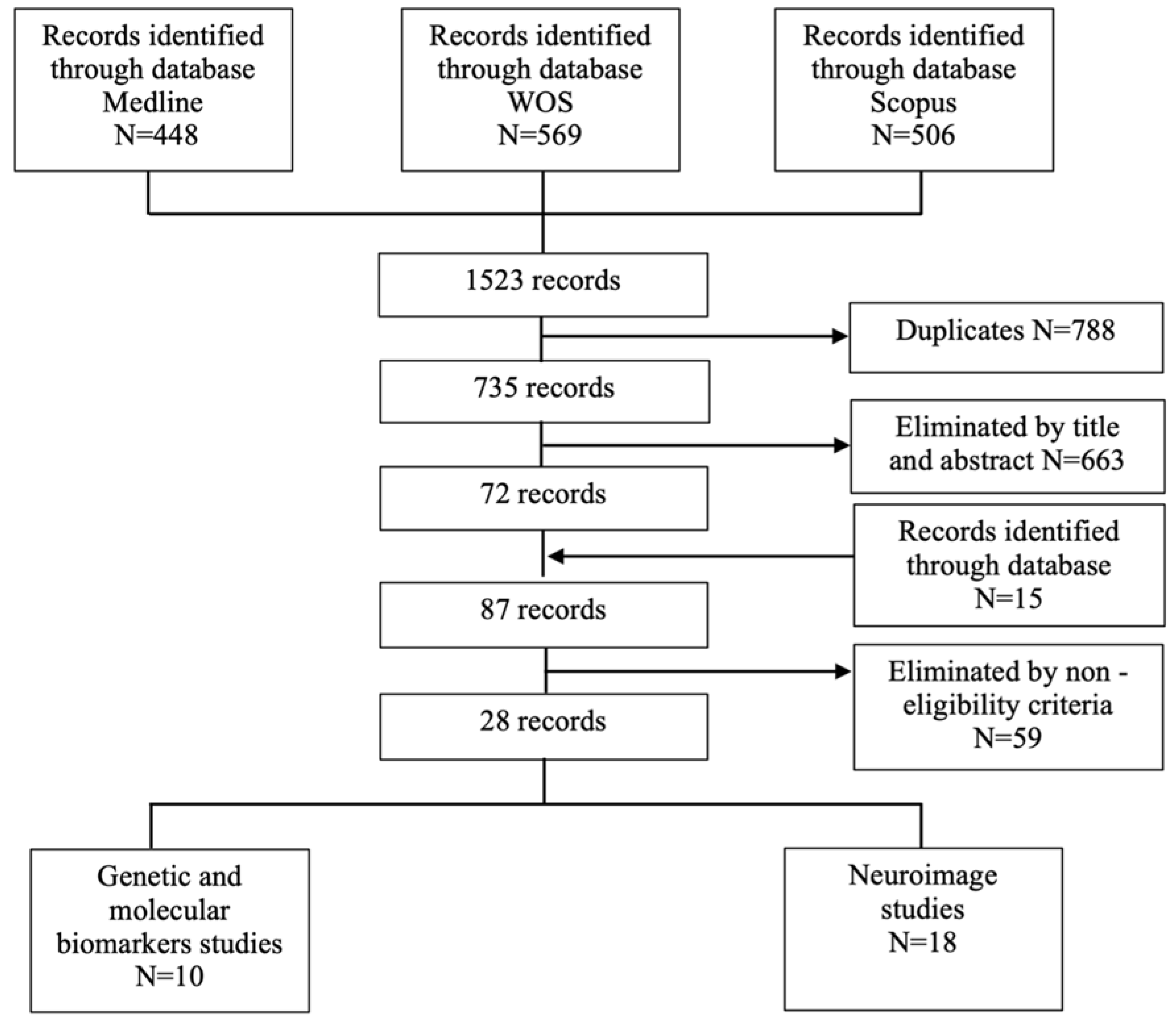
2. Materials and Methods
3. Results
3.1. Genetic and Molecular Biomarkers
3.1.1. Protein S-100 and Neuron-Specific Enolase (NSE)
3.1.2. Aβ Peptides
3.1.3. Genetics
3.1.4. Cortisol
3.2. Neuroimaging-Based Biomarkers
3.2.1. Structural Magnetic Resonance Imaging
3.2.2. Functional Magnetic Resonance Imaging
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lisanby, S.H.; McClintock, S.M.; Alexopoulos, G.; Bailine, S.H.; Bernhardt, E.; Briggs, M.C.; Cullum, C.M.; De Deng, Z.; Dooley, M.; Geduldig, E.T.; et al. Neurocognitive Effects of Combined Electroconvulsive Therapy (ECT) and Venlafaxine in Geriatric Depression: Phase 1 of the PRIDE Study. Am. J. Geriatr. Psychiatry 2020, 28, 304–316. [Google Scholar] [CrossRef] [PubMed]
- McClintock, S.M.; Choi, J.; Deng, Z.-D.; Appelbaum, L.G.; Krystal, A.D.; Lisanby, S.H. Multifactorial Determinants of the Neurocognitive Effects of Electroconvulsive Therapy. J. ECT 2014, 30, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Sobin, C.; Sackeim, H.A.; Prudic, J.; Devanand, D.P.; Moody, B.J.; McElhiney, M.C. Predictors of retrograde amnesia following ECT. Am. J. Psychiatry 1995, 152, 995–1001. [Google Scholar] [CrossRef] [PubMed]
- Loo, C.K.; Schweitzer, I.; Pratt, C. Recent advances in optimizing electroconvulsive therapy. Aust. N. Z. J. Psychiatry 2006, 40, 632–638. [Google Scholar] [CrossRef]
- Sackeim, H.A. The impact of electroconvulsive therapy on brain grey matter volume: What does it mean? Brain Stimul. 2020, 13, 1226–1231. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Min, S.; Wei, K.; Li, P.; Dong, J.; Liu, Y.-F.Y.-F.Y. Propofol protects against impairment of learning-memory and imbalance of hippocampal Glu/GABA induced by electroconvulsive shock in depressed rats. J. Anesth. 2011, 25, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Reid, I.C.; Stewart, C.A. Seizures, memory and synaptic plasticity. Seizure 1997, 6, 351–359. [Google Scholar] [CrossRef]
- Zhang, F.; Luo, J.; Min, S.; Ren, L.; Qin, P. Propofol alleviates electroconvulsive shock-induced memory impairment by modulating proBDNF/mBDNF ratio in depressive rats. Brain Res. 2016, 1642, 43–50. [Google Scholar] [CrossRef]
- Wang, J.; Gallagher, D.; Devito, L.M.; Cancino, G.I.; Tsui, D.; He, L.; Keller, G.M.; Frankland, P.W.; Kaplan, D.R.; Miller, F.D. Metformin activates an atypical PKC-CBP pathway to promote neurogenesis and enhance spatial memory formation. Cell Stem Cell 2012, 11, 23–35. [Google Scholar] [CrossRef]
- Diehl, D.J.; Keshavan, M.S.; Kanal, E.; Nebes, R.D.; Nichols, T.E.; Gillen, J.S. Post-ECT increases in MRI regional T2 relaxation times and their relationship to cognitive side effects: A pilot study. Psychiatry Res. 1994, 54, 177–184. [Google Scholar] [CrossRef]
- Paszkiel, S. Data Acquisition Methods for Human Brain Activity, ANALYSIS and Classification of Eeg Signals for Brain-Computer Interfaces; Book Series: Studies in Computational Intelligence; Springer: Cham, Switzerland, 2020; Volume 852, pp. 3–9. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097-6. [Google Scholar] [CrossRef]
- Porta-Casteràs, D.; Cano, M.; Camprodon, J.A.; Loo, C.; Palao, D.; Soriano-Mas, C.; Cardoner, N. A multimetric systematic review of fMRI findings in patients with MDD receiving ECT. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 108. [Google Scholar] [CrossRef]
- Scottish Intercollegiate Guidelines Network. Methodology Checklist 2: Controlled Trials. 2012, pp. 3–5. Available online: https://www.sign.ac.uk/what-we-do/methodology/checklists/ (accessed on 22 September 2021).
- Li, W.; Chen, Z.; Wu, M.; Zhu, H.; Gu, L.; Zhao, Y.; Kuang, W.; Bi, F.; Kemp, G.J.; Gong, Q. Characterization of brain blood flow and the amplitude of low-frequency fluctuations in major depressive disorder: A multimodal meta-analysis. J. Affect. Disord. 2017, 210, 303–311. [Google Scholar] [CrossRef]
- Agelink, M.W.; Andrich, J.; Postert, T.; Würzinger, U.; Zeit, T.; Klotz, P.; Przuntek, H. Relation between electroconvulsive therapy, cognitive side effects, neuron specific enolase, and protein S-100. J. Neurol. Neurosurg. Psychiatry 2001, 71, 394–396. [Google Scholar] [CrossRef]
- Palmio, J.; Huuhka, M.; Laine, S.; Huhtala, H.; Peltola, J.; Leinonen, E.; Suhonen, J.; Keränen, T. Electroconvulsive therapy and biomarkers of neuronal injury and plasticity: Serum levels of neuron-specific enolase and S-100b protein. Psychiatry Res. 2010, 177, 97–100. [Google Scholar] [CrossRef]
- Kranaster, L.; Janke, C.; Mindt, S.; Neumaier, M.; Sartorius, A. Protein S-100 and neuron-specific enolase serum levels remain unaffected by electroconvulsive therapy in patients with depression. J. Neural. Transm. 2014, 121, 1411–1415. [Google Scholar] [CrossRef] [PubMed]
- Arts, B.; Peters, M.; Ponds, R.; Honig, A.; Menheere, P.; van Os, J. S100 and impact of ECT on depression and cognition. J. ECT 2006, 22, 206–212. [Google Scholar] [CrossRef]
- Piccinni, A.; Veltri, A.; Vizzaccaro, C.; Catena Dell’Osso, M.; Medda, P.; Domenici, L.; Vanelli, F.; Cecchini, M.; Franceschini, C.; Conversano, C.; et al. Plasma amyloid-β levels in drug-resistant bipolar depressed patients receiving electroconvulsive therapy. Neuropsychobiology 2013, 67, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Kranaster, L.; Aksay, S.S.; Bumb, J.M.; Janke, C.; Alonso, A.; Hoyer, C.; Zerr, I.; Schmitz, M.; Hausner, L.; Frölich, L.; et al. Electroconvulsive therapy selectively enhances amyloid β 1–42 in the cerebrospinal fluid of patients with major depression: A prospective pilot study. Eur. Neuropsychopharmacol. 2016, 26, 1877–1884. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, C.; Tamaoki, T.; Nunomura, A.; Tamai, K.; Yasuda, K.; Motohashi, N. Plasma Amyloid-beta and Alzheimer’s Disease-Related Changes in Late-Life Depression. J. Alzheimers. Dis. 2017, 58, 349–354. [Google Scholar] [CrossRef]
- Bousman, C.A.; Katalinic, N.; Martin, D.M.; Smith, D.J.; Ingram, A.; Dowling, N.; Ng, C.; Loo, C.K. Effects of COMT, DRD2, BDNF, and APOE genotypic variation on treatment efficacy and cognitive side effects of electroconvulsive therapy. J. ECT 2015, 31, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Karen, R.; McLoughlin, D.M. Telomere length in depression and association with therapeutic response to electroconvulsive therapy and cognitive side-effects. Psychol. Med. 2020, 50, 2096–2106. [Google Scholar] [CrossRef]
- Neylan, T.C.; Canick, J.D.; Hall, S.E.; Reus, V.I.; Sapolsky, R.M.; Wolkowitz, O.M. Cortisol levels predict cognitive impairment induced by electroconvulsive therapy. Biol. Psychiatry 2001, 50, 331–336. [Google Scholar] [CrossRef]
- Figiel, G.S.; Ranga, K.; Krishnan, R.; Doraiswamy, P.M. Subcortical Structural Changes in ECT-Induced Delirium. J. Geriatr. Psychiatry Neurol. 1990, 3, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Oudega, M.L.; Dols, A.; Adelerhof, I.; Rozing, M.; Wattjes, M.P.; Comijs, H.C.; Barkhof, F.; Eikelenboom, P.; Stek, M.L.; Van Exel, E. Contribution of white matter hyperintensities, medial temporal lobe atrophy and cortical atrophy on outcome, seven to twelve years after ECT in severely depressed geriatric patients (INTERROGANT). J. Affect. Disord. 2015, 185, 144–148. [Google Scholar] [CrossRef]
- Wagenmakers, M.J.; Vansteelandt, K.; van Exel, E.; Postma, R.; Schouws, S.N.T.M.; Obbels, J.; Rhebergen, D.; Bouckaert, F.; Stek, M.L.; Barkhof, F.; et al. Transient Cognitive Impairment and White Matter Hyperintensities in Severely Depressed Older Patients Treated With Electroconvulsive Therapy. Am. J. Geriatr. Psychiatry 2021. [Google Scholar] [CrossRef]
- Kunigiri, G.; Jayakumar, P.N.; Janakiramaiah, N.; Gangadhar, B.N. MRI T(2) relaxometry of brain regions and cognitive dysfunction following electroconvulsive therapy. Indian J. Psychiatry 2007, 49, 195–199. [Google Scholar] [CrossRef]
- Gbyl, K.; Rostrup, E.; Raghava, J.M.; Carlsen, J.F.; Schmidt, L.S.; Lindberg, U.; Ashraf, A.; Jørgensen, M.B.; Larsson, H.B.W.; Rosenberg, R.; et al. Cortical thickness following electroconvulsive therapy in patients with depression: A longitudinal MRI study. Acta Psychiatr. Scand. 2019, 140, 205–216. [Google Scholar] [CrossRef]
- Xu, J.; Wang, J.; Bai, T.; Zhang, X.; Li, T.; Hu, Q.; Li, H.; Zhang, L.; Wei, Q.; Tian, Y.; et al. Electroconvulsive Therapy Induces Cortical Morphological Alterations in Major Depressive Disorder Revealed with Surface-Based Morphometry Analysis. Int. J. Neural. Syst. 2019, 29, 1950005. [Google Scholar] [CrossRef]
- Lekwauwa, R.; McQuoid, D.; Steffens, D.C. Hippocampal volume is associated with physician-reported acute cognitive deficits after electroconvulsive therapy. J. Geriatr. Psychiatry Neurol. 2006, 19, 21–25. [Google Scholar] [CrossRef]
- Nordanskog, P.; Larsson, M.R.; Larsson, E.M.; Johanson, A. Hippocampal volume in relation to clinical and cognitive outcome after electroconvulsive therapy in depression. Acta Psychiatr. Scand. 2014, 129, 303–311. [Google Scholar] [CrossRef]
- Van Oostrom, I.; Van Eijndhoven, P.; Butterbrod, E.; Van Beek, M.H.; Janzing, J.; Donders, R.; Schene, A.; Tendolkar, I. Decreased Cognitive Functioning after Electroconvulsive Therapy Is Related to Increased Hippocampal Volume: Exploring the Role of Brain Plasticity. J. ECT 2018, 34, 117–123. [Google Scholar] [CrossRef]
- Gbyl, K.; Støttrup, M.M.; Mitta Raghava, J.; Xue Jie, S.; Videbech, P. Hippocampal volume and memory impairment after electroconvulsive therapy in patients with depression. Acta Psychiatr. Scand. 2020. [Google Scholar] [CrossRef]
- Abbott, C.C.; Jones, T.; Lemke, N.T.; Gallegos, P.; McClintock, S.M.; Mayer, A.R.; Bustillo, J.; Calhoun, V.D. Hippocampal structural and functional changes associated with electroconvulsive therapy response. Transl. Psychiatry 2014, 4, S562–S563. [Google Scholar] [CrossRef] [PubMed]
- Bai, T.; Wei, Q.; Xie, W.; Wang, A.; Wang, J.; Ji, G.J.; Wang, K.; Tian, Y. Hippocampal-subregion functional alterations associated with antidepressant effects and cognitive impairments of electroconvulsive therapy. Psychol. Med. 2019, 49, 1357–1364. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wei, Q.; Wang, C.; Xu, J.; Wang, K.; Tian, Y.; Wang, J. Altered functional connectivity patterns of insular subregions in major depressive disorder after electroconvulsive therapy. Brain Imaging Behav. 2019, 14, 753–761. [Google Scholar] [CrossRef]
- Wang, D.; Tian, Y.; Li, M.; Dahmani, L.; Wei, Q.; Bai, T.; Galiè, F.; Ren, J.; Farooq, R.K.; Wang, K.; et al. Functional connectivity underpinnings of electroconvulsive therapy-induced memory impairments in patients with depression. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2020, 45, 1579–1587. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.; Reddy, R.V.; Srivastava, P.; Mehta, U.M.; Bharath, R.D. Network neurobiology of electroconvulsive therapy in patients with depression. Psychiatry Res.-Neuroimaging 2019, 287, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Bai, T.; Brown, E.C.; Xie, W.; Chen, Y.; Ji, G.; Ramasubbu, R.; Tian, Y.; Wang, K. Thalamocortical connectivity in electroconvulsive therapy for major depressive disorder. J. Affect. Disord. 2020, 264, 163–171. [Google Scholar] [CrossRef]
- Wei, Q.; Ji, Y.; Bai, T.; Zu, M.; Guo, Y.; Mo, Y.; Ji, G.; Wang, K.; Tian, Y. Enhanced cerebro-cerebellar functional connectivity reverses cognitive impairment following electroconvulsive therapy in major depressive disorder. Brain Imaging Behav. 2020. [Google Scholar] [CrossRef]
- Donato, R.; Cannon, B.; Sorci, G.; Riuzzi, F.; Hsu, K.; Weber, D.; Geczy, C. Functions of S100 Proteins. Curr. Mol. Med. 2012, 13, 24–57. [Google Scholar] [CrossRef]
- Haque, A.; Polcyn, R.; Matzelle, D.; Banik, N.L. New insights into the role of neuron-specific enolase in neuro-inflammation, neurodegeneration, and neuroprotection. Brain Sci. 2018, 8, 33. [Google Scholar] [CrossRef]
- Gatti, L.; Tinelli, F.; Scelzo, E.; Arioli, F.; Di Fede, G.; Obici, L.; Pantoni, L.; Giaccone, G.; Caroppo, P.; Parati, E.A.; et al. Understanding the pathophysiology of cerebral amyloid angiopathy. Int. J. Mol. Sci. 2020, 21, 3435. [Google Scholar] [CrossRef]
- Janelidze, S.; Zetterberg, H.; Mattsson, N.; Palmqvist, S.; Vanderstichele, H.; Lindberg, O.; van Westen, D.; Stomrud, E.; Minthon, L.; Blennow, K.; et al. CSF Aβ42/Aβ40 and Aβ42/Aβ38 ratios: Better diagnostic markers of Alzheimer disease. Ann. Clin. Transl. Neurol. 2016, 3, 154–165. [Google Scholar] [CrossRef] [PubMed]
- Colaianna, M.; Tucci, P.; Zotti, M.; Morgese, M.; Schiavone, S.; Govoni, S.; Cuomo, V.; Trabace, L. Soluble βamyloid 1-42: A critical player in producing behavioural and biochemical changes evoking depressive-related state? Br. J. Pharmacol. 2010, 159, 1704–1715. [Google Scholar] [CrossRef] [PubMed]
- Cano, M.; Martínez-Zalacaín, I.; Bernabéu-Sanz, A.; Contreras-Rodríguez, O.; Hernández-Ribas, R.; Via, E.; De Arriba-Arnau, A.; Gálvez, V.; Urretavizcaya, M.; Pujol, J.; et al. Brain volumetric and metabolic correlates of electroconvulsive therapy for treatment-resistant depression: A longitudinal neuroimaging study. Transl. Psychiatry 2017, 7, e1023–e1028. [Google Scholar] [CrossRef]
- Dukart, J.; Regen, F.; Kherif, F.; Colla, M.; Bajbouj, M.; Heuser, I.; Frackowiak, R.S.; Draganski, B. Electroconvulsive therapy-induced brain plasticity determines therapeutic outcome in mood disorders. Proc. Natl. Acad. Sci. USA 2014, 111, 1156–1161. [Google Scholar] [CrossRef]
- Joshi, S.H.; Espinoza, R.T.; Pirnia, T.; Shi, J.; Wang, Y.; Ayers, B.; Leaver, A.; Woods, R.P.; Narr, K.L. Structural plasticity of the hippocampus and amygdala induced by electroconvulsive therapy in major depression. Biol. Psychiatry 2016, 79, 282–292. [Google Scholar] [CrossRef] [PubMed]
- Seung-Gul, K.; Seo-Eun, C. Neuroimaging Biomarkers for Predicting Treatment Response and Recurrence of Major Depressive Disorder. Mol. Sci. 2020, 21, 2148. [Google Scholar] [CrossRef]
- Dickerson, B.C.; Eichenbaum, H. The episodic memory system: Neurocircuitry and disorders. Neuropsychopharmacology 2010, 35, 86–104. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Liu, S.; Guo, M.; Yang, C.X.; Xu, Y. The principles of electroconvulsive therapy based on correlations of schizophrenia and epilepsy: A view from brain networks. Front. Neurol. 2019, 10, 688. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Kar, S.K. How electroconvulsive therapy works?: Understanding the neurobiological mechanisms. Clin. Psychopharmacol. Neurosci. 2017, 15, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Oltedal, L.; Bartsch, H.; Sørhaug, O.J.E.; Kessler, U.; Abbott, C.; Dols, A.; Stek, M.L.; Ersland, L.; Emsell, L.; van Eijndhoven, P.; et al. The Global ECT-MRI Research Collaboration (GEMRIC): Establishing a multi-site investigation of the neural mechanisms underlying response to electroconvulsive therapy. NeuroImage Clin. 2017, 14, 422–432. [Google Scholar] [CrossRef]
- Soda, T.; McLoughlin, D.M.; Clark, S.R.; Oltedal, L.; Kessler, U.; Haavik, J.; Bousman, C.; Smith, D.J.; Bioque, M.; Clements, C.C.; et al. International Consortium on the Genetics of Electroconvulsive Therapy and Severe Depressive Disorders (Gen-ECT-ic). Eur. Arch. Psychiatry Clin. Neurosci. 2020, 270, 921–932. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.M.; Gálvez, V.; Lauf, S.; Dong, V.; Baily, S.A.; Cardoner, N.; Chan, H.N.; Davidson, D.; Fam, J.; De Felice, N.; et al. The Clinical Alliance and Research in Electroconvulsive Therapy Network: An Australian Initiative for Improving Service Delivery of Electroconvulsive Therapy. J. ECT 2018, 34, 7–13. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Measure | N | Diagnosis Gender/Age (Mean, Years) Medication Status | ECT Parameters | Time-Points | Cognitive Scales | Significant Results | Quality Index |
|---|---|---|---|---|---|---|---|---|
| Agelink et al. 2001 | NSE, S-100 | 14 | MDD, Schizoaffective depression 5W, 9M/54 Y NM (only lorazepam) | Not described | 1 day before ECT, 6 h, 24 h, and 48 h after the 1st to 3rd ECT and 24 h after the 4th, 5th, 6th, and last ECT | IMC, a subtest of Blessed dementia scales (orientation, memory, and concentration), digit span test, and A-E SKT | Patients with higher post-ECT S-100 values showed better cognitive performance | 4 |
| Palmio et al. 2009 | NSE, S-100b | 10 | Unipolar depression (with psychotic symptoms) 7W, 3M/56 Y SM | BFT, brief 3.8 sessions | Pre-ECT and 1 h, 2 h, 6 h, 24 h, and 48 h after | MMSE | - | 5 |
| Kranaster et al. 2014 | NSE, S-100 | 19 | Unipolar and bipolar depression 11W, 8M/66 Y | 9.4 sessions | Pre-ECT, 30 and 60 min after the 3rd ECT and post-ECT | MMSE | Pre-ECT NSE concentration was negatively correlated with MMSE scores at baseline | 5.5 |
| Arts et al. 2006 | S100-beta | 12 | Unipolar and bipolar depression 8W, 2M/54 Y SM | BFT, brief 6 sessions 2/week | Before ECT, 1 h and 3 h after ECT | MMSE, 15-Word Learning Task, Memory Comparisons Task, Concept Shifting Test, Letter-Digit Modalities Test, Stroop Color-Word Test, Fluency Task, CFQ, and SCL-90 | S100-b levels increased 1 h and 3 h after ECT; higher S-100b concentration at baseline was associated with poorer memory function at 5 and 30 days of follow-up | 6 |
| Piccinni et al. 2013 | Aβ40, Aβ42 | 25 | Bipolar depression 12M, 13W/44 Y SM, STOP ST | BFT, brief 8.3 sessions 2/week | Pre-TEC, 1 week after last ECT | MMSE | Aβ40 levels negatively correlated with pre- and post-ECT MMSE scores; Aβ40/Aβ42 negatively correlated with post-ECT MMSE score | 6 |
| Kranaster et al. 2016 | Aβ42 | 12 | Unipolar and bipolar depression 7W, 5M/59 Y SM | RUL 10.6 sessions 2–3/week | Pre-ECT and 1–7 days post-ECT | MMSE | - | 6 |
| Yamazaki et al. 2017 | Aβ40, Aβ42 | 42 (13 ECT) | Unipolar and bipolar depression 31W, 11M (9W, 4M ECT)/69 Y SM | BFT, brief 3/week | Pre-ECT, 2–4 weeks after ECT | MMSE, CDR, Logical Memory I and II subscales of WMS-R, Wisconsin Card Sorting Test and VFT | Aβ40 levels before discharge were negatively correlated with VFT scores; Aβ40 levels on admission were significantly higher in MCI-non-reversors compared with cognitively preserved patients or MCI-reversors | 7 |
| Bousman et al. 2015 | COMT, DRD2, BDNF, APOE | 117 | Unipolar and bipolar depression 42% M/48 Y | BFT, BF, RUL, PW 0.3–1 ms 9 sessions 3/week | 1–3 days after ECT | MCG, HVLT-R, VFT, Cross Out task, SDMT, AMI-SF, and WTAR | Interaction between DRD2 C957T and BDNF Val66Met polymorphisms on anterograde memory | 5.5 |
| Ryan et al. 2019 | TL | 180 (100 P) | Unipolar and bipolar depression P (62W, 38M), C (54W, 26M)/54 Y SM | BFT, RUL 8 sessions | Pre- and post-ECT | Time to recovery orientation, MMSE and CAMI-SF | - | 7 |
| Neylan et al. 2001 | Cortisol | 16 | Unipolar and bipolar depression 11W, 5M/49 Y SM | RUL, brief pulse 6 sessions 3/week | 1 day before ECT (saliva—8 A.M., 4 P.M., and 10 P.M.) and cognitive post-ECT assessment 1 day after ECT | Mattis Dementia Rating Scale, TMT, Stroop Color and Word Test, SDMT WMS subtest of Visual Recall, Employee Aptitude Survey and CVLT | Higher cortisol levels predicted ECT-induced cognitive dysfunction | 5 |
| Study | Measure | N | Diagnosis Gender/Age (Mean, Years) Medication Status | ECT Parameters | Time-Points | Cognitive Scales | Significant Results | Quality Index |
|---|---|---|---|---|---|---|---|---|
| Figiel et al. 1990 | WMH | 36 | MDD (ECT-induced delirium) | BFT, brief 3/week | Post-ECT | Mental Status Examination by Strub and Black | WMH within the basal ganglia after ECT | 4.5 |
| Oudega et al. 2015 | WMH, MTLA, GCA | 39 | MDD 26% W/73 Y NM | RUL (18 switch BFT) 2/week | Pre-ECT | IQ CODE | - | 4.5 |
| Wagenmakers et al. 2021 | WMH, MTLA, GCA | 80 | LLD 54% W/73 Y NM | RUL, BFT 11 sessions 2/week | Pre-ECT | MMSE | Worse cognitive functioning before ECT in patients with severe WMH | 5 |
| Diehl et al. 1993 | MTL and thalamic T2 relaxation time | 6 | MDD 1W, 5M/21–55 Y Without APS | RUL, brief 3/week | 1–2 days before ECT, 1 day before 2nd ECT, and 2–2.5 h post 2nd ECT | TMT, Temporal Orientation Test, Benton Visual Retention Test, HVLT, In-house verbal retrograde memory test | Post hoc correlational analyses revealed a significant relationship between left thalamus T2 relaxation time increases and ECT-induced verbal anterograde memory impairment | 5 |
| Kunigiri et al. 2007 | Thalamus, hippocampal, MTL, and DLPFC T2 relaxation time | 15 | Melancholic depression 8W, 7M/32 Y NM | BFT, RUL 3/week | 48 h after 1st ECT and 2 h after 2nd ECT | OBT, TMT-A, WMS, VLT and BVRT | - | 5.5 |
| Gbyl et al. 2019 | Cortical thickness and hippocampal volume | 18 | Unipolar and bipolar depression 10W, 8M/47 Y SM | BFT, brief 11.9 sessions 3/week | 2 days pre-ECT, 2 days, 6 days, and 6 months post-ECT | SCIP-D | - | 6 |
| Xu et al. 2019 | Cortical thickness, surface area, and local gyrification index | 23 | MDD 12W, 11M/39 Y | BFT, brief 7.3 sessions 3/week | 12–24 h pre-ECT and 24–72 h after ECT | AVLT | Cortical thickness increases in the left inferior parietal gyrus were positively correlated with AVLT score after ECT | 6 |
| Lekwauwa et al. 2006 | Hippocampal volume | 15 | Unipolar depression 12W, 3M/74 Y | BFT, RUL 11.4 sessions | 47 days after ECT | MMSE | The hippocampal volume mean of those patients with moderate or severe memory problems after ECT was significantly smaller compared to those patients without or mild memory problems | 5.5 |
| Nordanskog et al. 2014 | Hippocampal volume | 20 | Unipolar and bipolar depression 10W, 2M/40 Y SM | RUL, BFT, brief 10.2 sessions 3/week | 1-week pre-ECT, 1 week, 6 months, and 1-year post-ECT | RAVLT, RCFT, TMT-A, B, Stroop Test, VFT, Digit Symbol, Digit Span, and Block Design Test | Hippocampal volume increases one week after ECT and decreases 6 months after ECT; left hippocampal volume increase was positively correlated to TMT-A score improvement after ECT (disappeared after controlling for the number of ECT sessions) | 6 |
| Van Oostrom et al. 2018 | Hippocampal volume | 37 (19 P) | Unipolar depression P (37% M/50 Y), C (39% M/52 Y) NM | BFT, brief 17.7 sessions 2/week | 1 week before ECT and 1 week after | TMT-A, B, VFT, RAVLT, WMS II, Visual Reproduction I-I, I and National Adult Reading Test | Hippocampal volume increases were correlated with ECT-induced decrease cognitive functioning | 7 |
| Gbyl et al. 2020 | Hippocampal subfields volume | 22 | Unipolar and bipolar depression 11W, 11M/45 Y SM | BFT, brief 12.5 sessions 3/week | Pre-ECT, 1 week and 6 months after ECT | SCIP | Hippocampal subfields volume increases were associated with decline in cognitive performance during ECT while hippocampal subfields volume decreases correlated with cognitive recovery at 6 months follow-up | 6 |
| Study | ROI | N | Diagnosis Gender/Age (Mean, Years) Medication Status | ECT Parameters | Time-Points | Cognitive SCALES | Significant Results | Quality Index |
|---|---|---|---|---|---|---|---|---|
| Abbot et al. 2014 | Hippocampus | 19 | MDD 13W, 6M/65 Y 19 AD and 11 APS | RUL, BFT 11 sessions 3/week | Post-ECT | RBANS | Hippocampal FC normalization after ECT | 5.5 |
| Bai et al. 2018 | Hippocampus | 45 | MDD 28W, 17M/38 Y | BFT 6–12 sessions 3/week | Pre-ECT and post-ECT | CVFT | Decreased hippocampal-angular FC was associated with cognitive impairment after ECT | 6 |
| Wang et al. 2019 | Salience network | 23 | MDD 11W, 11M/37 Y | BFT, brief 3/week | Pre-ECT and post-ECT | AVLT | Functional and effective connectivity changes within the salience network correlated with delayed memory dysfunction | 6 |
| Wang et al. 2020 | Whole-brain | 24 | MDD 11 W, 13M/37 Y STOP ST, BZD | BFT, brief 6.9 sessions 3/week | Pre-ECT, 1–7 days post-ECT and 1-month post-ECT | RAVLT | Functional connectivity within the FPN, the DMN, and subcortical structures were able to predict RAVLT changes after ECT | 6 |
| Sinha et al. 2019 | Frontal and limbic lobes | 17 | MDD 10W, 7M/45 Y SM | BFT, brief 7.2 sessions | Pre-ECT and after 6th ECT | WMS | - | 6 |
| Wei et al. 2019 | Whole-brain | 28 P 20 HC | MDD 16 W, 12M/37 Y SM | BFT, brief 7.64 sessions 3/week | Pre-ECT and post-ECT | VFT | Left pulvinar-bilateral precuneus FC was associated with poor cognitive functioning after ECT | 7 |
| Wei et al. 2020 | DMN | 28 P 20 HC | MDD 16W, 12M/37 Y SM | BFT, brief 7.64 sessions 3/week | Pre-ECT and post-ECT | VFT | Increased left sgACC—left cerebellar lobule VI FC correlated with VFT scores after ECT | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bassa, A.; Sagués, T.; Porta-Casteràs, D.; Serra, P.; Martínez-Amorós, E.; Palao, D.J.; Cano, M.; Cardoner, N. The Neurobiological Basis of Cognitive Side Effects of Electroconvulsive Therapy: A Systematic Review. Brain Sci. 2021, 11, 1273. https://doi.org/10.3390/brainsci11101273
Bassa A, Sagués T, Porta-Casteràs D, Serra P, Martínez-Amorós E, Palao DJ, Cano M, Cardoner N. The Neurobiological Basis of Cognitive Side Effects of Electroconvulsive Therapy: A Systematic Review. Brain Sciences. 2021; 11(10):1273. https://doi.org/10.3390/brainsci11101273
Chicago/Turabian StyleBassa, Adriana, Teresa Sagués, Daniel Porta-Casteràs, Pilar Serra, Erika Martínez-Amorós, Diego J. Palao, Marta Cano, and Narcís Cardoner. 2021. "The Neurobiological Basis of Cognitive Side Effects of Electroconvulsive Therapy: A Systematic Review" Brain Sciences 11, no. 10: 1273. https://doi.org/10.3390/brainsci11101273